1. Introduction
Cadmium is a cumulative toxic non-essential transition metal that poses a serious public health threat [
1]. Earlier studies have suggested that cadmium is associated with chronic kidney disease, bone disease, cardiovascular disease, and malignancy [
2,
3,
4,
5]. The relationship between cadmium exposure and mortality in populations exposed to high cadmium concentrations, including labors with occupational exposure [
6] or residents living in polluted areas, has been confirmed [
7]. Among the cadmium pollution incidents in Taiwan, those caused by chemical plants in Taoyuan City from 1983 to 1984 are the most famous. As a result, the nearby farmland was seriously polluted, and it was not replanted. It has been 37 years since the incident, and the half-life of cadmium in the human body has been reported to be approximately 30 years. Most of the patients of Chang Gung Memorial Hospital come from Taoyuan city due to its geographical location. Cadmium measurements conducted on these patients is expected to be able to detect the residual amount of exposure and its effect on local residents.
Cadmium exposure has been reported to inhibit saliva secretion of the parotid gland and reduce the concentration of the main salivary digestive enzyme amylase [
8]. It has been suggested that these effects of cadmium may be due to the suppression of acetylcholine release and the destruction of parasympathetic impulses, which play an important role in regulating saliva secretion [
8]. The competitive inhibitory effect of cadmium on calcium channels [
9,
10] and the induction of oxidative stress in the salivary glands can also decrease the function of saliva [
11]. Some protein components inside saliva can help reduce the caries rate due to their antibacterial and remineralization functions [
12]. Amylase acts on carbohydrates and cleaves starches into smaller polysaccharides, and it has antibacterial properties as well as buffering effects [
13]. Proline-rich proteins, statherin and histatins, help with remineralization by increasing the local calcium concentrations due to their affinity for enamel surfaces [
