
A Scoping Review on Long COVID-19: Physiological and Psychological Symptoms Post-Acute, Long-Post and Persistent Post COVID-19

 , , ,
, , ,
Abstract
:1. Introduction
Objectives
- critically analyze and comprehend the available literature on post/long COVID-19 symptoms.
- examine the long-term consequences of COVID-19 on the psychological and physiological health of long haulers of COVID-19.
- report on the common physiological as well as psychological symptoms and their prevalence among patients recovered from COVID-19.
- identify the factors that are associated with the severity of long COVID-19 symptoms.
- identify the population at risk and complications that cause prolongation of COVID-19 symptoms.
- discuss the potential impact of long COVID-19 symptoms on health andquality of life.
2. Methodology

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S.No | Major Step | Objective | Method | |
|---|---|---|---|---|
| 2.1 | Search strategy | The review will seek to identify existing research literature that may be used to support evidence-based practice. | The present scoping review used the iterative five-stage methodological framework of Arkskey and O’Malley that included the following steps:
| |
| Database Used | Pub Med | |||
| Key words and Medical Subject Headings (MeSH): | Long COVID, Long haul COVID, Post-acute COVID-19, post-acute sequalae of SARS-CoV-2, Chronic COVID-19, Chronic COVID-19 syndrome, Corona virus, long term effect, long-term sequalae, signs and symptoms and mental health. | |||
| 2.2 | Identification of relevant studies | To conduct a thorough literature search on the physiological and psychological symptoms of post/long COVID-19 | Original articles published from 2020 to 2022 as researched in the MEDLINE database of Pub Med. The search and extraction of data were conducted in the month of September 2022. The inclusion and exclusion criteria are as follows: | |
| 2.3 | Inclusion Criteria | The articles that were included for this review were selected based on the inclusion criteria mentioned in Methods. | Criteria | Inclusion Eligibility |
| Theme of study | Studies related to the long-term effects of Covid-19, or post-sequalae of COVID-19 or post COVID-19. | |||
| Study Design | Original studies including Classical Article, Clinical Study, Clinical Trial, Multicenter Study and Observational Study. | |||
| Grey Literature | Preprints, case reports (Grey literature) specific to the objective | |||
| Publication Journal | The articles should have been published in a pre-reviewed journal. | |||
| Language | Articles in the English language | |||
| 2.4 | Exclusion Criteria | The articles that were excluded from selection for this review was based on the exclusion criteria as previously mentioned. | Criteria | Excluded articles |
| Theme of study | Those irrelevant to COVID-19 | |||
| Study Description | Studies not specific to objectives, studies reporting on patient characteristics and studies among participants that did not have a prior COVID-19 infection | |||
| Full text access | Unavailable full text | |||
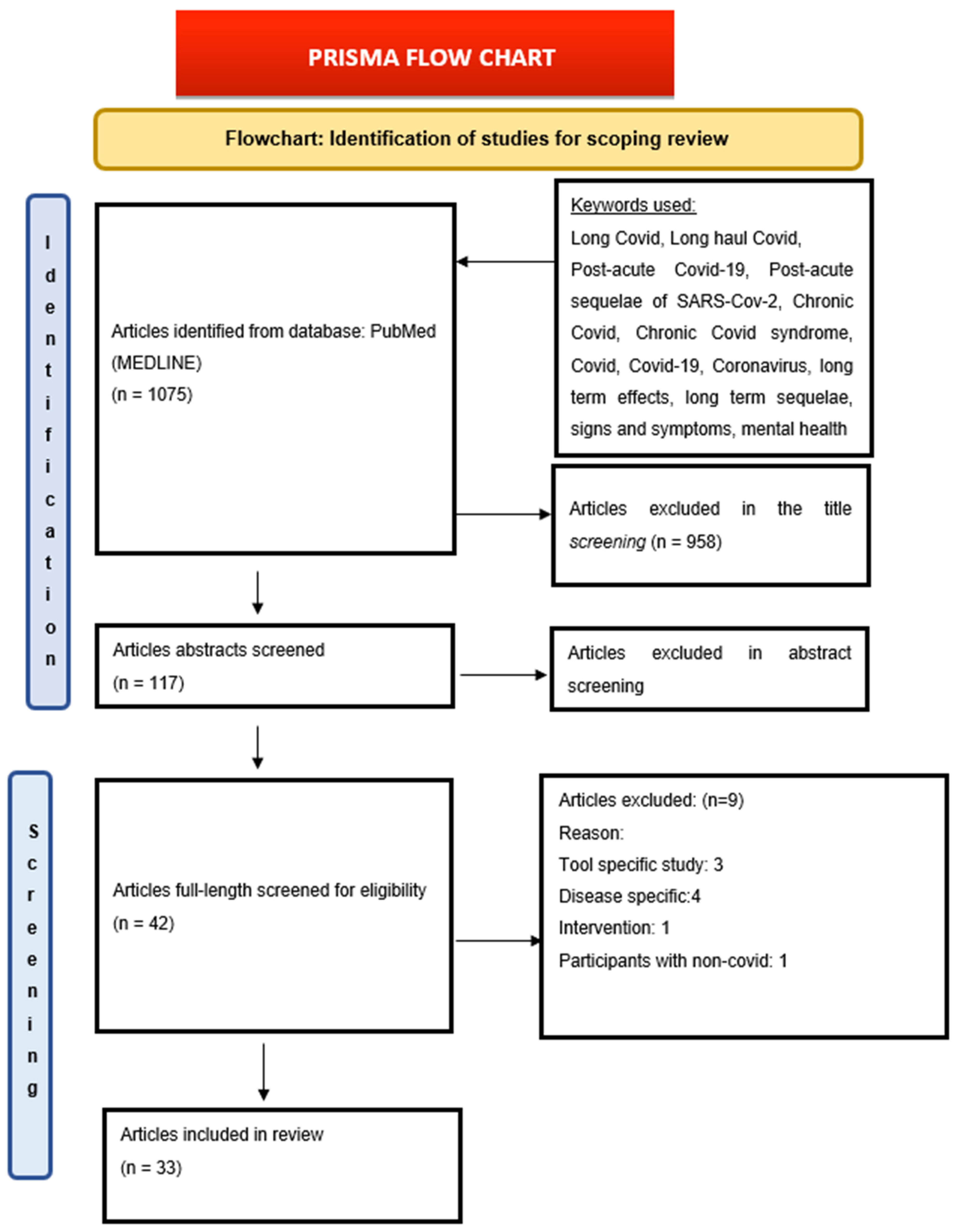
| 2.5 | Selection of sources of evidence | To select the appropriate articles from the results of the search | Using the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) extension for Scoping Reviews/(PRISMA-ScR) Checklist, we retrieved 1075 articles from our search (Figure 1). Title screening—958 articles were excluded as they were not in the context of post-COVID-19 but were included for Abstract screening—117 articles Full-text screening—42 included and 75 articles were excluded. (The reasons for exclusion are mentioned in Figure 1 in the results section). Included articles—33 The studies for this review were chosen in two stages. 1. The titles and abstracts of all retrieved studies were evaluated by one reviewer and then checked by another reviewer in the first stage. 2. The same reviewers read the entire texts of papers included in the first step independently in the second step. Any differences between the two reviewers were resolved by consulting a third reviewer. | |
| 2.6 | Data charting | To comprehensively review the articles included for the study and extract the variables under different categories for critical analysis | Data variables identified from the full text of articles are: Year of study, Study objectives, Keywords mentioned, Study design, study location, Study Population, Study sample size, Inclusion and exclusion criteria, COVID-19 Phase studied, Follow up, Symptoms reported, Major findings and Study limitations. | |
3. Results
3.1. Study Characteristics
3.2. Types of Articles Included
3.3. Timeline Brief
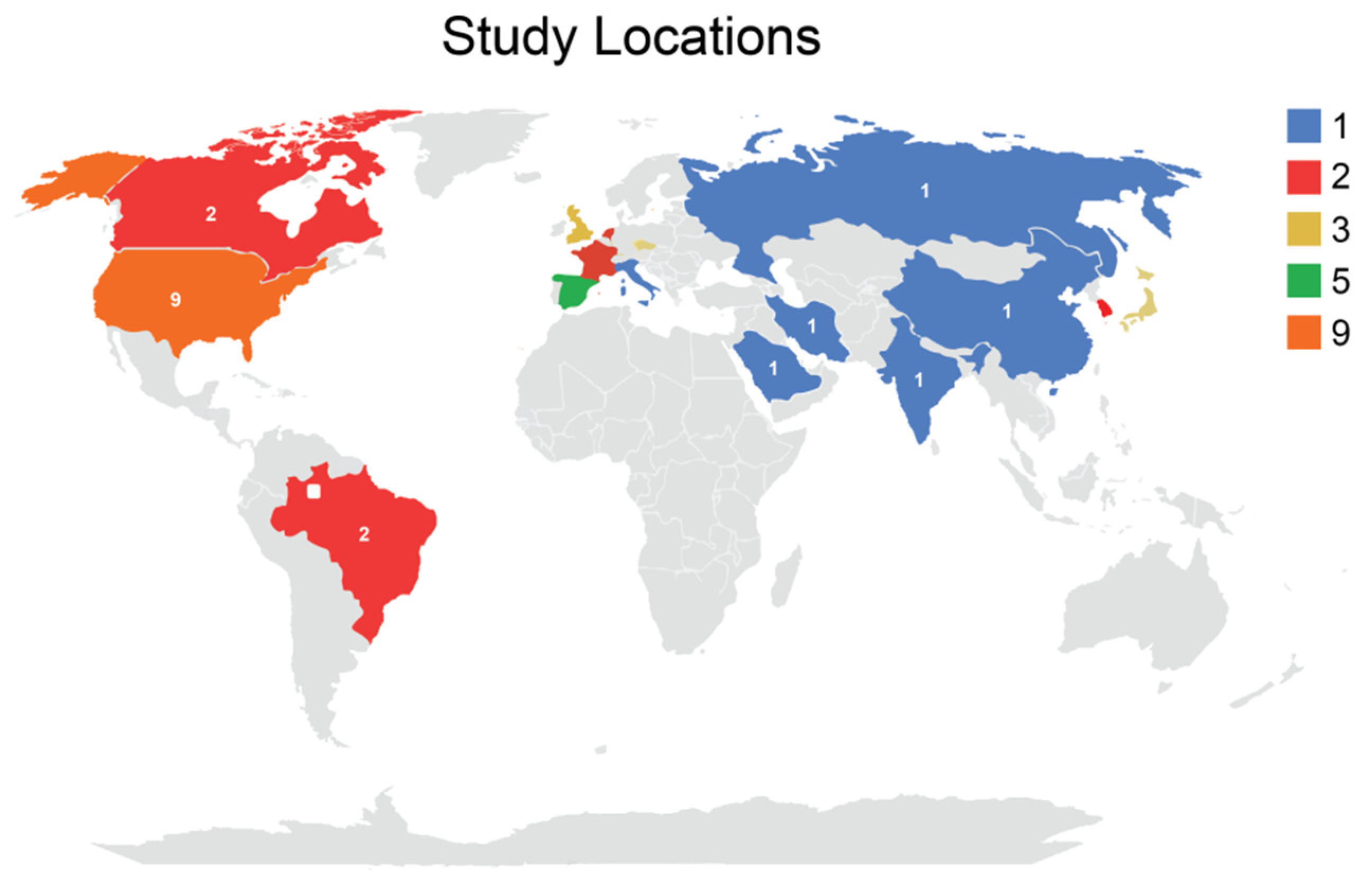
3.4. Study Location
3.5. Income Classification
3.6. Study Population
3.7. Number of Participants
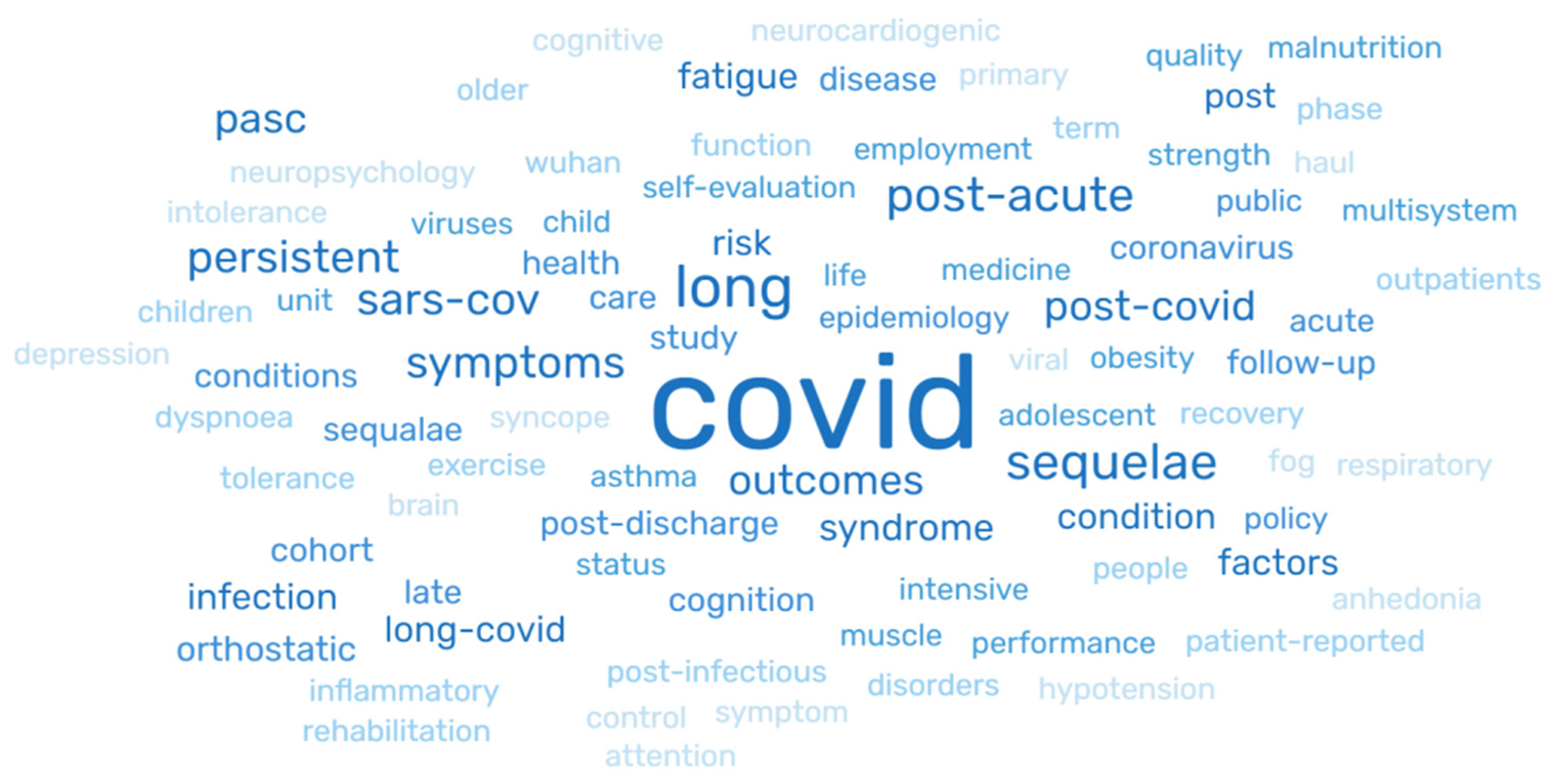
3.8. Keywords
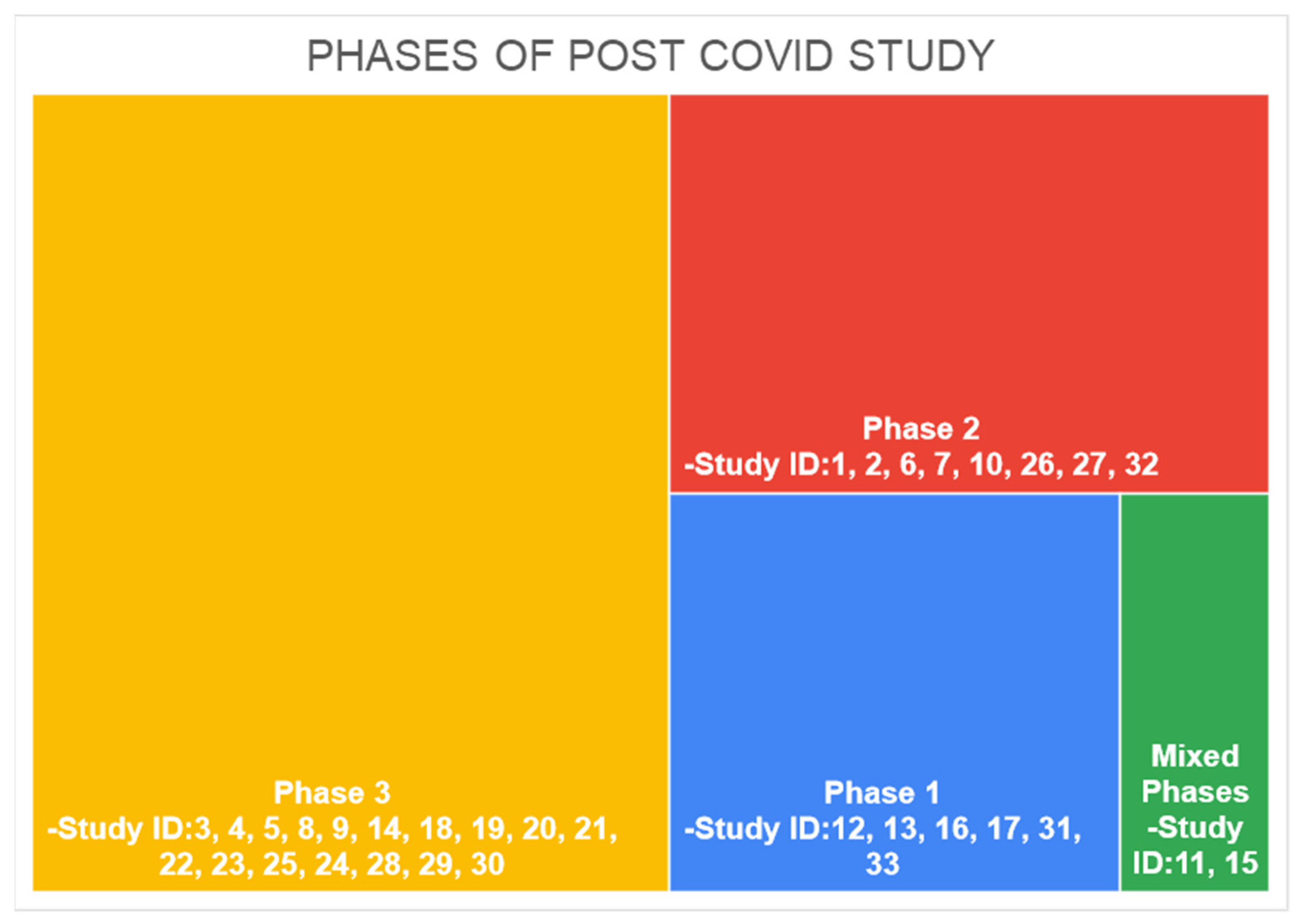
3.9. Phase of COVID Study
3.10. System Studied
3.11. Symptoms Presented
3.12. Physiological Symptoms Presented
3.13. Psychological Symptoms
3.14. Major Findings
4. Discussion
4.1. COVID Phase
4.2. Study Population
4.3. Signs and Symptoms
4.4. Risk Factors, Major Findings and Limitations
4.5. Impact of Long COVID-19 on Health and Quality of Lifestyle
4.6. Knowledge Gaps
5. Conclusions
6. Limitations
7. Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jahan, N.; Rubeshkumar, P.; Karuppiah, M.; Sambath, I.; Sendhilkumar, M.; Ilangovan, K.; Ongesh, R.; Sakthivel, M.; Mohankumar, R.; Kumar, M.S.; et al. Entry and initial spread of COVID-19 in India: Epidemiological analysis of media surveillance data, India, 2020. Clin. Epidemiol. Glob. Health 2020, 9, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Pollard, C.A.; Morran, M.P.; Nestor-Kalinoski, A.L. The COVID-19 pandemic: A global health crisis. Physiol. Genom. 2020, 52, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Harrich, D.; Li, Z.; Hu, D.; Li, D. The unique features of SARS-CoV-2 transmission: Comparison with SARS-CoV, MERS-CoV and 2009 H1N1 pandemic influenza virus. Rev. Med. Virol. 2021, 31, e2171. [Google Scholar] [CrossRef] [PubMed]
