
Associations between Personality Traits, Intolerance of Uncertainty, Coping Strategies, and Stress in Italian Frontline and Non-Frontline HCWs during the COVID-19 Pandemic—A Multi-Group Path-Analysis

 ,
,  ,
,  ,
, 
 ,
, 
Abstract
:1. Introduction
1.1. Intolerance of Uncertainty, Personality, and Coping
1.2. Coping, Personality, Intolerance of Uncertainty
1.3. Current Study
2. Methods
2.1. Data Collection
- Twelve questions, aiming to collect socio-demographic, employment information, and information concerning the exposure of HCWs to COVID-19;
- Four validated scales (see Section 2.2. “Measures”), aiming to measure HCWs’ personality traits, intolerance of uncertainty, coping strategies, and perceived stress;
- One final open-ended question (which is not taken into account in the present study, as it is the specific subject of another paper that we are going to submit), aiming to know whether and how the experience of having worked during the pandemic had an emotional impact on HCWs.
2.2. Measures
2.2.1. Personal Information Data
2.2.2. Big Five Inventory, Short Version (BFI-2-S)
2.2.3. Intolerance of Uncertainty Scale (IUS-12)
2.2.4. Brief-COPE Scale
2.2.5. Italian Perceived Stress Scale (IPSS-10)
2.3. Procedures
- First, tested if there were significant differences between the two groups of HCWs (frontline and non-frontline) in relation to each of the variables considered;
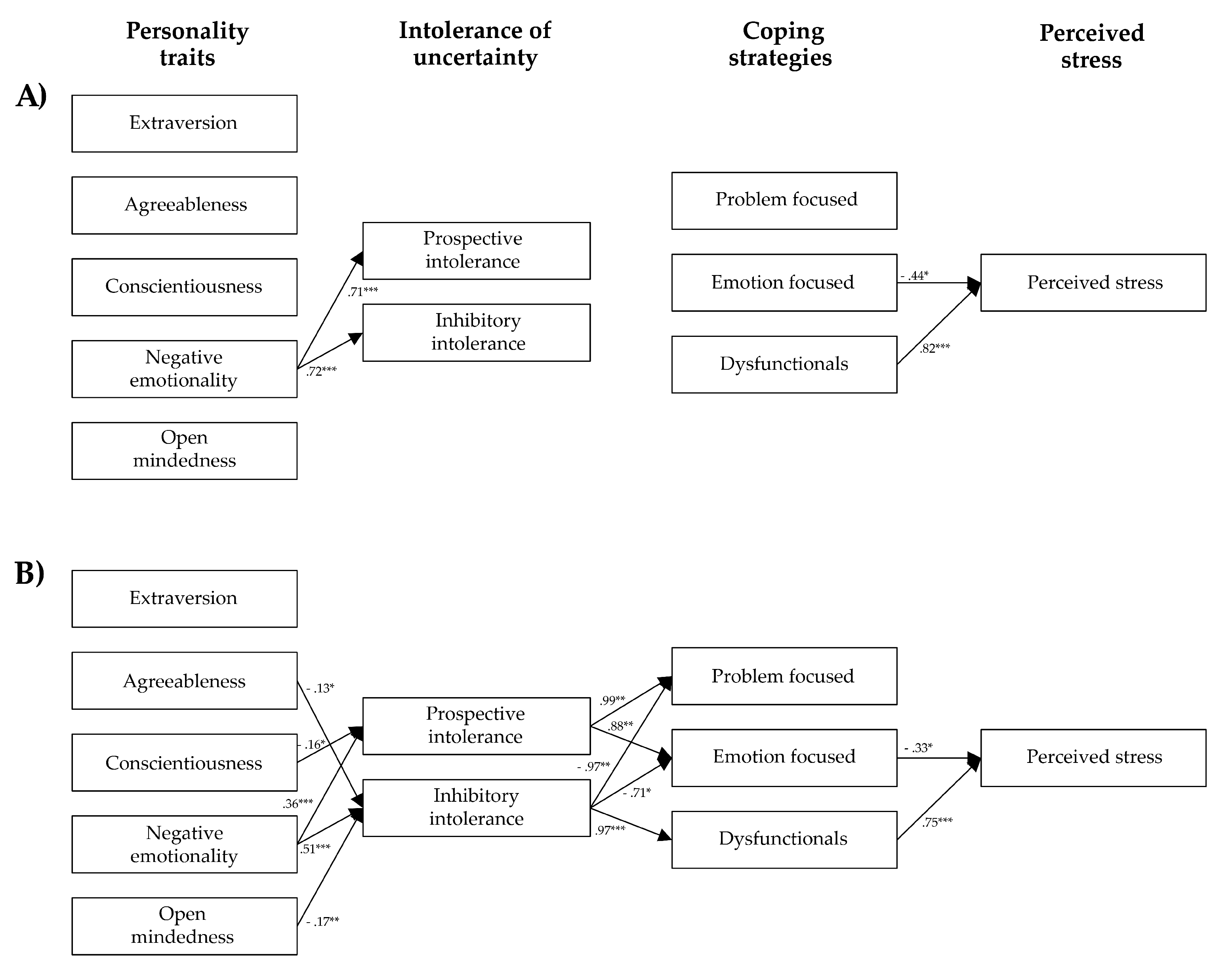
- Second, developed and tested a model (see Figure 1), according to which personality traits can differentially impact on intolerance of uncertainty, intolerance of uncertainty can differently impact on the use of coping strategies, and coping strategies can differently affect the level of perceived stress;
- Finally, tested whether the structure of the relations (see Figure 1) vary in the two groups of HCWs.