14]. Cadmium can inhibit saliva secretion and it can act as a calcium channel blocker that can interfere with calcium metabolism during the formation of tooth enamel. Therefore, cadmium exposure is believed to increase the caries rate [
15,
16,
17].
Cadmium can be consumed through food and obtained from environmental sources such as emissions from mining, smelting, fuel combustion, phosphate fertilizer use, sewage sludge application, disposal of metal wastes, and industrial uses of cadmium in the manufacturing of batteries, pigments, stabilizers, and alloys [
17,
18,
19]. Once cadmium enters the body, it accumulates in the kidneys, liver, and bones and is slowly excreted from the body in urine [
19]. A continuous loss of calcium and phosphorus and a disturbed vitamin D metabolism due to renal tubular dysfunction will occur once cadmium enters the body [
20]. Cadmium poisoning can affect human organs and cause Itai-itai disease [
21]. Bone is one of the target organs for cadmium toxicity [
22]. Various changes in the skeletal system characterized by osteopenia, osteoporosis, and/or osteomalacia with an increased incidence of bone fractures are the main unfavorable health effects of chronic environmental exposure to cadmium [
23,
24,
25].
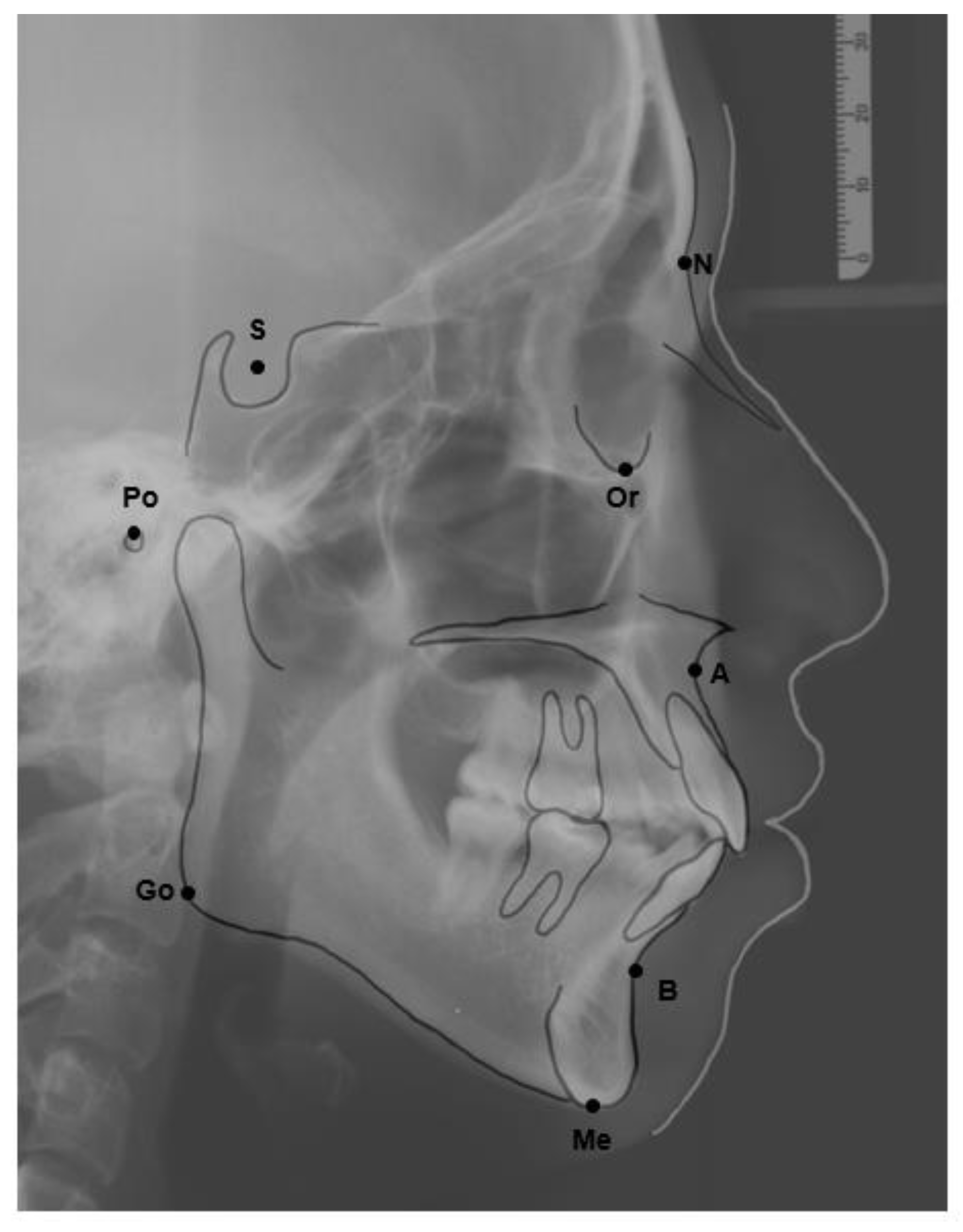
The bone density could vary depending on the amount of contact with cadmium. The facial pattern is believed to be associated with bone density according to the research of facial patterns associated with alveolar bone quality by Li et al. in 2014 and Amini et al. in 2017 [
26,
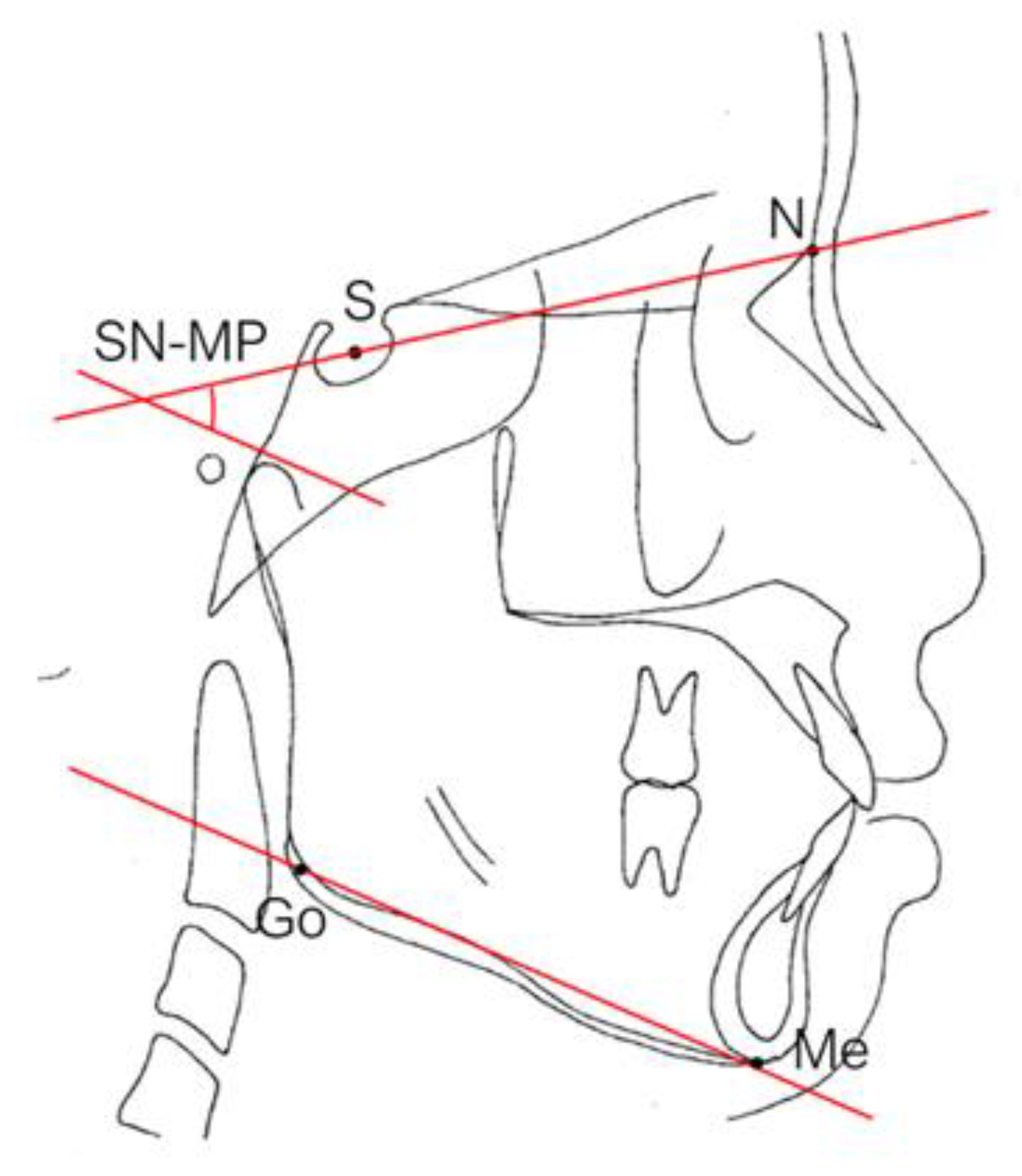
27]. There are three basic types of vertical facial patterns: low-angle, average-angle, and high-angle patterns used in orthodontic dentistry [
27]. The facial pattern is an important determinant of orthodontic treatment because it can affect treatment goals, prognosis, and plans, and it affects growth prediction, anchoring systems, bite force, and function [
26]. Bone density has been reported to be the lowest in patients with high angles among these three patterns [
27]. The association between the exposure to cadmium and bone density, and its association with the facial pattern, has led to the question of whether there is a connection between the amount of cadmium exposure and the type of facial pattern.