- Cramer, H. The Other Pandemic: Mental Health Before, During, and After COVID-19. J. Integr. Complement. Med. 2022, 28, 108–109. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, Y.; Chen, Y.; Qin, Q. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J. Med. Virol. 2020, 92, 568–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, M.S.; Shaik, R.A.; Ahmad, R.K.; Yusuf, M.; Khan, M.; Almutairi, A.B.; Alghuyaythat, W.K.Z.; Almutairi, S.B. “LONG COVID”: An insight. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5561–5577. [Google Scholar]
- Long Covid or Post-Covid Conditions. Centers for Disease Control and Prevention. Post-COVID Conditions | CDC. Saving Lives, Protecting People. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html#print (accessed on 22 October 2022).
- Brodin, P. Immune determinants of COVID-19 disease presentation and severity. Nat. Med. 2021, 27, 28–33. [Google Scholar] [CrossRef]
- Davido, B.; Seang, S.; Tubiana, R.; de Truchis, P. Post-COVID-19 chronic symptoms: A postinfectious entity? Clin. Microbiol. Infect. 2020, 26, 1448–1449. [Google Scholar] [CrossRef]
- Fernández-De-Las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Cuadrado, M.; Florencio, L. Defining Post-COVID Symptoms (Post-Acute COVID, Long COVID, Persistent Post-COVID): An Integrative Classification. Int. J. Environ. Res. Public Health 2021, 18, 2621. [Google Scholar] [CrossRef]
- Townsend, L.; Dowds, J.; O’Brien, K.; Sheill, G.; Dyer, A.H.; O’Kelly, B.; Hynes, J.P.; Mooney, A.; Dunne, J.; Ni Cheallaigh, C.; et al. Persistent Poor Health after COVID-19 Is Not Associated with Respiratory Complications or Initial Disease Severity. Ann. Am. Thorac. Soc. 2021, 18, 997–1003. [Google Scholar] [CrossRef]
- Coronavirus Disease (COVID-19): Post COVID-19 Condition [Internet]. World Health Organization. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-post-covid-19-condition (accessed on 22 October 2022).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Dennis, A.; Wamil, M.; Alberts, J.; Oben, J.; Cuthbertson, D.J.; Wootton, D.; Crooks, M.; Gabbay, M.; Brady, M.; Hishmeh, L.; et al. Multiorgan impairment in low-risk individuals with post-COVID-19 syndrome: A prospective, community-based study. BMJ Open 2021, 11, e048391. [Google Scholar] [CrossRef] [PubMed]
- Naik, S.; Haldar, S.N.; Soneja, M.; Mundadan, N.G.; Garg, P.; Mittal, A.; Desai, D.; Trilangi, P.K.; Chakraborty, S.; Begam, N.N.; et al. Post COVID-19 sequelae: A prospective observational study from Northern India. Drug Discov. Ther. 2021, 15, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Tabacof, L.; Tosto-Mancuso, J.; Wood, J.; Cortes, M.; Kontorovich, A.; McCarthy, D.; Rizk, D.; Rozanski, G.; Rozanski, E.; Nasr, L.; et al. Post-acute COVID-19 Syndrome Nega-tively Impacts Physical Function, Cognitive Function, Health-Related Quality of Life, and Participation. Am. J. Phys. Med. Rehabil. 2022, 101, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Bellan, M.; Baricich, A.; Patrucco, F.; Zeppegno, P.; Gramaglia, C.; Balbo, P.E.; Carriero, A.; Amico, C.S.; Avanzi, G.C.; Barini, M.; et al. Long-term sequelae are highly prevalent one year after hospitalization for severe COVID-19. Sci. Rep. 2021, 11, 22666. [Google Scholar] [CrossRef] [PubMed]
- Munblit, D.; Bobkova, P.; Spiridonova, E.; Shikhaleva, A.; Gamirova, A.; Blyuss, O.; Nekliudov, N.; Bugaeva, P.; Andreeva, M.; DunnGalvin, A.; et al. Incidence and risk factors for persistent symptoms in adults previously hospitalized for COVID-19. Clin. Exp. Allergy 2021, 51, 1107–1120. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nemati, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; et al. Risk factors associated with long covid syndrome: A retrospective study. Iran J. Med. Sci. 2021, 46, 428–436. [Google Scholar]
- Darcis, G.; Bouquegneau, A.; Maes, N.; Thys, M.; Henket, M.; Labye, F.; Rousseau, A.-F.; Canivet, P.; Desir, C.; Calmes, D.; et al. Long-term clinical follow-up of patients suffering from moderate-to-severe COVID-19 infection: A monocentric prospective observational cohort study. Int. J. Infect. Dis. 2021, 109, 209–216. [Google Scholar] [CrossRef]
- Gérard, M.; Mahmutovic, M.; Malgras, A.; Michot, N.; Scheyer, N.; Jaussaud, R.; Nguyen-Thi, P.-L.; Quilliot, D. Long-Term Evolution of Malnutrition and Loss of Muscle Strength after COVID-19: A Major and Neglected Component of Long COVID-19. Nutrients 2021, 13, 3964. [Google Scholar] [CrossRef]
- Cervia, C.; Zurbuchen, Y.; Taeschler, P.; Ballouz, T.; Menges, D.; Hasler, S.; Adamo, S.; Raeber, M.E.; Bächli, E.; Rudiger, A.; et al. Immunoglobulin signature predicts risk of post-acute COVID-19 syndrome. Nat. Commun. 2022, 13, 446. [Google Scholar] [CrossRef]
- Fink, T.T.; Marques, H.H.; Gualano, B.; Lindoso, L.; Bain, V.; Astley, C.; Martins, F.; Matheus, D.; Matsuo, O.M.; Suguita, P.; et al. Persistent symptoms and decreased health-related quality of life after symptomatic pediatric COVID-19: A prospective study in a Latin American tertiary hospital. Clinics 2021, 76, e3511. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.A.; Leavy, O.C.; Richardson, M.; Elneima, O.; McCauley, H.J.C.; Shikotra, A.; Singapuri, A.; Sereno, M.; Saunders, R.M.; Harris, V.C.; et al. Clinical characteristics with inflammation profiling of long COVID and association with 1-year recovery following hospitalisation in the UK: A prospective observation-al study. Lancet Respir. Med. 2022, 10, 761–775. [Google Scholar] [CrossRef] [PubMed]
