
Research on Urban Medical and Health Services Efficiency and Its Spatial Correlation in China: Based on Panel Data of 13 Cities in Jiangsu Province


Abstract
:1. Introduction
2. Materials and Methods
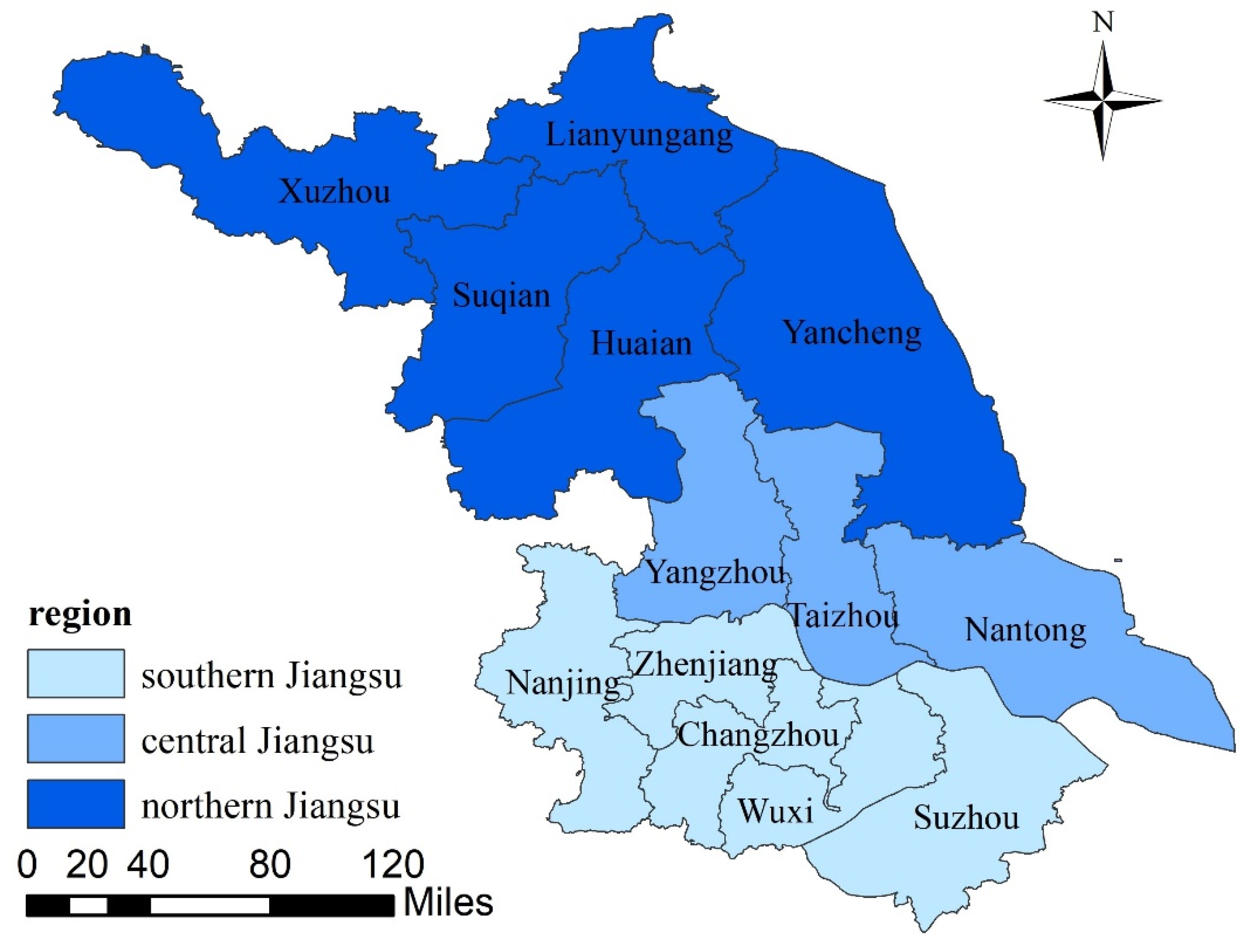
2.1. Study Areas
2.2. Methods
2.2.1. Data Envelopment Analysis
- (1)
- DEA-SE-SBM Model
- (2)
- DEA-Malmquist Model
2.2.2. Exploratory Spatial Data Analysis
- (1)
- Global Spatial Autocorrelation
- (2)
- Local Spatial Autocorrelation
2.3. Selection of Indicators and Data Sources
2.4. Medical and Health Input-Output in Jiangsu Province
3. Results of the Comprehensive Evaluation of the Efficiency of Medical and Health Services
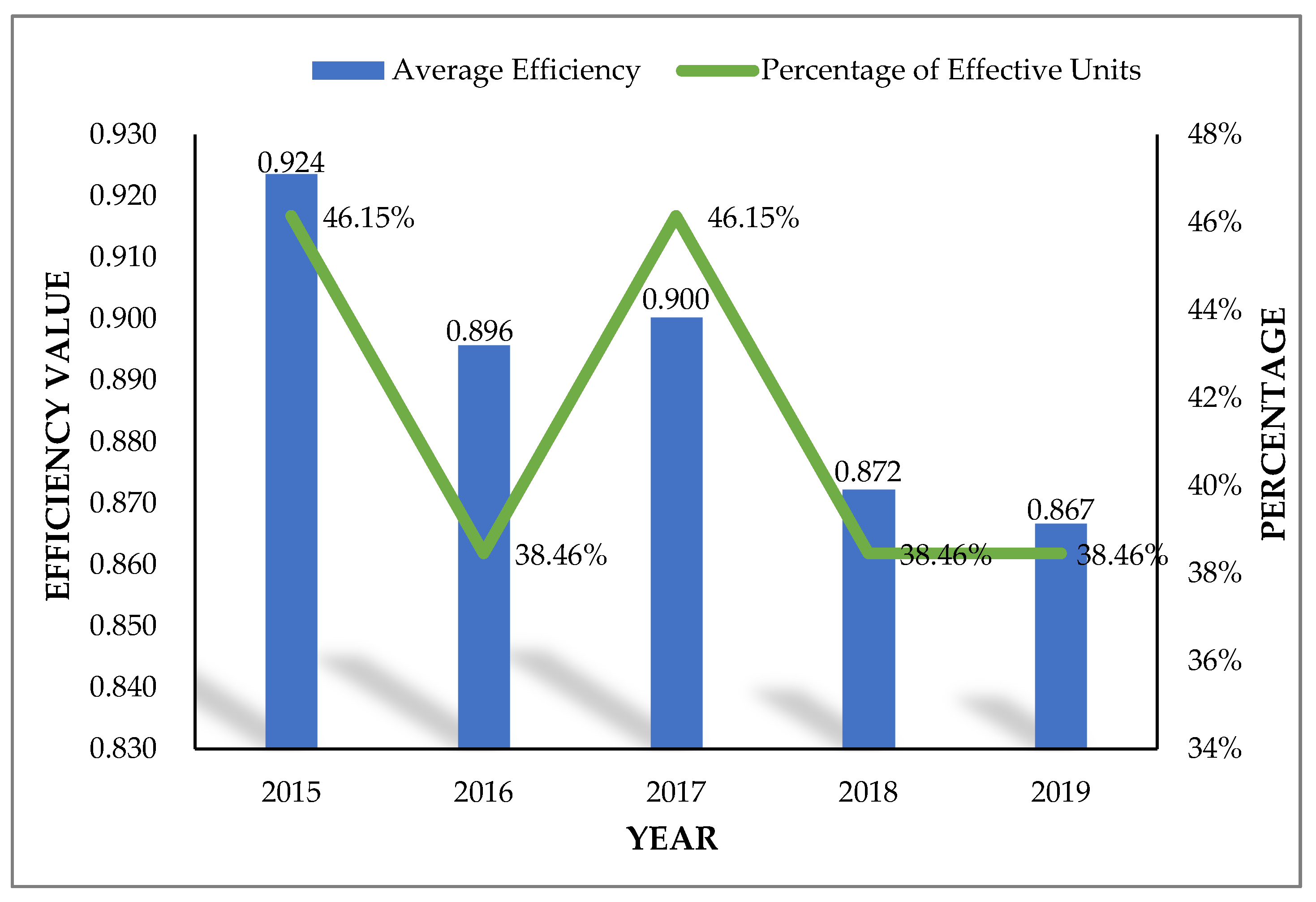
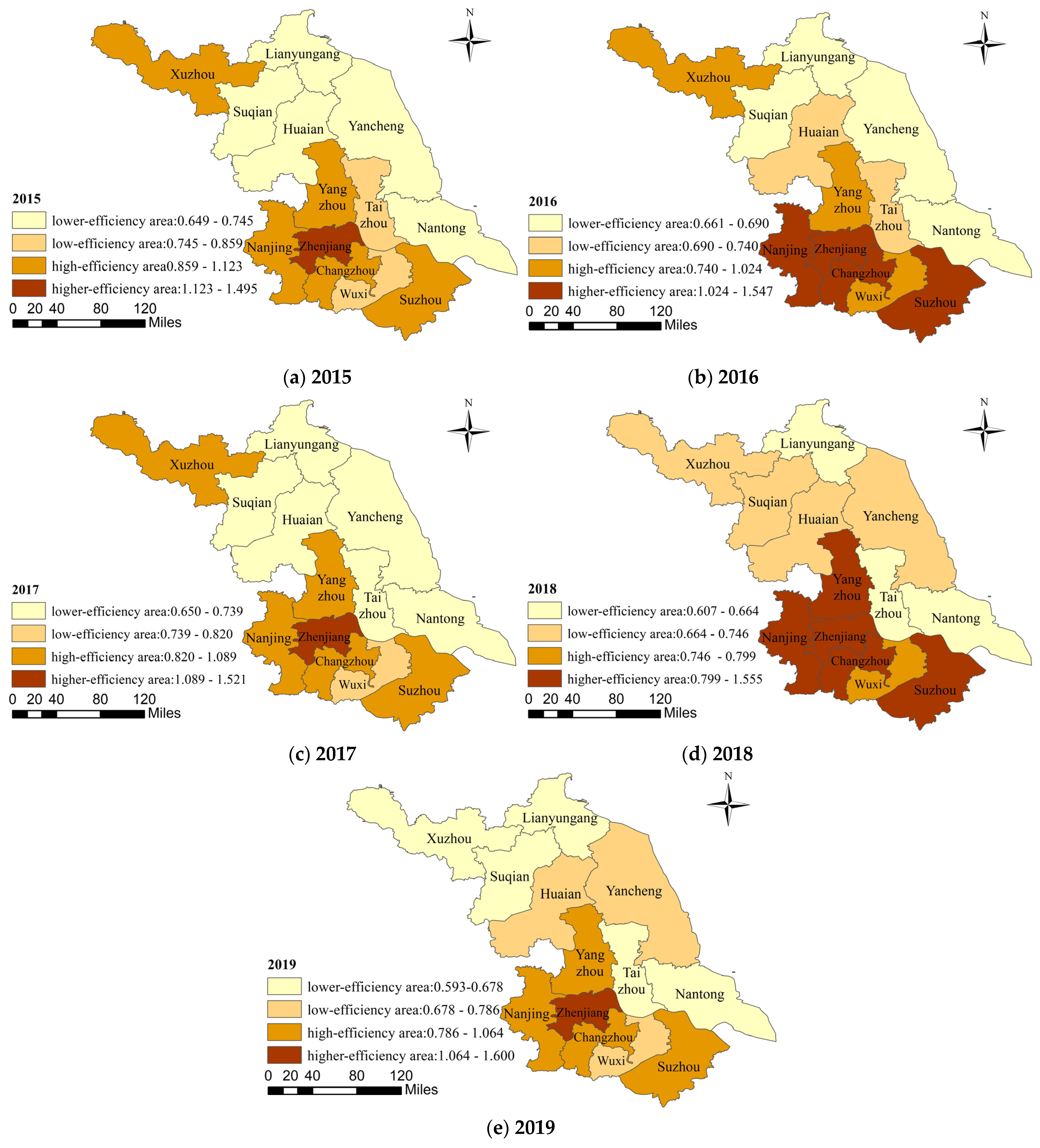
3.1. Results of the DEA-SE-SBM Model
3.2. Results of the DEA-Malmquist Model
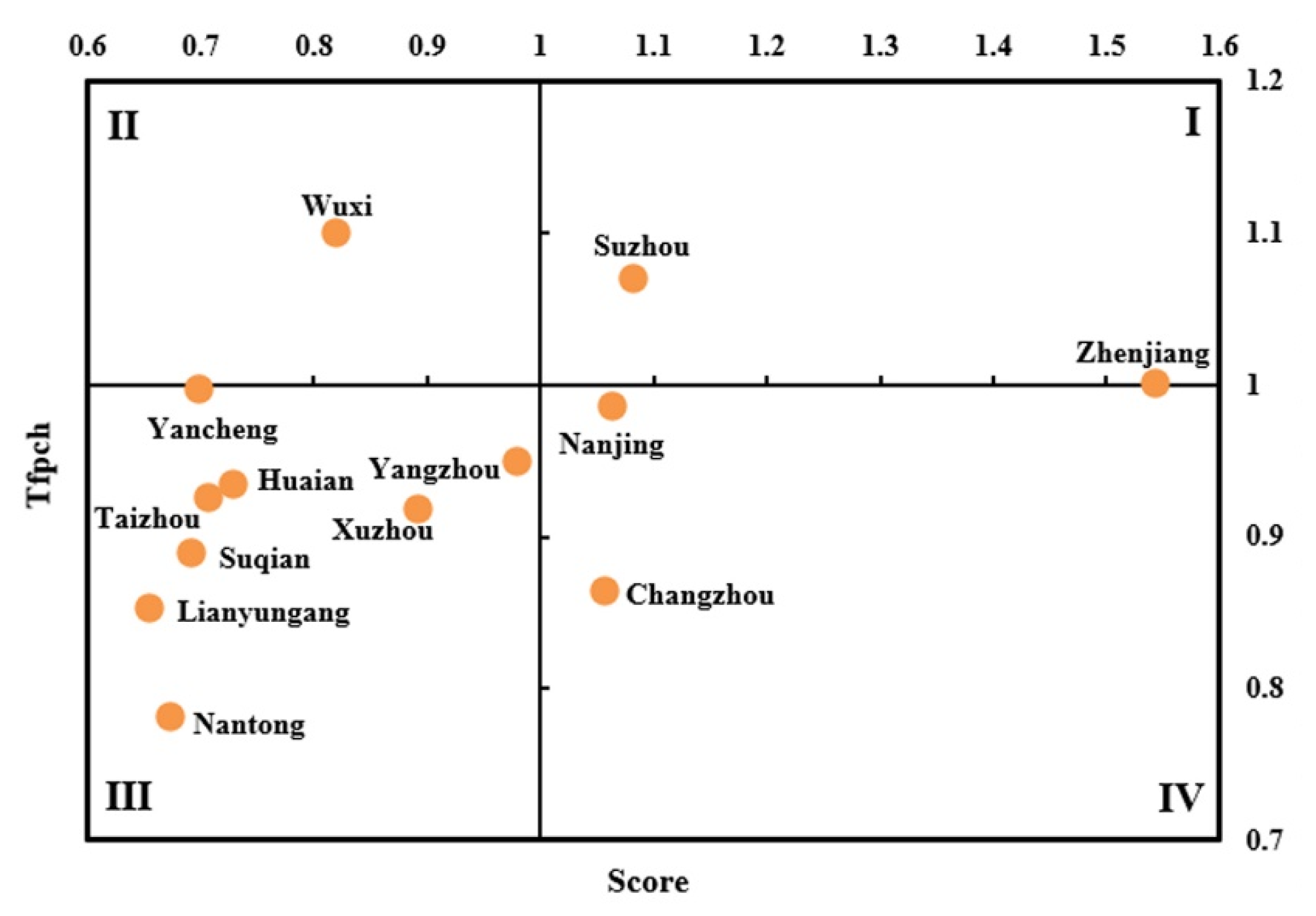
3.3. Results of the Comprehensive Evaluation
4. Results of Spatial Correlation Analysis of the Efficiency of Medical and Health Services
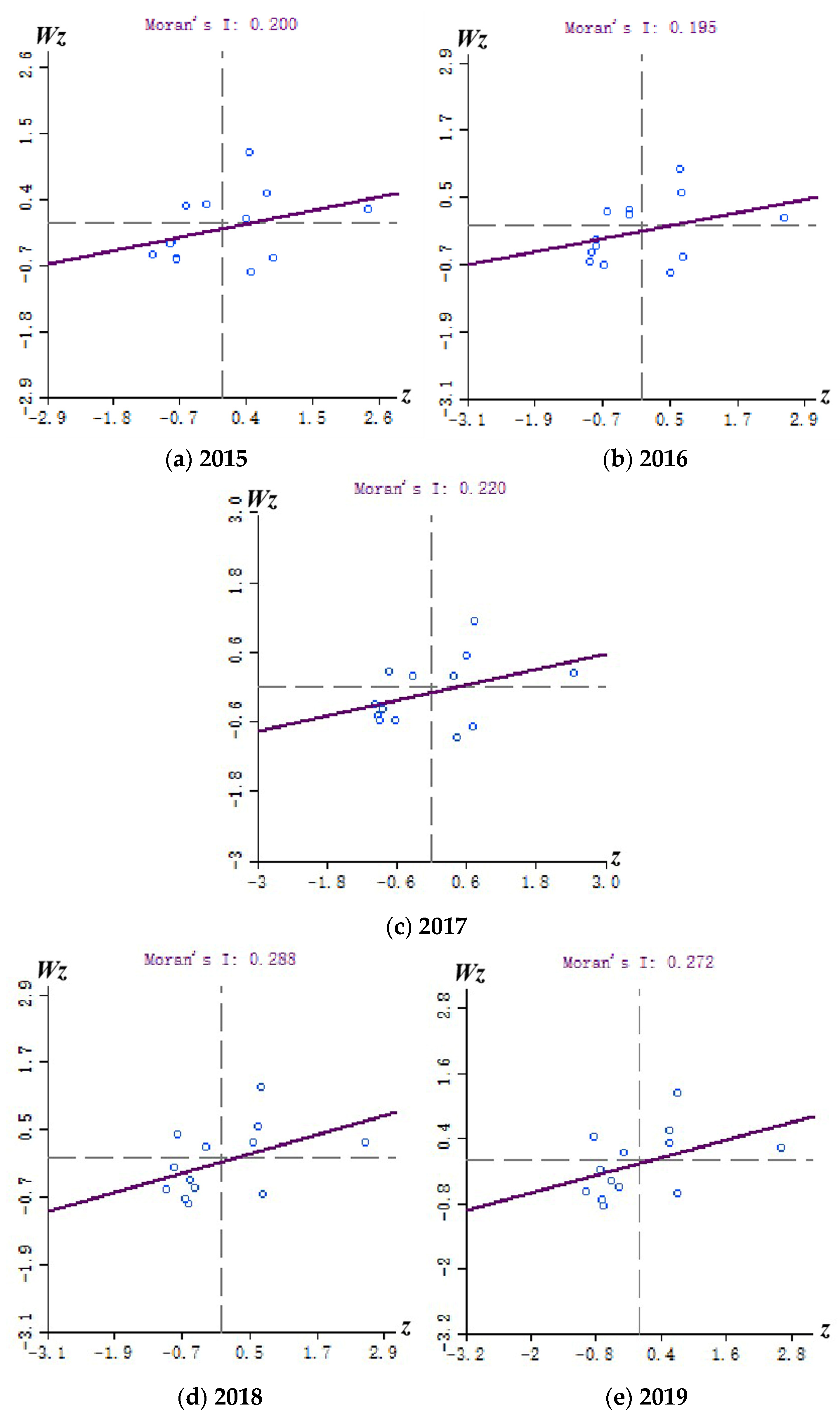
4.1. Results of Global Autocorrelation Analysis
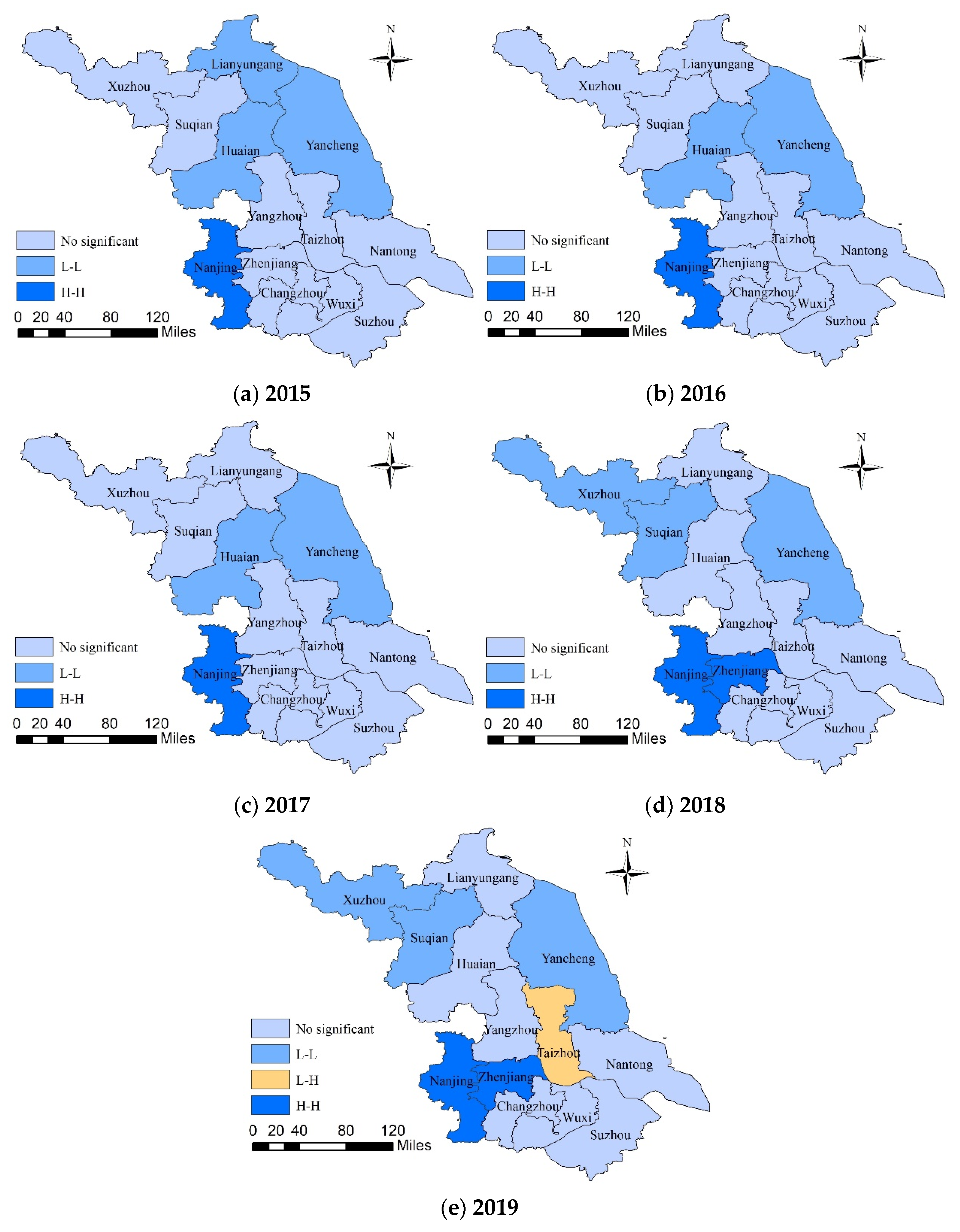
4.2. Results of Local Autocorrelation Analysis
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DEA | Data Envelopment Analysis; |
| SFA | Stochastic Frontier Analysis; |
| BCC | Banker, Charnes, and Cooper model; |
| CCR | Charnes, Cooper, and Rhodes model; |
| SBM | slack-based measure model; |
| SE-SBM | super efficiency slack-based measure model; |
| ESDA | Exploratory Spatial Data Analysis; |
| DMUs | Decision-making units; |
| TFPCH | Total Factor Productivity Change index; |
| EFFCH | Technical Efficiency Change index; |
| TECHCH | Technical Change index; |
| VRS | variable returns to scale; |
| PECH | Pure Efficiency Change index; |
| SECH | Scale Efficiency Change index; |
| LISA | Local Indicator of Spatial Association; |
References
- Johns, B.; Steinhardt, L.; Walker, D.G.; Peters, D.H.; Bishai, D. Horizontal equity and efficiency at primary health care facilities in rural Afghanistan: A seemingly unrelated regression approach. Soc. Sci. Med. 2013, 89, 25–31. [Google Scholar] [CrossRef]
- Farrell, M.J. The Measurement of Productive Efficiency. J. R. Stat. Soc. 1957, 120, 253–290. [Google Scholar] [CrossRef]
