Are Special Care Dentistry Services Prepared for a Global Disruption in Healthcare? A Call for a Wider Promotion of Dental Conscious Sedation Training

 , ,
, ,
Abstract
:1. Introduction
2. Professional Guidance and Recommendations for the Use of Dental Sedation during COVID-19 Pandemic
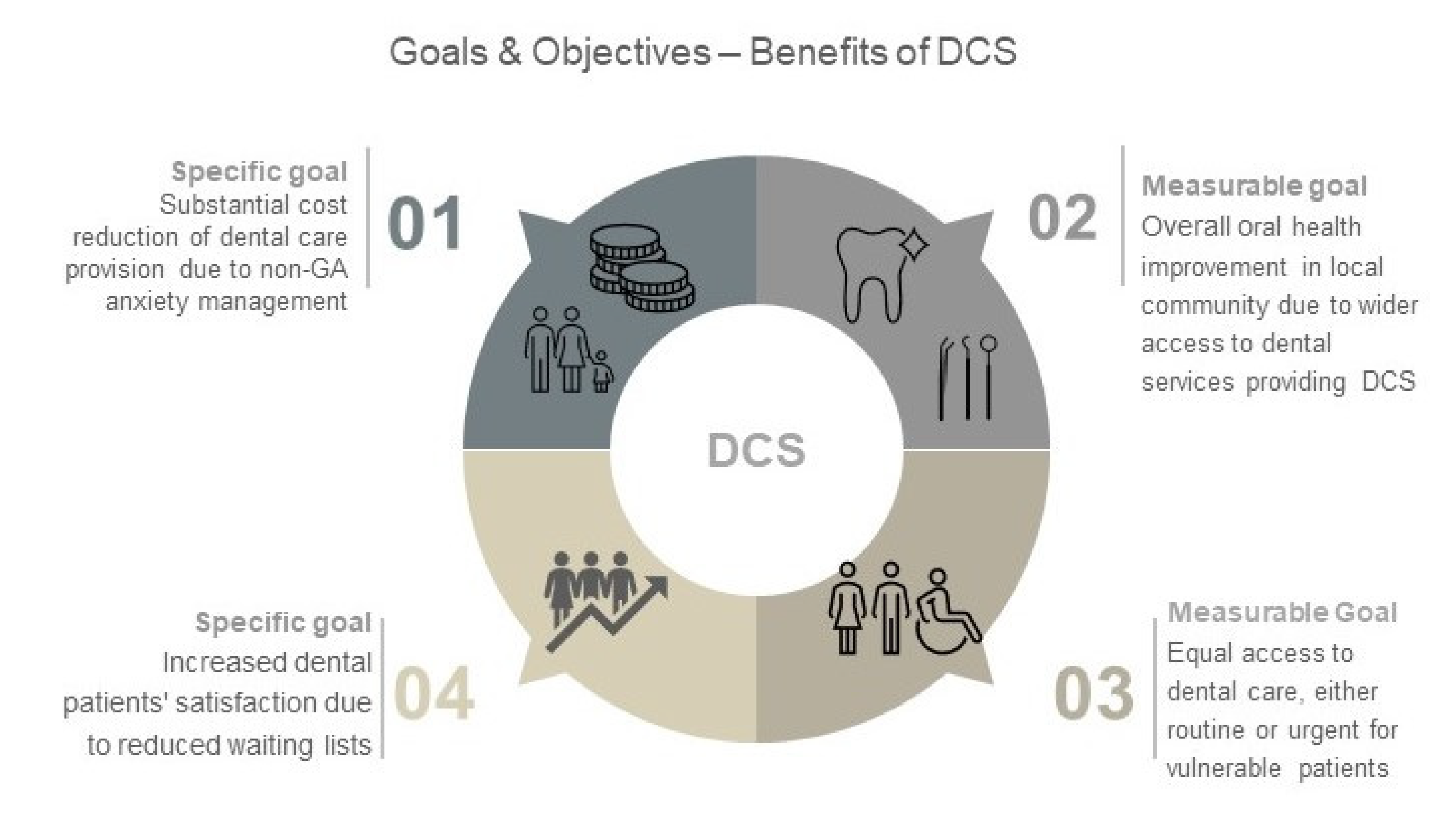
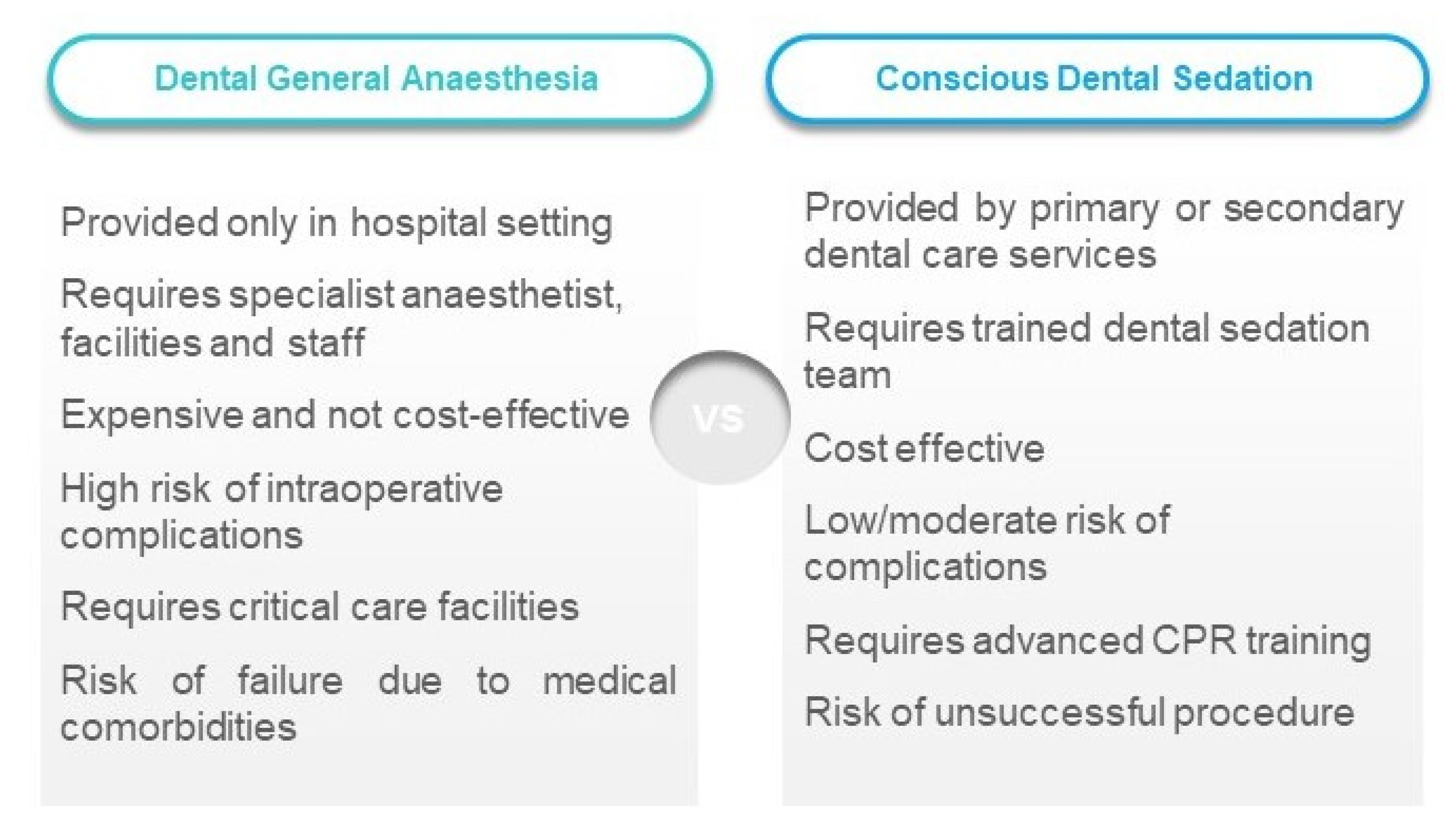
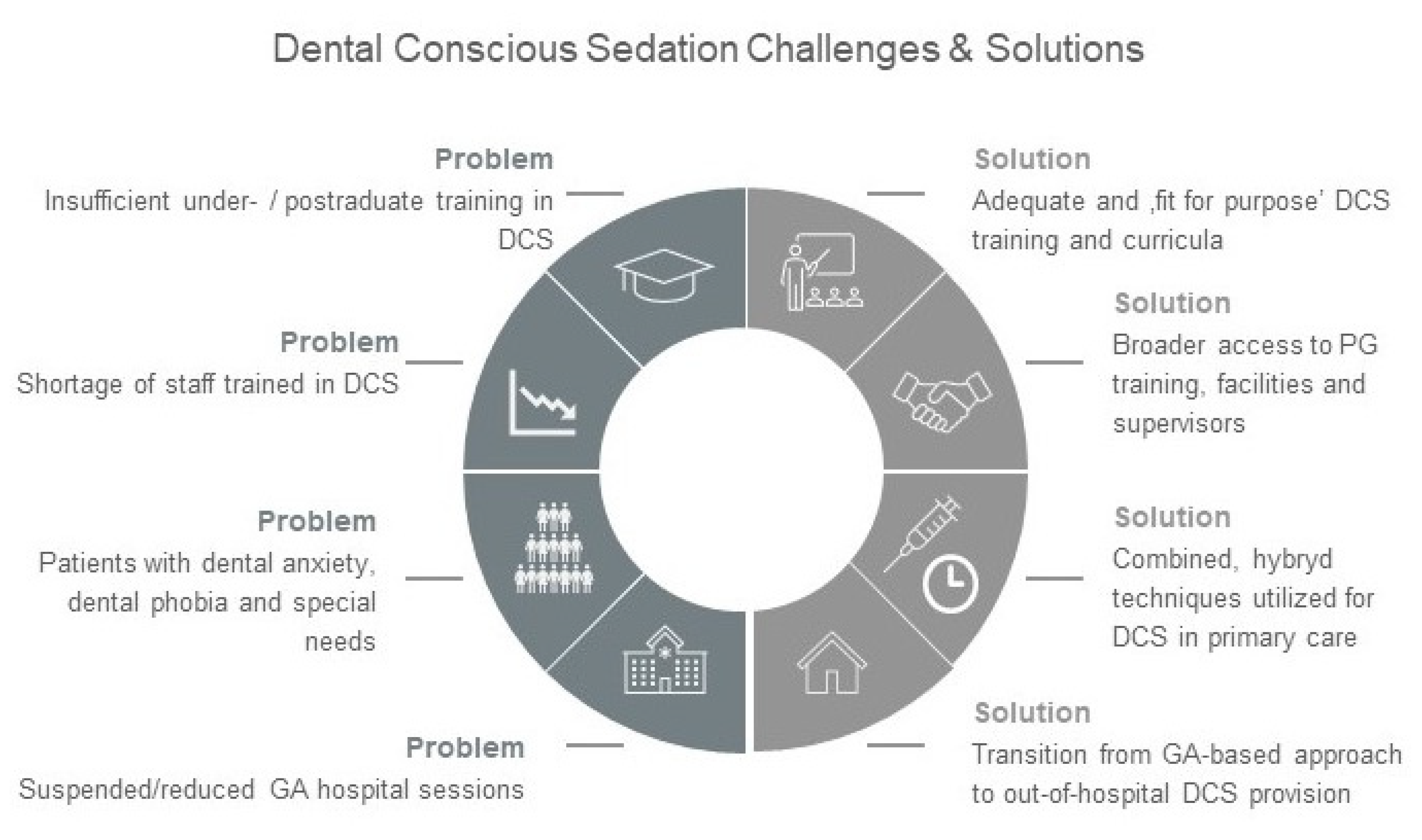
3. Transition from a General Anaesthesia-Based Model to the Use of Various Dental Sedation Methods for Anxiety Management
4. Enhancement of Dental Conscious Sedation Students’ Curricula
5. Broader Access to Postgraduate Dental Training for Newly Graduated Dentists and Experienced Practitioners. Promotion of Local On-Site Training in DCS
6. Dedicated Support for Research with Direct Relevance to Dental Conscious Sedation
7. Summary
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Alzahrani, S.B.; Alrusayes, A.A.; Aldossary, M.S. Impact of COVID-19 pandemic on dental education, research, and students. Int. J. Health Sci. Res. 2020, 10, 207–212. [Google Scholar]