- Twomey, R.; Demars, J.; Franklin, K.; Nicole Culos-Reed, S.; Weatherald, J.; Wrightson, J.G. Chronic Fatigue and Postexertional Ma-laise in People Living with Long COVID: An Observational Study. Phys. Ther. 2022, 102, pzac005. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.M.; Liu, T.C.; Motwani, Y.; Sim, M.S.; Viswanathan, N.; Samras, N.; Hsu, F.; Wenger, N.S. Factors Associated with Post-Acute Sequelae of SARS-CoV-2 (PASC) after Diagnosis of Symptomatic COVID-19 in the Inpatient and Outpatient Setting in a Diverse Cohort. J. Gen. Intern. Med. 2022, 37, 1988–1995. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Pellicer-Valero, O.J.; Navarro-Pardo, E.; Palacios-Ceña, D.; Florencio, L.L.; Guijarro, C.; Martín-Guerrero, J.D. Symptoms Experienced at the Acute Phase of SARS-CoV-2 Infection as Risk Factor of Long-term Post-COVID Symptoms: The LONG-COVID-EXP-CM Multicenter Study. Int. J. Infect. Dis. 2022, 116, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I.; Zyskind, I.; Naiditch, H.; Zimmerman, J.; Glatt, A.E.; Pinter, A.; Theel, E.S.; Joyner, M.J.; Hill, D.A.; Lieberman, M.R.; et al. Predictors of chronic COVID-19 symptoms in a community-based cohort of adults. PLoS ONE 2022, 17, e0271310. [Google Scholar] [CrossRef] [PubMed]
- AlRadini, F.A.; Alamri, F.; Aljahany, M.S.; Almuzaini, Y.; Alsofayan, Y.; Khan, A.; Albogami, N.; Abdulrahim, M.; Almogbil, A.; Alahmari, A. Post-acute COVID-19 condition in Saudi Arabia: A national representative study. J. Infect. Public Health 2022, 15, 526–532. [Google Scholar] [CrossRef]
- Berg, S.K.; Palm, P.; Nygaard, U.; Bundgaard, H.; Petersen, M.N.S.; Rosenkilde, S.; Thorsted, A.B.; Ersbøll, A.K.; Thygesen, L.C.; Nielsen, S.D.; et al. Long COVID symptoms in SARS-CoV-2-positive children aged 0-14 years and matched controls in Denmark (LongCOVIDKidsDK): A national, cross-sectional study. Lancet Child Adolesc. Health 2022, 6, 614–623. [Google Scholar] [CrossRef]
- Fang, X.; Ming, C.; Cen, Y.; Lin, H.; Zhan, K.; Yang, S.; Li, L.; Cao, G.; Li, Q.; Ma, X. Post-sequelae one year after hospital discharge among older COVID-19 patients: A multi-center prospective cohort study. J. Infect. 2021, 84, 179–186. [Google Scholar] [CrossRef]
- Battistella, L.R.; Imamura, M.; De Pretto, L.R.; Van Cauwenbergh, S.K.; Ramos, V.D.; Uchiyama, S.S.T.; Matheus, D.; Kuhn, F.; de Oliveira, A.A.A.; Naves, G.S.; et al. Long-term function-ing status of COVID-19 survivors: A prospective observational evaluation of a cohort of patients surviving hospitalisation. BMJ Open 2022, 12, e057246. [Google Scholar] [CrossRef]
- Seang, S.; Itani, O.; Monsel, G.; Abdi, B.; Marcelin, A.; Valantin, M.; Palich, R.; Fayçal, A.; Pourcher, V.; Katlama, C.; et al. Long COVID-19 symptoms: Clinical characteristics and recovery rate among non-severe outpatients over a six-month follow-up. Infect. Dis. Now 2022, 52, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Kingery, J.R.; Safford, M.M.; Martin, P.; Lau, J.D.; Rajan, M.; Wehmeyer, G.T.; Li, H.A.; Alshak, M.N.; Jabri, A.; Kofman, A.; et al. Health Status, Persistent Symptoms, and Effort Intolerance One Year After Acute COVID-19 Infection. J. Gen. Intern. Med. 2022, 37, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Han, J.H.; Womack, K.N.; Tenforde, M.W.; Files, D.C.; Gibbs, K.W.; Shapiro, N.I.; Prekker, M.E.; Erickson, H.L.; Steingrub, J.S.; Qadir, N.; et al. Associations between persistent symptoms after mild COVID-19 and long-term health status, quality of life, and psychological distress. Influenza Other Respir. Viruses 2022, 16, 680–689. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Izquierdo, M.; Láinez-Ramos-Bossini, A.J.; de Alba, I.G.F.; Ortiz-González-Serna, R.; Serrano-Ortiz, Á.; Fernández-Martínez, N.F.; Ruiz-Montero, R.; Cervilla, J.A. Long COVID 12 months after discharge: Persistent symptoms in patients hospitalised due to COVID-19 and pa-tients hospitalised due to other causes—A multicentre cohort study. BMC Med. 2022, 20, 92. [Google Scholar] [CrossRef] [PubMed]
- Fernández-De-Las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Palacios-Ceña, M.; Rodríguez-Jiménez, J.; De-La-Llave-Rincón, A.I.; Velasco-Arribas, M.; Fuensalida-Novo, S.; Ambite-Quesada, S.; Guijarro, C.; et al. Fatigue and Dyspnoea as Main Persistent Post-COVID-19 Symptoms in Previously Hospitalized Patients: Related Functional Limitations and Disability. Respiration 2021, 101, 132–141. [Google Scholar] [CrossRef]
- Schouborg, L.B.; Molsted, S.; Lendorf, M.E.; Hegelund, M.H.; Ryrsø, C.K.; Sommer, D.H.; Kolte, L.; Nolsöe, R.L.; Pedersen, T.I.; Harboe, Z.B.; et al. Risk factors for fatigue and impaired function eight months after hospital admission with COVID-19. Dan. Med. J. 2022, 69, A08210633. [Google Scholar]
- Jamal, S.M.; Landers, D.B.; Hollenberg, S.M.; Turi, Z.G.; Glotzer, T.V.; Tancredi, J.; Parrillo, J.E. Prospective Evaluation of Autonomic Dys-function in Post-Acute Sequela of COVID-19. J. Am. Coll. Cardiol. 2022, 79, 2325–2330. [Google Scholar] [CrossRef]
- Krishnan, K.; Miller, A.K.; Reiter, K.; Bonner-Jackson, A. Neurocognitive Profiles in Patients With Persisting Cognitive Symptoms Associated With COVID-19. Arch. Clin. Neuropsychol. 2022, 37, 729–737. [Google Scholar] [CrossRef]
- Pérez-González, A.; Araújo-Ameijeiras, A.; Fernández-Villar, A.; Crespo, M.; Poveda, E.; Cohort COVID-19 of the Galicia Sur Health Research Institute. Long COVID in hospi-talized and non-hospitalized patients in a large cohort in Northwest Spain, a prospective cohort study. Sci. Rep. 2022, 12, 3369. [Google Scholar] [CrossRef]
- Romero-Duarte, Á.; Rivera-Izquierdo, M.; de Alba, I.G.-F.; Pérez-Contreras, M.; Fernández-Martínez, N.F.; Ruiz-Montero, R.; Serrano-Ortiz, Á.; González-Serna, R.O.; Salcedo-Leal, I.; Jiménez-Mejías, E.; et al. Sequelae, persistent symptomatology and outcomes after COVID-19 hospitalization: The ANCOHVID multicentre 6-month follow-up study. BMC Med. 2021, 19, 129. [Google Scholar] [CrossRef]