- Palmer, S.; Torgerson, D.J. Definitions of efficiency. Br. Med. J. 1999, 318, 1136. [Google Scholar] [CrossRef]
- National Bureau of Statistics of the People’s Republic of China. China Statistical Yearbook in 2020. Available online: http://www.stats.gov.cn/tjsj/ndsj/2020/indexch.htm. (accessed on 26 August 2021).
- Yi, M.; Peng, J.; Zhang, L.; Zhang, Y. Is the allocation of medical and health resources effective? Characteristic facts from regional heterogeneity in China. Int. J. Equity Health 2020, 19, 89. [Google Scholar] [CrossRef]
- Lu, C.; Zhang, Z.; Lan, X. Impact of China’s Referral Reform on the Equity and Spatial Accessibility of Healthcare Resources: A Case Study of Beijing. Soc. Sci. Med. 2019, 235, 112386. [Google Scholar] [CrossRef] [PubMed]
- The Fourteenth Five-Year Plan for National Economic and Social Development of the People’s Republic of China and the Outline of Long-Term Goals for 2035. Available online: http://www.xinhuanet.com/2021-03/13/c_1127205564.htm (accessed on 7 April 2021).
- Hollingsworth, B. The measurement of efficiency and productivity of health care delivery. Health Econ. 2008, 17, 1107–1128. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Cai, M.; Tao, H.; He, Z.; Lin, X.; Zuo, Y. Efficiency and productivity measurement of rural township hospitals in China: A bootstrapping data envelopment analysis. BMJ Open 2016, 6, e011911. [Google Scholar] [CrossRef] [Green Version]
- Kohl, S.; Schoenfelder, J.; Fügener, A.; Brunner, J.O. The use of Data Envelopment Analysis (DEA) in healthcare with a focus on hospitals. Health Care Manag. Sci. 2019, 22, 245–286. [Google Scholar] [CrossRef]
- Ahmed, S.; Hasan, M.Z.; Maclennan, M.; Dorin, F.; Ahmed, M.W.; Hasan, M.M.; Hasan, S.M.; Islam, M.T.; Khan, J.A.M. Measuring the efficiency of health systems in Asia: A data envelopment analysis. BMJ Open 2019, 9, e022155. [Google Scholar] [CrossRef] [Green Version]
- Andrews, A. Investigating Technical Efficiency and its Determinants: Case of New Zealand District Health Boards. Health Policy Technol. 2020, 9, 323–334. [Google Scholar] [CrossRef]
- Sherman, H.D. Hospital efficiency measurement and evaluation: Empirical test of a new technique. Med. Care 1984, 22, 922–938. [Google Scholar] [CrossRef] [PubMed]
