
The Effect of Nordic Walking Training with Poles with an Integrated Resistance Shock Absorber on the Body Balance of Women over the Age of 60

 , , and
, , and
Abstract
:1. Introduction
2. Methods
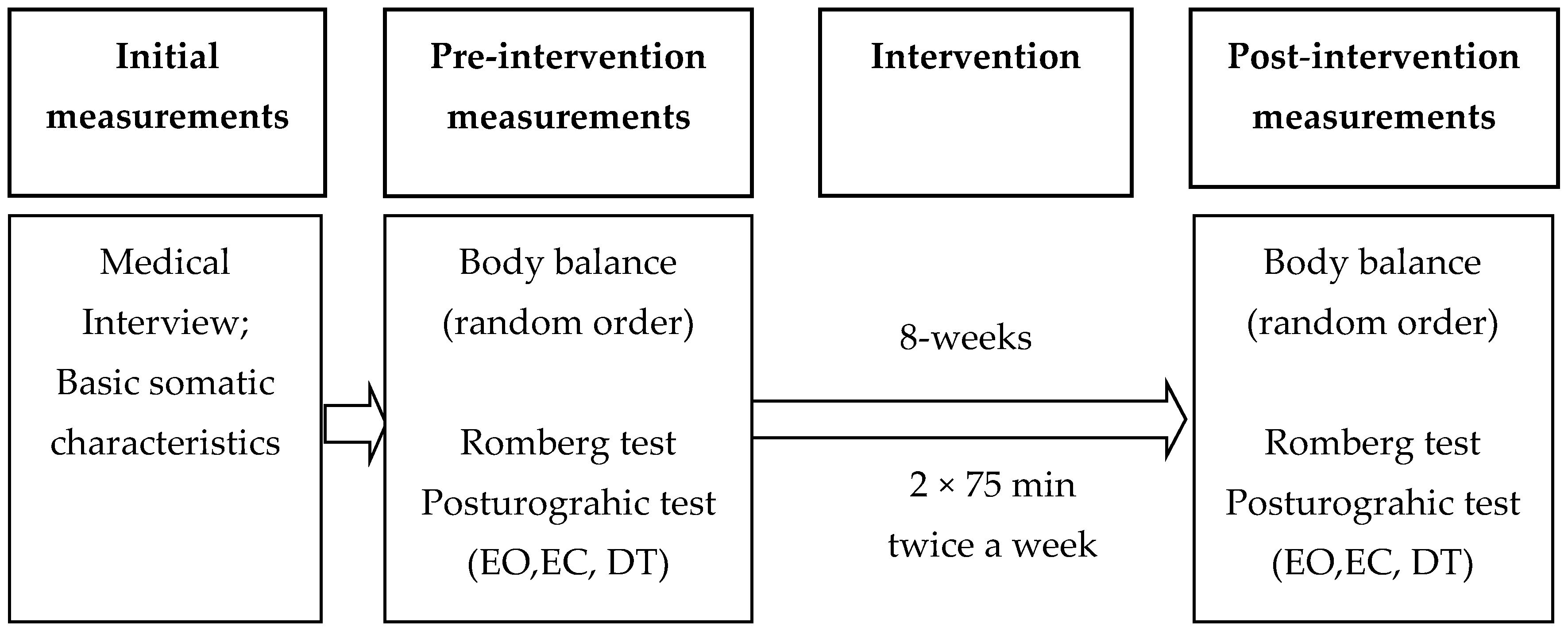