- Horwitz, L.I.; Garry, K.; Prete, A.M.; Sharma, S.; Mendoza, F.; Kahan, T.; Karpel, H.; Duan, E.; Hochman, K.A.; Weerahandi, H. Six-Month Outcomes in Patients Hospitalized with Severe COVID-19. J. Gen. Intern. Med. 2021, 36, 3772–3777. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Barnett, J.; Brill, S.E.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; Hillman, T.E.; Jacob, J.; Jarvis, H.C.; et al. ‘Long-COVID’: A cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax 2020, 76, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.A.; McAuley, H.; Harrison, E.M.; Shikotra, A.; Singapuri, A.; Sereno, M.; Elneima, O.; Docherty, A.B.; Lone, N.I.; Leavy, O.C.; et al. Physical, cognitive, and mental health im-pacts of COVID-19 after hospitalisation (PHOSP-COVID): A UK multicentre, prospective cohort study. Lancet Respir. Med. 2021, 9, 1275–1287. [Google Scholar] [CrossRef] [PubMed]
- Lamontagne, S.J.; Winters, M.F.; Pizzagalli, D.A.; Olmstead, M.C. Post-acute sequelae of COVID-19: Evidence of mood & cognitive impairment. Brain Behav. Immun.-Health 2021, 17, 100347. [Google Scholar] [CrossRef]
- Fernández-De-Las-Peñas, C. Long COVID: Current definition. Infection 2021, 50, 285–286. [Google Scholar] [CrossRef]
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Houben, S.; Bonnechère, B. The Impact of COVID-19 Infection on Cognitive Function and the Implication for Rehabilitation: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 7748. [Google Scholar] [CrossRef]
- Shanbehzadeh, S.; Tavahomi, M.; Zanjari, N.; Ebrahimi-Takamjani, I.; Amiri-Arimi, S. Physical and mental health complications post-COVID-19: Scoping review. J. Psychosom. Res. 2021, 147, 110525. [Google Scholar] [CrossRef]
- van Kessel, S.A.M.; Olde Hartman, T.C.; Lucassen, P.L.B.J.; van Jaarsveld, C.H.M. Post-acute and long-COVID-19 symptoms in patients with mild diseases: A systematic review. Fam. Pract. 2022, 39, 159–167. [Google Scholar] [CrossRef]
- Mokhtari, T.; Hassani, F.; Ghaffari, N.; Ebrahimi, B.; Yarahmadi, A.; Hassanzadeh, G. COVID-19 and multiorgan failure: A narrative review on potential mechanisms. J. Mol. Histol. 2020, 51, 613–628. [Google Scholar] [CrossRef]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat. Med. 2022, 28, 1706–1714. [Google Scholar] [CrossRef] [PubMed]
- Burekovic, A.; Halilovic, D.; Sahbaz, A. Hypothyroidism and Subclinical Hypothyroidism as a Consequence of COVID-19 In-fection. Med. Arch. 2022, 76, 12. [Google Scholar] [CrossRef] [PubMed]
- Lui, D.T.W.; Lee, C.H.; Chow, W.S.; Lee, A.C.H.; Tam, A.R.; Fong, C.H.Y.; Law, C.Y.; Leung, E.K.H.; To, K.K.W.; Tan, K.C.B.; et al. Thyroid Dysfunction in Relation to Immune Profile, Disease Status, and Outcome in 191 Patients with COVID-19. J. Clin. Endocrinol. Metab. 2020, 106, e926–e935. [Google Scholar] [CrossRef]
- Peghin, M.; Palese, A.; Venturini, M.; De Martino, M.; Gerussi, V.; Graziano, E.; Bontempo, G.; Marrella, F.; Tommasini, A.; Fabris, M.; et al. Post-COVID-19 symptoms 6 months after acute infection among hospitalized and non-hospitalized patients. Clin. Microbiol. Infect. 2021, 27, 1507–1513. [Google Scholar] [CrossRef] [PubMed]
- Rudroff, T.; Workman, C.D.; Bryant, A.D. Potential Factors That Contribute to Post-COVID-19 Fatigue in Women. Brain Sci. 2022, 12, 556. [Google Scholar] [CrossRef] [PubMed]
- Taribagil, P.; Creer, D.; Tahir, H. ‘Long COVID’ syndrome. BMJ Case Rep. 2021, 14, 241485. [Google Scholar] [CrossRef] [PubMed]
- NHS. Long-Term Effects of Coronavirus (Long COVID)—NHS [Internet]. Available online: https://www.nhs.uk/conditions/coronavirus-covid-19/long-term-effects-of-coronavirus-long-covid/ (accessed on 22 October 2022).
- Bryant, V.; Holmes, A.; Irving, L. The mystery of “long COVID”: Up to 1 in 3 People Who Catch the Virus Suffer for Months. Here’s What We Know So Far [Internet]. Gavi.org. 2021. Available online: https://www.gavi.org/vaccineswork/mystery-long-covid-1-3-people-who-catch-virus-suffer-months-heres-what-we-know-so (accessed on 22 October 2022).
- Long COVID: Long-Term Effects of COVID-19|Johns Hopkins Medicine [Internet]. Johns Hopkins Medicine. p. 2022. Available online: https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/covid-long-haulers-long-term-effects-of-covid19 (accessed on 22 October 2022).
- Strain, W.D.; Sherwood, O.; Banerjee, A.; Van der Togt, V.; Hishmeh, L.; Rossman, J. The Impact of COVID Vaccination on Symptoms of Long COVID: An International Survey of People with Lived Experience of Long COVID. Vaccines 2022, 10, 652. [Google Scholar] [CrossRef]
- Chambers, P. Antioxidants and Long Covid [Internet]. preprints.org. Preprints. 2022. Available online: https://www.preprints.org/manuscript/202210.0195/v2 (accessed on 22 October 2022).
- Different SARS-CoV-2 Variants May Cause Different Long COVID Symptoms. Available online: https://www.medicalnewstoday.com/articles/different-sars-cov-2-variants-may-cause-different-long-covid-symptoms (accessed on 22 October 2022).
- Shah, W.; Hillman, T.; Playford, E.D.; Hishmeh, L. Managing the long term effects of covid-19: Summary of NICE, SIGN, and RCGP rapid guideline. Bmj 2021, 372, n136. [Google Scholar] [CrossRef]
- Alkodaymi, M.S.; Omrani, O.A.; Fawzy, N.A.; Abou Shaar, B.; Almamlouk, R.; Riaz, M.; Obeidat, M.; Obeidat, Y.; Gerberi, D.; Taha, R.M.; et al. Prevalence of post-acute COVID-19 syn-drome symptoms at different follow-up periods: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 28, 657–666. [Google Scholar] [CrossRef]
- Schou, T.M.; Joca, S.; Wegener, G.; Bay-Richter, C. Psychiatric and neuropsychiatric sequelae of COVID-19—A systematic review. Brain Behav. Immun. 2021, 97, 328–348. [Google Scholar] [CrossRef]




| S.No | Major Step | Methods |
|---|---|---|
| 3.1 | Results of Search | The electronic search of the Pub Med (MEDLINE) database generated 1075 research articles using relevant keywords that can provide maximum information available based on inclusion and exclusion criteria. The authors of the current study then screened the articles by their titles and abstracts. They then analyzed the entire texts of selected research publications, and 33 research publications (Table 3) were selected and included in the review (Figure 1). |