To evaluate and identify patients with likely success who might take longer to treat, various indices can be used after performing measurements. The indices of complexity outcome and need (ICON) and the decayed, missing, and filled surfaces (DMFS) are used to analyze whether the patient in need has been properly treated at our department. The ICON includes both an esthetic score and an occlusal index of malocclusion severity for the evaluation of treatment need [
28]. DMFS is the expression of caries prevalence; thus, it is used to estimate how much dentition is affected by dental caries. A higher score on the DMFS represents more severe dental destruction and therefore might be associated with a higher score on ICON [
29].
It has been reported that cadmium exposure results in dental caries, but most of the papers are limited to animal studies and epidemiological data from specific areas. Arora et al. [
17] demonstrated that among children with a history of caries in their deciduous teeth, an interquartile range increase in urine cadmium concentration was related to a 17% increase in the number of decayed or filled surfaces. The authors concluded that environmental cadmium exposure could be associated with an increased hazard of dental caries in deciduous teeth. Nevertheless, there was no correlation between urine cadmium concentration and caries in adult teeth [
17]. On the other hand, it has also been reported that there is a positive correlation between the cadmium content in the enamel of human premolars and the caries score of permanent teeth. It has also been pointed out that increases in the concentrations of cadmium and tin in human teeth are associated with higher dental caries rates, but the concentrations of copper, lead, and selenium are not [
30]. Furthermore, Malara et al. [
31] reported that cadmium concentrations in impacted third molars were significantly higher for people living in the relatively polluted Ruda Slaska region than for people living in the Bielsko-Biala region. Combining the above studies, the conclusion is still not clear. The effect of early-life cadmium exposure and repeated lifetime cadmium exposures need to be investigated further.