- Deery, C. The COVID-19 pandemic: Implications for dental education. Evid. Based Dent. 2020, 21, 46–47. [Google Scholar] [CrossRef] [PubMed]
- Sneyd, J.R.; Mathoulin, S.E.; O’Sullivan, E.P.; So, V.C.; Roberts, F.R.; Paul, A.A.; Cortinez, L.I.; Ampofo, R.S.; Miller, C.J.; Balkisson, M.A. Impact of the COVID-19 pandemic on anaesthesia trainees and their training. Br. J. Anaesth. 2020, 125, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Standards for Conscious Sedation in the Provision of Dental Care: Report of the Intercollegiate Advisory Committee for Sedation in Dentistry (IACSD). 2015. Available online: www.rcseng.ac.uk/dental-faculties/fds/publications-guidelines/standards-for-conscious-sedation-inthe-provision-of-dental-care-and-accreditation/ (accessed on 4 September 2020).
- Scottish Dental Clinical Effectiveness Programme. Conscious Sedation in Dentistry. Dental Clinical Guidance; Scottish Dental Clinical Effectiveness Programme: Dundee, Scotland, UK, 2017. [Google Scholar]
- Registration Standards. Available online: http://www.dentalboard.gov.au/Registration-Standards.aspx (accessed on 5 September 2020).