| 3.2 | Listing of selected studies | The lists of studies discussed in this review are presented in Table 3 with the assigned study number that would be used as the study identifier (Study ID) throughout the study. |
| Study ID | Title | First Author |
|---|---|---|
| 1 | Multi organ impairment in low-risk individuals with post-COVID-19 syndrome: a prospective, community-based study [14]. | Dennis, A. |
| 2 | Post COVID-19 squealae: A prospective observational study from Northern India [15]. | Naik, S. |
| 3 | Post-acute COVID-19 Syndrome Negatively Impacts Physical Function, Cognitive Function, Health-Related Quality of Life, and Participation [16]. | Tabacof, L. |
| 4 | Long-term sequelae are highly prevalent one year after hospitalization for severe COVID-19 [17]. | Bellan, M. |
| 5 | Incidence and risk factors for persistent symptoms in adults previously hospitalized for COVID-19 [18]. | Munblit, D. |
| 6 | Risk Factors Associated with Long COVID Syndrome: A Retrospective Study [19]. | Asadi-Pooya, A.A. |
| 7 | Long-term clinical follow-up of patients suffering from moderate-to-severe COVID-19 infection: a mono centric prospective observational cohort study [20]. | Darcis, G |
| 8 | Long-Term Evolution of Malnutrition and Loss of Muscle Strength after COVID-19: A Major and Neglected Component of Long COVID-19 [21]. | Gérard, M. |
| 9 | Immunoglobulin signature predicts risk of post-acute COVID-19 syndrome [22]. | Cervia, C. |
| 10 | Persistent symptoms and decreased health-related quality of life after symptomatic paediatric COVID-19: A prospective study in a Latin American tertiary hospital [23]. | Fink, T.T. |
| 11 | Clinical characteristics with inflammation profiling of long COVID and association with 1-year recovery following hospitalization in the UK: a prospective observational study [24]. | Evans, R.A. |
| 12 | Chronic Fatigue and Post exertional Malaise in People Living With Long COVID: An Observational Study [25]. | Twomey, R. |
| 13 | Factors Associated with Post-Acute Sequalae of SARS-CoV-2 (PASC) After Diagnosis of Symptomatic COVID-19 in the Inpatient and Outpatient Setting in a Diverse Cohort [26]. | Yoo, S.M. |
| 14 | Symptoms Experienced at the Acute Phase of SARS-CoV-2 Infection as Risk Factor of Long-term Post-COVID Symptoms: The LONG-COVID-EXP-CM Multicentre Study [27]. | Fernández-de-Las-Peñas, C. |
| 15 | Predictors of chronic COVID-19 symptoms in a community-based cohort of adults [28]. | Silverberg, J.I. |
| 16 | Post-acute COVID-19 condition in Saudi Arabia: A national representative study [29]. | AlRadini, F.A. |
| 17 | Long COVID symptoms in SARS-CoV-2-positive children aged 0–14 years and matched controls in Denmark (LongCOVIDKidsDK): a national, cross-sectional study [30]. | Kikkenborg Berg, S. |
| 18 | Post-sequalae one year after hospital discharge among older COVID-19 patients: A multi-centre prospective cohort study [31]. | Fang, X. |
| 19 | The long-term functioning status of COVID-19 survivors: a prospective observational evaluation of a cohort of patients surviving hospitalization [32]. | Battistella, L.R. |
| 20 | Long COVID-19 symptoms: Clinical characteristics and recovery rate among non-severe outpatients over a six-month follow-up [33]. | Seang, S. |
| 21 | Health Status, Persistent Symptoms, and Effort Intolerance One Year After Acute COVID-19 Infection [34]. | Kingery, J.R. |
| 22 | Associations between persistent symptoms after mild COVID-19 and long-term health status, quality of life, and psychological distress [35]. | Han, J.H. |
| 23 | Long COVID 12 months after discharge: persistent symptoms in patients hospitalised due to COVID-19 and patients hospitalized due to other causes-a multicentre cohort study [36]. | Rivera-Izquierdo, M. |
| 24 | Fatigue and Dyspnoea as Main Persistent Post-COVID-19 Symptoms in Previously Hospitalized Patients: Related Functional Limitations and Disability [37]. | Fernández-de-Las-Peñas, C. |
| 25 | Risk factors for fatigue and impaired function eight months after hospital admission with COVID-19 [38]. | Schouborg, L.B. |
| 26 | Prospective Evaluation of Autonomic Dysfunction in Post-Acute Sequela of COVID-19 [39]. | Jamal, S.M. |
| 27 | Neurocognitive Profiles in Patients With Persisting Cognitive Symptoms Associated With COVID-19 [40]. | Krishnan, K. |
| 28 | Long COVID in hospitalized and non-hospitalized patients in a large cohort in Northwest Spain, a prospective cohort study [41]. | Pérez-González, A. |
| 29 | Sequelae, persistent symptomatology and outcomes after COVID-19 hospitalization: the ANCOHVID multicentre 6-month follow-up study [42]. | Romero-Duarte, Á. |
| 30 | Six-Month Outcomes in Patients Hospitalized with Severe COVID-19 [43]. | Horwitz, L.I. |
| 31 | Long-COVID’: a cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalization for COVID-19 [44]. | Mandal, S. |
| 32 | Physical, cognitive, and mental health impacts of COVID-19 after hospitalization (PHOSP-COVID): a UK multicentre, prospective cohort study [45]. | Evans, R.A. |
| 33 | Post-acute sequelae of COVID-19: Evidence of mood and cognitive impairment [46]. | Lamontagne, S.J. |
| Study ID | Title | First Author | Year of Study | Location | Study Design | Keywords | Study Population Age Group (in years) | Sample Size (No. of Patients) | Phase of COVID-19 | Physiological Symptoms Assessed | Psychological Symptoms Assessed |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Multi organ impairment in low-risk individuals with post-COVID-19 syndrome: a prospective, community-based study [14]. | Dennis, A. | 2021 | UK | Observational study | COVID-19, epidemiology, health policy, public health | 18–64 | 201 | 2 | Fever, Headache, Cough, Dyspnea, Fatigue | - |
