
The Road to Developing Standard Time for Efficient Nursing Care: A Time and Motion Analysis

 ,
,
Abstract
:1. Introduction
1.1. Rationale
- Observed time is the time recorded by the observer during observation using the appropriate means to calculate the time nurses spend on a specific activity;
- The performance rating factor refers to the nurse’s speed and the efficiency of a nurse in performing a task in comparison to other nurses, and this is expressed as a percentage of the efficiency and may range from 80 to 130% with the standard performance being equal to 100% [26];
- Adjustment time is the additional time added above the basic time to perform the activity and account for delays. It is the most debatable part of calculating ST, because it differs from nurse to nurse, activity to activity, unit to unit, situation to situation, institution to institution and season to season for example. Therefore, specific standardized norms of adjustment time have been set [26]: (i) fatigue adjustment (intended to provide for the physiological and psychological effects of carrying out specified work under specified conditions such as patients with high acuity, traveling time, number of patients, assigned to additional tasks), (ii) personal needs adjustment (intended to provide rest to recover from the physiological and psychological effects, and attend personal needs), and (iii) unavoidable delay adjustment (intended to provide for unavoidable delays such as interruption, multitasking, searching for missing or out-of-stock items, system breakdown, waiting for patients to transfer from the operating room).
1.2. Study Aim
2. Methods
2.1. Study Design
2.2. Setting
- nurse-to-patient ratio should be within the 1:4 range;
- the shift should be an 8 h morning shift, since the nurses’ work peak is evident during the morning shift;
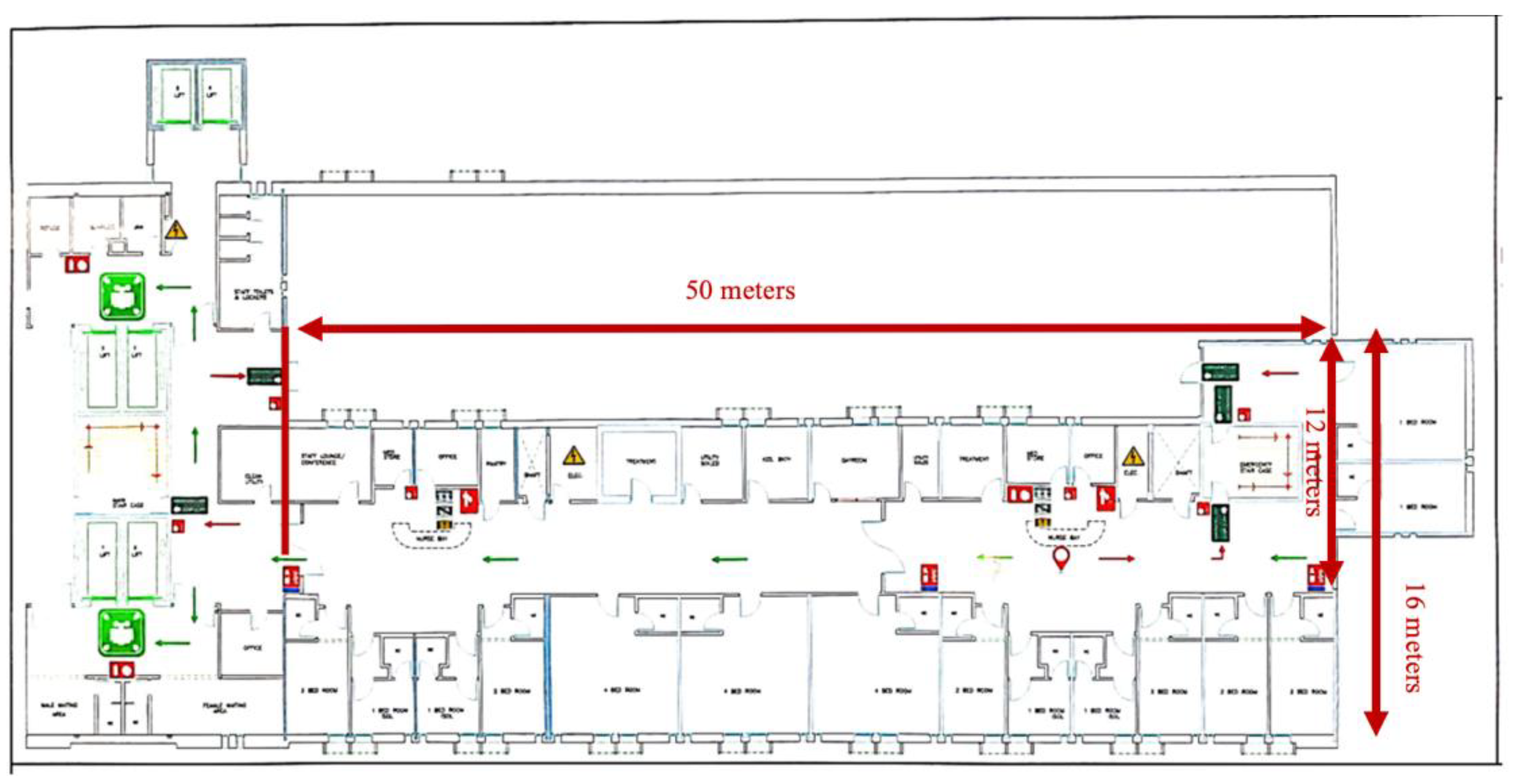
- a long, straight corridor layout.
2.3. Recruitment
2.4. Observational Tool
- Direct patient care, which involves activities such as health assessment, vital signs, medication, patient comfort, procedures;
- Indirect patient care, which involves activities such as handover, doctor rounds, diagnostic tests;
- Documentation, which involves activities such as paper-based charting, electronic-based charting;
- Professional communication, which involves activities such as exchange information, in-hospital phoning, refereeing;
- Unit/room, which involves activities such as bed-making, room- and nursing station-tidying, infection control measures, supplies maintenance, unit learning;
- Personal, which involves activities such as self-learning, praying, eating, visiting administrative offices, personal phone calls, aside-chatting.
2.5. Observer and Inter-Observer Reliability Assessment
2.6. Data Collection Procedure
2.7. Analysis
3. Results
3.1. Time Allocated
3.2. Observational Comments
3.3. Calculating the Standard Time (Effective Minutes)
- Equation (1) Effective hours
- Equation (2) Performance rating factor
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oner, B.; Zengul, F.D.; Oner, N.; Ivankova, N.V.; Karadag, A.; Patrician, P.A. Nursing-sensitive indicators for nursing care: A systematic review (1997–2017). Nurs. Open 2021, 8, 1005–1022. [Google Scholar] [CrossRef] [PubMed]
