
Women’s Perception of Male Involvement in Antenatal, Childbirth and Postnatal Care in Urban Slum Areas in Bangladesh: A Community-Based Cross-Sectional Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Participants
2.2. Data Collection
2.3. Measure of Outcome Variables
2.4. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics of the Respondents and Their Husbands
3.2. Respondents’ and Their Husbands’ Access to Maternal and Reproductive Health Services
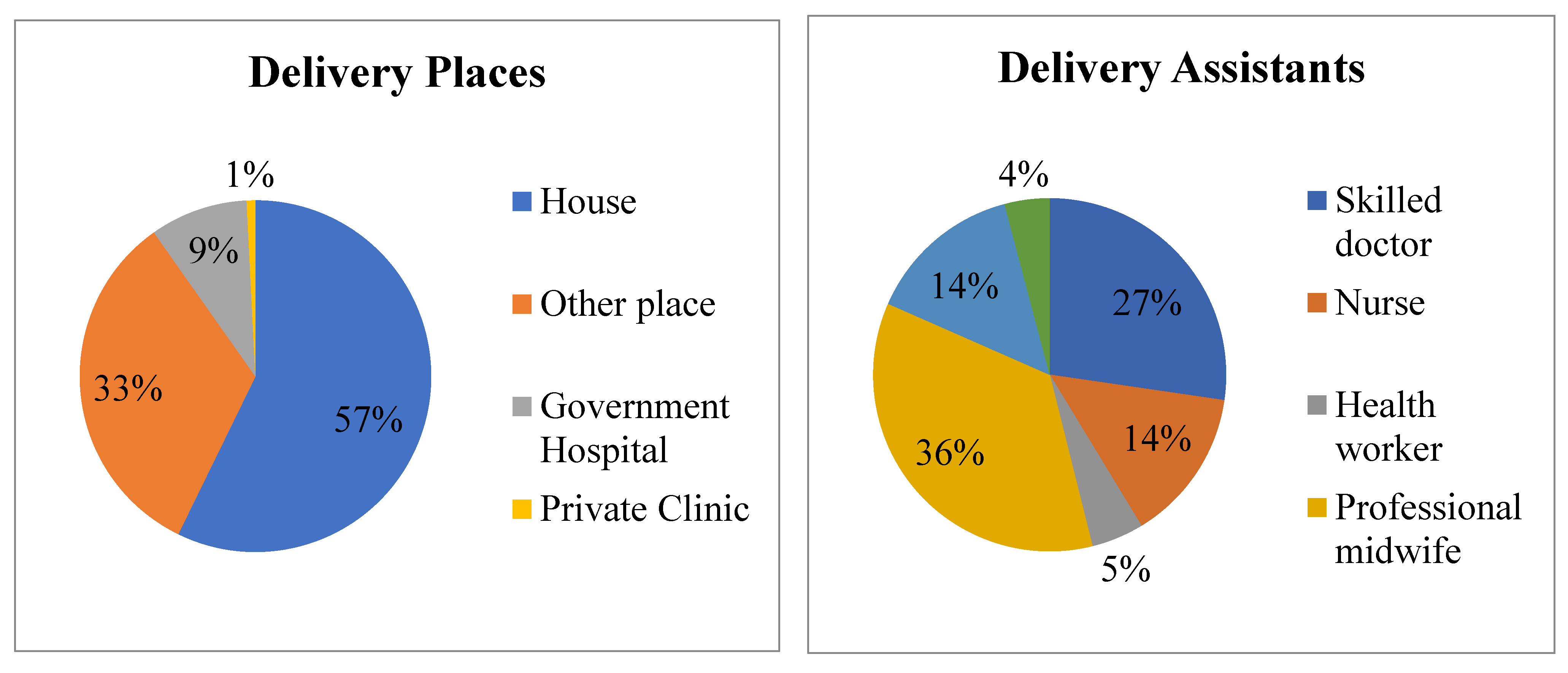
3.3. Delivery Location and Birth Attendants during the Last Delivery of Respondents
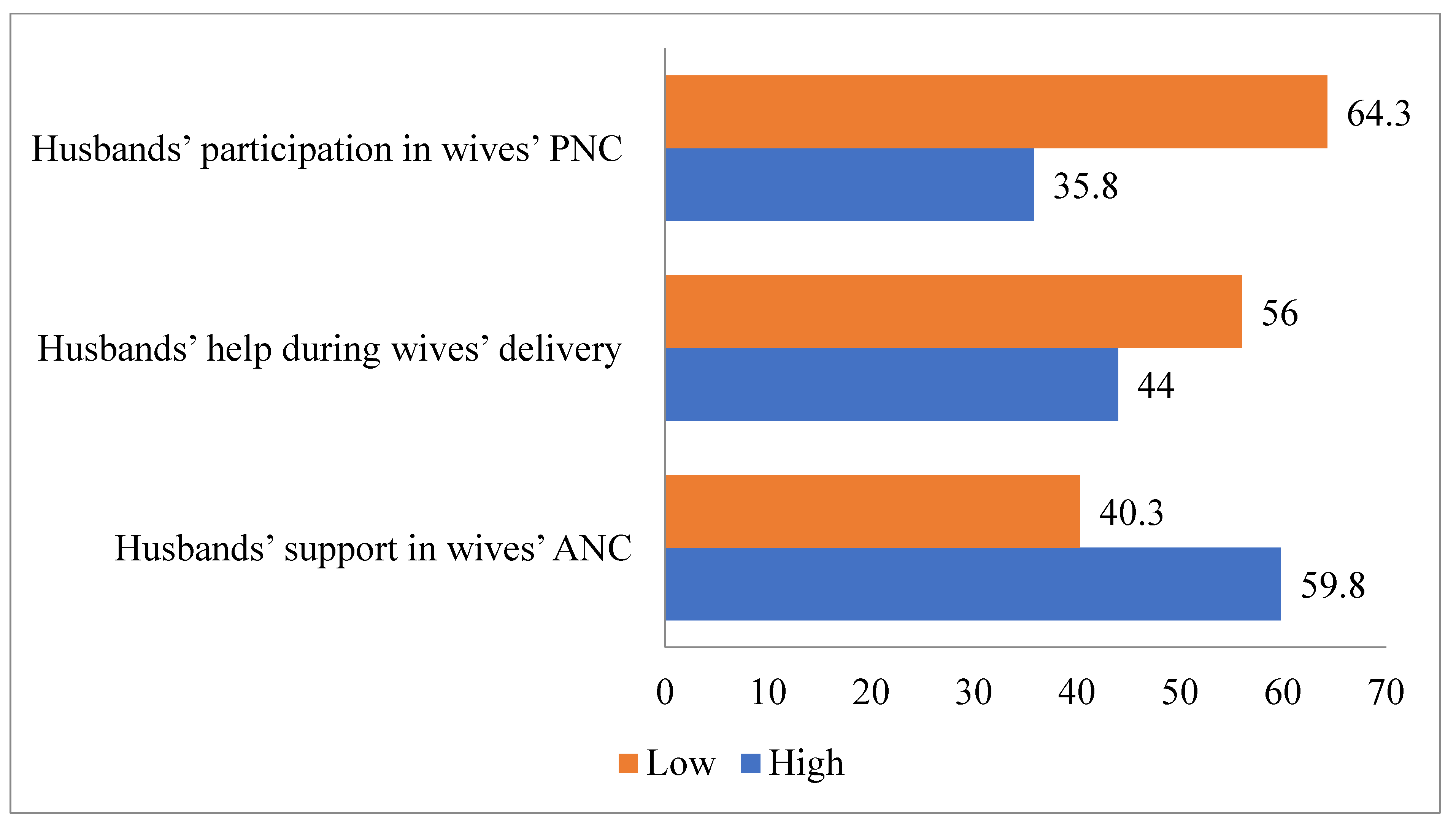
3.4. Male Participation in Antenatal, Delivery and Postnatal Care
3.5. Predictors of the Husbands’ Participation in Wives’ Antenatal, Delivery and Postnatal Care
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Islam, M.; Sultana, N. Risk factors for pregnancy related complications among urban slum and non-slum women in Bangladesh. BMC Pregnancy Childbirth 2019, 19, 235. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Population Research and Training (NIPORT); ICDDRB; MEASURE Evaluation. Bangladesh Urban Health Survey 2013 Final Report; MEASURE Evaluation: Dhaka, Bangladesh; Chapel Hill, NC, USA, 2015; Available online: https://www.measureevaluation.org/resources/publications/tr-15-117 (accessed on 15 February 2020).