| 2 | Post COVID-19 sequelae: A prospective observational study from Northern India [15]. | Naik, S. | 2021 | India | Observational study | COVID-19, long COVID-19, post COVID-19 sequelae, post COVID-19 syndrome | 18–64 | 1234 | 2 | Chest Pain, Myalgia Insomnia, Cough, Dyspnea, Fatigue | Depression, Mood Disorders, Brain Fog |
| 3 | Post-acute COVID-19 Syndrome Negatively Impacts Physical Function, Cognitive Function, Health-Related Quality of Life, and Participation [16]. | Tabacof, L. | 2022 | USA | Observational study | Post-acute COVID-19, fatigue, cognition, employment, quality of life | 18–64 | 156 | 3 | Loss Of Appetite, Sweating, Tinnitus, Sexual Dysfunction, Neuropathic Pain, Abdominal Pain, Sore Throat, Dizziness, Vertigo, Syncope, Visual Impairment, Nausea, Hair loss, Diarrhea, Palpitation, Arthralgia, Chest Pain, Insomnia, Headache, Dyspnea, Fatigue | Memory Loss, Forgetfulness, Confusion |
| 4 | Long-term sequelae are highly prevalent one year after hospitalization for severe COVID-19 [17]. | Bellan, M. | 2021 | Italy | Observational study | microbiology virology | 18–64 | 238 | 3 | Hair Loss, Arthralgia, Anosmia, Chest Pain, Myalgia, Cough, Dyspnea, Fatigue | - |
| 5 | Incidence and risk factors for persistent symptoms in adults previously hospitalized for COVID-19 [18]. | Munblit, D. | 2021 | Russia | Clinical Trial | COVID-19, PAASC, asthma, long COVID-19, post COVID-19 Condition, Post COVID-19 syndrome, Post acute sequelae, SARS-CoV-2 infection, risk factor | 18–64 | 2649 | 3 | Vision Impairment, Hair loss, Myalgia Insomnia, Dyspnea, Fatigue | Memory Loss, Forgetfulness |
| 6 | Risk Factors Associated with Long COVID-19 Syndrome: A Retrospective Study [19]. | Asadi-Pooya, A.A. | 2021 | Iran | Multicentric study | COVID-19, medicine, SARA-CoV-2 Viruses | 18–64 | 4681 | 2 | Exertional Intolerance, Myalgia, Dyspnea, Fatigue | - |
| 7 | Long-term clinical follow-up of patients suffering from moderate-to-severe COVID-19 infection: a monocentric prospective observational cohort study [20]. | Darcis, G. | 2021 | Belgium | Observational study | COVID-19, long COVID-19, post COVID-19, post- acute COVID-19, sequelae | 18–64 | 199 | 2 | Hair Loss, Chest Pain, Cough, Dyspnea, Fatigue | - |
| 8 | Long-Term Evolution of Malnutrition and Loss of Muscle Strength after COVID-19: A Major and Neglected Component of Long COVID-19 [21]. | Gérard, M. | 2021 | England | Cohort study | Cohort study, intensive care unit, long COVID-19, malnutrition, muscle strength, obesity, performance status, self-evaluation. | 18–64 | 549 | 3 | Malnutrition, Palpitation | Memory Loss, Forgetfulness, Depression, Mood Disorders, Anxiety, Concentration Cognitive Impairment, Post Traumatic Stress, |
| 9 | Immunoglobulin signature predicts risk of post-acute COVID-19 syndrome [22]. | Cervia, C. | 2022 | Switzerland | Observational study | Not mentioned | 18–64 | 175 | 3 | Anosmia, Dyspnea, Fatigue, Ageusia | Depression, Mood Disorders, Anxiety |
| 10 | Persistent symptoms and decreased health-related quality of life after symptomatic pediatric COVID-19: A prospective study in a Latin American tertiary hospital [23]. | Fink, T.T. | 2021 | Brazil | Observational study | Long corona virus disease 2019, child, adolescent, sequelae, multisystem inflammatory syndrome in children | <18 | 105 | 2 | Anemia, Arthralgia, Myalgia, Insomnia, Headache, Dyspnea | Concentration and Cognitive Impairment |
| 11 | Clinical characteristics with inflammation profiling of long COVID-19 and association with 1-year recovery following hospitalization in the UK: a prospective observational study [24]. | Evans, R.A. | 2022 | UK | Observational study | Not mentioned | 18–64 | 2320 | Mixed | Exertional Intolerance, Arthralgia, Insomnia, Dyspnea, Fatigue, Ageusia | Memory Loss, Forgetfulness, Slowed Down Thinking |
| 12 | Chronic Fatigue and Post exertional Malaise in People Living With Long COVID-19: An Observational Study [25]. | Twomey, R. | 2022 | USA | Observational study | COVID-19, exercise tolerance, fatigue, long COVID-19, patient-reported outcomes, rehabilitation. | 18–64 | 213 | 1 | Loss Of Appetite, Sore Throat, Rashes, Dizziness, Vertigo, Vision Impairment, Nausea, Diarrhea, Fever Palpitation, Ageusia, Myalgia, Headache, Cough, Dyspnea, Fatigue | Brain Fog |
| 13 | Factors Associated with Post-Acute Sequelae of SARS-CoV-2 (PASC) After Diagnosis of Symptomatic COVID-19 in the Inpatient and Outpatient Setting in a Diverse Cohort [26]. | Yoo, S.M. | 2022 | USA | Observational study | Not mentioned | 18–64 | 1038 | 1 | Sinus, Rashes, Fever, Anosmia, Chest Pain, Ageusia, Dyspnea, Fatigue | Memory Loss, Forgetfulness, Brain Fog |
| 14 | Symptoms Experienced at the Acute Phase of SARS-CoV-2 Infection as Risk Factor of Long-term Post-COVID-19 Symptoms: The LONG-COVID-19-EXP-CM Multicentre Study [27]. | Fernández-de-Las-Peñas, C. | 2022 | Spain | Multicentric study | COVID-19, acute phase, persistent, risk factors symptoms | 18–64 | 1969 | 3 | Sore Throat, Rashes, Vision Impairment, Diarrhea, Palpitation, Anosmia, Ageusia, Dyspnea, Fatigue | - |
| 15 | Predictors of chronic COVID-19 symptoms in a community-based cohort of adults [28]. | Silverberg, J.I. | 2022 | USA | Observational study | Not mentioned | 18–64 | 390 | Mixed | Abdominal Pain, Headache, Fatigue | - |
| 16 | Post-acute COVID-19 condition in Saudi Arabia: A national representative study [29]. | AlRadini, F.A. | 2022 | Saudi Arabia | Multicentric study | Late symptoms, resistant symptoms, post-acute COVID-19, SARS-CoV-2 | 18–64 | 225 | 1 | Fever, Arthralgia, Anosmia, Ageusia, Headache, Dyspnea, Fatigue | - |
| 17 | Long COVID-19 symptoms in SARS-CoV-2-positive children aged 0–14 years and matched controls in Denmark (LongCOVID19 KidsDK): a national, cross-sectional study [30]. | Kikkenborg Berg, S. | 2022 | Denmark | Observational study | Not mentioned | <18 | 10997 | 1 | Arthralgia, Anosmia, Chest Pain, Myalgia Cough, Dyspnea, Fatigue | - |