- Needleman, J.; Liu, J.; Shang, J.; Larson, E.L.; Stone, P.W. Association of registered nurse and nursing support staffing with inpatient hospital mortality. BMJ Qual. Saf. 2020, 29, 10–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, Y.W.; Chen, W.Y.; Lee, J.L.; Huang, L.C. Nurse staffing, direct nursing care hours and patient mortality in Taiwan: The longitudinal analysis of hospital nurse staffing and patient outcome study. BMC Health Serv. Res. 2012, 12, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michel, O.; Manjon, A.G.; Pasquier, J.; Bucher, C.O. How do nurses spend their time? A time and motion analysis of nursing activities in an internal medicine unit. J. Adv. Nurs. 2021, 77, 4459–4470. [Google Scholar] [CrossRef] [PubMed]
- Van Belle, E.; Giesen, J.; Conroy, T.; van Mierlo, M.; Vermeulen, H.; Huisman-de Waal, G.; Heinen, M. Exploring person-centred fundamental nursing care in hospital wards: A multi-site ethnography. J. Clin. Nurs. 2020, 29, 1933–1944. [Google Scholar] [CrossRef]
- Swiger, P.A.; Patrician, P.A.; Miltner, R.S.; Raju, D.; Breckenridge-Sproat, S.; Loan, L.A. The Practice Environment Scale of the Nursing Work Index: An updated review and recommendations for use. Int. J. Nurs. Stud. 2017, 74, 76–84. [Google Scholar] [CrossRef]
- Lindqvist, R.; Smeds Alenius, L.; Runesdotter, S.; Ensio, A.; Jylhä, V.; Kinnunen, J.; Sjetne, I.S.; Tvedt, C.; Tjønnfjord, M.W.; Tishelman, C. Organization of nursing care in three Nordic countries: Relationships between nurses’ workload, level of involvement in direct patient care, job satisfaction, and intention to leave. BMC Nurs. 2014, 13, 27. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.X.; Wang, L.P.; Wang, Q.Q.; Fang, Y.Y.; Lv, W.J.; Huang, H.L.; Yang, T.T.; Qian, R.L.; Zhang, Y.H. Related factors influencing Chinese psychiatric nurses’ turnover: A Cross-Sectional study. J. Psychiatr. Ment. Health Nurs. 2022, 29, 698–708. [Google Scholar] [CrossRef]
- Yen, P.-Y.; Kellye, M.; Lopetegui, M.; Saha, A.; Loversidge, J.; Chipps, E.M.; Gallagher-Ford, L.; Buck, J. Nurses’ time allocation and multitasking of nursing activities: A time motion study. AMIA Annu. Symp. Proc. 2018, 2018, 1137. [Google Scholar]
- Yakusheva, O.; Weiss, M.E.; Bobay, K.L.; Costa, L.; Hughes, R.G.; Hamilton, M.; Bang, J.; Buerhaus, P.I. Individual nurse productivity in preparing patients for discharge is associated with patient likelihood of 30-day return to hospital. Med. Care 2019, 57, 688. [Google Scholar] [CrossRef]
- Kaddourah, B.; Abu-Shaheen, A.K.; Al-Tannir, M. Quality of nursing work life and turnover intention among nurses of tertiary care hospitals in Riyadh: A cross-sectional survey. BMC Nurs. 2018, 17, 43. [Google Scholar] [CrossRef]
- Allen-Duck, A.; Robinson, J.C.; Stewart, M.W. Healthcare quality: A concept analysis. Nurs. Forum 2017, 52, 377–386. [Google Scholar] [CrossRef]
- Cho, E.; Lee, N.J.; Kim, E.Y.; Kim, S.; Lee, K.; Park, K.O.; Sung, Y.H. Nurse staffing level and overtime associated with patient safety, quality of care, and care left undone in hospitals: A cross-sectional study. Int. J. Nurs. Stud. 2016, 60, 263–271. [Google Scholar] [CrossRef]