- Westgarth, D. COVID-19 and Community Dental Services: The challenges ahead. BDJ Pract. 2020, 33, 14–19. [Google Scholar] [CrossRef]
- Blumenthal, D.; Fowler, E.J.; Abrams, M.; Collins, S.R. Covid-19—Implications for the Health Care System. N. Engl. J. Med. 2020, 8, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, N.T.; Nunn, J.H.; Evans, D.J. A comparison of costs in providing dental care for special needs patients under sedation or general anaesthesia in the North East of England. Prim. Dent. Care 2006, 13, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Surgeons of England. Recommendations for Special Care Dentistry During COVID-19 Pandemic. 2020. Available online: https://www.rcseng.ac.uk/dental-faculties/fds/coronavirus/ (accessed on 20 August 2020).
- SAAD. Restarting IV Sedation in the Clinical Environment. 2020. Available online: https://www.saad.org.uk/ (accessed on 22 August 2020).
- NHS. Dental Standard Operating Procedure: Transition to Recovery; NHS: England, UK, 2020. [Google Scholar]
- Glassman, P.; Caputo, A.; Dougherty, N.; Lyons, R.; Messieha, Z.; Miller, C.; Peltier, B.; Romer, M. Special Care Dentistry Association. Special Care Dentistry Association consensus statement on sedation, anesthesia, and alternative techniques for people with special needs. Spec. Care Dent. 2009, 29, 2–8. [Google Scholar] [CrossRef]
- National Clinical Guideline Centre. Sedation in Children and Young People: Sedation for Diagnostic and Therapeutic Procedures in Children and Young People; NICE Clinical Guidelines, No. 112; National Clinical Guideline Centre (UK), Royal College of Physicians: London, UK, 2010. [Google Scholar]
- Shepherd, A.R.; Ali, H. A Care Pathway for Children Unable to Accept Dental Care Within the General Dental Services Involving the Use of Inhalation Sedation and General Anaesthesia. Prim. Dent. J. 2015, 4, 29–34. [Google Scholar] [CrossRef]
- Macfarlane, A.J.R.; Harrop-Griffiths, W.; Pawa, A. Regional anaesthesia and COVID-19: First choice at last? Br. J. Anaesth. 2020, 125, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Conscious Sedation. Available online: https://www.baos.org.uk/resources/BDAGuidanceconscious_sedation_-_nov_11.pdf (accessed on 5 September 2020).
