
Immune Responses after Heavy Alcohol Consumption: Cytokine Concentrations in Hangover-Sensitive and Hangover-Resistant Drinkers

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Schrojenstein Lantman, M.; van de Loo, A.J.; Mackus, M.; Verster, J.C. Development of a definition for the alcohol hangover: Consumer descriptions and expert consensus. Curr. Drug Abuse Rev. 2016, 9, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Scholey, A.; van de Loo, A.J.A.E.; Benson, S.; Stock, A.-K. Updating the definition of the alcohol hangover. J. Clin. Med. 2020, 9, 823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penning, R.; McKinney, A.; Verster, J.C. Alcohol hangover symptoms and their contribution to the overall hangover severity. Alcohol Alcohol. 2012, 47, 248–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Schrojenstein Lantman, M.; Mackus, M.; van de Loo, A.J.A.E.; Verster, J.C. The impact of alcohol hangover symptoms on cognitive and physical functioning, and mood. Hum. Psychopharmacol. 2017, 32, e2623. [Google Scholar] [CrossRef]
- Verster, J.C.; Bervoets, A.C.; de Klerk, S.; Vreman, R.A.; Olivier, B.; Roth, T.; Brookhuis, K.A. Effects of alcohol hangover on simulated highway driving performance. Psychopharmacology 2014, 231, 2999–3008. [Google Scholar] [CrossRef]
- Alford, C.; Broom, C.; Carver, H.; Johnson, S.; Lands, S.; Reece, R.; Verster, J.C. The impact of alcohol hangover on simulated driving performance during a ‘commute to work’—Zero and residual alcohol effects compared. J. Clin. Med. 2020, 9, 1435. [Google Scholar] [CrossRef]
- McKinney, A. A review of the next day effects of alcohol on subjective mood ratings. Curr. Drug Abuse Rev. 2010, 3, 88–91. [Google Scholar] [CrossRef]
- Verster, J.C.; Arnoldy, L.; van de Loo, A.J.A.E.; Benson, S.; Scholey, A.; Stock, A. The impact of mood and subjective intoxication on hangover severity. J. Clin. Med. 2020, 9, 2462. [Google Scholar] [CrossRef]
- Van de Loo, A.J.A.E.; Mackus, M.; Kwon, O.; Krishnakumar, I.; Garssen, J.; Kraneveld, A.D.; Scholey, A.; Verster, J.C. The inflammatory response to alcohol consumption and its role in the pathology of alcohol hangover. J. Clin. Med. 2020, 9, 2081. [Google Scholar] [CrossRef]
- Mackus, M.; van de Loo, A.J.E.A.; Garssen, J.; Kraneveld, A.D.; Scholey, A.D.; Verster, J.C. The role of alcohol metabolism in the pathology of alcohol hangover. J. Clin. Med. 2020, 9, 3421. [Google Scholar] [CrossRef]
- Maier, S.F. Bi-directional immune-brain communication: Implications for understanding stress, pain and cognition. Brain Behav. Immun. 2003, 17, 69–85. [Google Scholar] [CrossRef]
- Maier, S.F.; Watkins, L.R. Cytokines for psychologists: Implications of bidirectional immune-to-brain communication for understanding behavior, mood, and cognition. Psychol. Rev. 1998, 105, 83–107. [Google Scholar] [CrossRef] [PubMed]
- Parnet, P.; Amindari, S.; Wu, C.; Brunke-Reese, D.; Goujon, E.; Weyhenmeyer, J.A.; Dantzer, R.; Kelley, K.W. Expression of type I and type II interleukin-1 receptors in mouse brain. Mol. Brain Res. 1994, 27, 63–70. [Google Scholar] [CrossRef]