- Ball, J.E.; Griffiths, P. Consensus Development Project (CDP): An overview of staffing for safe and effective nursing care. Nurs. Open 2022, 9, 872–879. [Google Scholar] [CrossRef]
- Antinaho, T.; Kivinen, T.; Turunen, H.; Partanen, P. Improving the quality of registered nurses’ working time use data. J. Clin. Nurs. 2017, 26, 3031–3043. [Google Scholar] [CrossRef] [Green Version]
- Antinaho, T.; Kivinen, T.; Turunen, H.; Partanen, P. Nurses’ working time use—How value adding it is? J. Nurs. Manag. 2015, 23, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Canzan, F.; Heilemann, M.V.; Saiani, L.; Mortari, L.; Ambrosi, E. Visible and invisible caring in nursing from the perspectives of patients and nurses in the gerontological context. Scand. J. Caring Sci. 2014, 28, 732–740. [Google Scholar] [CrossRef] [PubMed]
- Lavander, P.; Meriläinen, M.; Turkki, L. Working time use and division of labour among nurses and health-care workers in hospitals–a systematic review. J. Nurs. Manag. 2016, 24, 1027–1040. [Google Scholar] [CrossRef] [PubMed]
- Farquharson, B.; Bell, C.; Johnston, D.; Jones, M.; Schofield, P.; Allan, J.; Ricketts, I.; Morrison, K.; Johnston, M. Frequency of nursing tasks in medical and surgical wards. J. Nurs. Manag. 2013, 21, 860–866. [Google Scholar] [CrossRef]
- D’Amour, D.; Dubois, C.A.; Déry, J.; Clarke, S.; Tchouaket, É.; Blais, R.; Rivard, M. Measuring actual scope of nursing practice: A new tool for nurse leaders. JONA J. Nurs. Adm. 2012, 42, 248–255. [Google Scholar] [CrossRef]
- Hossny, E.K. Studying nursing activities in inpatient units: A road to sustainability for hospitals. BMC Nurs. 2022, 21, 148. [Google Scholar] [CrossRef]
- Dall’Ora, C.; Griffiths, P.; Hope, J.; Briggs, J.; Jeremy, J.; Gerry, S.; Redfern, O.C. How long do nursing staff take to measure and record patients’ vital signs observations in hospital? A time-and-motion study. Int. J. Nurs. Stud. 2021, 118, 103921. [Google Scholar] [CrossRef] [PubMed]
- Sinsky, C.; Colligan, L.; Li, L.; Prgomet, M.; Reynolds, S.; Goeders, L.; Westbrook, J.; Tutty, M.; Blike, G. Allocation of physician time in ambulatory practice: A time and motion study in 4 specialties. Ann. Intern. Med. 2016, 165, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Yazdi, P.G.; Azizi, A.; Hashemipour, M. A hybrid methodology for validation of optimization solutions effects on manufacturing sustainability with time study and simulation approach for SMEs. Sustainability 2019, 11, 1454. [Google Scholar] [CrossRef] [Green Version]
- Bridger, R. Introduction to Ergonomics; CRC Press: Boca Raton, FL, USA, 2008. [Google Scholar]
- Konz, S. Work Design: Occupational Ergonomics; CRC Press: Boca Raton, FL, USA, 2018. [Google Scholar]
- Lopetegui, M.; Bai, S.; Yen, P.-Y.; Lai, A.; Embi, P.; O Payne, P.R. Inter-observer reliability assessments in time motion studies: The foundation for meaningful clinical workflow analysis. AMIA Annu. Symp. Proc. 2013, 2013, 889. [Google Scholar]
- Vichoray, C.; Deogaonkar, A.; Pais, R.; Dhote, S. There are just too many labours: Productivity improvement in collecting waste at ASL. CASE J. 2023, 19, 241–251. [Google Scholar] [CrossRef]
