
Benefits of VR Physical Exercise on Cognition in Older Adults with and without Mild Cognitive Decline: A Systematic Review of Randomized Controlled Trials

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Quality Assessment
3. Results
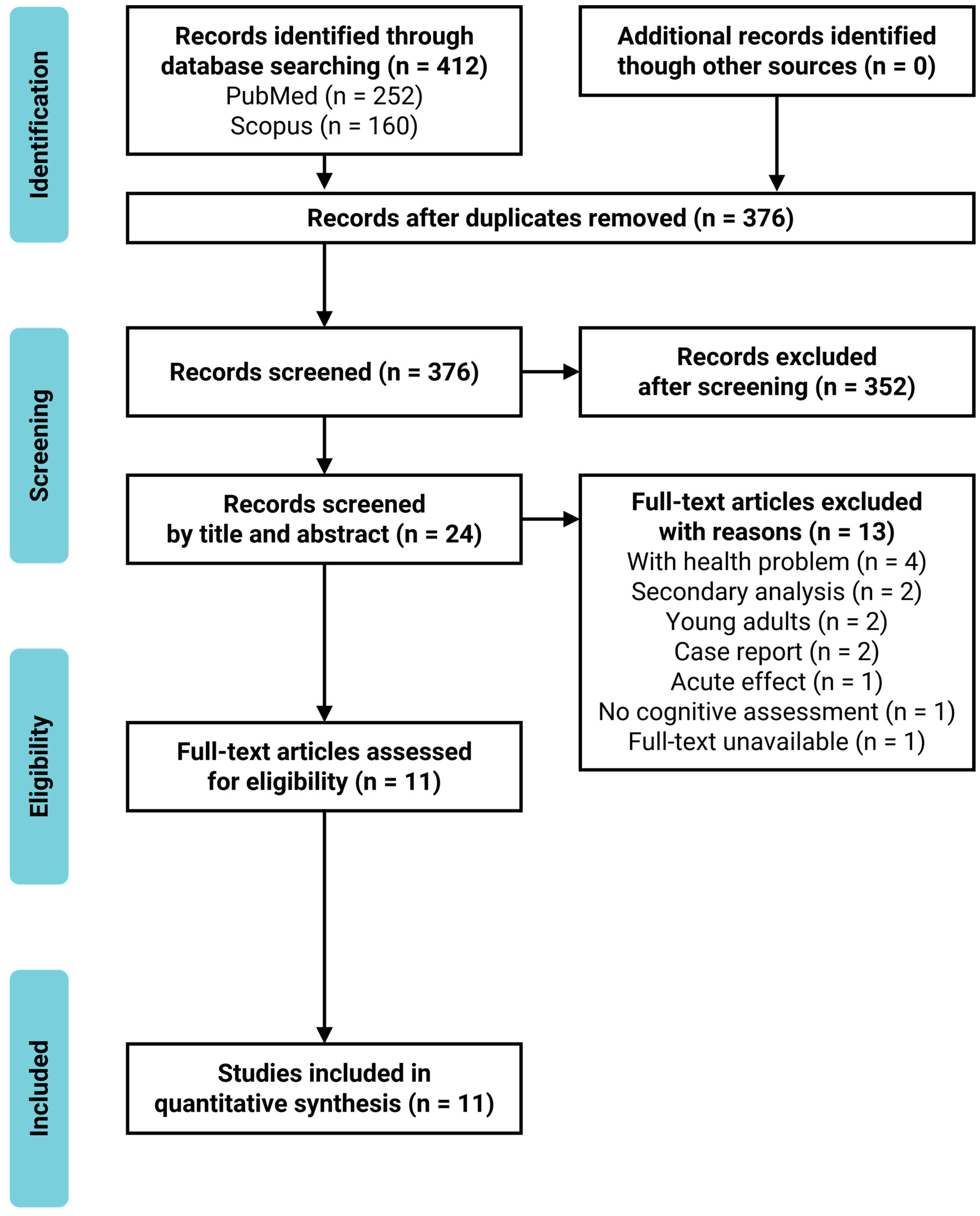
3.1. Study Selection and Characteristics
3.2. Quality Assessment
3.3. Intervention
3.4. Outcome
3.4.1. General Cognitive Functions
3.4.2. Executive Function
3.4.3. Working Memory Capacity and Short-Term Memory
3.4.4. Episodic (Long-Term) Memory
3.4.5. Processing Speed
3.4.6. Attention
3.4.7. Others
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilson, R.S.; Wang, T.; Yu, L.; Bennett, D.A.; Boyle, P.A. Normative Cognitive Decline in Old Age. Ann. Neurol. 2020, 87, 816–829. [Google Scholar] [CrossRef]
- Yagi, A.; Nouchi, R.; Murayama, K.; Sakaki, M.; Kawashima, R. The Role of Cognitive Control in Age-Related Changes in Well-Being. Front. Aging Neurosci. 2020, 12, 198. [Google Scholar] [CrossRef]
- Jongstra, S.; van Gool, W.A.; Moll van Charante, E.P.; van Dalen, J.W.; Eurelings, L.S.M.; Richard, E.; Ligthart, S.A. Improving Prediction of Dementia in Primary Care. Ann. Fam. Med. 2018, 16, 206–210. [Google Scholar] [CrossRef] [Green Version]
- Xie, H.; Mayo, N.; Koski, L. Predictors of future cognitive decline in persons with mild cognitive impairment. Dement. Geriatr. Cogn. Disord. 2011, 32, 308–317. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Guure, C.B.; Ibrahim, N.A.; Adam, M.B.; Said, S.M. Impact of Physical Activity on Cognitive Decline, Dementia, and Its Subtypes: Meta-Analysis of Prospective Studies. Biomed. Res. Int. 2017, 2017, 9016924. [Google Scholar] [CrossRef]
- Larson, E.B.; Wang, L.; Bowen, J.D.; McCormick, W.C.; Teri, L.; Crane, P.; Kukull, W. Exercise is associated with reduced risk for incident dementia among persons 65 years of age and older. Ann. Intern. Med. 2006, 144, 73–81. [Google Scholar] [CrossRef]
- Hsu, C.L.; Best, J.R.; Davis, J.C.; Nagamatsu, L.S.; Wang, S.; Boyd, L.A.; Hsiung, G.R.; Voss, M.W.; Eng, J.J.; Liu-Ambrose, T. Aerobic exercise promotes executive functions and impacts functional neural activity among older adults with vascular cognitive impairment. Br. J. Sports Med. 2018, 52, 184–191. [Google Scholar] [CrossRef]
- Formenti, D.; Cavaggioni, L.; Duca, M.; Trecroci, A.; Rapelli, M.; Alberti, G.; Komar, J.; Iodice, P. Acute Effect of Exercise on Cognitive Performance in Middle-Aged Adults: Aerobic Versus Balance. J. Phys. Act. Health 2020, 1–8. [Google Scholar] [CrossRef]
- Nouchi, R.; Taki, Y.; Takeuchi, H.; Sekiguchi, A.; Hashizume, H.; Nozawa, T.; Nouchi, H.; Kawashima, R. Four weeks of combination exercise training improved executive functions, episodic memory, and processing speed in healthy elderly people: Evidence from a randomized controlled trial. Age 2014, 36, 787–799. [Google Scholar] [CrossRef] [Green Version]