- Dantzer, R.; Bluthe, R.M.; Laye, S.; Bret-Dibat, J.-L.; Partnet, P.; Kelley, K.W. Cytokines and sickness behavior. Ann. N. Y. Acad. Sci. 1998, 840, 586–590. [Google Scholar] [CrossRef] [PubMed]
- Dantzer, R.; Kelley, K.W. Twenty years of research on cytokine-induced sickness behavior. Brain Behav. Immun. 2007, 21, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afshar, M.; Richards, S.; Mann, D.; Cross, A.; Smith, G.B.; Netzer, G.; Kovacs, E.; Hasday, J. Acute immunomodulatory effects of binge alcohol ingestion. Alcohol 2015, 49, 57–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neupane, S.P.; Skulberg, A.; Skulberg, K.R.; Aass, H.C.; Bramness, J.G. Cytokine changes following acute ethanol intoxication in healthy men: A crossover study. Mediat. Inflamm. 2016, 2016, 3758590. [Google Scholar] [CrossRef]
- Kim, D.J.; Kim, W.; Yoon, S.J.; Choi, B.M.; Kim, J.S.; Go, H.J.; Kim, Y.K.; Jeong, J. Effects of alcohol hangover on cytokine production in healthy subjects. Alcohol 2003, 31, 167–170. [Google Scholar] [CrossRef]
- Kim, H.; Kim, Y.J.; Jeong, H.Y.; Kim, J.Y.; Choi, E.K.; Chae, S.W.; Kwon, O. A standardized extract of the fruit of Hovenia dulcis alleviated alcohol-induced hangover in healthy subjects with heterozygous ALDH2: A randomized, controlled, crossover trial. J. Ethnopharmacol. 2017, 209, 167–174. [Google Scholar] [CrossRef]
- Mammen, R.R.; Natinga Mulakal, J.; Mohanan, R.; Maliakel, B.; Krishnakumar, I.M. Clove bud polyphenols alleviate alterations in inflammation and oxidative stress markers associated with binge drinking: A randomized double-blinded placebo-controlled crossover study. J. Med. Food 2018, 21, 1188–1196. [Google Scholar] [CrossRef]
- Howland, J.; Rohsenow, D.J.; Edwards, E.M. Are some drinkers resistant to hangover? A literature review. Curr. Drug Abuse Rev. 2008, 1, 42–46. [Google Scholar] [CrossRef]
- Verster, J.C.; de Klerk, S.; Bervoets, A.C.; Kruisselbrink, D. Can Hangover Immunity be Really Claimed? Curr. Drug Abuse Rev. 2013, 6, 253–254. [Google Scholar] [CrossRef]
- Kruisselbrink, L.D.; Bervoets, A.C.; de Klerk, S.; van de Loo, A.J.A.E.; Verster, J.C. Hangover resistance in a Canadian university student population. Addict. Behav. Rep. 2017, 5, 14–18. [Google Scholar] [CrossRef]
- Terpstra, C.; Benson, S.; Verster, J.C.; Scholey, A. Prevalence of hangover resistance according to two methods for calculating estimated blood alcohol concentration (eBAC). J. Clin. Med. 2020, 9, 2923. [Google Scholar] [CrossRef]
- Hogewoning, A.; van de Loo, A.J.A.E.; Mackus, M.; Raasveld, S.J.; De Zeeuw, R.; Bosma, E.R.; Bouwmeester, N.H.; Brookhuis, K.A.; Garssen, J.; Verster, J.C. Characteristics of social drinkers with and without a hangover after heavy alcohol consumption. Subs. Abuse Rehab. 2016, 7, 161–167. [Google Scholar] [CrossRef] [Green Version]