The influence of cadmium exposure on the dental indices of orthodontic or dental patients is unknown, which initiated our interest in this research. In this study, we hypothesized that cadmium exposure could be relevant to dental caries and bone density. Therefore, this cross-sectional study attempted to determine whether tooth decay with tooth loss following cadmium exposure is associated with some dental or skeletal traits such as malocclusions, sagittal skeletal pattern, and tooth decay.
3. Results
Table 1 shows the baseline demographics of the orthodontic patients stratified according to their urine cadmium concentrations as high or low. The patients were 25.07 ± 4.33 years old, and most were female (85%). The average body mass index was 21.73 ± 3.76 kg/m
2. These 60 patients did not have diabetes mellitus, hypertension, or smoking habits, but a few engaged in alcohol consumption (3.3%) and some had bruxism (31.7%). There were more women in the low urine cadmium group than in the high urine cadmium group (
p = 0.02). There were no significant differences in any other variables between the groups.
As shown in
Table 2, the skeletal relationship of the orthodontic patients was mainly Class I (48.3%), followed by Class II (35.0%) and Class III (16.7%). No significant difference was found between the groups (
p = 0.74).
Class I molar relationships occurred in 46.7% of these patients, 15% had Class II molar relationships, and 38.3% had Class III molar relationships (
Table 3). No significant difference was found between the two groups (
p = 0.79).