- Nouchi, R.; Nouchi, H.; Kawashima, R. A Single 30 Minutes Bout of Combination Physical Exercises Improved Inhibition and Vigor-Mood in Middle-Aged and Older Females: Evidence From a Randomized Controlled Trial. Front. Aging Neurosci. 2020, 12, 179. [Google Scholar] [CrossRef]
- Voelcker-Rehage, C.; Godde, B.; Staudinger, U.M. Cardiovascular and Coordination Training Differentially Improve Cognitive Performance and Neural Processing in Older Adults. Front. Hum. Neurosci. 2011, 5, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef] [Green Version]
- Justine, M.; Azizan, A.; Hassan, V.; Salleh, Z.; Manaf, H. Barriers to participation in physical activity and exercise among middle-aged and elderly individuals. Singap. Med. J. 2013, 54, 581–586. [Google Scholar] [CrossRef]
- De Bruin, P.D.E.; Schoene, D.; Pichierri, G.; Smith, S. Use of virtual reality technique for the training of motor control in the elderly. Z. Gerontol. Geriatr. 2010, 43, 229–234. [Google Scholar] [CrossRef]
- Anderson-Hanley, C.; Arciero, P.J.; Brickman, A.M.; Nimon, J.P.; Okuma, N.; Westen, S.C.; Merz, M.E.; Pence, B.D.; Woods, J.A.; Kramer, A.F.; et al. Exergaming and older adult cognition: A cluster randomized clinical trial. Am. J. Prev. Med. 2012, 42, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Barcelos, N.M.; Zimmerman, E.A.; Gillen, R.W.; Dunnam, M.; Cohen, B.D.; Yerokhin, V.; Miller, K.E.; Hayes, D.J.; Arciero, P.J.; et al. The Aerobic and Cognitive Exercise Study (ACES) for Community-Dwelling Older Adults With or At-Risk for Mild Cognitive Impairment (MCI): Neuropsychological, Neurobiological and Neuroimaging Outcomes of a Randomized Clinical Trial. Front. Aging Neurosci. 2018, 10, 76. [Google Scholar] [CrossRef] [PubMed]
- Bacha, J.M.R.; Gomes, G.C.V.; de Freitas, T.B.; Viveiro, L.A.P.; da Silva, K.G.; Bueno, G.C.; Varise, E.M.; Torriani-Pasin, C.; Alonso, A.C.; Luna, N.M.S.; et al. Effects of Kinect Adventures Games Versus Conventional Physical Therapy on Postural Control in Elderly People: A Randomized Controlled Trial. Games Health J. 2018, 7, 24–36. [Google Scholar] [CrossRef]
- Delbroek, T.; Vermeylen, W.; Spildooren, J. The effect of cognitive-motor dual task training with the biorescue force platform on cognition, balance and dual task performance in institutionalized older adults: A randomized controlled trial. J. Phys. Ther. Sci. 2017, 29, 1137–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggenberger, P.; Schumacher, V.; Angst, M.; Theill, N.; de Bruin, E.D. Does multicomponent physical exercise with simultaneous cognitive training boost cognitive performance in older adults? A 6-month randomized controlled trial with a 1-year follow-up. Clin. Interv. Aging 2015, 10, 1335–1349. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, C.-C.; Lin, P.-S.; Hsu, W.-C.; Wang, J.-S.; Huang, Y.-C.; Lim, A.Y.; Hsu, Y.-C. The Effectiveness of a Virtual Reality-Based Tai Chi Exercise on Cognitive and Physical Function in Older Adults with Cognitive Impairment. Dement. Geriatr. Cogn. Disord. 2018, 46, 358–370. [Google Scholar] [CrossRef]