- Campos, M.S.; Fernandez-Montes, A.; Gavilan, J.M.; Velasco, F. Public resource usage in health systems: A data envelopment analysis of the efficiency of health systems of autonomous communities in Spain. Public Health 2016, 138, 33–40. [Google Scholar] [CrossRef]
- Ozcan, Y.A.; Khushalani, J. Assessing efficiency of public health and medical care provision in OECD countries after a decade of reform. Cent. Eur. J. Oper. Res. 2017, 25, 325–343. [Google Scholar] [CrossRef] [Green Version]
- Mohamadi, E.; Manesh, A.O.; Takian, A.; Majdzadeh, R.; Lotfi, F.H.; Sharafi, H.; Jowett, M.; Kiani, M.M.; Abadi, L.H.Q.; Fazaeli, A.a.; et al. Technical Efficiency in health production: A comparison between Iran and other upper middle-income countries. Health Policy Technol. 2020, 9, 335–347. [Google Scholar] [CrossRef]
- Giménez, V.; Prieto, W.; Prior, D.; Tortosa-Ausina, E. Evaluation of efficiency in Colombian hospitals: An analysis for the post-reform period. Socioecon. Plan. Sci. 2019, 65, 20–35. [Google Scholar] [CrossRef]
- Tigga, N.S.; Mishra, U.S. On measuring technical efficiency of the health system in India: An application of data envelopment analysis. J. Health Manag. 2015, 17, 285–298. [Google Scholar] [CrossRef]
- Hu, Y.J. Regional Differences in the Efficiency of Health Public Service Supply in China. Syst. Eng. 2018, 36, 150–158. [Google Scholar]
- Yang, S.L.; Liu, T.; Chen, J. Measurement and dynamic analysis of the efficiency of rural medical and health services in the western region. Rural Econ. 2020, 11, 129–135. [Google Scholar]
- Ben, H.; Zhang, Y. Research on the Influence of Social Networks on the Allocation Efficiency of Public Medical Resources—Taking Jiangsu as an Example. Jiangxi Soc. Sci. 2018, 38, 227–234. [Google Scholar]
- Yan, J.J.; Jiang, H.L.; Cheng, Y.Z.; Wang, X.Y. Evaluation of Input-Output Efficiency of Chinese Hospital under the Background of Supply-Side Structural Reform—Based on Factor Analysis and DEA Method. Financ. Econ. 2016, 9, 112–123. [Google Scholar]
- Li, J.; Yang, F.; Mao, Z.F. Analysis on the Equity and Efficiency of County-level Medical and Health Resources Allocation in Hubei Province. Stat. Decis. 2017, 13, 114–117. [Google Scholar]
- Fang, P.Q.; Zhao, L. Analysis of Achieving Health Equity Based on Utilization of Health Resources. Popul. Dev. 2013, 19, 74–83. [Google Scholar]