2.4. Data Analysis
3. Results
3.1. Sample Characteristics
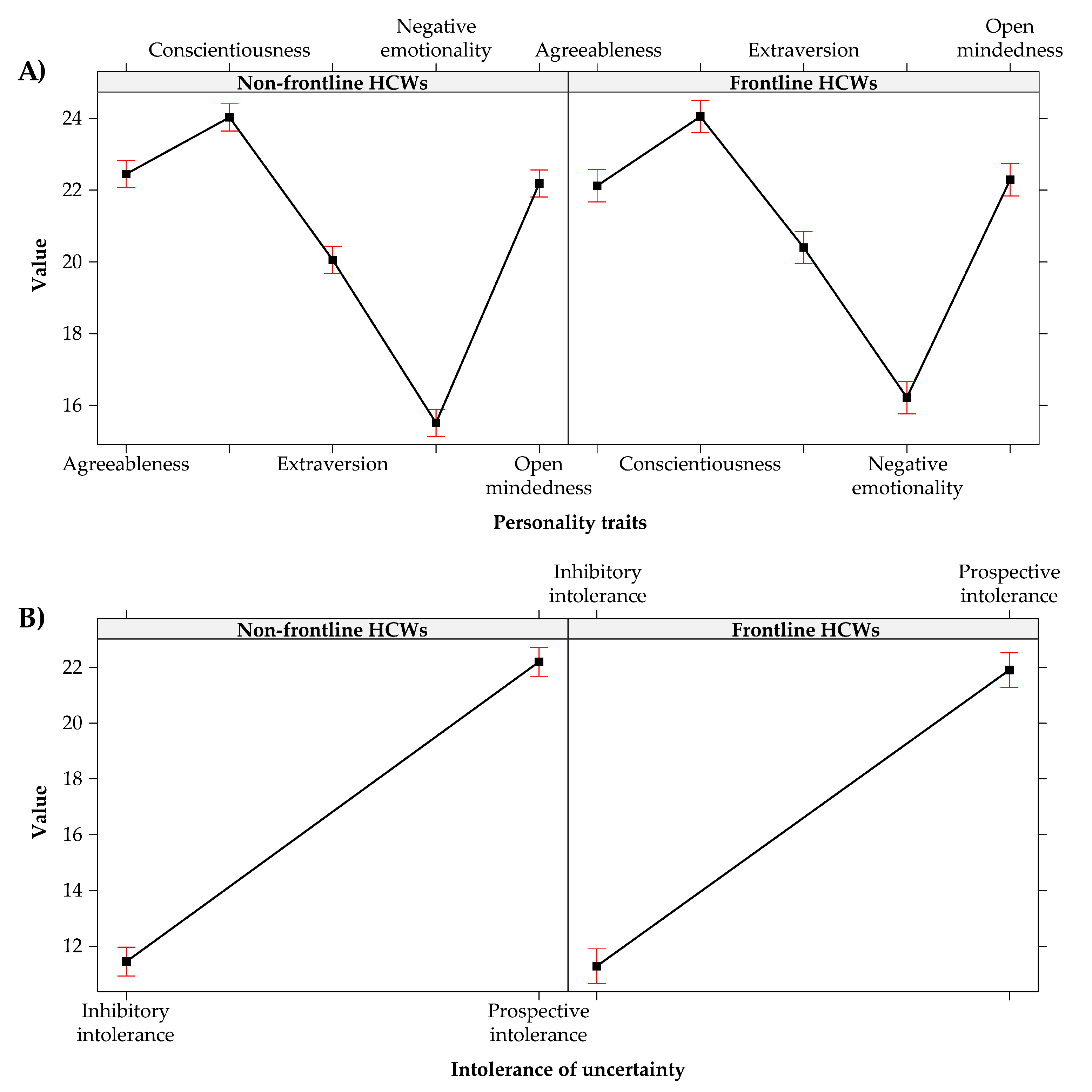
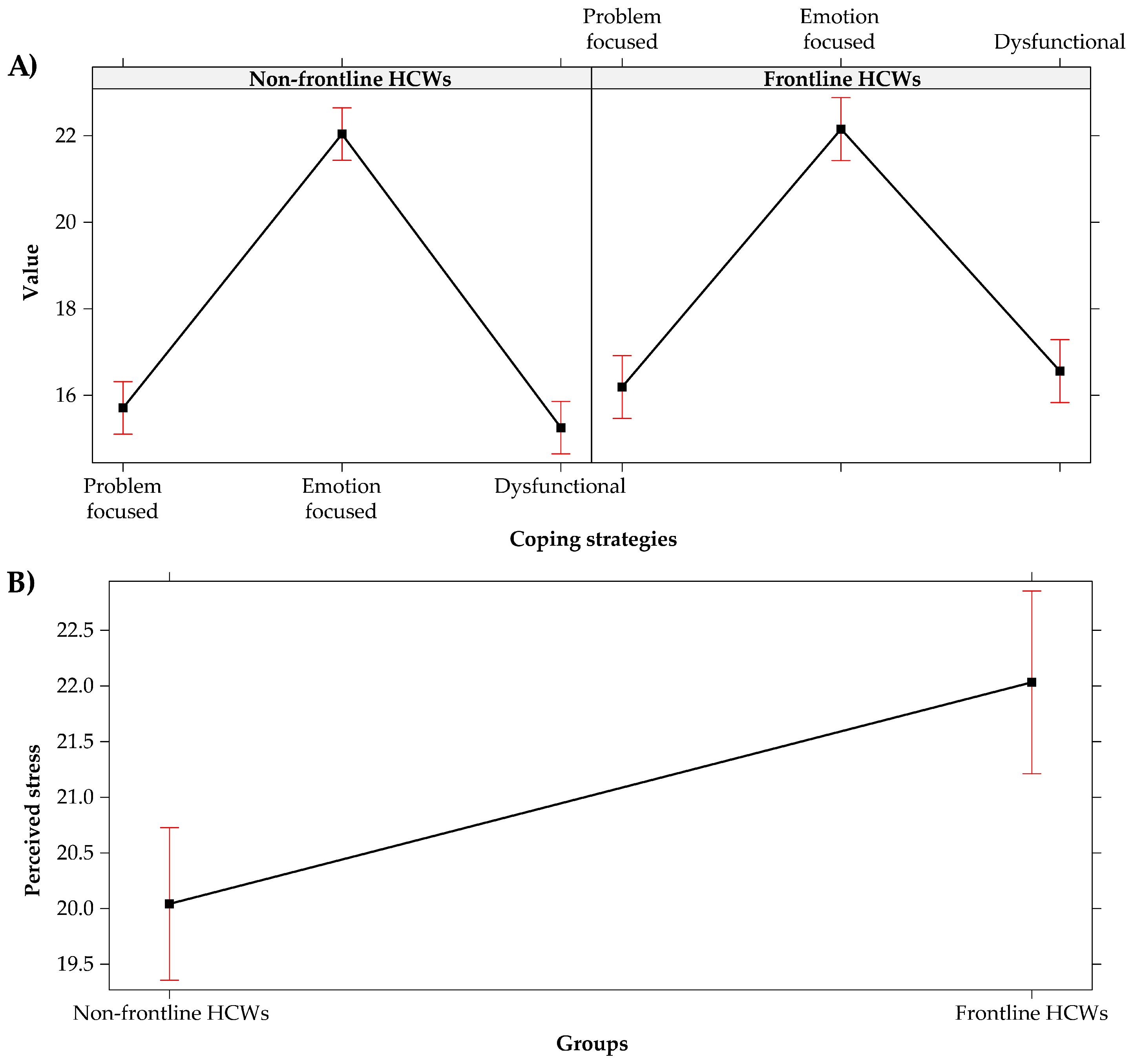
3.2. Analysis of Variance
- The conscientiousness (i.e., organization, productiveness, and responsibility) was the most prevalent personality trait;
- Levels of prospective intolerance of uncertainty were higher than the levels of inhibitory one;
- Emotion-focused coping strategies were more used than problem-focused and dysfunctional coping strategies.