- Htut, T.Z.C.; Hiengkaew, V.; Jalayondeja, C.; Vongsirinavarat, M. Effects of physical, virtual reality-based, and brain exercise on physical, cognition, and preference in older persons: A randomized controlled trial. Eur. Rev. Aging Phys. Act. 2018, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mrakic-Sposta, S.; Di Santo, S.G.; Franchini, F.; Arlati, S.; Zangiacomi, A.; Greci, L.; Moretti, S.; Jesuthasan, N.; Marzorati, M.; Rizzo, G.; et al. Effects of Combined Physical and Cognitive Virtual Reality-Based Training on Cognitive Impairment and Oxidative Stress in MCI Patients: A Pilot Study. Front. Aging Neurosci. 2018, 10, 282. [Google Scholar] [CrossRef] [Green Version]
- Liao, Y.-Y.; Tseng, H.-Y.; Lin, Y.-J.; Wang, C.-J.; Hsu, W.-C. Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment. Eur. J. Phys. Rehabil. Med. 2020, 56, 47–57. [Google Scholar] [CrossRef]
- Monteiro-Junior, R.S.; Figueiredo, L.; Maciel-Pinheiro, P.T.; Abud, E.L.R.; Engedal, K.; Barca, M.L.; Nascimento, O.J.M.; Laks, J.; Deslandes, A.C. Virtual Reality-Based Physical Exercise With Exergames (PhysEx) Improves Mental and Physical Health of Institutionalized Older Adults. J. Am. Med. Dir. Assoc. 2017, 18, 454.e1–454.e9. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Yim, J. A New Approach to Improve Cognition, Muscle Strength, and Postural Balance in Community-Dwelling Elderly with a 3-D Virtual Reality Kayak Program. Tohoku J. Exp. Med. 2016, 238, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Holden, M.K.; Todorov, E. Use of virtual environments in motor learning and rehabilitation. In Handbook of Virtual Environments: Design, Implementation, and Applications; CRC Press: Boca Raton, FL, USA, 2002; pp. 999–1026. [Google Scholar]
- Van Schaik, P.; Blake, J.; Pernet, F.; Spears, I.; Fencott, C. Virtual Augmented Exercise Gaming for Older Adults. Cyber Psychol. Behav. 2008, 11, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Nouchi, R.; Hu, Q.; Saito, T.; Kawata, N.; Nouchi, H.; Kawashima, R. Brain Training and Sulforaphane Intake Interventions Separately Improve Cognitive Performance in Healthy Older Adults, Whereas a Combination of These Interventions Does Not Have More Beneficial Effects: Evidence from a Randomized Controlled Trial. Nutrients 2021, 13, 352. [Google Scholar] [CrossRef]
- Nouchi, R.; Kobayashi, A.; Nouchi, H.; Kawashima, R. Newly Developed TV-Based Cognitive Training Games Improve Car Driving Skills, Cognitive Functions, and Mood in Healthy Older Adults: Evidence From a Randomized Controlled Trial. Front. Aging Neurosci. 2019, 11, 99. [Google Scholar] [CrossRef] [Green Version]