- AoMRC London. Safe Sedation Practice for Healthcare Procedures: Standards and Guidance. 2013. Available online: http://www.aomrc.org.uk/publications/reports-aguidance/doc_view/9737-safe-sedation-practice-for-healthcare-proceduresstandards-and-guidance.htm (accessed on 5 September 2020).
- Picciani, B.L.S.; Bausen, A.G.; Dos Santos, B.M.; Marinho, M.A.; Faria, M.B.; Bastos, L.F.; Dziedzic, A. The challenges of dental care provision in patients with learning disabilities and special requirements during COVID-19 pandemic. Spec. Care Dent. 2020, 40, 525–527. [Google Scholar] [CrossRef] [PubMed]
- Tobin, C.D.; Clark, C.A.; McEvoy, M.D.; Reves, J.G.; Schaefer, J.J.; Wolf, B.J.; Reeves, S.T. An approach to moderate sedation simulation training. Simul. Healthc. 2013, 8, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Kyaw, B.M.; Saxena, N.; Posadzki, P.; Vseteckova, J.; Nikolaou, C.K.; George, P.P.; Divakar, U.; Masiello, I.; Kononowicz, A.A.; Zary, N.; et al. Virtual Reality for Health Professions Education: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration. J. Med. Internet Res. 2019, 21, e12959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Symington, L.; McGugam, E.; Graham, C.; Gordon, M.; Thakore, S. Training in conscious sedation techniques: Meeting the recommendations of the UK Academy of Medical Royal Colleges. Emerg. Med. J. 2007, 24, 576–578. [Google Scholar] [CrossRef] [PubMed]
- O’Halloran, M. The use of anaesthetic agents to provide anxiolysis and sedation in dentistry and oral surgery. Australas. Med. J. 2013, 6, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Kapur, A.; Kapur, V. Conscious Sedation in Dentistry. Ann. Maxillofac. Surg. 2018, 8, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Nadershahi, N.A.; Bender, D.J.; Beck, L.; Alexander, S. A case study on development of an integrated, multidisciplinary dental curriculum. J. Dent. Educ. 2013, 77, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.Y.; Kim, E.J. Current trends in intravenous sedative drugs for dental procedures. J. Dent. Anesth. Pain Med. 2016, 16, 89–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, K.P.; Seth, N. Future of paediatric sedation: Towards a unified goal of improving practice. Br. J. Anaesth. 2019, 122, 652–661. [Google Scholar] [CrossRef] [PubMed]
- Perel, A. Non-anaesthesiologists should not be allowed to administer propofol for procedural sedation: A Consensus Statement of 21 European National Societies of Anaesthesia. Eur. J. Anaesthesiol. 2011, 28, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Dziedzic, A.; Tanasiewicz, M.; Tysiąc-Miśta, M. Dental Care Provision during Coronavirus Disease 2019 (COVID-19) Pandemic: The Importance of Continuous Support for Vulnerable Patients. Medicina 2020, 56, 294. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Conscious Sedation Method | Advantages | Disadvantages |
|---|---|---|
| Oral sedation (OS) | Simple method, does not require specific training/equipment, side effects are rare if any, can be combined with other DCS methods | Age restricted, unpredictable pharmacokinetics and patients’ response, limited efficiency of anxiolysis, risk of oversedation or undersedation, unpredictable sedative effect, sometimes prolonged recovery, may require a chaperone person |
| Inhalation sedation (IHS) | No age restrictions, although it requires good cooperation, wide safety margin, can be enhanced by additional techniques, such as music and tranquilizing verbal descriptions, quick recovery, does not require chaperone person | Limited efficiency, requires special, expensive equipment; anxiolysis less effective in adults; special facilities requirements (scavenging); operator sensitive; technique sensitive |