| 18 | Post-sequelae one year after hospital discharge among older COVID-19 patients: A multi-centre prospective cohort study [31]. | Fang, X. | 2022 | China | Multicentric study | COVID-19, sequelae, older people, Wuhan, SARS-CoV-2 | >64 | 1233 | 3 | Sweating, Palpitations, Anosmia, Chest Pain, Ageusia, Myalgia, Cough Fatigue | Anxiety |
| 19 | The long-term functioning status of COVID-19 survivors: a prospective observational evaluation of a cohort of patients surviving hospitalization [32]. | Battistella, L.R. | 2022 | Italy | Multicentric study | COVID-19, rehabilitation, medicine, respiratory infections | 18–64 | 149 | 3 | Excessive Sleep, Exertional Intolerance, Insomnia, Dyspnea | Depression and More Disorders |
| 20 | Long COVID-19 symptoms: Clinical characteristics and recovery rate among non-severe outpatients over a six-month follow-up [33]. | Seang, S. | 2022 | France | Observational study | Long COVID-19, outpatients, post infectious disorders, recovery | 18–64 | 36 | 3 | Fever, Arthralgia, Anosmia, Chest Pain, Ageusia, Myalgia, Headache, Cough, Dyspnea | - |
| 21 | Health Status, Persistent Symptoms, and Effort Intolerance One Year After Acute COVID-19 Infection [34]. | Kingery, J.R. | 2022 | USA | Observational study | COVID-19, PASCA, Persistent symptoms | 18–64 | 530 | 3 | Numbness, Abdominal Pain, Diarrhea, Headache, Dyspnea, Fatigue | Brain Fog |
| 22 | Associations between persistent symptoms after mild COVID-19 and long-term health status, quality of life, and psychological distress [35]. | Han, J.H. | 2022 | USA | Multicentric study | COVID-19, outcomes, long COVID-19 postacute sequalae of COVID-19, PASC, post COVID-19conditions | 18–64 | 2092 | 3 | Hair loss, Exertional Intolerance, Chest Pain, Ageusia, Insomnia, Fatigue, Dyspnea | Concentration and Cognition Impairment |
| 23 | Long COVID-19 12 months after discharge: persistent symptoms in patients hospitalized due to COVID-19 and patients hospitalized due to other causes-a multicentre cohort study [36]. | Rivera-Izquierdo, M. | 2022 | Spain | Multicentric study | Cohort, follow up, long term, persistent COVID-19, sequalae | 18–64 | 163 | 3 | Arthralgia, Insomnia, Headache, Fatigue | Memory Loss, Forgetfulness, Depression, Mood Disorders, Anxiety, Confusion |
| 24 | Fatigue and Dyspnea as Main Persistent Post-COVID-19 Symptoms in Previously Hospitalized Patients: Related Functional Limitations and Disability [37]. | Fernández-de-Las-Peñas, C. | 2022 | Spain | Multicentric study | COVID-19, dyspnea, fatigue, function, risk factors | 18–64 | 1142 | 3 | Diarrhoea, Palpitation, Chest Pain, Cough, Fatigue, Dyspnea | - |
| 25 | Risk factors for fatigue and impaired function eight months after hospital admission with COVID-19 [38]. | Schouborg, L.B. | 2022 | Denmark | Observational study | Not mentioned | 18–64 | 83 | 3 | Loss Of Functional Status Fatigue | - |
| 26 | Prospective Evaluation of Autonomic Dysfunction in Post-Acute Sequela of COVID-19 [39]. | Jamal, S.M. | 2022 | USA | Observational study | HUTT, neurocardiogenic syncope, orthostatic hypotension, intolerance, POTS | 18–64 | 24 | 2 | Palpitations, Exertional Intolerance, Chest Pain, Headache, Fatigue | Concentration and Cognition Impairment |
| 27 | Neurocognitive Profiles in Patients With Persisting Cognitive Symptoms Associated With COVID-19 [40]. | Krishnan, K. | 2022 | USA | Observational study | Brain fog, COVID-19, cognition, long COVID-19, neuropsychology | 18–64 | 20 | 2 | Dizziness, Vertigo, Nausea, Diarrhea, Palpitation, Exertional Intolerance, Arthralgia, Insomnia, Cough, Dyspnea, Fatigue | Memory Loss, Forgetfulness, Brain Fog, Concentration and Cognition Impairment |
| 28 | Long COVID-19 in hospitalized and non-hospitalized patients in a large cohort in Northwest Spain, a prospective cohort study [41]. | Pérez-González, A. | 2022 | Spain | Clinical trial | Not mentioned | 18–64 | 248 | 3 | Hair Loss, Anosmia, Ageusia, Myalgia, Insomnia, Headache, Cough, Dyspnea, Fatigue | - |
| 29 | Sequelae, persistent symptomatology and outcomes after COVID-19 hospitalization: the ANCOHVID multicentre 6-month follow-up study [42]. | Romero-Duarte, Á. | 2021 | Spain | Observational study | COVID-19, long COVID-19, post discharge, sequelae, persistent symptoms, primary care, follow up | 18–64 | 797 | 3 | Fever, Numbness, Malnutrition, Anemia, Constipation, Rib Pain, Dysuria, Hemautria, Oliguria, Exertional Intolerance Abdominal Pain, Nausea, Glycemia, Renal Problems, Rashes, Hair loss, Diarrhea, Dizziness, Vertigo Or Syncope, Vision Impairment, Anosmia, Myalgia, Insomnia, Cough, Fatigue | Anxiety and Confusion |
| 30 | Six-Month Outcomes in Patients Hospitalized with Severe COVID-19 [43]. | Horwitz, L.I. | 2021 | USA | Observational study | COVID-19, long COVID-19, patient reported outcomes, post discharge outcomes | 18–64 | 152 | 3 | Numbness, Tinnitus, Rashes, Dizziness, Vertigo Or Syncope, Vision Impairment, Nausea, Palpitations, Anosmia, Insomnia, Headache, Dyspnea, Fatigue | Memory Loss, Forgetfulness, Brain Fog, Concentration and Cognition Impairment |
| 31 | Long-COVID-19: a cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalization for COVID-19 [44]. | Mandal, S. | 2021 | UK | Observational study | Respiratory infection, viral infection | 18–64 | 348 | 1 | Dyspnea, Fatigue, Cough | Depression and Mood Disorders |
| 32 | Physical, cognitive, and mental health impacts of COVID-19 after hospitalization (PHOSP-COVID): a UK multicentre, prospective cohort study [45]. | Evans, R.A. | 2021 | UK | Multicentric study | Not mentioned | 18–64 | 1077 | 2 | Exertional Intolerance, Arthralgia, Insomnia, Dyspnea, Fatigue | Memory Loss, Forgetfulness, Slowed Down Thinking |
| 33 | Post-acute sequelae of COVID-19: Evidence of mood & cognitive impairment [46]. | Lamontagne, S.J. | 2021 | Canada | Multicentric study | Corona virus disease, SARS-CoV-2, PASC, ANT, inflammation, cognitive control, anhedonia, depression, | 18–64 | 50 | 1 | Sinus, Sore Throat Nausea, Diarrhea, Fever, Ageusia, Headache, Cough, Dyspnea, Fatigue | - |