3.3. Multi-Group Path-Analysis
- (a)
- Personality traits and Intolerance of uncertainty. While neuroticism was positively related to inhibitory and prospective intolerance of uncertainty (i.e., the more neuroticism the more intolerance of uncertainty both prospective and inhibitory) in both groups, other significant relations were found exclusively in the non-frontline HCWs. Specifically: conscientiousness was negatively related to prospective intolerance of uncertainty (i.e., the more conscientiousness, the less prospective intolerance of uncertainty. In other words, the more organized, productive, and responsible HCWs are, the less they are engaged in information-seeking to increase certainty), while agreeableness and open mindedness were negatively related to the inhibitory intolerance of uncertainty (i.e., the more agreeableness and open mindedness, the less inhibitory intolerance of uncertainty. In other words, the more confident, and intellectually creative and curious HCWs are, the less they seem to be paralyzed by uncertainty). These results seem to suggest that personality traits of frontline HCWs have a poor influence on levels of intolerance to uncertainty, except for the negative emotionality, which seems to act analogously in both HCWs’ groups.
- (b)
- Intolerance of uncertainty and Coping strategies. No significant relation was found in the frontline group of HCWs. Vice versa, in the non-frontline one, while prospective intolerance of uncertainty was positively related to problem and emotion focused coping strategies (i.e., the more prospective intolerance of uncertainty, the more problem and emotion focused coping strategies), inhibitory intolerance of uncertainty was negatively related both to problem and emotion-focused coping (i.e., the more inhibitory intolerance of uncertainty, the less problem and emotion focused coping strategies), and positively related to dysfunctional coping ones (i.e., the more inhibitory intolerance of uncertainty, the more dysfunctional coping strategies).
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, H.; Xia, Q.; Xiong, Z.; Li, Z.; Xiang, W.; Yuan, Y.; Liu, Y.; Li, Z. The psychological distress and coping styles in the early stages of the 2019 coronavirus disease (COVID-19) epidemic in the general mainland Chinese population: A web-based survey. PLoS ONE 2020, 15, e0233410. [Google Scholar] [CrossRef]
- Shi, L.; Lu, Z.A.; Que, J.Y.; Huang, X.L.; Liu, L.; Ran, M.S.; Gong, Y.M.; Yuan, K.; Yan, W.; Sun, Y.K.; et al. Prevalence of and risk factors associated with mental health symptoms among the general population in China during the coronavirus disease 2019 pandemic. JAMA Netw. Open 2020, 3, e2014053. [Google Scholar] [CrossRef] [PubMed]
- Moccia, L.; Janiri, D.; Pepe, M.; Dattoli, L.; Molinaro, M.; De Martin, V.; Chieffo, D.; Janiri, L.; Fiorillo, A.; Sani, G.; et al. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: An early report on the Italian general population. Brain Behav. Immun. 2020, 87, 75–79. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 pandemic and lockdown measures impact on mental health among the general population in Italy. Front. Psychiatry 2020, 11, 79. [Google Scholar] [CrossRef] [PubMed]
- Lanciano, T.; Graziano, G.; Curci, A.; Costadura, S.; Monaco, A. Risk perceptions and psychological effects during the italian COVID-19 emergency. Front. Psychiatry 2020, 11, 2434. [Google Scholar] [CrossRef] [PubMed]
- Cullen, W.; Gulati, G.; Kelly, B.D. Mental health in the Covid-19 pandemic. QJM 2020, 113, 311–312. [Google Scholar] [CrossRef]
- Luo, M.; Guo, L.; Yu, M.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.; Chen, J.H.; Xu, Y.F. Patients with mental health disorders in the COVID-19 epidemic. Lancet Psychiatry 2020, 7, e21. [Google Scholar] [CrossRef]
- Hao, F.; Tan, W.; Jiang, L.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; Jiang, X.; McIntyre, R.S.; et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav. Immun. 2020, 87, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Al-Quteimat, O.M.; Amer, A.M. The impact of the COVID-19 pandemic on cancer patients. Am. J. Clin. Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Romito, F.; Dellino, M.; Loseto, G.; Opinto, G.; Silvestris, E.; Cormio, C.; Guarini, A.; Minoia, C. Psychological Distress in Outpatients With Lymphoma During the COVID-19 Pandemic. Front. Oncol. 2020, 10, 1270. [Google Scholar] [CrossRef] [PubMed]
- Bargon, C.; Batenburg, M.; van Stam, L.; van der Molen, D.M.; van Dam, I.; van der Leij, F.; Baas, I.; Ernst, M.; Maarse, W.; Vermulst, N.; et al. The impact of the COVID-19 pandemic on quality of life, physical and psychosocial wellbeing in breast cancer patients—A prospective, multicenter cohort study. Eur. J. Cancer 2020, 138, S17. [Google Scholar] [CrossRef]
- Chan, C.; Oey, N.E.; Tan, E.K. Mental health of scientists in the time of COVID-19. Brain Behav. Immun. 2020, 88, 956. [Google Scholar] [CrossRef] [PubMed]
- Chong, M.Y.; Wang, W.C.; Hsieh, W.C.; Lee, C.Y.; Chiu, N.M.; Yeh, W.C.; Huang, T.L.; Wen, J.H.; Chen, C.L. Psychological impact of severe acute respiratory syndrome on health workers in a tertiary hospital. Br. J. Psychiatry 2004, 185, 127–133. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.M.; Wong, J.G.; McAlonan, G.M.; Cheung, V.; Cheung, C.; Sham, P.C.; Chu, C.M.; Wong, P.C.; Tsang, K.; Chua, S.E. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can. J. Psychiatry 2007, 52, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J.; et al. The psychological impact of the SARS epidemic on hospital employees in China: Exposure, risk perception, and altruistic acceptance of risk. Can. J. Psychiatry 2009, 54, 302–311. [Google Scholar] [CrossRef]