- Gill, F.J.; Nelson, H.; Bear, N.; Tallon, M.; Pienaar, C.; Ferullo, J.; Baker, S. A new children’s hospital with a larger floor space, single rooms, and V-shaped ward design: A pre–post evaluation of nurse time providing patient care and nurse, patient, and family experiences. J. Health Serv. Res. Policy 2023, 28, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.; Park, B. Calculating the optimal number of nurses based on nursing intensity by patient classification groups in general units in South Korea: A cross-sectional study. Nurs. Open 2023, 10, 3982–3991. [Google Scholar] [CrossRef]
- Kalne, P.S.; Mehendale, A.M. The purpose of time-motion studies (TMSs) in healthcare: A literature review. Cureus 2022, 14, e29869. [Google Scholar] [CrossRef]
- Baumgart, A.; Neuhauser, D. Frank and Lillian Gilbreth: Scientific management in the operating room. BMJ Qual. Saf. 2009, 18, 413–415. [Google Scholar] [CrossRef]
- Ejebu, O.Z.; Dall’Ora, C.; Griffiths, P. Nurses’ experiences and preferences around shift patterns: A scoping review. PLoS ONE 2021, 16, e0256300. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K.; Rani, R. Nurse-to-patient ratio and nurse staffing norms for hospitals in India: A critical analysis of national benchmarks. J. Fam. Med. Prim. Care 2020, 9, 2631. [Google Scholar] [CrossRef] [PubMed]
- Alluhidan, M.; Tashkandi, N.; Alblowi, F.; Omer, T.; Alghaith, T.; Alghodaier, H.; Alazemi, N.; Tulenko, K.; Herbst, C.H.; Hamza, M.M.; et al. Challenges and policy opportunities in nursing in Saudi Arabia. Hum. Resour. Health 2020, 18, 98. [Google Scholar] [CrossRef]
- Pachilova, R.; Sailer, K. Providing care quality by design: A new measure to assess hospital ward layouts. J. Archit. 2020, 25, 186–202. [Google Scholar] [CrossRef]
- Lopetegui, M.; Yen, P.-Y.; Lai, A.M.; Embi, P.J.; O Payne, P.R. Time Capture Tool (TimeCaT): Development of a comprehensive application to support data capture for Time Motion Studies. AMIA Annu. Symp. Proc. 2012, 2012, 596. [Google Scholar]
- Battini, D.; Calzavara, M.; Persona, A.; Sgarbossa, F. Additional effort estimation due to ergonomic conditions in order picking systems. Int. J. Prod. Res. 2017, 55, 2764–2774. [Google Scholar] [CrossRef]
- Martinelli, J.L. Incorporating Worker-Specific Factors in Operations Management Models; Erasmus Research Institute of Management: Rotterdam, The Netherlands, 2010. [Google Scholar]
- Upenieks, V.V.; Akhavan, J.; Kotlerman, J. Value-added care: A paradigm shift in patient care delivery. Nurs. Econ. 2008, 26, 294–301. [Google Scholar] [PubMed]
- Lim, M.L.; Ang, S.Y. A time–motion observation study to measure and analyse clinical nursing workload in an acute care hospital in Singapore. Proc. Singap. Healthc. 2019, 28, 124–128. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Workload Indicators of Staffing Need (WISN). User’s Manual; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Al-Dabbagh, S.A.; Sulaiman, H.M.; Abdulkarim, N.A. Workload assessment of medical doctors at primary health care centers in the Duhok governorate. Hum. Resour. Health 2022, 19, 117. [Google Scholar] [CrossRef]
- Mohamed, N.; Al-Lawati, N. How to make the best use of the workload indicators of staffing needs method in determining the proportion of time spent in each of the workload components and its implication in decision making: The experience of the Sultanate of Oman. Hum. Resour. Health 2022, 19, 113. [Google Scholar] [CrossRef]