2.1. Study Design
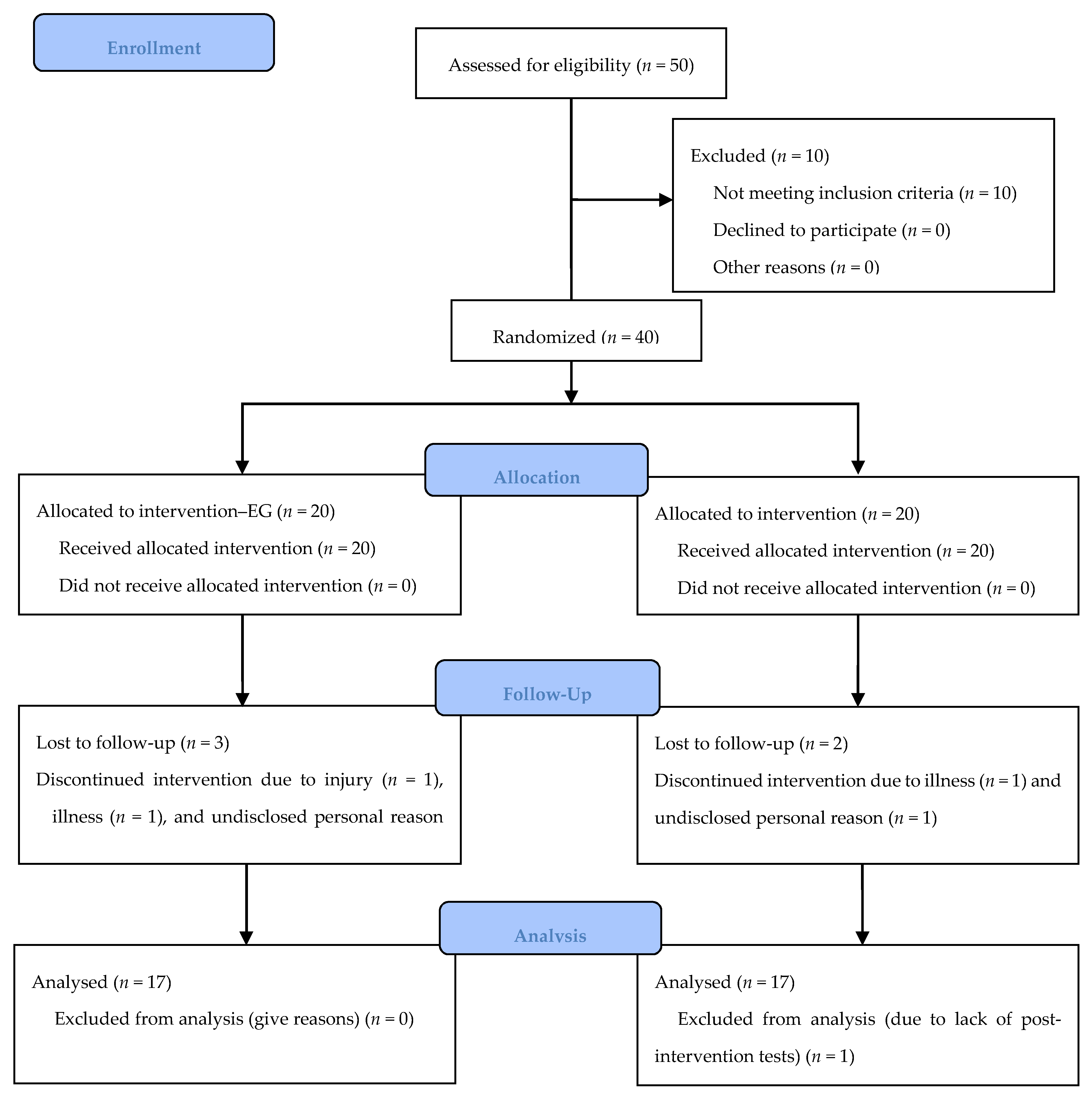
2.2. Participants
2.3. Intervention
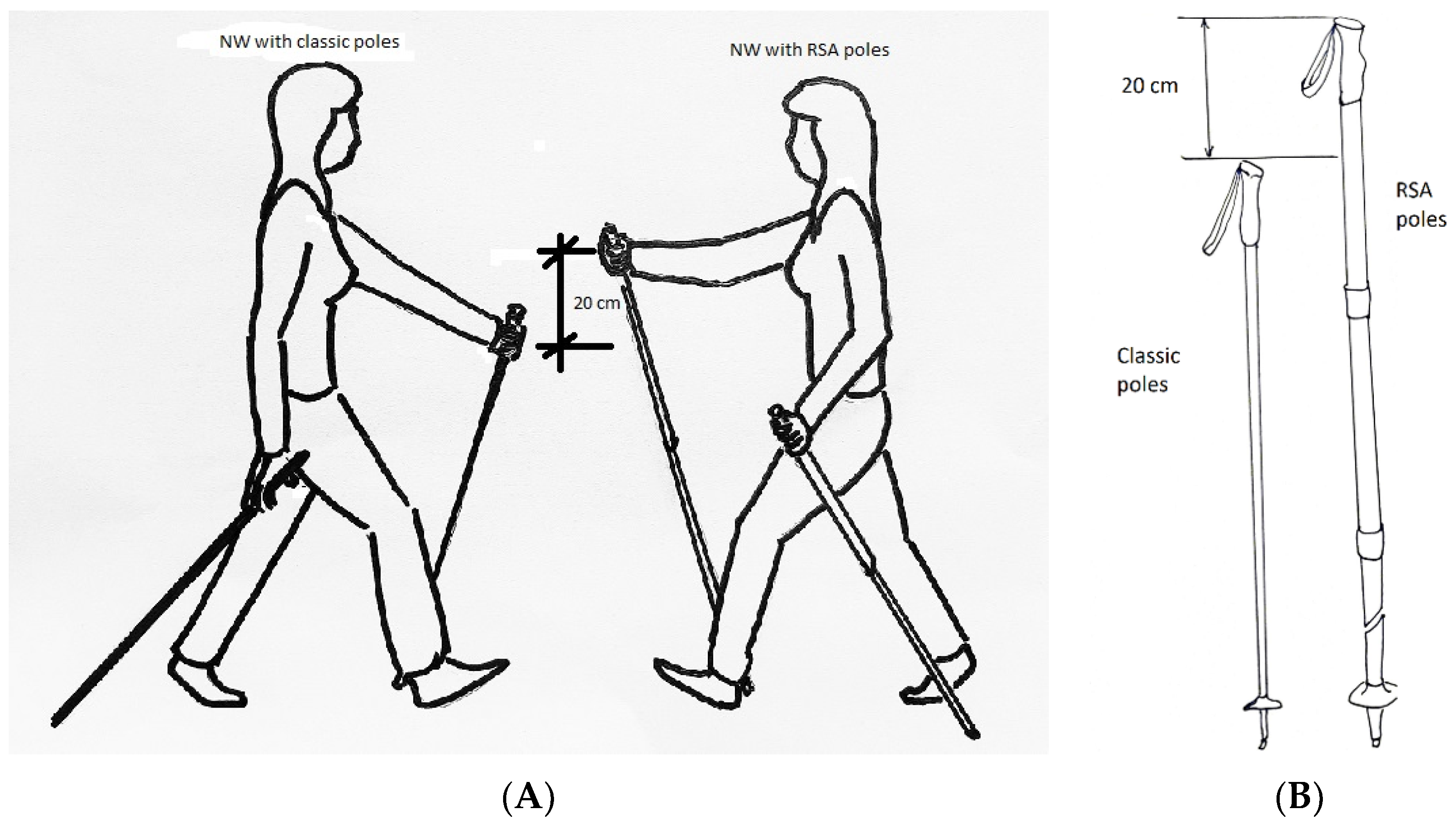
2.4. Walking Technique with the Use of Poles
2.5. Measurements
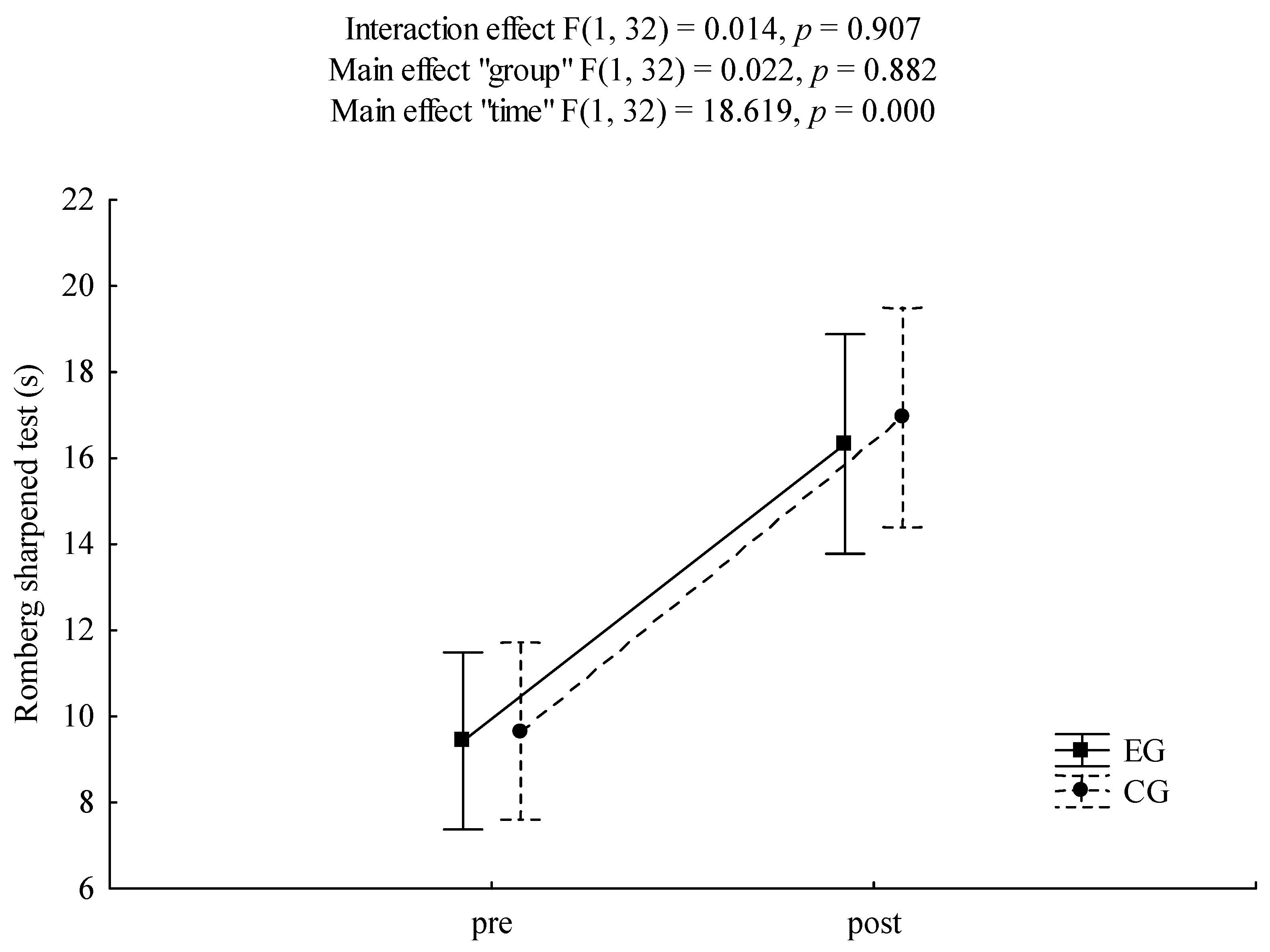
2.5.1. Romberg Sharpened Test
2.5.2. Posturography Measurements
- -
- standing with the eyes open (EO),
- -
- standing with the eyes closed (EC),
- -
- testing body stability under dual task (DT) conditions.
2.6. Outcomes
- (a)
- number of seconds during which the subject held the position without losing balance in Romberg test;
- (b)
- average velocity of COP displacements (and its components in anterior-posterior and medio-lateral directions), as well as ellipse area of 95% in posturographic measurements.