- Cabarkapa, S.; Nadjidai, S.E.; Murgier, J.; Ng, C.H. The psychological impact of COVID-19 and other viral epidemics on frontline healthcare workers and ways to address it: A rapid systematic review. Brain Behav. Immun. Health 2020, 100144. [Google Scholar] [CrossRef]
- Ahn, M.H.; Shin, Y.W.; Kim, J.H.; Kim, H.J.; Lee, K.U.; Chung, S. High Work-related Stress and Anxiety Response to COVID-19 among Healthcare Workers in South Korea. SAVE Study 2020. [Google Scholar] [CrossRef]
- Barello, S.; Palamenghi, L.; Graffigna, G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 2020, 290, 113129. [Google Scholar] [CrossRef] [PubMed]
- Ricci-Cabello, I.; Meneses-Echavez, J.F.; Serrano-Ripoll, M.J.; Fraile-Navarro, D.; Fiol-Roque, M.A.; Moreno, G.P.; Castro, A.; Ruiz-Pérez, I.; Campos, R.Z.; Gonçalves-Bradley, D. Impact of viral epidemic outbreaks on mental health of healthcare workers: A rapid systematic review and meta-analysis. J. Affect. Disord. 2020, 277, 347–357. [Google Scholar] [CrossRef]
- Du, J.; Dong, L.; Wang, T.; Yuan, C.; Fu, R.; Zhang, L.; Bo, L.; Zhang, M.; Yin, Y.; Qin, J.; et al. Psychological symptoms among frontline healthcare workers during COVID-19 outbreak in Wuhan. Gen. Hosp. Psychiatry 2020, 67, 144–145. [Google Scholar] [CrossRef]
- Giusti, E.M.; Pedroli, E.; D’Aniello, G.E.; Badiale, C.S.; Pietrabissa, G.; Manna, G.; Badiale, M.S.; Riva, G.; Castelnuovo, G.; Molinari, E. The psychological impact of the COVID-19 outbreak on health professionals: A cross-sectional study. Front. Psychol. 2020, 11, 1684. [Google Scholar] [CrossRef]
- Guo, J.; Liao, L.; Wang, B.; Li, X.; Guo, L.; Tong, Z.; Guan, Q.; Zhou, M.; Wu, Y.; Zhang, J.; et al. Psychological effects of COVID-19 on hospital staff: A national cross-sectional survey in mainland China. Vasc. Investig. Ther. 2021, 4, 6–11. Available online: https://www.vitonline.org/article.asp?issn=2589-9686;year=2021;volume=4;issue=1;spage=6;epage=11;aulast=Guo (accessed on 23 July 2021). [CrossRef]
- Ho, C.S.; Chee, C.; Ho, R. Mental health strategies to combat the psychological impact of coronavirus disease 2019 (COVID-19) beyond paranoia and panic. Ann. Acad. Med. Singap. 2020, 49, 1–6. Available online: http://www.anmm.org.mx/descargas/Ann-Acad-Med-Singapore.pdf (accessed on 18 August 2021). [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.C.; Arora, T.; Grey, I.; Suen, L.K.P.; Huang, E.Y.Z.; Li, D.; Lam, K.B.H. Perceived risk and protection from infection and depressive symptoms among healthcare workers in mainland China and Hong Kong during COVID-19. Front. Psychiatry 2020, 11, 686. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N.; Tripepi, G.; Di Prinzio, R.R. Symptoms in health care workers during the covid-19 epidemic. A cross-sectional survey. Int. J. Environ. Res. Public Health 2020, 17, 5218. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Preti, E.; Di Mattei, V.; Perego, G.; Ferrari, F.; Mazzetti, M.; Taranto, P.; Di Pierro, R.; Madeddu, F.; Calati, R. The psychological impact of epidemic and pandemic outbreaks on healthcare workers: Rapid review of the evidence. Curr. Psychiatry Rep. 2020, 22, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental health outcomes among frontline and second-line health care workers during the coronavirus disease 2019 (COVID-19) pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Ni, C.; Cai, W.; Hou, T.; Lian, B.; Chen, A.; Yin, Q.; Deng, G.; Li, H. Psychological Status of Health Care Workers during the Outbreak of Coronavirus Disease in China: A Cross-Sectional Study. 2020. Available online: https://europepmc.org/api/fulltextRepo?pprId=PPR121860&type=FILE&fileName=EMS99045-pdf.pdf&mimeType=application/pdf (accessed on 23 July 2021). [CrossRef] [Green Version]
- Spoorthy, M.S.; Pratapa, S.K.; Mahant, S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic–A review. Asian J. Psychiatry 2020, 51, 102119. [Google Scholar] [CrossRef]
- Talevi, D.; Socci, V.; Carai, M.; Carnaghi, G.; Faleri, S.; Trebbi, E.; Di Bernardo, A.; Capelli, F.; Pacitti, F. Mental health outcomes of the CoViD-19 pandemic. Riv. Psichiatry 2020, 55, 137–144. [Google Scholar] [CrossRef]
- Vagni, M.; Maiorano, T.; Giostra, V.; Pajardi, D. Hardiness, stress and secondary trauma in italian healthcare and emergency workers during the COVID-19 pandemic. Sustainability 2020, 12, 5592. [Google Scholar] [CrossRef]
- Zhang, W.R.; Wang, K.; Yin, L.; Zhao, W.F.; Xue, Q.; Peng, M.; Min, B.; Tian, Q.; Leng, H.; Du, J.; et al. Mental health and psychosocial problems of medical health workers during the COVID-19 epidemic in China. Psychother. Psychosom. 2020, 89, 242–250. [Google Scholar] [CrossRef]
- Zhu, Z.; Xu, S.; Wang, H.; Liu, Z.; Wu, J.; Li, G.; Miao, J.; Zhang, C.; Yang, Y.; Sun, W.; et al. COVID-19 in Wuhan: Sociodemographic characteristics and hospital support measures associated with the immediate psychological impact on healthcare workers. EClinicalMedicine 2020, 24, 100443. [Google Scholar] [CrossRef] [PubMed]
- Rapisarda, F.; Vallarino, M.; Cavallini, E.; Barbato, A.; Brousseau-Paradis, C.; De Benedictis, L.; Lesage, A. The early impact of the Covid-19 emergency on mental health workers: A survey in Lombardy, Italy. Int. J. Environ. Res. Public Health 2020, 17, 8615. [Google Scholar] [CrossRef] [PubMed]