- Bangladesh Bureau of Statistics (BBS). Census of Slum Areas and Floating Population 2014; BBS: Dhaka, Bangladesh, 2015; Available online: http://203.112.218.65:8008/WebTestApplication/userfiles/Image/Slum/FloatingPopulation2014.pdf (accessed on 15 February 2020).
- National Institute of Population Research and Training (NIPORT); MEASURE Evaluation; ICDDRB; ACPR. 2006 Bangladesh Urban Health Survey; NIPORT, MEASURE Evaluation, ICDDR,B and ACPR: Dhaka, Bangladesh; Chapel Hill, NC, USA, 2008; Available online: https://www.measureevaluation.org/resources/publications/tr-08-68/at_download/document (accessed on 16 February 2020).
- Cairo Programme of Action. International Conference on Population and Development Cairo. 1994. Available online: http://www.iisd.ca/cairo/program/p00000.html (accessed on 16 February 2020).
- Maharaj, P. Promoting Male Involvement in Reproductive Health Agenda. Empower. Women Gend. Equity 2000, 44, 37–47. [Google Scholar] [CrossRef]
- Drennan, M. Reproductive Health: New Perspectives on Men’s Participation. Popul. Rep. 1998, 46, 1–35. [Google Scholar]
- Zakaria, M.; Bhuiyan, M.M. Determinants of Male Involvement in Women’s Reproductive Health: A Multilevel Study in Bangladesh. Malays. J. Public Health Med. 2016, 16, 3, 211–218. [Google Scholar]
- Rob, U. Men and Reproductive Health. In Equality between Man and Woman is Slovene, [Souvenir (in Bengali Version) on World Population Day] Directorate General of Family Planning; Ministry of Health & Family Welfare: Dhaka, Bangladesh, 2005. [Google Scholar]
- National Institute of Population Research and Training (NIPORT); Mitra and Associates; ICF International. Bangladesh Demographic and Health Survey 2011; NIPORT, Mitra and Associates, and ICF International: Dhaka, Bangladesh; Calverton, MD, USA, 2013; Available online: https://dhsprogram.com/pubs/pdf/fr265/fr265.pdf (accessed on 16 February 2020).
- World Population Review. Population of Cities in Bangladesh. 2019. Available online: http://worldpopulationreview.com/countries/bangladesh-population/cities/ (accessed on 5 May 2020).
- Tolossa, D.; Medhin, G.; Legesse, M. Community knowledge, attitude, and practices towards tuberculosis in Shinile town, Somali regional state, eastern Ethiopia: A cross-sectional study. BMC Public Health 2014, 14, 804. [Google Scholar] [CrossRef] [Green Version]
- Bishwajit, G.; Tang, S.; Yaya, S.; Ide, S.; Fu, H.; Wang, H.; He, Z.; Da, F.; Feng, Z. Factors associated with male involvement in reproductive care in Bangladesh. BMC Public Health 2017, 17, 3. [Google Scholar] [CrossRef] [Green Version]
- Zakaria, M.; Xu, J.; Karim, F.; Cheng, F. Reproductive health communication between mother and adolescent daughter in Bangladesh: A cross-sectional study. BMC Reprod. Health 2019, 16, 114. [Google Scholar] [CrossRef] [Green Version]
- Zakaria, M. Women’s Perception on Male Involvement in Reproductive Health in Rural and Urban Bangladesh: A Comparative Study. J. Rural Dev. 2015, 40, 67–90. [Google Scholar]
- National Institute of Population Research and Training (NIPORT); Mitra and Associates; ICF International. Bangladesh Demographic and Health Survey 2014; NIPORT, Mitra and Associates, ICF International: Dhaka, Bangladesh; Rockville, MD, USA, 2016; Available online: https://dhsprogram.com/pubs/pdf/FR311/FR311.pdf (accessed on 5 May 2020).