The mean DMFS score was 8.05 ± 5.54, including 2.03 ± 3.11 for the decayed index, 0.58 ± 1.17 for the missing index, and 5.52 ± 3.92 for the filled index (
Table 4). There was no significant difference between the patients of the two groups in any dimension of the index (
p > 0.05).
Among the 60 patients, the average ICON score was 53.35 ± 9.01, which included esthetic, crowding, spacing, crossbite, open bite, overbite, and buccal relationships (
Table 5). There was no significant difference between the groups (
p = 0.59).
As shown in
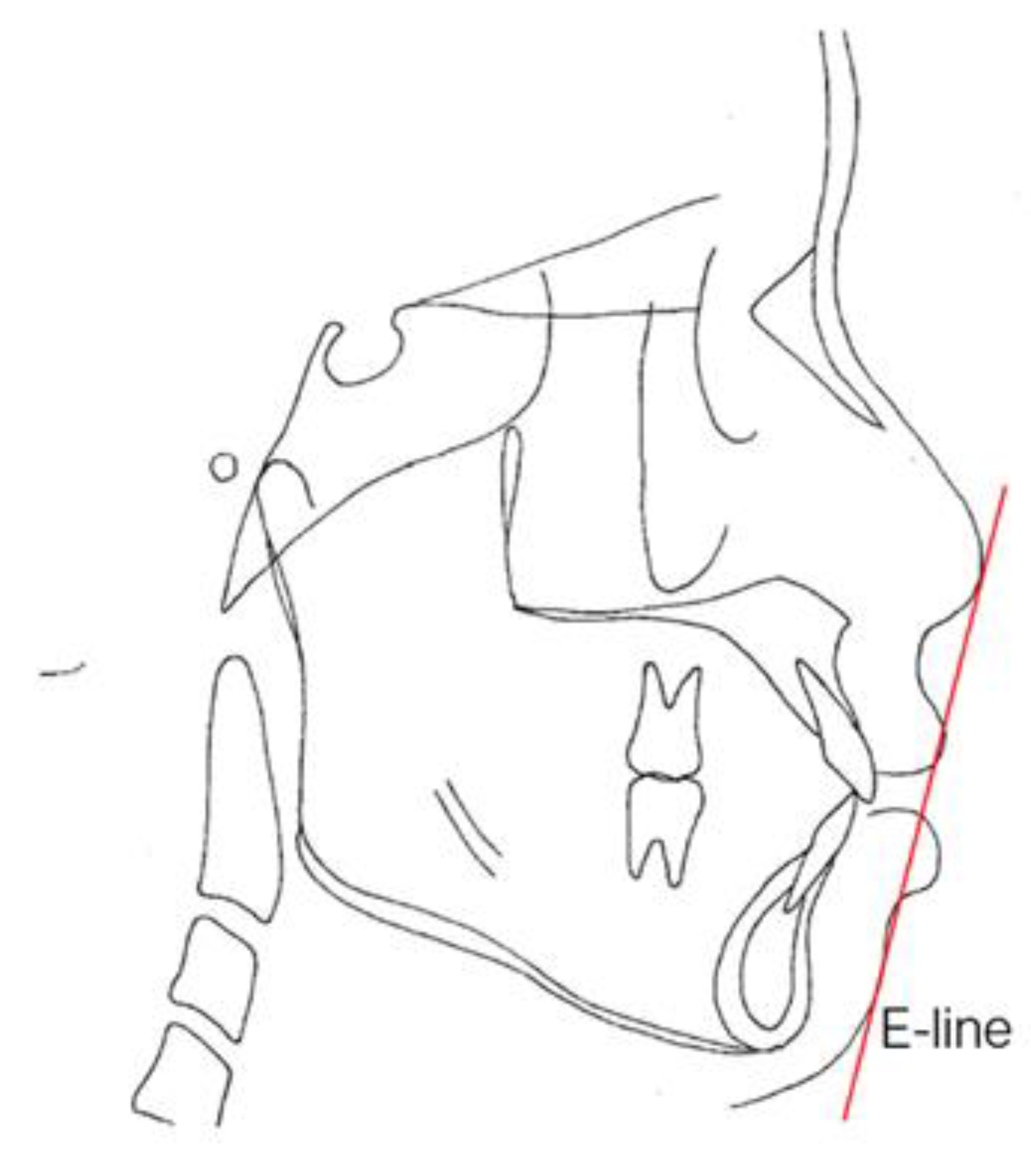
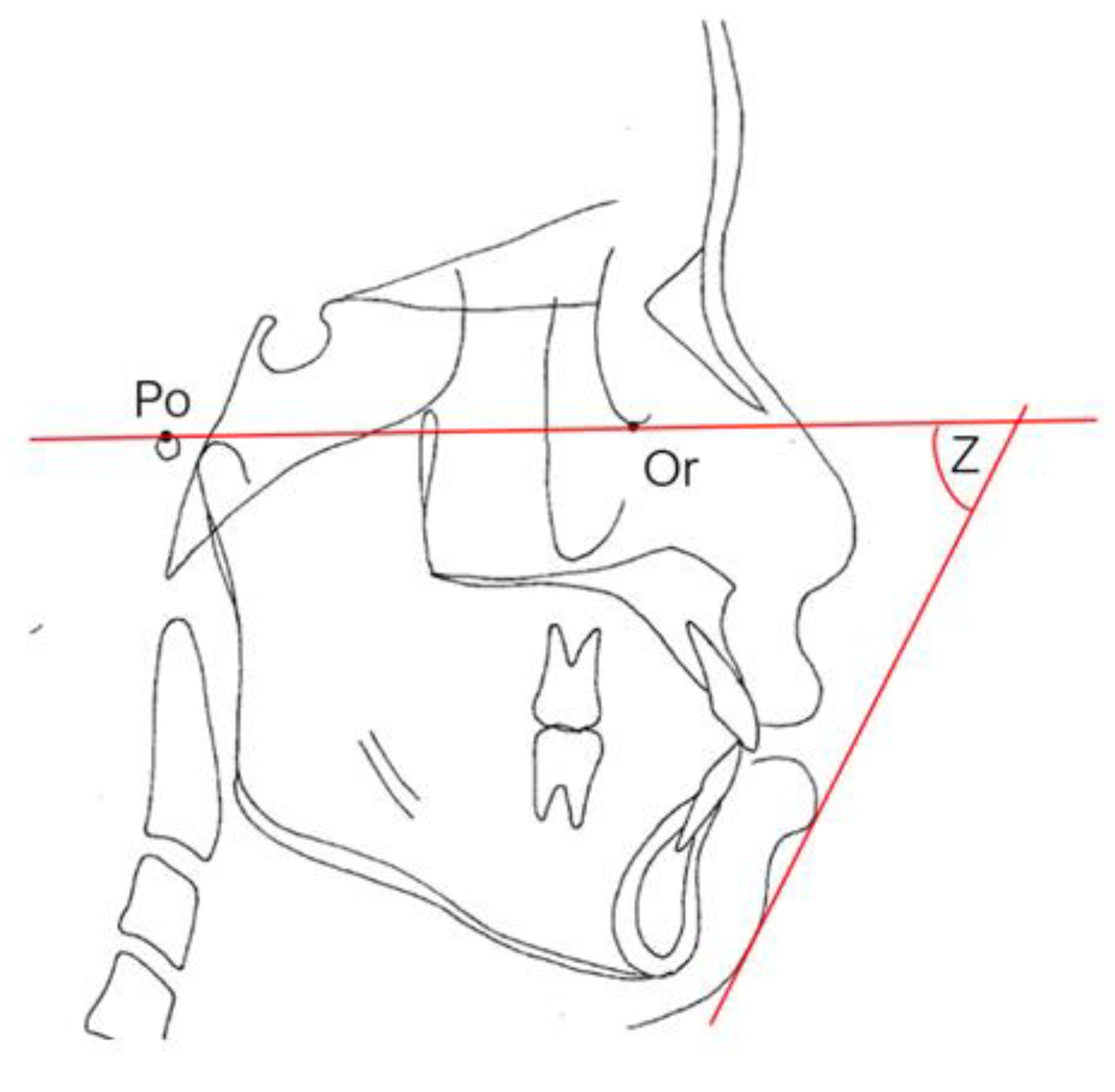
Table 6, the facial patterns of these 60 patients were within the average in the low margin (26.65 ± 5.53 for FMA, 35.62 ± 5.11 for SN-mandibular plane). There were no significant differences between the groups in terms of facial esthetic measurement using the Z angle, E-line to the upper lip, or the E-line to the lower lip (
p > 0.05).
Table 7 shows the comparison of urine cadmium concentrations in orthodontic patients with different FMAs. Patients were stratified into low (<27,
n = 34), average (27–34,
n = 23), and high (>34,
n = 3) FMA group. There were no statistically significant differences in the urine cadmium concentration among the three groups. Nevertheless, a marginally significant
p value of 0.05 for urine cadmium concentration was noted between patients with low FMA and patients with high FMA.
4. Discussion
The mean age of our subjects who were seeking orthodontic treatment was 25.07 years, range 20–35 years. Younger adults (aged 19–30 years) are more likely to seek orthodontic care according to the data from the Medical Expenditure Panel Survey in the United States [
46]. With reference to other national orthodontic patients, their mean age was 26.43 years in the United Kingdom [
47]. Trends in adult orthodontic patients have also been reported in Singapore, with a higher proportion of adult patients aged 21–25 years undergoing orthodontic treatment at the National Dental Centre Singapore from 2011 to 2017 [
48]. In contrast to the increase in adult patients in other countries, the Australian Society of Orthodontists recommends that children visit a registered specialist orthodontist for an assessment at approximately 7 years of age and that most cases in Australia be treated at ages 12–15. However, there has been an increase in the number of adults seeking orthodontic treatment in most countries. This phenomenon may be attributed to several factors, including esthetics, function and self-esteem, according to the literature findings. In addition to these insights, the improved appearance of braces and the invention of aligners may have increased patients’ motivation [
49].
Out of 60 orthodontic patients treated in our department, 51 (85%) of the subjects were female, whereas 15% were male. The majority of orthodontic patients are female in Korea (69.5%) [
50], and over 66% of patients in the USA are also female. [
46] The motivation of adult female patients seeking orthodontic treatment may include the need for esthetics, function and psychological factors such as self-perception, self-confidence, and avoiding negative thoughts about their teeth and criticism from others [
51].