- Verster, J.C.; van de Loo, A.J.A.E.; Adams, S.; Stock, A.-K.; Benson, S.; Alford, C.; Scholey, A.; Bruce, G. Advantages and limitations of naturalistic study designs and their implementation in alcohol hangover research. J. Clin. Med. 2019, 8, 2160. [Google Scholar] [CrossRef] [Green Version]
- Verster, J.C.; van de Loo, A.J.A.E.; Benson, S.; Scholey, A.; Stock, A.-K. The assessment of overall hangover severity. J. Clin. Med. 2020, 9, 786. [Google Scholar] [CrossRef] [Green Version]
- Watson, P.E.; Watson, I.D.; Batt, R.D. Prediction of blood alcohol concentrations in human subjects. Updating the Widmark Equation. J. Stud. Alcohol 1981, 42, 547–556. [Google Scholar] [CrossRef]
- Prat, G.; Adan, A.; Sánchez-Turet, M. Alcohol hangover: A critical review of explanatory factors. Hum. Psychopharmacol. 2009, 24, 259–267. [Google Scholar] [CrossRef]
- Penning, R.; van Nuland, M.; Fliervoet, L.A.; Olivier, B.; Verster, J.C. The pathology of alcohol hangover. Curr. Drug Abuse Rev. 2010, 3, 68–75. [Google Scholar] [CrossRef]
- Tipple, C.; Benson, S.; Scholey, A. A review of the physiological factors associated with an alcohol-induced hangover. Curr. Drug Abuse Rev. 2017, 9, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Palmer, E.; Tyacke, R.; Sastre, M.; Lingford-Hughes, A.; Nutt, D.; Ward, R.J. Alcohol hangover: Underlying biochemical, inflammatory and neurochemical mechanisms. Alcohol Alcohol. 2019, 54, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Mackus, M.; van de Loo, A.J.A.E.; Korte-Bouws, G.A.H.; van Neer, R.H.P.; Wang, X.; Nguyen, T.T.; Brookhuis, K.A.; Garssen, J.; Verster, J.C. Urine methanol concentration and alcohol hangover severity. Alcohol 2017, 59, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Mackus, M.; van de Loo, A.J.A.E.; Raasveld, S.J.; Hogewoning, A.; Sastre Toraño, J.; Flesch, F.M.; Korte-Bouws, G.A.H.; van Neer, R.H.P.; Wang, X.; Nguyen, T.T.; et al. Biomarkers of the alcohol hangover state: Ethyl glucuronide (EtG) and ethyl sulfate (EtS). Hum. Psychopharmacol. 2017, 32. [Google Scholar] [CrossRef] [Green Version]
- Van de Loo, A.J.A.E.; Mackus, M.; Korte-Bouws, G.A.H.; Brookhuis, K.A.; Garssen, J.; Verster, J.C. Urine ethanol concentration and alcohol hangover severity. Psychopharmacology 2017, 234, 73–77. [Google Scholar] [CrossRef] [Green Version]
- Mackus, M.; van Schrojenstein Lantman, M.; van de Loo, A.J.A.E.; Brookhuis, K.A.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Alcohol metabolism in hangover sensitive versus hangover resistant social drinkers. Drug Alcohol Depend. 2018, 185, 351–355. [Google Scholar] [CrossRef]
- Mackus, M.; van de Loo, A.J.E.A.; Garssen, J.; Kraneveld, A.D.; Scholey, A.; Verster, J.C. The association between ethanol elimination rate and hangover severity. Int. J. Environ. Res. Public Health 2020, 17, 4324. [Google Scholar] [CrossRef]
- Verster, J.C.; Stam, N.; Sterk, A.Y.; van de Loo, A.J.A.E.; Mackus, M.; Balikji, S.; Kraneveld, A.D.; Scholey, A.; Garssen, J. Food intake before, during, and after a heavy drinking session. Alcohol. Clin. Exp. Res. 2018, 42 (Suppl. S1), 52A. [Google Scholar]