- Rahman, A.E.; Perkins, J.; Islam, S.; Siddique, A.B.; Moinuddin, M.; Anwar, M.R.; Mazumder, T.; Ansar, A.; Rahman, M.M.; Raihana, S.; et al. Knowledge and involvement of husbands in maternal and newborn health in rural Bangladesh. BMC Pregnancy Childbirth 2018, 18, 247. [Google Scholar] [CrossRef] [Green Version]
- Gibore, N.S.; Bali, T.A.L.; Kibusi, S.M. Factors influencing men’s involvement in antenatal care services: A cross-sectional study in a low resource setting, Central Tanzania. Reprod. Health 2019, 16, 52. [Google Scholar] [CrossRef] [Green Version]
- Falade-Fatila, O.; Adebayo, A.M. Male partners’ involvement in pregnancy related care among married men in Ibadan, Nigeria. Reprod. Health 2020, 17, 14. [Google Scholar] [CrossRef] [Green Version]
- Adams, Y.J.; Stommel, M.; Ayoola, A.; Horodynski, M.; Malata, A.; Smith, B. Husbands’ knowledge and attendance at wives’ postpartum care among rural farmers. Health Care Women Int. 2018, 39, 1020–1037. [Google Scholar] [CrossRef]
- Kamal, M.M.; Islam, M.S.; Alam, M.S.; Hassan, A.B.M. Determinants of Male Involvement in Family Planning and Reproductive Health in Bangladesh. Am. J. Hum. Ecol. 2013, 2, 83–93. [Google Scholar] [CrossRef] [Green Version]
- Stelin, B. This Is Not Your Life: Television as the Third Parent. In Mass Media Issues, 3rd ed.; Rodman, G., Ed.; Kendall/Hunt Publishing Company: Dubuque, IA, USA, 1986; pp. 112–115. [Google Scholar]
- Gamble, M.W.; Gamble, T.K. Introducing Mass Communication; McGraw-Hill Inc.: New York, NY, USA, 1986. [Google Scholar]
- Adams, D.M.; Fuchs, M. The Video Media and Cultural Misunderstanding. In Mass Media Issues; Rodman, G., Ed.; Kendall/Hunt Publishing Company: Dubuque, IA, USA, 1989; pp. 107–112. [Google Scholar]
- Shahjahan, M.; Mumu, S.J.; Afroz, A.; Chowdhury, H.A.; Kabir, R.; Ahmed, K. Determinants of male participation in reproductive healthcare services: A cross-sectional study. Reprod. Health 2013, 10, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Ditekemena, J.; Koole, O.; Engmann, C.; Matendo, R.; Tshefu, A.; Ryder, R.; Colebunders, R. Determinants of male involvement in maternal and child health services in sub-Saharan Africa: A review. BMC Reprod. Health 2012, 9, 32. [Google Scholar] [CrossRef] [Green Version]
- Rogers, E.M. Diffusion of Innovations, 4th ed.; Free Press: New York, NY, USA, 1995. [Google Scholar]
- Schiavo, R. Health Communication: From Theory to Practice; Jossey-Bass: San Francisco, CA, USA, 2007. [Google Scholar]
- Thomas, R.K. Health Communication; Springer: New York, NY, USA, 2006. [Google Scholar]
- Gibore, N.S.; Ezekiel, M.J.; Meremo, A.; Munyogwa, M.J.; Kibusi, S.M. Determinants of men’s involvement in maternity care in Dodoma Region, Central Tanzania. J. Pregnancy 2019, 1–10. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Frequency | Percentage |
|---|---|---|
| Respondents’ education (mean years 2.79, SD = 3.30) | ||
| No education | 202 | 50.5 |
| Up to class 5 | 117 | 29.3 |
| >class 5 | 81 | 20.3 |