2.7. Sample Size and Randomization
2.8. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fahn, S.; Jankovic, J. Principles and Practice of Movement Disorders; Churchill Livingstone: Philadelphia, PA, USA, 2007; ISBN 9780443079412. [Google Scholar]
- Maranhão-Filho, P.A.; Maranhão, E.T.; da Silva, M.M.; Lima, M.A. Rethinking the neurological examination I: Static balance assessment. Arq. Neuro Psiquiatr. 2011, 69, 954–958. [Google Scholar] [CrossRef] [Green Version]
- Michalska, J.; Kamieniarz, A.; Sobota, G.; Stania, M.; Juras, G.; Słomka, K. Age-related changes in postural control in older women: Transitional tasks in step initiation. BMC Geriatr. 2021, 21, 17. [Google Scholar] [CrossRef] [PubMed]
- Callisaya, M.; Blizzard, L.; Schmidt, M.-D.; Martin, K.L.; Mcginley, J.L.; Sanders, L.M.; Srikanth, V.K. Gait, gait variability and the risk of multiple incident falls in people: A population-based study. Age Ageing 2011, 40, 481–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sample, R.B.; Jackson, K.; Kinney, A.L.; Wiebke, S.; Diestelkamp, W.S.; Reinert, S.S.; Bigelow, K.E. Manual and Cognitive Dual Tasks Contribute to Fall-Risk Differentiation in Posturography Measures. J. Appl. Biomechan. 2016, 32, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Barak, Y.; Wagenaar, R.C.; Holt, K.G. Gait characteristics of elderly people with a history of falls: A dynamic approach. Phys. Ther. 2006, 86, 1501–1510. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, S.; Schumacher, V. The Interplay between Cognitive and Motor Functioning in Healthy Adults: Findings from Dual-Task Studies and Suggestions for Intervention. Gerontology 2011, 57, 239–246. [Google Scholar] [CrossRef] [Green Version]
- Chase, J.A.D. Physical Activity Interventions among Adults: A Literature Review. Res. Theory NursPract. 2013, 27, 53–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milanović, Z.; Pantelić, S.; Trajković, N.; Sporiš, G.; Kostić, R.; James, N. Age-related decrease in physical activity and functional fitness among elderly men and women. Clin. Interv. Aging 2013, 8, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Halaweh, H.; Willen, C.; Grimby-Ekman, A.; Svantesson, U. Physical Activity and Health-Related Quality of Life among Community Dwelling Elderly. J. Clin. Med. Res. 2015, 7, 845–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langhammer, B.; Bergland, A.; Rydwik, E. The Importance of Physical Activity Exercise among People. Biomed. Res. Int. 2018, 7856823. [Google Scholar] [CrossRef]
- Fahey, T.D.; Insel, P.; Roth, T. Fit & Well: Core Concepts and Labs in Physical Fitness and Wellness; McGraw Hill: New York, NY, USA, 2018; ISBN 10:1260397130. [Google Scholar]
- Rivera-Torres, S.; Fahey, T.D.; Rivera, M.A. Adherence to Exercise Programs in Adults: Informative Report. Gerontol. Geriatr. Med. 2019, 5, 1–10. [Google Scholar] [CrossRef]
- Yorston, L.C.; Rosenkranz, R.R.; Kolt, G.S. Physical Activity and Physical Function in Adults: The 45 and Up Study. J. Am. Geriatr. Soc. 2012, 60, 719–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, C.H.; Hwang, C.L.; Wu, Y.T. Effect of exercise on physical function, daily living activities, and quality of life in the frail adults: A meta-analysis. Arch. Phys. Med. Rehabil. 2012, 93, 237–244. [Google Scholar] [CrossRef]
- Wang, R.Y.; Wang, Y.L.; Cheng, F.C.; Chao, Y.H.; Chen, C.L.; Yang, Y.R. Effects of combined exercise on gait variability in community-dwelling older adults. Age 2015, 37, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrell, J.W.; Merkas, J.; Pilutti, L.A. The Effect of Exercise Training on Gait, Balance, and Physical Fitness Asymmetries in Persons With Chronic Neurological Conditions: A Systematic Review of Randomized Controlled Trials. Front. Physiol. 2020, 11, 585765. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, S.; Finch, L.; Mai, J.; Ahmed, S.; Huang, A.; Mayo, N.-E. Nordic walking for geriatric rehabilitation: A randomized pilot trial. Disabil. Rehabil. 2013, 35, 968–975. [Google Scholar] [CrossRef]