- Verster, J.C.; Vermeulen, S.A.; van de Loo, A.J.A.E.; Balikji, S.; Kraneveld, A.D.; Garssen, J.; Scholey, A. Dietary nutrient intake, alcohol metabolism, and hangover severity. J. Clin. Med. 2019, 8, 1316. [Google Scholar] [CrossRef] [Green Version]
- Kösem, Z.; van de Loo, A.J.A.E.; Fernstrand, A.M.; Garssen, J.; Verster, J.C. The impact of consuming food or drinking water on alcohol hangover. Eur. Neuropsychopharmacol. 2015, 25 (Suppl. S2), S604. [Google Scholar] [CrossRef]
- Verster, J.C.; Anogeianaki, A.; Kruisselbrink, L.D.; Alford, C.; Stock, A.-K. Relationship of alcohol hangover and physical endurance performance: Walking the Samaria Gorge. J. Clin. Med. 2020, 9, 114. [Google Scholar] [CrossRef] [Green Version]
- Gorodischer, R.; Burtin, P.; Hwang, P.; Levine, M.; Koren, G. Saliva versus blood sampling for therapeutic drug monitoring in children: Patient and parental preferences and an economic analysis. Ther. Drug Monit. 1994, 16, 437–443. [Google Scholar] [CrossRef]
- Dhima, M.; Salinas, T.J.; Wermers, R.A.; Weaver, A.L.; Koka, S. Preference changes of adult outpatients for giving saliva, urine and blood for clinical testing after actual sample collection. J. Prosthodont. Res. 2013, 57, 51–56. [Google Scholar] [CrossRef]
- Ouellet-Morin, I.; Danese, A.; Williams, B.; Arseneault, L. Validation of a high-sensitivity assay for C-reactive protein in human saliva. Brain Behav. Immun. 2011, 25, 640–646. [Google Scholar] [CrossRef]
- Riis, J.L.; Out, D.; Dorn, L.D.; Beal, S.J.; Denson, L.A.; Pabst, S.; Jaedicke, K.; Granger, D.A. Salivary cytokines in healthy adolescent girls: Intercorrelations, stability, and associations with serum cytokines, age, and pubertal stage. Dev. Psychobiol. 2014, 56, 797–811. [Google Scholar] [CrossRef] [Green Version]
- La Fratta, I.; Tatangelo, R.; Campagna, G.; Rizzuto, A.; Franceschelli, S.; Ferrone, A.; Patruno, A.; Speranza, L.; de Lutiis, M.A.; Felaco, M.; et al. The plasmatic and salivary levels of IL-1β, IL-18 and IL-6 are associated to emotional difference during stress in young male. Sci. Rep. 2018, 8, 3031. [Google Scholar] [CrossRef] [Green Version]
- Pasala, S.; Barr, T.; Messaoudi, I. Impact of alcohol abuse on the adaptive immune system. Alcohol Res. 2015, 37, 185–197. [Google Scholar]
- McKinney, A.; Coyle, K. Alcohol hangover effects on measures of affect the morning after a normal night’s drinking. Alcohol Alcohol. 2006, 41, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verster, J.C.; van Schrojenstein Lantman, M.; Mackus, M.; van de Loo, A.J.A.E.; Garssen, J.; Scholey, A. Differences in the temporal typology of alcohol hangover. Alcohol. Clin. Exp. Res. 2018, 2, 691–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakao, A. Temporal regulation of cytokines by the circadian clock. J. Immunol. Res. 2014, 2014, 614529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, P.W.; Nambiar, S.; Muhardi, L.; Abdul Kader, U.H.; Garssen, J.; Sandalova, E. Young children display diurnal patterns of salivary IgA and alpha-amylase expression which are independent of food intake and demographic factors. BioMed Res. Int. 2019, 2019, 3687416. [Google Scholar] [CrossRef]