| Husbands’ education (mean years 4.06, SD = 2.77) | ||
| No education | 151 | 37.8 |
| Up to class 5 | 113 | 28.3 |
| >class 5 | 136 | 34.0 |
| Respondents’ occupation | ||
| Housewife | 238 | 59.5 |
| Day laborer | 13 | 3.3 |
| Business/domestic worker | 90 | 22.6 |
| Service/garment worker | 59 | 14.8 |
| Husbands’ occupation | ||
| Day laborer/rickshaw puller/jobless | 116 | 26.6 |
| Business | 178 | 44.6 |
| Service/garment worker | 82 | 20.5 |
| Driver | 34 | 8.5 |
| Respondents’ age (mean ± SD) | 25.51 ± 5.72 | |
| Husbands’ age (mean ± SD) | 32.24 ± 6.63 | |
| Monthly household income | ||
| ≤5000 BDT (≤60 USD) | 59 | 14.8 |
| 5000–10,000 BDT (60–118 USD) | 131 | 32.8 |
| 10,001–15,000 BDT (119–176 USD) | 129 | 32.3 |
| ≥15,000 BDT (≥176 USD) | 81 | 20.3 |
| Number of children | ||
| 1 | 146 | 36.5 |
| 2 | 144 | 36.0 |
| >2 | 110 | 27.5 |
| Respondents’ TV viewing | ||
| Yes | 261 | 65.3 |
| No | 139 | 34.8 |
| Husbands’ TV viewing | ||
| Yes | 201 | 50.3 |
| No | 199 | 49.8 |
| Respondents’ radio listening | ||
| Yes | 61 | 15.3 |
| No | 338 | 84.5 |
| Husbands’ radio listening | ||
| Yes | 101 | 25.3 |
| No | 299 | 74.8 |
| Respondents’ internet use | ||
| Yes | 34 | 8.5 |
| No | 364 | 91.0 |
| Husbands’ internet use | ||
| Yes | 130 | 32.5 |
| No | 270 | 67.5 |
| Having a utility facility in the slum | ||
| Little | 200 | 50.0 |
| More | 200 | 50.0 |
| Variables | Yes (n (%)) | No (n (%)) |
|---|---|---|
| Ever had NGOs RH and MH awareness in slum areas | 147 (36.7) | 253 (63.3) |
| Husbands ever participated at any meeting on RH and MH | 17 (4.3) | 383 (95.7) |
| NGOs ever supplied contraceptives in slum areas | 8 (2.0) | 392 (98.0) |
| Husbands ever discussed with NGO/health worker on FP and RH | 125 (31.3) | 275 (68.7) |
| Items | Yes (n (%)) | No (n (%)) |
|---|---|---|
| Took care of wife’s nutrition and rest during pregnancy | 315 (78.7) | 85 (21.3) |
| Reminded the wife about ANC visits | 21 (5.3) | 379 (94.2) |
| Managed the total expense to visit the doctor for ANC check-up | 139 (34.7) | 261 (65.3) |
| Accompanied wife during visiting doctor for ANC check-up | 228 (57.0) | 172 (43.0) |
| Advised and took initiative for going to hospital/clinic during delivery | 19 (4.8) | 381 (95.2) |
| Managed the total expense to go to the health center during delivery | 141 (35.3) | 259 (64.8) |
| Took wife to the health center or hospital for delivery | 140 (35.0) | 260 (65.0) |
| Supported in arranging an SBA during delivery | 211 (52.7) | 189 (47.3) |
| Helped in visiting the doctor during the postnatal period | 161 (40.3) | 239 (59.7) |
| Took care of wife’s nutrition and rest during PNC | 270 (67.5) | 130 (32.5) |
| Characteristics (N = 400) | ANC | Delivery | PNC |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| ⸸ Husbands’ education | |||
| No education (ref.) | 1 | ||
| Have education | 1.40 (0.83–2.35) | ||
| Husbands’ occupation | |||
| Labor/rickshaw puller/business (ref.) | 1 | 1 | 1 |