- Nouchi, R.; Saito, T.; Nouchi, H.; Kawashima, R. Small Acute Benefits of 4 Weeks Processing Speed Training Games on Processing Speed and Inhibition Performance and Depressive Mood in the Healthy Elderly People: Evidence from a Randomized Control Trial. Front. Aging Neurosci. 2016, 8, 302. [Google Scholar] [CrossRef]
- Nouchi, R.; Taki, Y.; Takeuchi, H.; Hashizume, H.; Akitsuki, Y.; Shigemune, Y.; Sekiguchi, A.; Kotozaki, Y.; Tsukiura, T.; Yomogida, Y.; et al. Brain training game improves executive functions and processing speed in the elderly: A randomized controlled trial. PLoS ONE 2012, 7, e29676. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verhagen, A.P.; de Vet, H.C.; de Bie, R.A.; Kessels, A.G.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi list: A criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef] [Green Version]
- Nouchi, R.; Kawashima, R. Improving Cognitive Function from Children to Old Age: A Systematic Review of Recent Smart Ageing Intervention Studies. Adv. Neurosci. 2014, 2014, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Nouchi, R.; Suiko, T.; Kimura, E.; Takenaka, H.; Murakoshi, M.; Uchiyama, A.; Aono, M.; Kawashima, R. Effects of Lutein and Astaxanthin Intake on the Improvement of Cognitive Functions among Healthy Adults: A Systematic Review of Randomized Controlled Trials. Nutrients 2020, 12, 617. [Google Scholar] [CrossRef] [Green Version]
- Teng, E.L.; Hasegawa, K.; Homma, A.; Imai, Y.; Larson, E.; Graves, A.; Sugimoto, K.; Yamaguchi, T.; Sasaki, H.; Chiu, D.; et al. The Cognitive Abilities Screening Instrument (CASI): A practical test for cross-cultural epidemiological studies of dementia. Int. Psychogeriatr. 1994, 6, 45–58. [Google Scholar] [CrossRef]
- Gheysen, F.; Poppe, L.; DeSmet, A.; Swinnen, S.; Cardon, G.; De Bourdeaudhuij, I.; Chastin, S.; Fias, W. Physical activity to improve cognition in older adults: Can physical activity programs enriched with cognitive challenges enhance the effects? A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donath, L.; Rossler, R.; Faude, O. Effects of Virtual Reality Training (Exergaming) Compared to Alternative Exercise Training and Passive Control on Standing Balance and Functional Mobility in Healthy Community-Dwelling Seniors: A Meta-Analytical Review. Sports Med. 2016, 46, 1293–1309. [Google Scholar] [CrossRef]


{kind=link}
| Lead Author; Year; Country | Sample Size (Female (%)) | Age | Cognitive Status |
|---|---|---|---|
| Hsieh; 2018; Taiwan * | 60 (72%) | (mean ± SD) | MMSE score 11–26 |
| VE: 31 | VE: 76.4 ± 7.6 | ||
| NC: 29 | NC: 80.0 ± 7.5 | ||
| Eggenberger; 2015; Switzerland † | 71 (65%) | (mean ± SD) | MMSE (mean ± SD) |
| VE1: 24 | VE1: 77.3 ± 6.3 | VE1: 28.4 ± 1.4 | |
| VE2: 22 | VE2: 78.5 ± 5.1 | VE2: 28.3 ± 1.2 | |
| EC: 25 | EC: 80.8 ± 4.7 | EC: 28.0 ± 1.7 | |