{kind=link}
| Demographics | All Participants | Hangover-Resistant | Hangover-Sensitive | p-Value |
|---|---|---|---|---|
| N | 35 | 18 | 17 | |
| Male/female | 13/22 | 8/10 | 6/11 | |
| Age (year) | 21.1 (1.8) | 20.8 (2.0) | 21.4 (1.6) | 0.356 |
| Height (m) | 1.77 (0.1) | 1.78 (0.1) | 1.76 (0.1) | 0.397 |
| Weight (kg) | 68.5 (10.3) | 71.1(10.2) | 65.8 (1.0) | 0.126 |
| BMI (kg/m2) | 21.9 (2.2) | 21.4 (2.3) | 22.3 (2.0) | 0.186 |
| Alcoholic units consumed | 11.0 (5.1) | 10.7 (4.7) | 11.3 (5.6) | 0.715 |
| Estimated BAC (%) | 0.17 (0.7) | 0.17 (0.07) | 0.17 (0.07) | 0.701 |
| Test Day | Post-Alcohol Day | Control Day | |||
|---|---|---|---|---|---|
| Cytokine | Mean (SD) | % Below LOD | Mean (SD) | % Below LOD | p-Value |
| IL-1β | 158.7 (205.9) | 0.0% (0/35) | 198.4 (413.6) | 0.0% (0/35) | 0.523 |
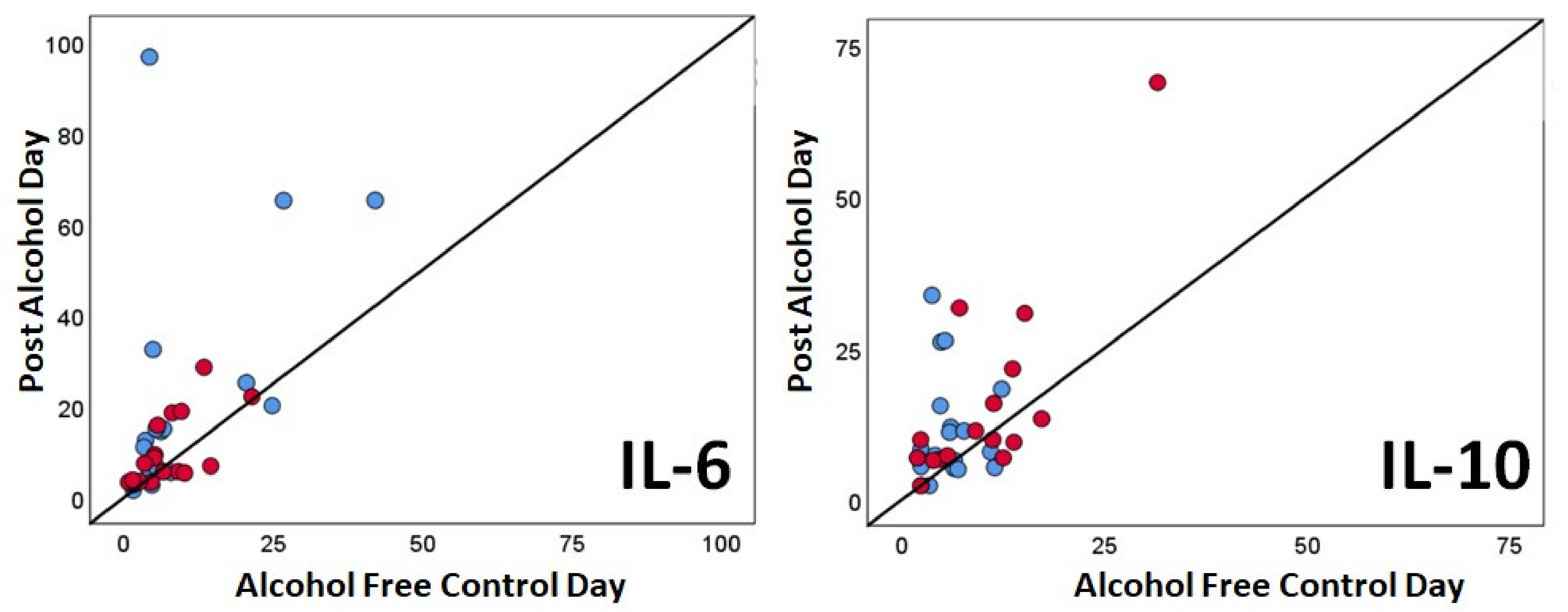
| IL-6 | 16.4 (20.5) | 2.9% (1/35) | 8.6 (8.8) | 2.9% (1/35) | 0.001 * |
| IL-8 | 584.3 (668.8) | 0.0% (0/35) | 809.3 (1725.0) | 0.0% (0/35) | 0.342 |
| IL-10 | 13.7 (12.9) | 5.7% (2/35) | 7.8 (5.9) | 17.1% (5/35) | 0.001 * |
| TNF-α | 85.2 (51.1) | 0.0% (0/35) | 70.6 (46.5) | 0.0% (0/35) | 0.038 |
| Hangover-Resistant Group (N = 18) | Hangover-Sensitive Group (N = 17) | |||||
|---|---|---|---|---|---|---|
| Cytokine | Post-Alcohol Mean (SD) | Control Day Mean (SD) | p-Value | Post-Alcohol Mean (SD) | Control Day Mean (SD) | p-Value |
| IL-1β | 179.4 (196.8) | 148.1 (237.2) | 0.732 | 136.7 (219.0) | 251.6 (545.8) | 0.981 |
| IL-6 | 22.4 (26.6) | 9.8 (11.2) | 0.005 * | 10.1 (7.6) | 7.4 (5.4) | 0.084 |
| IL-8 | 582.3 (614.6) | 626.7 (1004.7) | 0.472 | 586.4 (741.0) | 1002.7 (2274.6) | 0.523 |
| IL-10 | 12.0 (8.8) | 6.0 (3.1) | 0.011 | 15.4 (16.2) | 9.8 (7.6) | 0.041 |
| TNF-α | 79.6 (42.2) | 62.9 (38.3) | 0.048 | 91.2 (59.8) | 78.8 (53.8) | 0.332 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van de Loo, A.J.; Raasveld, S.J.; Hogewoning, A.; Zeeuw, R.d.; Bosma, E.R.; Bouwmeester, N.H.; Lukkes, M.; Knipping, K.; Mackus, M.; Kraneveld, A.D.; et al. Immune Responses after Heavy Alcohol Consumption: Cytokine Concentrations in Hangover-Sensitive and Hangover-Resistant Drinkers. Healthcare 2021, 9, 395. https://doi.org/10.3390/healthcare9040395
van de Loo AJ, Raasveld SJ, Hogewoning A, Zeeuw Rd, Bosma ER, Bouwmeester NH, Lukkes M, Knipping K, Mackus M, Kraneveld AD, et al. Immune Responses after Heavy Alcohol Consumption: Cytokine Concentrations in Hangover-Sensitive and Hangover-Resistant Drinkers. Healthcare. 2021; 9(4):395. https://doi.org/10.3390/healthcare9040395
Chicago/Turabian Stylevan de Loo, Aurora JAE, S. Jorinde Raasveld, Anna Hogewoning, Raymond de Zeeuw, Else R Bosma, Noor H Bouwmeester, Melanie Lukkes, Karen Knipping, Marlou Mackus, Aletta D Kraneveld, and et al. 2021. "Immune Responses after Heavy Alcohol Consumption: Cytokine Concentrations in Hangover-Sensitive and Hangover-Resistant Drinkers" Healthcare 9, no. 4: 395. https://doi.org/10.3390/healthcare9040395