- Marton, G.; Vergani, L.; Mazzocco, K.; Garassino, M.C.; Pravettoni, G. 2020s heroes are not fearless: The impact of the COVID-19 pandemic on wellbeing and emotions of italian health care workers during Italy Phase 1. Front. Psychol. 2020, 11, 2781. [Google Scholar] [CrossRef]
- Carmassi, C.; Foghi, C.; Dell’Oste, V.; Cordone, A.; Bertelloni, C.A.; Bui, E.; Dell’Osso, L. PTSD symptoms in Healthcare Workers facing the three Coronavirus outbreaks: What can we expect after the COVID-19 pandemic. Psychiatry Res. 2020, 292, 113312. [Google Scholar] [CrossRef]
- Yin, Q.; Sun, Z.; Liu, T.; Ni, X.; Deng, X.; Jia, D.; Shang, Z.; Zhou, Y.; Liu, W. Posttraumatic stress symptoms of health care workers during the corona virus disease 2019 (COVID-19). Clin. Psychol. Psychother. 2020, 27, 384–395. [Google Scholar] [CrossRef]
- Gupta, S.; Sahoo, S. Pandemic and mental health of the front-line healthcare workers: A review and implications in the Indian context amidst COVID-19. Gen. Psychiatry 2020, 33, e100284. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Cohen, J.B. Environmental Stress. In Human Behavior and Environment; Altman, I., Wohlwill, J.F., Eds.; Springer: Boston, MA, USA, 1977; pp. 89–127. [Google Scholar]
- Rutter, H.; Wolpert, M.; Greenhalgh, T. Managing uncertainty in the covid-19 era. BMJ 2020, 370. [Google Scholar] [CrossRef]
- Taylor, S. The Psychology of Pandemics: Preparing for the Next Global Outbreak of Infectious Disease; Cambridge Scholars Publishing: Newcastle, UK, 2019. [Google Scholar]
- Di Trani, M.; Mariani, R.; Ferri, R.; De Berardinis, D.; Frigo, M.G. From resilience to burnout in healthcare workers during the COVID-19 emergency: The role of the ability to tolerate uncertainty. Front. Psychol. 2021, 12, 987. [Google Scholar] [CrossRef]
- Carleton, R.N. The intolerance of uncertainty construct in the context of anxiety disorders: Theoretical and practical perspectives. Expert Rev. Neurother. 2012, 12, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Fergus, T.A. A comparison of three self-report measures of intolerance of uncertainty: An examination of structure and incremental explanatory power in a community sample. Psychol. Assesment 2013, 25, 1322–1331. [Google Scholar] [CrossRef]
- Fergus, T.A.; Bardeen, J.R. Anxiety sensitivity and intolerance of uncertainty: Evidence of incremental specificity in relation to health anxiety. Personal. Individ. Differ. 2013, 55, 640–644. [Google Scholar] [CrossRef]
- McEvoy, P.M.; Mahoney, A.E. Achieving certainty about the structure of intolerance of uncertainty in a treatment-seeking sample with anxiety and depression. J. Anxiety Disord. 2011, 25, 112–122. [Google Scholar] [CrossRef] [PubMed]
- McCann, S.J.H. Emotional health and the Big Five personality factors at the American state level. J. Happiness Stud. 2011, 12, 547–560. [Google Scholar] [CrossRef]
- Asmundson, G.J.; Taylor, S. Coronaphobia: Fear and the 2019-nCoV outbreak. J. Anxiety Disord. 2020, 70, 102196. [Google Scholar] [CrossRef] [PubMed]
- Bakioğlu, F.; Korkmaz, O.; Ercan, H. Fear of COVID-19 and positivity: Mediating role of intolerance of uncertainty, depression, anxiety, and stress. Int. J. Ment. Health Addict 2020, 28, 1–14. [Google Scholar] [CrossRef]
- Gica, S.; Kavakli, M.; Durduran, Y.; Ak, M. The Effect of COVID-19 Pandemic on psychosomatic complaints and investigation of the mediating role of intolerance to uncertainty, biological rhythm changes and perceived COVID-19 threat in this relationship: A web-based community survey. Psychiatry Clin. Psych. 2020, 30, 89–96. [Google Scholar] [CrossRef]
- Satici, B.; Saricali, M.; Satici, S.A.; Griffiths, M.D. Intolerance of uncertainty and mental wellbeing: Serial mediation by rumination and fear of COVID-19. Int. J. Ment. Health Addict 2020, 1–12. [Google Scholar] [CrossRef]
- Voitsidis, P.; Gliatas, I.; Bairachtari, V.; Papadopoulou, K.; Papageorgiou, G.; Parlapani, E.; Syngelakis, M.; Holeva, V.; Diakogiannis, I. Insomnia during the COVID-19 pandemic in a Greek population. Psychiatry Res. 2020, 289, 113076. [Google Scholar] [CrossRef]
- Aksoy, Y.E.; Koçak, V. Psychological effects of nurses and midwives due to COVID-19 outbreak: The case of Turkey. Arch. Psychiatry Nurs. 2020, 34, 427–433. [Google Scholar] [CrossRef] [PubMed]
- McKay, D.; Minaya, C.; Storch, E.A. Conducting exposure and response prevention treatment for contamination fears during COVID-19: The behavioral immune system impact on clinician approaches to treatment. J. Anxiety Disord. 2020, 74, 102270. [Google Scholar] [CrossRef]
- Tull, M.T.; Barbano, A.C.; Scamaldo, K.M.; Richmond, J.R.; Edmonds, K.A.; Rose, J.P.; Gratz, K.L. The prospective influence of COVID-19 affective risk assessments and intolerance of uncertainty on later dimensions of health anxiety. J. Anxiety Disord. 2020, 75, 102290. [Google Scholar] [CrossRef]
- McEvoy, P.M.; Mahoney, A.E. Intolerance of uncertainty and negative metacognitive beliefs as transdiagnostic mediators of repetitive negative thinking in a clinical sample with anxiety disorders. J. Anxiety Disord. 2013, 27, 216–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: New York, NY, USA, 1984. [Google Scholar]
- Lazarus, R.S. Psychological Stress and the Coping Process; McGraw-Hill: New York, NY, USA, 1996. [Google Scholar]