| Anderson-Hanley; 2018; United States * | 14 (50%) | (mean ± SD) | MoCA (mean ± SD) |
| VE: 7 | VE: 75.4 ± 9.83 | VE: 22.0 ± 3.21 | |
| EC: 7 | EC: 80.9 ± 12.3 | EC: 21.6 ± 2.70 | |
| Mrakic-Sposta; 2018; Italy (n.s.) | 10 (60%) | (mean ± SD) | MMSE (mean ± SD) 23.0 ± 3.4 |
| VE: 5 | VE: 72.0 ± 5.15 | ||
| NC: 5 | NC: 74.6 ± 6.43 | ||
| Anderson-Hanley; 2012; United States * | 79 (78%) | (mean ± SD) | Performance ≤ −1.5 SD of norm on at least one subtest (n) |
| VE: 38 | VE: 75.7 ± 9.9 | VE: 16 | |
| EC: 41 | EC: 81.6 ± 6.2 | EC: 14 | |
| Bacha; 2018; Brazil † | 46 (74%) | (Medium [Q1; Q3]) | MoCA (mean ± SD) |
| VE: 23 | VE: 71.0 (66.0; 74.5) | VE: 23.48 ± 4.94 | |
| EC: 23 | EC: 66.5 (65.0; 71.8) | EC: 22.52 ± 3.47 | |
| Htut; 2018; Thailand * | 84 (44%) | (mean ± SD) | MMSE (mean ± SD) |
| VE: 21 | VE: 75.8 ± 4.89 | VE: 25.5 ± 1.22 | |
| EC: 21 | EC: 75.9 ± 5.65 | EC: 24.7 ± 0.96 | |
| CC: 21 | CC: 75.6 ± 5.33 | CC: 25.2 ± 1.41 | |
| NC: 21 | NC: 76.0 ± 5.22 | NC: 25.2 ± 1.00 | |
| Delbroek; 2017; Belgium (n.s.) | 20 (65%) | (mean ± SD) | MoCA (mean ± SD) |
| VE: 10 (dropout: 2) | VE: 86.9 ± 5.6 | VE: 17.7 ± 5.3 | |
| NC: 10 (dropout: 1) | NC: 87.5 ± 6.6 | NC: 16.8 ± 5.8 | |
| Liao; 2020; Taiwan † | 34 (68%) | (mean ± SD) | MMSE (mean ± SD) |
| VE: 18 | VE: 75.5 ± 5.2 | VE: 27.2 ± 1.9 | |
| ECC: 16 | ECC: 73.1 ± 6.8 | ECC: 28.3 ± 1.2 | |
| Monteiro-Junior; 2017; Brazil * | 18 (67%) | (mean ± SD) | MMSE (mean ± SD) |
| VE: 9 | VE: 85.0 ± 8.0 | VE: 21.0 ± 5.0 | |
| EC: 9 | EC: 86.0 ± 5.0 | EC: 24.0 ± 4.0 | |
| Park; 2016; Korea * | 72 (94%) | (mean ± SD) | MoCA (mean ± SD) |
| VE: 36 | VE: 73.0 ± 3.0 | VE: 22.6 ± 4.9 | |
| EC: 36 | EC: 74.1 ± 2.9 | EC: 22.9 ± 4.2 |
| Lead Author; Year; Country | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Total Score (Max. = 14) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hsieh; 2018; Taiwan | N | ? | Y | Y | N | N | N | Y | Y | N | N | Y | Y | N | 6 |
| Eggenberger; 2015; Switzerland | Y | Y | Y | Y | N | N | Y | N | N | Y | Y | Y | Y | Y | 10 |
| Anderson-Hanley; 2018; United States | Y | ? | Y | Y | ? | ? | ? | Y | N | N | Y | Y | Y | Y | 8 |
| Mrakic-Sposta; 2018; Italy | Y | ? | Y | Y | ? | ? | ? | Y | N | N | N | Y | Y | N | 6 |
| Anderson-Hanley; 2012; United States | Y | Y | Y | Y | Y | ? | ? | Y | Y | Y | Y | Y | Y | Y | 12 |
| Bacha; 2018; Brazil | Y | Y | Y | Y | Y | ? | N | Y | N | Y | Y | Y | Y | Y | 11 |
| Htut; 2018; Thailand | Y | ? | Y | Y | Y | ? | N | N | N | N | Y | Y | Y | N | 7 |
| Delbroek; 2017; Belgium | Y | ? | Y | Y | Y | ? | ? | Y | N | N | N | N | Y | N | 6 |
| Liao; 2020; Taiwan | Y | Y | Y | Y | Y | N | N | Y | N | N | Y | Y | Y | N | 9 |
| Monteiro-Junior; 2017; Brazil | Y | ? | Y | Y | ? | N | Y | N | N | N | Y | Y | Y | N | 7 |
| Park; 2016; Korea | Y | Y | Y | Y | ? | ? | ? | Y | N | N | Y | Y | N | N | 7 |