- Mansour, K.B.; Gorce, P.; Rezzoug, N. The impact of Nordic walking training on the gait of the elderly. J. Sport Sci. Med. 2018, 38, 2368–2374. [Google Scholar] [CrossRef] [PubMed]
- Virag, A.; Karoczi, C.K.; Jakab, Á.; Vass, Z.; Kovács, É.; Gondos, T. Short-term and long-term effects of nordic Walking on balance, functional mobility, muscle strength and aerobic endurance among Hungarian community-living people: A feasibility study. J. Sports Med. Phys. Fitness. 2014, 55, 1285–1292. [Google Scholar] [PubMed]
- Song, M.S.; Yoo, Y.K.; Choi, C.H.; Kim, N.C. Effects of nordic walking on body composition, muscle strength, and lipid profile in elderly women. Asian Nurs. Res. Korean Soc. Nurs. Sci. 2013, 7, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Keogh, J.; Rice, J.; Taylor, D.; Kilding, A. Objective benefits, participant perceptions and retention rates of a New Zealand community-based, -adult exercise programme. J. Prim. Health Care 2014, 1172–6164. [Google Scholar] [CrossRef]
- Lee, H.S.; Park, J.H. Effects of Nordic walking on physical functions and depression in frail people aged 70 years and above. J. Phys. Ther. Sci. 2015, 27, 2453–2456. [Google Scholar] [CrossRef] [Green Version]
- Franzoni, L.T.; Monteiro, E.P.; Oliveira, H.B.; da Rosa, R.G.; Costa, R.R.; Rieder, K.; Martinez, F.G.; Peyré-Tartaruga, L.A. A 9-Week Nordic and Free Walking Improve Postural Balance in Parkinson’s Disease. Sports Med. Int. Open 2018, 2, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Kocur, P.; Wiernicka, M.; Wilski, M.; Kamińska, E.; Furmaniuk, L.; Flis- Masłowska, M.; Lewandowski, J. Does Nordic walking improves the postural control and gait parameters of women between the age 65 and 74: A randomized trial. J. Phys. Ther. Sci. 2015, 27, 3733–3737. [Google Scholar] [CrossRef] [Green Version]
- Gomeñuka, N.A.; Oliveira, H.B.; Silva, E.S.; Costa, R.R.; Kanitz, A.C.; Liedtke, G.V.; Schuch, F.B.; Peyre-Tartaruga, L.-A. Effects of Nordic walking training on quality of life, balance and functional mobility in elderly: A randomized clinical trial. PLoS ONE 2019, 14, 0211472. [Google Scholar] [CrossRef]
- Marciniak, K.; Maciaszek, J.; Cyma-Wejchenig, M.; Szeklicki, R.; Maćkowiak, Z.; Sadowska, D.; Stemplewski, R. The Effect of Nordic Walking Training with Poles with an Integrated Resistance Shock Absorber on the Functional Fitness of Women over the Age of 60. Int. J. Environ. Res. Public Health 2020, 17, 2197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American College of Sports Medicine. ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription. 7; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Behm, D.G.; Muehlbauer, T.; Kibele, A.; Granacher, U. Effects of Strength Training Using Unstable Surfaces on Strength, Power and Balance Performance Across the Lifespan: A Systematic Review and Meta-analysis. Sports Med. 2015, 45, 1645–1669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.D.; Yu, S.H. The effects of Nordic and general walking on depression disorder patients’ depression, sleep, and body composition. J. Phys. Ther. Sci. 2015, 27, 2481–2485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padulo, J.; Iuliano, E.; Iacono, A.D.; Milić, M.; Rizzi, M.; Ardigò, L.P. Nordic walking versus natural walking: An easy approach to comparing metabolic demands. Int. J. Perf. Anal. Sport 2018, 18, 686–692. [Google Scholar] [CrossRef]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S.; American College of Sport Medicine Position Stand. Exercise and physical activity for adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef]
- Lee, C.T. Sharpening the Sharpened Romberg. SPUMS J. 1998, 28, 125–132. [Google Scholar]
- Herdman, S.J.; Clendaniel, R.A. Vestibular Rehabilitation: A Competency-Based Course; Department of Rehabilitation Medicine; Emory Physical Therapy Association: Atlanta, GA, USA, 2010; Available online: https://www.emorydpt.org/wp-content/uploads/2017/05/Vestibular2018_PlanningOnly_4.21.2017.pdf (accessed on 22 February 2021).