| Driver/service/garment worker | 2.07 (1.16–3.68) a | 1.61 (0.91–2.84) | 1.73 (0.95–3.15) |
| ⸸ Husbands’ TV viewing | |||
| No (ref.) | 1 | 1 | |
| Yes | 1.18 (0.69–2.00) | 2.08 (1.20–3.60) b | |
| Number of children | |||
| 1 (ref.) | 1 | 1 | 1 |
| 2 | 0.56 (0.30–1.04) | 0.72 (0.39–1.31) | 0.36 (0.18–0.69) b |
| >2 | 0.70 (0.33–1.52) | 0.35 (0.16–0.75) b | 0.70 (0.31–1.58) |
| ⸸ Having a utility facility in the slum | |||
| Little (ref.) | 1 | 1 | |
| More | 3.10 (1.61–5.96) c | 2.33 (1.17–4.64) a | |
| Relationship between husband and wife | |||
| Not good (ref.) | 1 | 1 | 1 |
| Good | 2.53 (1.50–4.26) c | 2.18 (1.27–3.75) b | 4.61 (2.43–8.76) c |
| Couple communication on FP and RH | |||
| Rare (ref.) | 1 | 1 | 1 |
| Sometimes | 1.75 (0.97–3.14) | 1.96 (1.04–3.73) a | 1.46 (0.73–2.91) |
| Often/regular | 1.48 (0.74–2.98) | 2.81 (1.34–5.91) b | 2.20 (0.98–4.94) |
| Starting time of couple communication on FP and RH | |||
| After marriage (ref.) | 1 | 1 | 1 |
| After the birth of the first baby | 1.33 (0.72–2.47) | 1.41 (0.77–2.57) | 1.28 (0.67–2.45) |
| After the birth of the second baby | 1.33 (0.62–2.86) | 0.82 (0.37–1.84) | 0.55 (0.22–1.39) |
| Respondents’ perception of husbands’ FP, RH and MH knowledge | |||
| Poor (ref.) | 1 | 1 | 1 |
| Moderate | 0.62 (0.33–1.15) | 0.70 (0.36–1.36) | 0.48 (0.23–1.02) |
| Good | 0.48 (0.16–1.44) | 1.18 (0.41–3.36) | 0.43 (0.14–1.32) |
| Respondents’ self-reported FP, RH and MH knowledge | |||
| Poor (ref.) | 1 | 1 | 1 |
| Moderate | 2.19 (1.12–4.26) a | 1.40 (0.66–2.99) | 1.03 (0.45–2.39) |
| Good | 1.90 (0.57–6.36) | 1.29 (0.38–4.37) | 2.01 (0.57–7.08) |
| NGO’s RH and MH program in the slum | |||
| No (ref.) | 1 | 1 | 1 |
| Yes | 1.89 (1.00–3.55) a | 0.75 (0.40–1.41) | 0.87 (0.45–1.69) |
| Husbands ever discussed with a health worker about RH and MH issues | |||
| No (ref.) | 1 | 1 | 1 |
| Yes | 7.00 (3.33–14.70) c | 5.55 (2.89–10.66) c | 5.52 (2.92–10.43) c |
| Model chi-square | 128.46 c | 150.75 c | 165.69 c |
| −2 log likelihood | 410.75 | 397.99 | 355.88 |
| Nagelkerke R2 | 0.37 | 0.42 | 0.47 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zakaria, M.; Khan, A.K.M.Z.R.; Ahmad, M.S.; Cheng, F.; Xu, J. Women’s Perception of Male Involvement in Antenatal, Childbirth and Postnatal Care in Urban Slum Areas in Bangladesh: A Community-Based Cross-Sectional Study. Healthcare 2021, 9, 473. https://doi.org/10.3390/healthcare9040473
Zakaria M, Khan AKMZR, Ahmad MS, Cheng F, Xu J. Women’s Perception of Male Involvement in Antenatal, Childbirth and Postnatal Care in Urban Slum Areas in Bangladesh: A Community-Based Cross-Sectional Study. Healthcare. 2021; 9(4):473. https://doi.org/10.3390/healthcare9040473
Chicago/Turabian StyleZakaria, Muhammad, A. K. M. Ziaur Rahman Khan, Md. Sarwar Ahmad, Feng Cheng, and Junfang Xu. 2021. "Women’s Perception of Male Involvement in Antenatal, Childbirth and Postnatal Care in Urban Slum Areas in Bangladesh: A Community-Based Cross-Sectional Study" Healthcare 9, no. 4: 473. https://doi.org/10.3390/healthcare9040473