| Intravenous sedation with single-drug titration (midazolam IVS) | Effective in situations where OS or IHS failed or for patients with severe dental phobia who cannot be sedated with IHS, well-controlled patient’s response due to drug titration, allows a profound anxiolysis, post-operative amnesia effect, may substitute dental general anaesthesia in selected cases, reversal agent in case of intraoperative complications or abnormal reaction associated with the use of benzodiazepine agent | Age limited, usually not used in children below 12 y.o.a., risk of systemic complications, age-restricted, requires advanced training and cannulation skills, requires training in advanced life support, chaperone person required, comprehensive pre- and postoperative instructions for patient |
| Intranasal, transmucosal sedation with a short-acting benzodiazepine (midazolam) | Non-invasive, often used as an adjunct to IV sedation prior to cannulation, allowing a better patient’s co-operation during cannulation; does not require specific facilities or equipment; reversal agent in case of complications | Unpredictable sedative effect, unpleasant sensations during administration, usually not used alone, requires advanced training and cannulation skills (in case of adverse effects) |
| Tool/Method | Educational Application and Features |
|---|---|
| Lecture: traditional, online, blended/mixed type | Mainly theoretical aspects, knowledge transfer with limited interaction |
| Student’s presentation: classroom, online | Direct involvement in a certain subject, deep understanding of required knowledge, communication skills development |
| Assignment: tentative, summative | Assessment of acquired knowledge and understanding |
| Case study reflection: classroom, online | Personal opinion about clinical case, with involvement of other students, learning from reflecting on past experience |
| Simulation: high-fidelity simulation with patient simulator and low-fidelity simulation with actors as simulated patients | Practical aspects of DCS without patient’s involvement |
| Workshop | Sharing experience, open discussion, exchange of thoughts and ideas, practical exercises |
| Virtual Reality Training | Expensive equipment, requires special software and knowledge/training, does not provide real interaction or tactile sensations, purely “technical feedback” |
| Clinical sessions | Practical training with patient’s presence, real interaction in clinical environment, communication skills practice |
| Peer Review and Research | Evidence-based aspects of DCS practice |
| Conference attendance | Variety of different topics, experts’ opinions, and experience, limited feedback |
| Self-learning (online) | Lack of interaction, no feedback, wide/uninterrupted access |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dziedzic, A.; Tanasiewicz, M.; Abed, H.; Dickinson, C.; Picciani, B. Are Special Care Dentistry Services Prepared for a Global Disruption in Healthcare? A Call for a Wider Promotion of Dental Conscious Sedation Training. Healthcare 2020, 8, 419. https://doi.org/10.3390/healthcare8040419
Dziedzic A, Tanasiewicz M, Abed H, Dickinson C, Picciani B. Are Special Care Dentistry Services Prepared for a Global Disruption in Healthcare? A Call for a Wider Promotion of Dental Conscious Sedation Training. Healthcare. 2020; 8(4):419. https://doi.org/10.3390/healthcare8040419
Chicago/Turabian StyleDziedzic, Arkadiusz, Marta Tanasiewicz, Hassan Abed, Chris Dickinson, and Bruna Picciani. 2020. "Are Special Care Dentistry Services Prepared for a Global Disruption in Healthcare? A Call for a Wider Promotion of Dental Conscious Sedation Training" Healthcare 8, no. 4: 419. https://doi.org/10.3390/healthcare8040419