- Melzer, I.; Marx, R.; Kurz, I. Regular exercise in the elderly is effective to preserve the speed of voluntary stepping under single-task condition but not under dual-task condition. A case-control study. Gerontology 2009, 55, 49–57. [Google Scholar] [CrossRef] [PubMed]
- McNamara, A.J.; Pavol, M.J.; Gunter, K.B. Meeting physical activity guidelines through community-based group exercise: “Better bones and balance”. J. Aging Phys. Act. 2013, 21, 155–166. [Google Scholar] [CrossRef]
- Stemplewski, R. Effect of moderate physical exercise on postural control among 65–74 years old man. Arch. Gerontol. Geriatr. 2012, 54, 279–283. [Google Scholar] [CrossRef]
- Stemplewski, R.; Maciaszek, J.; Osiński, W.; Szeklicki, R. Test-Retest Reliability of Measurements of the Center of Pressure Displacement in Quiet Standing and During Maximal Voluntary Body Leaning Among Healthy Elderly Men. J. Hum. Kinet. 2011, 28, 15–23. [Google Scholar] [CrossRef]
- Takeshima, N.; Islam, M.M.; Rogers, M.E.; Rogers, N.L.; Sengoku, N.; Koizumi, D.; Kitabayashi, Y.; Imai, A.; Naruse, A. Effects of nordic walking compared to conventional walking and band-based resistance exercise on fitness in adults. J. Sport Sci. Med. 2013, 12, 422–430. [Google Scholar] [PubMed]
- Chomiuk, T.; Folga, A.; Mamcarz, A. The influence of systematic pulse-limited physical exercise on the parameters of the cardiovascular system in patients over 65 years of age. Arch. Med. Sci. 2013, 9, 201–209. [Google Scholar] [CrossRef]
- Lajoie, Y. Effect of computerized feedback postural training on posture and attentional demands in older adults. Aging Clin. Exp. Res. 2004, 16, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Gobbo, S.; Bergamin, M.; Sieverdes, J.C.; Ermolao, A.; Zaccaria, M. Effects of exercise on dual-task ability and balance in older adults: A systematic review. Arch. Gerontol. Geriatr. 2014, 58, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Stemplewski, R.; Maciaszek, J.; Tomczak, M.; Szeklicki, R.; Sadowska, S.; Osiński, W. Habitual physical activity as a determinant of the effect of moderate physical exercise on postural control in older men. Am. J. Mens Health 2013, 7, 58–65. [Google Scholar] [CrossRef]
- Handrigan, G.A.; Berrigan, F.; Hue, O.; Simoneau, M.; Corbeil, P.; Tremblay, A.; Teasdale, N. The effects of muscle strength on center of pressure-based measures of postural sway in obese and heavy athletic individuals. Gait Posture 2012, 35, 88–91. [Google Scholar] [CrossRef]
- Capodaglio, P.; Cimolin, V.; Tacchini, E.; Parisio, C.; Galli, M. Balance Control and Balance Recovery in Obesity. Ergonomy 2012, 1, 166–173. [Google Scholar] [CrossRef] [Green Version]
- Carral, J.M.C.; Ayán, C.; Sturzinger, L. Relationships between Body Mass Index and Static and Dynamic balance in active and inactive older adults. J. Geriatr. Phys. Ther. 2019, 42, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35, 7–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EG (n = 20) | CG (n = 20) | t (p) | |||
|---|---|---|---|---|---|