- Monzani, D.; Steca, P.; Greco, A.; D’Addario, M.; Cappelletti, E.; Pancani, L. The situational version of the Brief COPE: Dimensionality and relationships with goal-related variables. Eur. J. Psychol. 2015, 11, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Mache, S. Coping with job stress by hospital doctors: A comparative study. Wiener Medizinische Wochenschrift 2012, 162, 440–447. [Google Scholar] [CrossRef]
- Folkman, S.; Lazarus, R.S. An analysis of coping in a middle-aged community sample. J. Health Soc. Behav. 1980, 21, 219–239. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Personal. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef]
- Carver, C.S. You want to measure coping but your protocol’s too long: Consider the brief cope. Int. J. Behav. Med. 1997, 4, 92. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S.; Scheier, M.F. On the Self-Regulation of Behavior; Cambridge University Press: New York, NY, USA, 1998. [Google Scholar]
- Meyer, B. Coping with severe mental illness: Relations of the Brief COPE with symptoms, functioning, and well-being. J. Psychopathol. Behav. 2001, 23, 265–277. [Google Scholar] [CrossRef]
- Connor-Smith, J.K.; Flachsbart, C. Relations between personality and coping: A meta-analysis. J. Personal. Soc. Psychol. 2007, 93, 1080–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leandro, P.G.; Castillo, M.D. Coping with stress and its relationship with personality dimensions, anxiety, and depression. Procedia Soc. Behav. Sci. 2010, 5, 1562–1573. [Google Scholar] [CrossRef] [Green Version]
- Afshar, H.; Roohafza, H.R.; Keshteli, A.H.; Mazaheri, M.; Feizi, A.; Adibi, P. The association of personality traits and coping styles according to stress level. J. Res. Med. Sci. 2015, 20, 353–358. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4468450/ (accessed on 22 August 2021). [PubMed]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmund, G. COVID stress syndrome: Concept, structure, and correlates. Depress. Anxiety 2020, 37, 706–714. [Google Scholar] [CrossRef]
- Munawar, K.; Choudhry, F.R. Exploring stress coping strategies of frontline emergency health workers dealing covid-19 in Pakistan: A qualitative inquiry. Am. J. Infect. Control 2020. Available online: https://www.ajicjournal.org/article/S0196-6553(20)30638-6/fulltext#seccesectitle0001 (accessed on 27 July 2021). [CrossRef]
- Salman, M.; Raza, M.H.; Mustafa, Z.U.; Khan, T.M.; Asif, N.; Tahir, H.; Shehzadi, N.; Hussain, K. The psychological effects of COVID-19 on frontline healthcare workers and how they are coping: A web-based, cross-sectional study from Pakistan. medRxiv 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.06.03.20119867v1 (accessed on 18 August 2021). [CrossRef]
- Huang, L.; Lei, W.; Xu, F.; Liu, H.; Yu, L. Emotional responses and coping strategies in nurses and nursing students during Covid-19 outbreak: A comparative study. PLoS ONE 2020, 15, e0237303. [Google Scholar] [CrossRef]
- Taha, S.; Matheson, K.; Cronin, T.; Anisman, H. Intolerance of uncertainty, appraisals, coping, and anxiety: The case of the 2009 H 1 N 1 pandemic. Br. J. Health Psych. 2014, 19, 592–605. [Google Scholar] [CrossRef]
- Rettie, H.; Daniels, J. Coping and tolerance of uncertainty: Predictors and mediators of mental health during the COVID-19 pandemic. Am. Psychol. 2020, 76, 427–437. [Google Scholar] [CrossRef]
- Sica, C.; Latzman, R.D.; Caudek, C.; Cerea, S.; Colpizzi, I.; Caruso, M.; Giulini, P.; Bottesi, G. Facing distress in Coronavirus era: The role of maladaptive personality traits and coping strategies. Personal. Individ. Differ. 2021, 177, 110833. [Google Scholar] [CrossRef]
- Liu, S.; Lithopoulos, A.; Zhang, C.Q.; Garcia-Barrera, M.A.; Rhodes, R.E. Personality and perceived stress during COVID-19 pandemic: Testing the mediating role of perceived threat and efficacy. Personal. Individ. Differ. 2021, 168, 110351. [Google Scholar] [CrossRef] [PubMed]
- Soto, C.J.; John, O.P. Short and extra-short forms of the Big Five Inventory–2: The BFI-2-S and BFI-2-XS. J. Res. Personal. 2017, 68, 69–81. [Google Scholar] [CrossRef]
- Soto, C.J.; John, O.P. The next big five inventory (BFI-2): Developing and assessing a hierarchical model with 15 facets to enhance bandwidth, fidelity, and predictive power. J. Personal. Soc. Psychol. 2017, 113, 117–143. [Google Scholar] [CrossRef]
- Goldberg, L.R. The structure of phenotypic personality traits. Am. Psychol. 1993, 48, 26–34. [Google Scholar] [CrossRef]
- John, O.P.; Naumann, L.P.; Soto, C.J. Paradigm shift to the integrative Big—Five trait taxonomy: History, measurement, and conceptual issues. In Handbook of Personality: Theory and Research, 3rd ed.; John, O.P., Robins, R.W., Pervin, L.A., Eds.; Guilford: New York, NY, USA, 2008; pp. 114–158. [Google Scholar]
- McCrae, R.R.; Costa, P.T. The Five-Factor theory of personality. In Handbook of Personality: Theory and Research, 3rd ed.; John, O.P., Robins, R.W., Pervin, L.A., Eds.; Guilford: New York, NY, USA, 2008; pp. 159–181. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation modeling, 4th ed.; Guilford: New York, NY, USA, 2016. [Google Scholar]
- Bottesi, G.; Ghisi, M.; Novara, C.; Bertocchi, J.; Boido, M.; De Dominicis, I. Intolerance of uncertainty scale (IUS-27 e IUS-12): Due studi preliminari. Psicoterapia Cognitiva e Comportamentale 2015, 21, 345–365. Available online: https://www.researchgate.net/profile/Mark-Freeston/publication/281899656_Intolerance_of_Uncertainty_Scale_IUS-27_and_IUS-12_Two_preliminary_studies/links/584683ba08ae61f75ddb7faa/Intolerance-of-Uncertainty-Scale-IUS-27-and-IUS-12-Two-preliminary-studies.pdf (accessed on 22 August 2021).