- Wei, C.K.; Chen, L.C.; Li, R.K.; Tsai, C.H. Exploration of efficiency underestimation of CCR model: Based on medical sectors with DEA-R model. Expert Syst. Appl. 2011, 38, 3155–3160. [Google Scholar] [CrossRef]
- Zhao, T. Efficiency of Institutional Health Care Service in Rural China Taking Account of Demand-Side Factors: Empirical Study Based on the Survey of Three Provinces. Nankai Econ. Stud. 2017, 3, 34–49. [Google Scholar]
- Zheng, D.; Gong, J.; Zhang, C. Efficiency of medical service systems in the rural areas of Mainland China: A comparative study from 2013 to 2017. Public Health 2019, 171, 139–147. [Google Scholar] [CrossRef]
- Ding, J.M.; Hu, X.J.; Zhang, X.Z.; Shang, L.; Yu, M.; Chen, H.L. Equity and efficiency of medical service systems at the provincial level of China’s mainland: A comparative study from 2009 to 2014. BMC Public Health 2018, 18, 214. [Google Scholar] [CrossRef] [PubMed]
- Du, T.; Ran, R.; Li, J.L.; Wang, S.S. Dynamic Evaluation of China’s Healthcare Service Efficiency based on DtSBM Model. J. Beijing Inst. Technol. (Soc. Sci. Ed.) 2019, 21, 82–94. [Google Scholar]
- Yu, J.L.; Qian, Z.W. Investment gap in health care industry and the temporal-spatial evolution of health service efficiency at provincial administrative institutions of China. J. Arid Land Resour. Environ. 2018, 32, 59–66. [Google Scholar]
- Charnes, A.; Cooper, W.W.; Rhodes, E. Measuring the efficiency of decision making units. Eur. J. Oper. Res. 1978, 2, 429–444. [Google Scholar] [CrossRef]
- Banker, R.D.; Charnes, A.; Cooper, W.W. Some Models for Estimating Technical and Scale Inefficiencies in Data Envelopment Analysis. Manag. Sci. 1984, 30, 1078–1092. [Google Scholar] [CrossRef] [Green Version]
- Avkiran, N.K.; Tone, K.; Tsutsui, M. Bridging radial and non-radial measures of efficiency in DEA. Ann. Oper. Res. 2008, 164, 127–138. [Google Scholar] [CrossRef]
- Adler, N.; Friedman, L.; Sinuany-Stern, Z. Review of ranking methods in the data envelopment analysis context. Eur. J. Oper. Res. 2002, 140, 249–265. [Google Scholar] [CrossRef]
- Tone, K. A slacks-based measure of efficiency in data envelopment analysis. Eur. J. Oper. Res. 2001, 130, 498–509. [Google Scholar] [CrossRef] [Green Version]
- Tone, K. A slacks-based measure of super-efficiency in data envelopment analysis. Eur. J. Oper. Res. 2002, 143, 32–41. [Google Scholar] [CrossRef] [Green Version]