| Total score across studies | 10 | 5 | 11 | 11 | 5 | 0 | 2 | 8 | 2 | 3 | 8 | 10 | 10 | 4 | - |
| Average of total score ± SD | 8.1 ± 2.02 |
| Lead Author; Year; Country | Periods of Intervention | VR Device | Experimental Group | Control Group |
|---|---|---|---|---|
| Hsieh; 2018; Taiwan * | Two 60 min sessions/week for 6 months | Xbox 360 Kinect, 100-inch flat screen | VE: VR-based Tai Chi exercise (Chinese mind-body exercise with biofeedback) | NC: No intervention |
| Eggenberger; 2015; Switzerland † | Two 60 min sessions/week for 6 months | Impact Dance Platform, large screen | VE1: Video game dancing on the pressure sensitive areas to detect steps VE2: Treadmill walking with verbal memory exercise | EC: Treadmill walking without an additional cognitive task |
| Anderson-Hanley; 2018; United States * | ≥Two ≥20 min sessions/week for 6 months | Cybercycle, virtual reality display (small monitor) | VE: VR-bike rides with effortful cognitive videogame | EC: VR-bike rides with passive cognitive processing |
| Mrakic-Sposta; 2018; Italy (n.s.) | Three 40–45 min sessions/week for 6 weeks | Cycle-ergometer, finger touch projector | VE: Cycling exercise with VR-based cognitive training | NC: No treatment |
| Anderson-Hanley; 2012; United States * | Five 45 min sessions/week for 3 months | Cybercycle, virtual reality display (small monitor) | VE: VR-bike rides with virtual 3D tours | EC: Traditional stationary bike rides |
| Bacha; 2018; Brazil † | Two 60 min sessions/week for 7 weeks | Xbox Kinect Adventures, 50-inch TV | VE: Playing Kinect games including cognitive demands | EC: Conventional physical therapy exercises |
| Htut; 2018; Thailand * | Three 30 min sessions/week for 8 weeks | Xbox 360 | VE: VR-based exercise games | EC: Strength and balance exercises CC: Brain exercise games NC: no exercise |
| Delbroek; 2017; Belgium (n.s.) | Two 18–30 min sessions/week for 6 weeks | BioRescue, 55-inch TV-flat screen | VE: VR cognitive-motor dual task training | NC: No intervention (usual care) |
| Liao; 2020; Taiwan † | Three 60 min sessions/week for 12 weeks | Microsoft Kinect, VIVE system | VE: VR-based physical and cognitive training | ECC: Combined physical and cognitive training |
| Monteiro-Junior; 2017; Brazil * | Two 30–45 min sessions/week for 6–8 weeks | Wii Fit Plus | VE: Playing VR-based exercise games | EC: Playing exercise games |
| Park; 2016; Korea * | Two 30+20 min sessions/week for 6 weeks | Kayak ergometers 3-D beam projector | VE: Conventional exercise & VR kayak paddling exercise | EC: Conventional exercise |
| Lead Author; Year; Country | Measured Cognitive Functions | Statistical Method | |||||||
|---|---|---|---|---|---|---|---|---|---|
| General Cognitive Function | Executive Function | Working Memory | Short-Term Memory | Episodic Memory | Processing Speed | Attention | Others | ||