- Carleton, R.N.; Norton, P.J.; Asmundson, G.J.G. Fearing the unknown: A short version of the Intolerance of Uncertainty Scale. J. Anxiety Disord. 2007, 21, 105–117. [Google Scholar] [CrossRef]
- Freeston, M.H.; Rhéaume, J.; Letarte, H.; Dugas, M.J.; Ladouceur, R. Why do people worry? Personal. Individ. Differ. 1994, 17, 791–802. [Google Scholar] [CrossRef]
- Lauriola, M.; Mosca, O.; Carleton, R.N. Hierarchical factor structure of the intolerance of uncertainty scale short form (IUS-12) in the Italian version. Test. Psychom. Methodol. Appl. Psychol. 2016, 23, 377–394. [Google Scholar] [CrossRef]
- Eisenberg, S.A.; Shen, B.J.; Schwarz, E.R.; Mallon, S. Avoidant coping moderates the association between anxiety and patient-rated physical functioning in heart failure patients. J. Behav. Med. 2012, 35, 253–261. [Google Scholar] [CrossRef]
- Fossati, A. Scala per lo Stress Percepito. Available online: https://www.futuremedicalinnovation.it//wp-content/uploads/2017/10/ps_questionario_stress.pdf (accessed on 18 August 2021).
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health. Soc. Behav. 1983, 24, 386–396. [Google Scholar] [CrossRef]
- Cohen, S.; Williamson, G. Perceived stress in a probability sample of the United States. In The Social Psychology of Health; Spacapan, S., Oskamp, S., Eds.; Sage: Newbury Park, CA, USA, 1988; pp. 31–67. [Google Scholar]
- Mondo, M.; Sechi, C.; Cabras, C. Psychometric evaluation of three versions of the Italian perceived stress scale. Curr. Psychol. 2019, 40, 1–9. [Google Scholar] [CrossRef]
- Cohen, S. Perceives Stress Scale. Available online: https://www.northottawawellnessfoundation.org/wp-content/uploads/2018/04/PerceivedStressScale.pdf (accessed on 22 August 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 18 August 2021).
- Rosseel, Y. Lavaan: An R Package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Usher, K.; Durkin, J.; Bhullar, N. The COVID-19 pandemic and mental health impacts. Int. J. Ment. Health Nurs. 2020, 29, 315–318. [Google Scholar] [CrossRef] [Green Version]
- Tam, C.W.; Pang, E.P.; Lam, L.C.; Chiu, H.F. Severe acute respiratory syndrome (SARS) in Hong Kong in 2003: Stress and psychological impact among frontline healthcare workers. Psychol. Med. 2004, 34, 1197–1204. [Google Scholar] [CrossRef]
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L.; et al. Psychological adjustment of healthcare workers in Italy during the COVID-19 pandemic: Differences in stress, anxiety, depression, burnout, secondary trauma, and compassion satisfaction between frontline and non-frontline professionals. Int. J. Environ. Res. Public Health 2020, 17, 8358. [Google Scholar] [CrossRef]
- Babore, A.; Lombardi, L.; Viceconti, M.L.; Pignataro, S.; Marino, V.; Crudele, M.; Candelori, C.; Bramanti, S.M.; Trumello, C. Psychological effects of the COVID-2019 pandemic: Perceived stress and coping strategies among healthcare professionals. Psychiatry Res. 2020, 293, 113366. [Google Scholar] [CrossRef]
- McEvoy, P.M.; Mahoney, A.E. To be sure, to be sure: Intolerance of uncertainty mediates symptoms of various anxiety disorders and depression. Behav. Ther. 2012, 43, 533–545. [Google Scholar] [CrossRef]
- Hawes, M.T.; Farrell, M.R.; Cannone, J.L.; Finsaas, M.C.; Olino, T.M.; Klein, N. Early childhood temperament predicts intolerance of uncertainty in adolescence. J. Anxiety Disord. 2021, 80, 102390. [Google Scholar] [CrossRef]
- Taylor, S.; Fong, A.; Asmundson, G.J. Predicting the severity of symptoms of the COVID stress syndrome from personality traits: A prospective network analysis. Front. Psychol. 2021, 12, 1582. [Google Scholar] [CrossRef]
- Ruckmani, V.S. Psychological perspective of uncertainty. In The Opportunities of Uncertainties: Flexibility and Adaptation Needed in Current Climate; Shahana, A.M., Sivakumar, A., Parthiban, V., Eds.; Lulu Publication: Raleigh, NC, USA, 2021; Volume 1, pp. 1–9. [Google Scholar]
- Fluharty, M.; Bu, F.; Steptoe, A.; Fancourt, D. Coping strategies and mental health trajectories during the first 21 weeks of COVID-19 lockdown in the United Kingdom. Soc. Sci. Med. 2021, 279, 113958. [Google Scholar] [CrossRef] [PubMed]
- Folkman, S.; Lazarus, R.S.; Gruen, R.J.; DeLongis, A. Appraisal, coping, health status, and psychological symptoms. J. Personal. Soc. Psychol. 1986, 50, 571. [Google Scholar] [CrossRef]
- Lambert, V.; Lambert, C.; Ito, M. Workplace stressors, ways of coping and demographic characteristics as predictors of physical and mental health of Japanese hospital nurses. Int. J. Nurs. Stud. 2004, 41, 85–97. [Google Scholar] [CrossRef]
- Laranjeira, C.A. The effects of perceived stress and ways of coping in a sample of Portuguese health workers. J. Clin. Nurs. 2012, 21, 1755–1762. [Google Scholar] [CrossRef]