According to our data, there were no significant differences in the DMFS index between patients with high urine cadmium concentrations and those with low urine cadmium concentrations. The average DMFS score was approximately 8.05, which is comparable to that of other countries, such as approximately 6.7 in the United States, 5 in Australia, 7.4 in Iran, 12.0 in Chile, 7.56 in Turkey, 10.8 in Belgium, and 12.5 in Spain [
52,
53,
54,
55,
56]. Our score is lower than that of European countries, similar to that of Middle-Eastern countries, and it is higher than that of Australia and the United States. Caries expressed as the mean DMFS at our clinic was relatively lower than that in most countries, which might be associated with the nature of the sample. The target patients, consisting of all persons planning for orthodontic treatment, were expected to pay more attention to tooth brushing and to maintain good oral hygiene. In addition, our filling index was higher than that of other countries, revealing that orthodontic patients are more focused on oral health management. The addition of fluoride to drinking water was carried out in the United States and Australia. Their DMFS data suggest that the fluoridation of drinking water can prevent dental caries.
The mean ICON score was 53.35 ± 9.01 for our sample. The ICON score was 44.6 in Iran [
57], 63.88 in the Netherlands by calibrated orthodontic [
58], 58.9 in South Asia, 57.3 for Americans, 56.6 for Australia, 55.8 for Africa, 52.4 for the Middle East, 50.3 for European countries, and 47.2 for North and East Asia [
59]. The cutoff value for treatment needed is 43, according to the paper of N.A. Fox and his coworkers published in the British Dental Journal in 2002 [
28]. Our data coincided with this range, and it is believed that the patients who need treatment have been properly treated at Chang Gung Memorial Hospital. The index of ICON offers several advantages, including the ability to assess the complexity of malocclusion and to estimate the treatment need and outcome with relatively high sensitivity and specificity. Despite these advantages, there are still some shortcomings. The cutoff points need to be adjusted in different countries due to the perception of treatment need. The occlusal indices do not cover all occlusal traits, and the assessments are opinion based [
60,
61]. In terms of facial esthetics other than the data from ICON, we also measured the Z angle and the lip protrusion (E-line to the upper lip and lower lip). The esthetic score from ICON is judged subjectively; in contrast, the Z angle and lip protrusion are obtained objectively by connecting the structures, including the nose, lips, and chin.
There were no significant differences regarding malocclusion in terms of dentition and skeleton between patients with high or low urine cadmium concentrations. There were also no significant differences between the groups in any dimension of the DMFS index. In summary, the previous hypothesis that cadmium may increase the caries rate and therefore may be correlated with subsequent malocclusion cannot be verified. It seems that previous cadmium pollution did not generate residual exposure in the local residents of Taoyuan city, and thereafter, the amount of cadmium detected in our patients was in the lower range of reported human cadmium urine concentrations.
Cadmium pollution can cause bone disease and affect bone quality and density on the basis of several literature searches [
62]. In other words, the amount of cadmium can be correlated with bone density. Therefore, the measurement of bone density and quality can be another indicator of exposure to cadmium in Chang Gung Memorial Hospital patients in addition to their urine test. According to previous studies [
26,
63], bone density is related to the facial shape. Among the three facial types (low, average, and high FMA), the patients with long faces tended to have a decreased bone density. In our research, we performed a statistical analysis for urine cadmium among these three facial types by pairwise comparisons, and indeed, there was a tendency for bone density to decrease among those with longer face shapes (
Table 3). There were no statistically significant differences in the urine cadmium concentration among the three FMA groups. Nevertheless, a marginally significant
p value of 0.05 for urine cadmium concentration was noted between patients with low FMA and patients with high FMA. However, there was still no conclusion about bone quality being associated with facial patterns because the sample sizes in the three groups were not equally distributed (the patients in the group with high FMA were only 3). Essentially, the facial pattern might be influenced by bone thickness and quality. Measuring the amount of cadmium in the body might also provide information on the tendency of facial growth patterns, which can be helpful in selecting orthodontic patients. To verify this statement, the collection of additional samples and computed tomography scans of the bone might be future research directions.
In general, the risk factors for dental caries formation include physical, biological, environmental, behavioral, and lifestyle factors such as cariogenic bacteria, a high sucrose diet, inadequate salivary flow, insufficient fluoride exposure, and poor oral hygiene [
64]. Therefore, this study is limited by the small sample size, lack of an equal distribution between sexes, short follow-up duration, and lack of traditional risk factor assessments. The potential limitation to the generalization of these results is the issue of sampling and selection. The sample did not reflect the general population due to the specific geographic scope of the experimental design, which aimed to investigate the cadmium exposure of local residents. A lack of previous research studies on this topic also provides only a limited theoretical foundation for the investigation.


 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}