- Färe, R.; Grosskopf, S.; Lindgren, B.; Roos, P. Productivity changes in Swedish pharmacies 1980–1989: A non-parametric Malmquist approach. J. Prod. Anal. 1992, 3, 81–97. [Google Scholar] [CrossRef]
- Anselin, L. Interactive techniques & exploratory spatial data analysis. In Geographical Information Systems: Principles, Techniques, Management and Applications; Longley, P.A., Goodchild, M.F., Maguire, D.J., Eds.; Wiley: New York, NY, USA, 1999; pp. 251–264. [Google Scholar]
- Yuan, S.Y.; Li, Y.W.; Chen, W.G.; Xie, Q.W. Study on Industrial Ecology and Spatial Agglomeration Effect—Panel Data from 31 Chinese Regions. Manag. Rev. 2020, 32, 72–81. [Google Scholar]
- Qiu, Y.S.; Zhu, Z.M.; Huang, H.P.; Bing, Z.H. Study on the evolution of B&Bs spatial distribution based on exploratory spatial data analysis (ESDA) and its influencing factors—With Yangtze River Delta as an example. Eur. J. Remote Sens. 2021, 54, 296–308. [Google Scholar]
- Jackson, M.C.; Huang, L.; Xie, Q.; Tiwari, R.C. A modified version of Moran’s I. Int. J. Health Geogr. 2010, 9, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.Y.; Huang, X.B.; Xiao, Y.; Jiang, Y.; Shan, X.W.; Zhang, J.; Cai, S.X.; Liu, J.B. Spatial analysis of Schistosomiasis in Hubei Province, China: A GIS-based analysis of Schistosomiasis from 2009 to 2013. PLoS ONE 2015, 10, e0118362. [Google Scholar] [CrossRef] [Green Version]
- Zhou, H.; Huang, J.J.; Yuan, Y.B. Analysis of the Spatial Characteristics of the Water Usage Patterns Based on ESDA-GIS: An Example of Hubei Province, China. Water Resour. Manag. 2017, 31, 1503–1516. [Google Scholar] [CrossRef]
- Anselin, L. Local Indicators of Spatial Association—LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Murray, C.J.; Frenk, J. Health metrics and evaluation: Strengthening the science. Lancet 2008, 371, 1191–1199. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Q.; Jiang, T.; Wang, J. Equity and efficiency of primary health care resource allocation in mainland China. Int. J. Equity Health 2018, 17, 140. [Google Scholar] [CrossRef] [Green Version]
- Top, M.; Konca, M.; Sapaz, B. Technical efficiency of healthcare systems in African countries: An application based on data envelopment analysis. Health Policy Technol. 2020, 9, 62–68. [Google Scholar] [CrossRef]