- Besirli, A.; Erden, S.C.; Atilgan, M.; Varlihan, A.; Habaci, M.F.; Yeniceri, T.; Isler, A.C.; Gumus, M.; Kizilerogu, S.; Ozturk, G.; et al. The Relationship between Anxiety and Depression Levels with Perceived Stress and Coping Strategies in Health Care Workers during the COVID-19 Pandemic. Sisli. Etfal. Hastan. Tıp. Bul. 2021, 55, 1. [Google Scholar] [CrossRef]
- Canestrari, C.; Bongelli, R.; Fermani, A.; Riccioni, I.; Bertolazzi, A.; Muzi, M.; Burro, R. Coronavirus disease stress among italian healthcare workers: The role of coping humor. Front. Psychol. 2021, 11, 3962. [Google Scholar] [CrossRef]
- Vagni, M.; Maiorano, T.; Giostra, V.; Pajardi, D. Coping with COVID-19: Emergency stress, secondary trauma and self-efficacy in healthcare and emergency workers in Italy. Front. Psychol. 2020, 11, 566912. [Google Scholar] [CrossRef] [PubMed]
- Maiorano, T.; Vagni, M.; Giostra, V.; Pajardi, D. COVID-19: Risk factors and protective role of resilience and coping strategies for emergency stress and secondary trauma in medical staff and emergency workers—An online-based inquiry. Sustainability 2020, 12, 9004. [Google Scholar] [CrossRef]
- Vagni, M.; Maiorano, T.; Giostra, V.; Pajardi, D. Protective factors against emergency stress and burnout in healthcare and emergency workers during second wave of COVID-19. Soc. Sci. 2021, 10, 178. [Google Scholar] [CrossRef]
- Kahneman, D.; Slovic, S.P.; Slovic, P.; Tversky, A. (Eds.) Judgment Under Uncertainty: Heuristics and Biases; Cambridge University Press: Cambridge, UK, 1982. [Google Scholar]
- Gigerenzer, G.; Gaissmaier, W. Heuristic decision making. Annu. Rev. Psychol. 2011, 62, 451–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) |
|---|---|
| Total | 682 (100.00%) |
| Socio-demographic characteristics | |
| Gender | |
| Female | 530 (77.71%) |
| Male | 152 (22.29%) |
| Age | |
| 18–30 | 128 (18.77%) |
| 31–40 | 131 (19.21%) |
| 41–50 | 182 (26.69%) |
| 51–60 | 193 (28.30%) |
| >60 | 48 (7.04%) |
| Marital status | |
| Married | 307 (45.01%) |
| Unmarried | 188 (27.57%) |
| Domestic partner | 107 (15.69%) |
| Divorced/separated | 67 (9.82%) |
| Widower/widow | 13 (1.91%) |
| Children | |
| Yes | 395 (57.92%) |
| No | 287 (42.08%) |
| Religion | |
| Believer occasionally practitioner | 262 (38.42%) |
| Believer non-practitioner | 162 (23.75%) |
| Non-Believer | 113 (16.57%) |
| Believer practitioner | 108 (15.84%) |
| Prefer not to answer | 37 (5.43%) |
| Job characteristics | |
| Place of work | |
| North Italy | 479 (70.23%) |
| Centre Italy | 128 (18.77%) |
| South Italy | 75 (11.00 %) |
| Job position | |
| Nurse | 518 (75.95%) |
| Physician | 164 (24.05%) |
| Job area | |
| Medical specialties | 353 (51.76%) |
| Diagnostic and therapeutic specialties | 144 (21.11%) |
| Surgical specialties | 106 (15.54%) |
| Primary care nurse. serv. | 79 (11.58%) |
| Seniority | |
| More than 20 years | 325 (47.65%) |
| Less than 5 years | 150 (21.99%) |
| 10–20 years | 121 (17.74%) |
| 5–10 years | 86 (12.61%) |
| Job exposure to COVID-19 | |
| Wards | |
| Worked in COVID-19-dedicated wards | 280 (41.06%) |
| Worked in other wards | 402 (58.94%) |
| Swabs for COVID-19 | |
| Done | 392 (57.48%) |
| Not done | 290 (42.52%) |
| COVID-19 contracted | |
| No | 534 (78.30%) |
| Perhaps | 91 (13.34%) |
| Yes | 57 (8.36%) |
| Model | Df | Chi-sq | Chi-sq Difference | Df Difference | p-Value | CFI Difference | TLI Difference | RMSEA Difference | SRMR Difference |
|---|---|---|---|---|---|---|---|---|---|
| Unconstrained | 44 | 131.810 | - | - | - | - | - | - | - |
| Constrained | 70 | 177.990 | 46.180 | 26 | 0.008 ** | 0.009 | −0.019 | 0.009 | −0.008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bongelli, R.; Canestrari, C.; Fermani, A.; Muzi, M.; Riccioni, I.; Bertolazzi, A.; Burro, R. Associations between Personality Traits, Intolerance of Uncertainty, Coping Strategies, and Stress in Italian Frontline and Non-Frontline HCWs during the COVID-19 Pandemic—A Multi-Group Path-Analysis. Healthcare 2021, 9, 1086. https://doi.org/10.3390/healthcare9081086
Bongelli R, Canestrari C, Fermani A, Muzi M, Riccioni I, Bertolazzi A, Burro R. Associations between Personality Traits, Intolerance of Uncertainty, Coping Strategies, and Stress in Italian Frontline and Non-Frontline HCWs during the COVID-19 Pandemic—A Multi-Group Path-Analysis. Healthcare. 2021; 9(8):1086. https://doi.org/10.3390/healthcare9081086
Chicago/Turabian StyleBongelli, Ramona, Carla Canestrari, Alessandra Fermani, Morena Muzi, Ilaria Riccioni, Alessia Bertolazzi, and Roberto Burro. 2021. "Associations between Personality Traits, Intolerance of Uncertainty, Coping Strategies, and Stress in Italian Frontline and Non-Frontline HCWs during the COVID-19 Pandemic—A Multi-Group Path-Analysis" Healthcare 9, no. 8: 1086. https://doi.org/10.3390/healthcare9081086