| Measure | M | SD | M | SD | |
| Age (years) | 67.71 | 4.16 | 65.88 | 4.09 | 1.29(0.207) |
| Body height (cm) | 161.94 | 4.04 | 159.25 | 5.45 | 1.64(0.112) |
| Body weight (kg) | 74.31 | 11.17 | 65.63 | 11.19 | 2.26(0.030) |
| BMI (kg/m2) | 28.31 | 3.90 | 25.90 | 4.53 | 1.66(0.106) |
| Pre | Post | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | M (sd) EG | M (sd) CG | M (sd) EG | M (sd) CG | Interaction F(p) | ɳ2 | Group F(p) | ɳ 2 | Time F(p) | ɳ 2 |
| EO | ||||||||||
| Vcop [cm/s] | 1.14(0.46) | 0.99(0.31) | 1.17(0.43) | 1.04(0.26) | 0.03(>0.05) | 0.00 | 1.41(>0.05) | 0.04 | 0.62(>0.05) | 0.02 |
| VcopY [cm/s] | 0.95(0.46) | 0.83(0.29) | 0.96(0.41) | 0.81(0.20) | 0.23(>0.05) | 0.01 | 1.33(>0.05) | 0.04 | 0.01(>0.05) | 0.00 |
| VcopX [cm/s] | 0.45(0.20) | 0.39(0.12) | 0.48(0.20) | 0.48(0.20) | 0.87(>0.05) | 0.03 | 0.26(>0.05) | 0.01 | 3.53(>0.05) | 0.10 |
| A95 [cm2] | 1.71(0.68) | 1.98(1.11) | 2.10(1.44) | 2.22(1.44) | 0.12(>0.05) | 0.00 | 0.32(>0.05) | 0.01 | 2.16(>0.05) | 0.06 |
| EC | ||||||||||
| Vcop [cm/s] | 1.55(0.69) | 1.36(0.45) | 1.59(0.64) | 1.46(0.69) | 0.12(>0.05) | 0.00 | 0.63(>0.05) | 0.02 | 0.86(>0.05) | 0.03 |
| VcopY [cm/s] | 1.34(0.67) | 1.19(0.41) | 1.35(0.62) | 1.21(0.60) | 0.00 (>0.05) | 0.00 | 0.62(>0.05) | 0.02 | 0.07(>0.05) | 0.00 |
| VcopX [cm/s] | 0.53(0.27) | 0.46(0.18) | 0.58(0.27) | 0.58(0.34) | 0.56(>0.05) | 0.02 | 0.13(>0.05) | 0.00 | 3.42(>0.05) | 0.10 |
| A95 [cm2] | 1.91(1.10) | 2.08(1.11) | 2.33(1.15) | 2.64(1.75) | 0.09(>0.05) | 0.00 | 0.41(>0.05) | 0.01 | 4.20(<0.05) | 0.12 |
| DT | ||||||||||
| Vcop [cm/s] | 1.63(0.91) | 1.50(0.81) | 1.54(0.57) | 1.64(0.83) | 1.23(>0.05) | 0.04 | 0.00(>0.05) | 0.00 | 0.06(>0.05) | 0.00 |
| VcopY [cm/s] | 1.29(0.60) | 1.21(0.64) | 1.26(0.48) | 1.30(0.69) | 0.66(>0.05) | 0.02 | 0.01(>0.05) | 0.00 | 0.16(>0.05) | 0.00 |
| VcopX [cm/s] | 0.73(0.60) | 0.65(0.41) | 0.65(0.26) | 0.74(0.42) | 1.55(>0.05) | 0.05 | 0.00(>0.05) | 0.00 | 0.00(>0.05) | 0.00 |
| A95 [cm2] | 3.32(3.79) | 3.40(4.57) | 2.84(1.96) | 5.12(6.41) | 3.52(>0.05) | 0.10 | 0.69(>0.05) | 0.02 | 1.13(>0.05) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marciniak, K.; Maciaszek, J.; Cyma-Wejchenig, M.; Szeklicki, R.; Stemplewski, R. The Effect of Nordic Walking Training with Poles with an Integrated Resistance Shock Absorber on the Body Balance of Women over the Age of 60. Healthcare 2021, 9, 267. https://doi.org/10.3390/healthcare9030267
Marciniak K, Maciaszek J, Cyma-Wejchenig M, Szeklicki R, Stemplewski R. The Effect of Nordic Walking Training with Poles with an Integrated Resistance Shock Absorber on the Body Balance of Women over the Age of 60. Healthcare. 2021; 9(3):267. https://doi.org/10.3390/healthcare9030267
Chicago/Turabian StyleMarciniak, Katarzyna, Janusz Maciaszek, Magdalena Cyma-Wejchenig, Robert Szeklicki, and Rafał Stemplewski. 2021. "The Effect of Nordic Walking Training with Poles with an Integrated Resistance Shock Absorber on the Body Balance of Women over the Age of 60" Healthcare 9, no. 3: 267. https://doi.org/10.3390/healthcare9030267