- Zhong, K.L.; Chen, L.; Chen, S.X.; Chen, H.J.; Long, F. The efficiency of primary health care institutions in the Counties of Hunan province, China: Data from 2009 to 2017. Int. J. Environ. Res. Public Health 2020, 17, 1781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tobler, W.R. A computer movie simulating urban growth in the Detroit region. Econ. Geogr. 1970, 46, 234–240. [Google Scholar] [CrossRef]
- Liu, W.; Wang, X. Spatial Analysis of the Factors to Influence the Efficiency of Rural Basic Public Health Services. Chin. Health Serv. Manag. 2020, 37, 687–691. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | Prefecture-Level City |
|---|---|
| southern Jiangsu | Zhenjiang, Nanjing, Changzhou, Suzhou, Wuxi |
| central Jiangsu | Yangzhou, Taizhou, Nantong |
| northern Jiangsu | Lianyungang, Suqian, Huaian, Yancheng, Xuzhou |
| Items | Specific Indicators | Explanation of Indicators | Significance of Indicators | References |
|---|---|---|---|---|
| Input | X1: Number of health technicians (person) | Health technicians mainly include registered nurses, licensed (assistant) physicians, pharmacists, health supervisors, technicians, and other health technicians. | Reflecting the investment scale of medical and health human resources in each year in the study area. | [5,9,21,48] |
| X2: Number of Health Institutions (unit) | Health Institutions mainly include hospitals, professional public health institutions, primary medical and health institutions, and other institutions. | Reflecting the input of medical and health material resources in each year in the study area. | [20,24,29,30,47] | |
| X3: Number of Beds (unit) | The number of beds is the sum of the number of beds in various medical and health institutions each year. | [9,20,27,28,46,47] | ||
| Output | Y1: Number of Outpatients and Emergency Visits (10,000 person) | Outpatient and emergency visits are the sum of outpatient visits and emergency visits. | Reflecting the supply of medical and health services of the research subjects in that year. | [9,23,28,48] |
| Y2: Utilization Rate of Beds (%) | The utilization rate of beds indicates the utilization of beds in all medical and health institutions in each region. | [5,24,27] |