- McQuide, P.A.; Kolehmainen-Aitken, R.L.; Forster, N. Applying the workload indicators of staffing need (WISN) method in Namibia: Challenges and implications for human resources for health policy. Hum. Resour. Health 2013, 11, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagopian, A.; Mohanty, M.K.; Das, A.; House, P.J. Applying WHO’s ‘workforce indicators of staffing need’(WISN) method to calculate the health worker requirements for India’s maternal and child health service guarantees in Orissa State. Health Policy Plan. 2012, 27, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qureshi, S.M.; Purdy, N.; Neumann, W.P. A Computerized Model Quantifying the Impact of Geographical Patient-Bed Assignment on Nurse Workload and Quality Care. Nurs. Econ. 2021, 39, 23–34. [Google Scholar]
- Lee, J.; Lee, H.; Shepley, M.M. Exploring the spatial arrangement of patient rooms for minimum nurse travel in hospital nursing units in Korea. Front. Archit. Res. 2020, 9, 711–725. [Google Scholar] [CrossRef]
- Acar, I.; Butt, S.E. Modeling nurse-patient assignments considering patient acuity and travel distance metrics. J. Biomed. Inform. 2016, 64, 192–206. [Google Scholar] [CrossRef]
- Guido, R.; Groccia, M.C.; Conforti, D. An efficient matheuristic for offline patient-to-bed assignment problems. Eur. J. Oper. Res. 2018, 268, 486–503. [Google Scholar] [CrossRef]
- Cignarale, C. Analysis and Optimization of Patient Bed Assignments within a Hospital unit while Considering Isolation Requirements; Rochester Institute of Technology: Rochester, NY, USA, 2013. [Google Scholar]
- House, S.; Havens, D. Nurses’ and physicians’ perceptions of nurse-physician collaboration. J. Nurs. Adm. 2017, 47, 165–171. [Google Scholar] [CrossRef]
- Moore, E.C.; Tolley, C.L.; Bates, D.W.; Slight, S.P. A systematic review of the impact of health information technology on nurses’ time. J. Am. Med. Inform. Assoc. 2020, 27, 798–807. [Google Scholar] [CrossRef]
- Salvendy, G. (Ed.) Handbook of Human Factors and Ergonomics; John Wiley & Sons: Hoboken, NJ, USA, 2012. [Google Scholar]
- Monteiro, C.; Avelar, A.F.; Pedreira, M.D. Interruptions of nurses’ activities and patient safety: An integrative literature review. Rev. Lat. -Am. De Enferm. 2015, 23, 169–179. [Google Scholar] [CrossRef] [Green Version]
- Hopkinson, S.G.; Jennings, B.M. Interruptions during nurses’ work: A state-of-the-science review. Res. Nurs. Health 2013, 36, 38–53. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Criteria | Study Protocol | |||
|---|---|---|---|---|
| Purpose | Baseline data for nursing activities | How nurses spent their break time | Nurse location and movement | Miscellaneous work |
| Data collected | All patient and unit activities during the 8 h morning shift | All personal activities during the 8 h morning shift | Travel time during the 8 h morning shift | All non-patient and unit activities during the 8 h morning shift |
| Values | Observed time | Time for personal needs | Fatigue time | Unavoidable delay time |