| Study Design | Number of Studies(%) | Study ID |
|---|---|---|
| Observational study | 20 (60.6) | 1, 2, 3, 4, 6, 7, 10, 11, 12, 13, 15, 17, 20, 21, 25, 26, 27, 29,30, 31 |
| Multicentric study | 10 (30.3) | 9, 14, 16, 18, 19, 22, 23, 24, 32, 33 |
| Clinical Trials | 2 (6) | 5, 28 |
| Cohort Study | 1 (3) | 8 |
| Study location Income Classification | Number of Studies = n (%) | Study ID |
|---|---|---|
| High-income economies | 27 (81.8) | 1, 3, 4, 7, 8, 9, 11, 12, 13, 14, 15, 16, 17, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33 |
| Upper-middle income | 4 (12.12) | 5, 10, 18, 19 |
| Lower-middle income | 2 (6) | 2, 6 |
| Study Population | Number of Studies = n (%) | Study ID |
|---|---|---|
| Children | 2 (6%) | 10, 17 |
| Elderly | 1 (3%) | 18 |
| Adult | 30 (91%) | All other studies |
| Physiological Symptoms | Total Studies = (n) (%) | Study IDs |
|---|---|---|
| Performance and Perceived Fatigue/tiredness/weakness | 29 (87) | 1, 2, 3, 4, 5, 6, 7, 9, 11, 12, 13, 14, 15, 16, 17, 18, 21, 22, 23, 24, 25, 26, 27,28, 29, 30, 31, 32, 33 |
| Shortness of breath/Dyspnea/Breathlessness | 26 (78) | 1, 2, 3, 4, 5, 6,7, 9, 10, 11, 12, 13, 14,16,17, 19, 20, 21, 22, 24, 27, 28, 30, 31, 32, 33 |
| Cough | 15 (45) | 1, 2, 4, 7, 12, 15, 17, 18, 20, 24, 27, 28, 29, 31, 33 |
| Headache | 13 (39) | 1, 3, 10, 12, 15, 16, 20, 21, 23, 26, 28, 30, 33 |
| Insomnia | 13 (39) | 2, 3, 5, 10, 11, 19, 22, 23, 27, 28, 29, 30, 32 |
| Myalgia | 12 (36) | 2, 4, 5,6, 10, 17, 18, 20, 28, 29, 33, 12 |
| Ageusia/loss of taste | 12(36) | 9, 11, 12, 13, 14, 16, 18, 20, 22, 28, 30, 33 |
| Chest pain/tightness | 11 (33) | 2, 3, 4, 7, 13, 17, 18, 20, 22, 24, 26 |
| Anosmia/loss of smell | 11(33) | 4, 9, 13, 14, 16, 17, 18, 20, 28, 29,30 |
| Arthralgia | 10 (30) | 3, 4, 10, 11, 16, 17, 20, 23, 27, 32 |
| Exertional intolerance | 8 (24) | 6, 11, 26. 27, 19, 22, 29, 32 |
| Palpitation | 8 (24) | 3, 8, 12, 14, 18, 24, 26, 27, 30 |
| Fever | 7 (21) | 1, 12, 13, 16, 20, 29, 33 |
| Diarrhoea | 8 (24) | 3, 12, 14, 21, 24, 27, 29, 33 |
| Hair loss | 7 (21) | 3, 4, 5, 7, 22, 28, 29 |
| Nausea/vomiting | 6 (18) | 3, 12, 27, 29, 30, 33 |
| Vision impairment/eye problems | 6 (18) | 3, 5, 12, 14, 29, 30 |
| Dizziness/vertigo/syncope | 5 (15) | 3, 12, 27, 29, 30 |
| Rashes in skin/skin disorders | 5 (15) | 12, 13, 14, 29, 30 |
| Sore throat/throat pain | 4 (12) | 3, 12, 14, 33 |
| Abdomen pain | 4 (12) | 3, 15, 21, 29 |
| Numbness/paresthesia | 3 (9) | 21, 29, 30 |
| loss of appetite | 2 (6) | 3, 12 |
| Malnutrition | 2 (6) | 8, 29 |
| Anemia | 2 (6) | 10, 29 |
| Sweating | 2 (6) | 3, 18 |
| Tinnitus | 2 (6) | 3, 30 |
| Sinus/nasal congestion | 2 (6) | 12, 33 |
| Sexual dysfunction | 1(3) | 3 |
| Excessive sleepiness | 1 (3) | 19 |
| Neuropathic pain | 1 (3) | 3 |
| Constipation | 1 (3) | 39 |
| Loss of functional status | 1 (3) | 25 |
| Rib pain/thoracic pain | 1 (3) | 29 |
| Dysuria, haematuria, oliguria | 1 (3) | 29 |
| Glycaemia/renal problems | 1 (3) | 29 |
| Psychological Symptoms | Total Studies, n (%) | Study IDs |
|---|---|---|
| Memory loss/forgetfulness | 9 (27) | 3, 5, 8, 11, 14, 23, 27, 30, 32 |
| Depression and Mood disorders | 7 (21) | 2, 3, 8, 9, 19, 23, 31 |
| Brain fog | 6 (18) | 2, 12, 14, 21, 27, 30 |
| Anxiety | 6 (18) | 8, 9, 18, 19, 23, 29 |
| Concentration/cognitive impairment | 6 (18) | 8, 10, 22, 26, 27, 30 |
| Confusion | 3 (9) | 3, 23,29 |
| Slowdowned thinking | 2 (6) | 11, 32 |
| Post-traumatic stress | 1 (3) | 8 |
| Phase | No. of Studies | Study ID | Major Limitations |
|---|---|---|---|
| 1 | 6 | 12, 13, 16, 17, 31, 33 | Selection bias: People presenting with symptoms were more likely to participate. Mothers of children with a greater number of symptoms are more inclined to join. No comparative group of participants representing non-hospitalised patients. Recall bias. Based on the purely behavioural nature of the study, precise mechanisms underlying the link between COVID-19 and depression remain unknown. |
| 2 | 8 | 1, 2, 6, 7, 10, 26, 27, 32 | Incidental findings were possible in asymptomatic individuals. The study population was not ethnically diverse. Selection bias: the study was only from tertiary hospitals; four studies reported this limitation. Phone data collection. Loss to follow up. Median of 4 months assessed; need long-term follow up. Relatively small sample size. |
| 3 | 17 | 3, 4, 5, 8, 9, 14, 18, 19, 20, 21, 22, 23, 25, 24, 28, 29, 30 | The lack of validated scales to measure most of the symptoms. Relatively small sample size. Failed to show a clear association between severity of symptoms. Retrospective studies have recall bias. Most studies used subjective methods to assess symptoms and not objective measures; for example, pulmonary tests, blood oxygen saturation, inflammatory biomarkers or chest X-rays. Telephonic data collection; the absence of a control group for comparison. Loss to follow up. |
| Mixed | 2 | 11, 15 | Selection bias for participants returning for a 1-yearvisit. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Surapaneni, K.M.; Singhal, M.; Saggu, S.R.; Bhatt, A.; Shunmathy, P.; Joshi, A. A Scoping Review on Long COVID-19: Physiological and Psychological Symptoms Post-Acute, Long-Post and Persistent Post COVID-19. Healthcare 2022, 10, 2418. https://doi.org/10.3390/healthcare10122418
Surapaneni KM, Singhal M, Saggu SR, Bhatt A, Shunmathy P, Joshi A. A Scoping Review on Long COVID-19: Physiological and Psychological Symptoms Post-Acute, Long-Post and Persistent Post COVID-19. Healthcare. 2022; 10(12):2418. https://doi.org/10.3390/healthcare10122418
Chicago/Turabian StyleSurapaneni, Krishna Mohan, Manmohan Singhal, Sofia Rani Saggu, Ashruti Bhatt, Priya Shunmathy, and Ashish Joshi. 2022. "A Scoping Review on Long COVID-19: Physiological and Psychological Symptoms Post-Acute, Long-Post and Persistent Post COVID-19" Healthcare 10, no. 12: 2418. https://doi.org/10.3390/healthcare10122418