| Region | Cities | 2015 | 2019 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| X1 | X2 | X3 | Y1 | Y2 | X1 | X2 | X3 | Y1 | Y2 | ||
| southern Jiangsu | Nanjing | 65,139 | 2337 | 46,643 | 7010.00 | 89.84 | 93,856 | 3242 | 59,046 | 9070.70 | 91.17 |
| Wuxi | 44,707 | 2243 | 37,366 | 4856.00 | 86.82 | 59,303 | 2770 | 50,478 | 5786.16 | 79.42 | |
| Changzhou | 29,616 | 1196 | 24,263 | 2804.00 | 98.06 | 37,086 | 1458 | 28,322 | 3223.91 | 90.53 | |
| Suzhou | 68,179 | 3121 | 59,304 | 8968.00 | 88.34 | 91,047 | 3720 | 71,657 | 10,085.47 | 86.52 | |
| Zhenjiang | 18,985 | 943 | 14,637 | 2326.00 | 77.90 | 21,691 | 1013 | 15,844 | 2484.23 | 84.99 | |
| central Jiangsu | Nantong | 41,067 | 3147 | 36,031 | 3908.00 | 93.53 | 50,329 | 3357 | 46,375 | 4253.57 | 87.99 |
| Yangzhou | 24,326 | 1780 | 20,121 | 2592.00 | 90.62 | 29,406 | 1890 | 24,994 | 2588.01 | 92.00 | |
| Taizhou | 24,215 | 1953 | 21,838 | 2405.00 | 87.32 | 31,673 | 2118 | 29,885 | 2508.03 | 86.45 | |
| northern Jiangsu | Xuzhou | 51,567 | 4601 | 47,949 | 5880.00 | 99.74 | 70,767 | 4594 | 60,988 | 6245.99 | 87.19 |
| Lianyungang | 23,056 | 2708 | 19,035 | 2729.00 | 75.90 | 31,117 | 2740 | 28,101 | 2859.41 | 75.85 | |
| Huaian | 30,475 | 2228 | 25,966 | 2776.00 | 91.01 | 35,963 | 2200 | 30,376 | 2731.71 | 88.64 | |
| Yancheng | 39,494 | 3242 | 37,169 | 3986.00 | 80.67 | 44,358 | 3270 | 40,301 | 4767.89 | 81.99 | |
| Suqian | 26,179 | 2426 | 23,290 | 2929.00 | 77.74 | 36,749 | 2424 | 29,548 | 3344.65 | 78.21 | |
| Cities | 2015 | 2016 | 2017 | 2018 | 2019 | Mean |
|---|---|---|---|---|---|---|
| Nanjing | 1.028 | 1.070 | 1.089 | 1.063 | 1.063 | 1.063 |
| Wuxi | 0.859 | 0.837 | 0.820 | 0.799 | 0.786 | 0.820 |
| Suzhou | 1.123 | 1.084 | 1.079 | 1.064 | 1.064 | 1.083 |
| Changzhou | 1.096 | 1.080 | 1.050 | 1.041 | 1.018 | 1.057 |
| Zhenjiang | 1.495 | 1.547 | 1.521 | 1.555 | 1.600 | 1.544 |
| Taizhou | 0.780 | 0.740 | 0.717 | 0.664 | 0.632 | 0.706 |
| Nantong | 0.724 | 0.685 | 0.650 | 0.647 | 0.663 | 0.674 |
| Yangzhou | 1.016 | 0.838 | 1.000 | 1.022 | 1.024 | 0.980 |
| Lianyungang | 0.741 | 0.665 | 0.667 | 0.607 | 0.593 | 0.655 |
| Xuzhou | 1.034 | 1.024 | 1.012 | 0.714 | 0.678 | 0.893 |
| Huaian | 0.745 | 0.726 | 0.739 | 0.719 | 0.718 | 0.729 |
| Yancheng | 0.649 | 0.661 | 0.675 | 0.746 | 0.759 | 0.698 |
| Suqian | 0.718 | 0.690 | 0.687 | 0.698 | 0.670 | 0.692 |