| Study period | All on-shift hours for ten days | All on-shift hours for ten days | All on-shift hours for ten days | All on-shift hours for ten days |
| Collecting tools |
|
|
|
|
| Observation division |
|
|
|
|
| Method | For each nursing activity
| For each observed nurse
| For each observed nurse
| For each non-nursing patient and unit activity
|
| Participation | All nurses agreed to participate | All nurses agreed to participate | All nurses agreed to participate | All nurses agreed to participate |
| Nurse shift studied | Morning shift | Morning shift | Morning shift | Morning shift |
| Activity Category | Multitasking and/or Interruption | Time and Percentage of the 8 h Shift Spent on Activities in Category |
|---|---|---|
| Direct Patient Care Category | (93 min) 19.4% | |
| Health assessment (charting not included) | Noted | 00:07:27 |
| Vital sign measurement and preparation (charting not included) | Noted | 00:11:21 |
| Medication including preparation and administering (charting not included) | Noted | 00:36:26 |
| Patient comfort care (e.g., daily living activities, feeding, answer Qs, fixing tubes) | Noted | 00:32:31 |
| Procedures including preparation time | Noted | 00:06:28 |
| Cannulation and intravenous fluids, including preparation, insertion and hanging | Noted | 00:05:21 |
| Indirect Patient Care Category | (58 min) 12% | |
| Handover (endorsement) including morning, admission, during and end of the shift | Noted | 00:33:20 |
| Doctor rounds | Noted | 00:19:13 |
| Diagnostic test including collecting and sending | Noted | 00:04:09 |
| Others | 00:00:55 | |
| Documentation | (68 min) 14.2% | |
| There were 15 distinctive inpatient stay paper-based records | Noted | |
| Professional Communication | (24 min) 5% | |
| W. Staff nurse (s) | 00:06:58 | |
| W. Doctor (Dr rounds not included here) | 00:03:07 | |
| W. Head nurse | 00:04:09 | |
| W. Charge Nurse | 00:00:54 | |
| W. Nurse Supervisor | 00:00:35 | |
| W. Clinical Instructor | 00:00:55 | |
| W. patient’s relative/watcher (including educating, explaining and instructing) | 00:01:58 | |
| W. Patient Care technician (PCT) | 00:01:09 | |
| Answer in-hospital call | 00:01:54 | |
| Make in-hospital call | 00:02:41 | |
| Ward/room mainly based on assignment | (87 min) 18% | |
| Apply infection control measures including, hand washing, rubbing, masking, donning and doffing personal protective equipment (PPE) | 00:03:01 | |
| Checking point of care testing (POCT) [assigned task] | 00:13:27 | |
| Arrange nurse stations [nurse who has free time and willing to do] | 00:08:29 | |
| Check and arrange medical equipment room [assigned task] | 00:17:56 | |
| Arrange the medication supply room [nurse who has free time and willing to do] | 00:09:21 | |
| Arrange admission and discharge logbook census | 00:02:01 | |
| Check patient room safety including curtains and electrical wiring [assigned task] | 00:02:58 | |
| Sending empty ampules of narcotic to the pharmacy [nurse who has free time and willing to do] | 00:02:00 | |
| Checking narcotic checklist [nurse who has free time and willing to do] | 00:04:08 | |
| Check the supply with the head nurse [nurse who has free time and willing to do] | 00:12:33 | |
| Others | 00:01:36 | |
| Total | 330 min out of the 480 min (69%) | |