| Hsieh; 2018; Taiwan | ABSTR in CASI *, ANML in CASI (n.s.) | short-term memory in CASI (n.s.) | ATTEN in CASI (n.s.) | subtests in CASI (MENMA, orientation, language, drawing, long-term memory) (n.s.) | generalized estimating equation (GEE) analyses | ||||
| Eggenberger; 2015; Switzerland | TMT-B †, executive control task † | digit backward tasks in WMS-R † | digit forward tasks in WMS-R (n.s.) | logical memory subtest (story recall) in WMS-R †, paired-associates learning task † | TMT-A †, DSST in WAIS-R † | age concentration tests A and B † | multiple regression analysis | ||
| Anderson-Hanley; 2018; United States | Stroop †, color trails (n.s.) | digit span (n.s.) | ADAS word list (immediate recall, delayed recall) * | ecological validity * | repeated measures ANCOVA | ||||
| Mrakic-Sposta; 2018; Italy | MMSE (n.s.) | FAB (n.s.), TMT-B (exculded), VF (n.s.) | RAVLT_I (n.s.), RAVLT_D (n.s.) | TMT-A (n.s) | AM (n.s.) | ROCFT (n.s.), FAQ (n.s.) | Mann-Whitney U-Test | ||
| Anderson-Hanley; 2012; United States | color trails *, Stroop C *, COWAT (n.s.), categories (n.s.) | digit span backwards * | RAVLT_I (n.s.), RAVLT_D (n.s.), Fuld delayed recall (n.s.), figure delayed recall (n.s.) | LDST (n.s.) | figure copy (n.s.), clock (n.s.) | repeated measures ANCOVA | |||
| Bacha; 2018; Brazil | MoCA † | repeated measures ANOVA | |||||||
| Htut; 2018; Thailand | MoCA * | TUG-cog * | two-way mixed ANOVA | ||||||
| Delbroek; 2017; Belgium | MoCA (n.s.) | TUG-DT (n.s.) | Wilcoxon signed-rank test two-sided | ||||||
| Liao; 2020; Taiwan † | MoCA † | EXIT-25 † | CVVLT (immediate recall, delayed recall) † | repeated measures ANOVA | |||||
| Monteiro-Junior; 2017; Brazil * | MMSE (n.s.) | FMT (route, recall) (n.s.), VF(n.s.) | digit span backward (n.s.) | digit span forward * | TMT-A (n.s.) | independent t tests | |||
| Park; 2016; Korea * | MoCA * | Independent t tests | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakaki, K.; Nouchi, R.; Matsuzaki, Y.; Saito, T.; Dinet, J.; Kawashima, R. Benefits of VR Physical Exercise on Cognition in Older Adults with and without Mild Cognitive Decline: A Systematic Review of Randomized Controlled Trials. Healthcare 2021, 9, 883. https://doi.org/10.3390/healthcare9070883
Sakaki K, Nouchi R, Matsuzaki Y, Saito T, Dinet J, Kawashima R. Benefits of VR Physical Exercise on Cognition in Older Adults with and without Mild Cognitive Decline: A Systematic Review of Randomized Controlled Trials. Healthcare. 2021; 9(7):883. https://doi.org/10.3390/healthcare9070883
Chicago/Turabian StyleSakaki, Kohei, Rui Nouchi, Yutaka Matsuzaki, Toshiki Saito, Jérôme Dinet, and Ryuta Kawashima. 2021. "Benefits of VR Physical Exercise on Cognition in Older Adults with and without Mild Cognitive Decline: A Systematic Review of Randomized Controlled Trials" Healthcare 9, no. 7: 883. https://doi.org/10.3390/healthcare9070883