| Mean | 0.924 | 0.896 | 0.900 | 0.872 | 0.867 | 0.892 |
| Year | EFFCH | TECHCH | PECH | SECH | TFPCH |
|---|---|---|---|---|---|
| 2015—2016 | 1.009 | 0.849 | 1.029 | 0.981 | 0.857 |
| 2016—2017 | 1.004 | 1.004 | 0.996 | 1.009 | 1.009 |
| 2017—2018 | 0.995 | 0.894 | 0.984 | 1.011 | 0.890 |
| 2018—2019 | 0.941 | 1.082 | 0.963 | 0.977 | 1.017 |
| Mean | 0.987 | 0.953 | 0.993 | 0.994 | 0.940 |
| Cities | EFFCH | TECHCH | PECH | SECH | TFPCH |
|---|---|---|---|---|---|
| Wuxi | 1.032 | 1.067 | 1.027 | 1.005 | 1.101 |
| Suzhou | 1.000 | 1.070 | 1.000 | 1.000 | 1.070 |
| Zhenjiang | 1.000 | 1.001 | 1.000 | 1.000 | 1.001 |
| Yancheng | 1.000 | 0.997 | 1.000 | 1.000 | 0.997 |
| Nanjing | 0.969 | 1.018 | 0.974 | 0.995 | 0.986 |
| Yangzhou | 0.991 | 0.959 | 0.991 | 1.000 | 0.950 |
| Huaian | 1.004 | 0.932 | 1.010 | 0.993 | 0.935 |
| Taizhou | 0.986 | 0.939 | 0.960 | 1.028 | 0.926 |
| Xuzhou | 0.973 | 0.944 | 0.968 | 1.005 | 0.918 |
| Suqian | 0.953 | 0.934 | 1.000 | 0.953 | 0.890 |
| Changzhou | 0.993 | 0.871 | 1.039 | 0.955 | 0.864 |
| Lianyungang | 1.000 | 0.853 | 1.000 | 1.000 | 0.853 |
| Nantong | 0.934 | 0.837 | 0.940 | 0.994 | 0.782 |
| Mean | 0.987 | 0.953 | 0.993 | 0.994 | 0.940 |
| Year | 2015 | 2016 | 2017 | 2018 | 2019 |
|---|---|---|---|---|---|
| Moran’s I | 0.200 | 0.195 | 0.220 | 0.288 | 0.272 |
| Z | 1.8455 | 1.8902 | 1.9777 | 2.4557 | 2.3843 |
| P | 0.051 | 0.046 | 0.039 | 0.017 | 0.021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, L.; Wu, F.; Chen, W.; Zhu, C.; Huang, T. Research on Urban Medical and Health Services Efficiency and Its Spatial Correlation in China: Based on Panel Data of 13 Cities in Jiangsu Province. Healthcare 2021, 9, 1167. https://doi.org/10.3390/healthcare9091167
Lin L, Wu F, Chen W, Zhu C, Huang T. Research on Urban Medical and Health Services Efficiency and Its Spatial Correlation in China: Based on Panel Data of 13 Cities in Jiangsu Province. Healthcare. 2021; 9(9):1167. https://doi.org/10.3390/healthcare9091167
Chicago/Turabian StyleLin, Lingling, Fang Wu, Wei Chen, Chenming Zhu, and Tao Huang. 2021. "Research on Urban Medical and Health Services Efficiency and Its Spatial Correlation in China: Based on Panel Data of 13 Cities in Jiangsu Province" Healthcare 9, no. 9: 1167. https://doi.org/10.3390/healthcare9091167