| Miscellaneous activities | 00:20:41 (4.3%) | |
| Searching for missing or out-of-stock item | 00:07:47 | |
| Printing forms | 00:01:43 | |
| Arrange patient files after doctors’ rounds and visits | 00:11:11 | |
| Total time in minutes (%) | 350 min |
| Personal Needs | Time and Percentage of Nurse Travel Path |
|---|---|
| Rest, coffee, eat, drink and pray | 00:42:24 |
| Personal affairs, emailing/texting, calling/helping friend(s) | 00:05:55 |
| Non-patient-related computer use | 00:04:58 |
| Chatting | 00:06:07 |
| Totals | (58 min) 12% |
| Travel Path | Time and Percentage of Nurse Travel Path |
|---|---|
| Moving between the two nursing stations | 00:06:16 |
| Moving between patient room and nursing stations | 00:04:08 |
| Moving between two patient rooms | 00:36:30 |
| Moving between patient room and supply/utility room | 00:06:11 |
| In-transit (traveling to pharmacy, X-ray and so on) | 00:16:59 |
| Totals | (69 min) 14% |
| Activity Category | Freq. of Interruption | Duration |
|---|---|---|
| Direct patient care category | 33 times | 00:43:28 |
| Indirect patient care category | 10 times | 00:10:06 |
| Documentation | 17 times | 00:19:38 |
| Total | 73 min (15%) |
| Activity Category | Observed Time | Calculation ST | Unavoidable Delay Adjustment | ST (Normal Time and Adjustment Time) | |
|---|---|---|---|---|---|
| 1 | Direct patient care activities | 93 min | (93) (1.05) = 97.65 min 97.65/1−0.20 = 122 min. | 20% | 122 min |
| 2 | Indirect patient care activities | 58 min | (58) (1.05) = 60.9 min 60.9/1−0.10 = 67.6 min. | 10% | 68 min |
| 3 | Documentation | 68 min | (68) (1.05) = 71.4 min 71.4/1−0.15 = 84 min. | 15% | 84 min |
| 4 | Professional communication | 24 min | (24) (1.05) = 25.2 min 25.2/1−0.05 = 26.5min. | 5% | 27 min |
| 5 | Ward/room | 87 min | (87) (1.05) = 93.4 min 93.4/1−0.05 = 98.3 min. | 5% | 98 min |
| 6 | Miscellaneous activities | 20 min | Imbedded with the activities | ||
| 7 | Personal needs adjustment | 58 min | 7% | - | 33 min |
| 8 | Fatigue adjustment | 69 min | 5% | - | 24 min |
| 9 | Unavoidable delay | 73 min | Imbedded with the activities | ||
| Total | 550 min | 456 min 7.6 h | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Moteri, M.; Alzahrani, A.A.; Althobiti, E.S.; Plummer, V.; Sahrah, A.Z.; Alkhaldi, M.J.; Rajab, E.F.; Alsalmi, A.R.; Abdullah, M.E.; Abduelazeez, A.E.A.; et al. The Road to Developing Standard Time for Efficient Nursing Care: A Time and Motion Analysis. Healthcare 2023, 11, 2216. https://doi.org/10.3390/healthcare11152216
Al-Moteri M, Alzahrani AA, Althobiti ES, Plummer V, Sahrah AZ, Alkhaldi MJ, Rajab EF, Alsalmi AR, Abdullah ME, Abduelazeez AEA, et al. The Road to Developing Standard Time for Efficient Nursing Care: A Time and Motion Analysis. Healthcare. 2023; 11(15):2216. https://doi.org/10.3390/healthcare11152216
Chicago/Turabian StyleAl-Moteri, Modi, Amer A. Alzahrani, Ensherah Saeed Althobiti, Virginia Plummer, Afnan Z. Sahrah, Maha Jabar Alkhaldi, Eishah Fahad Rajab, Amani R. Alsalmi, Merhamah E. Abdullah, Afra Ezeldeen Abduelaal Abduelazeez, and et al. 2023. "The Road to Developing Standard Time for Efficient Nursing Care: A Time and Motion Analysis" Healthcare 11, no. 15: 2216. https://doi.org/10.3390/healthcare11152216