
Implications of Type 2 Diabetes Mellitus in Patients with Acute Cholangitis: A Systematic Review of Current Literature
 ,
,  , and
, and 
Abstract
:1. Introduction
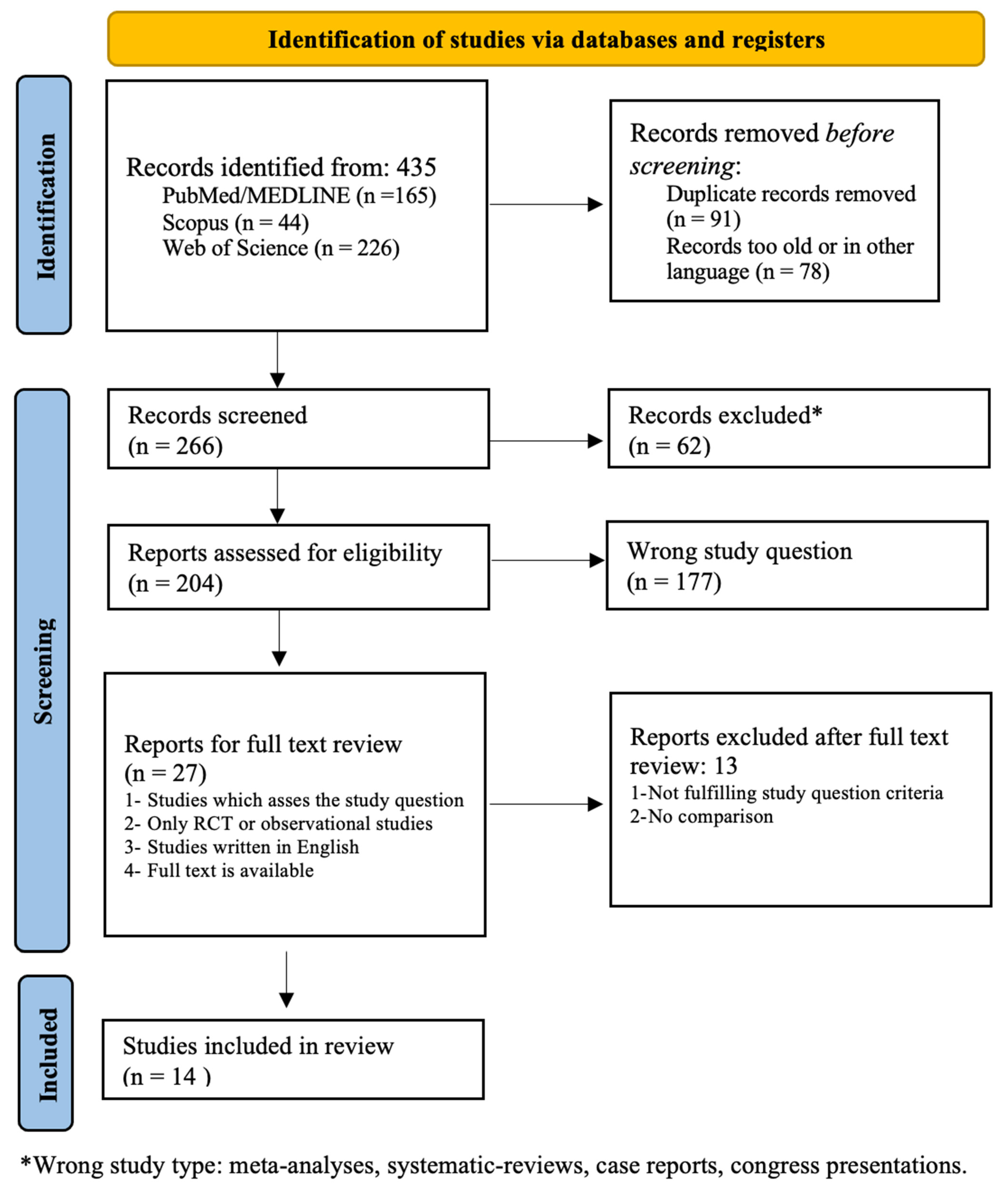
2. Materials and Methods
Data Sources and Searches
3. Results
4. Discussion
4.1. Research on T2DM and AC: Why Is There Still a Need for This Review?
4.2. Mechanism of Acute Cholangitis
4.2.1. Risk Factors for AC
4.2.2. Association of AC and T2DM
4.3. Predicting Bile Duct Complications
4.4. Assessing the Association of T2DM with Gallstone Pancreatitis and Bile Duct Complications
4.5. Post-ERCP Bile Duct Complications
4.6. T2DM Management Complicated by AC
4.7. Predicting the Severity of AC and the Risk of Mortality
4.8. Predicting Complications in the Treatment of AC
4.8.1. Non-Surgical Approach for AC in T2DM
4.8.2. Predicting Complications during AC Management in T2DM
4.8.3. Predicting Increased Length of Hospital Stay
4.8.4. Predicting Antibiotic Resistance
4.8.5. Aiming to Predict the Risk of Recurrence and Readmission after Treatment of AC
4.9. Recommendations for Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Reiter, F.P.; Obermeier, W.; Jung, J.; Denk, G.; Mahajan, U.M.; De Toni, E.N.; Schirra, J.; Mayerle, J.; Schulz, C. Prevalence, Resistance Rates, and Risk Factors of Pathogens in Routine Bile Cultures Obtained during Endoscopic Retrograde Cholangiography. Dig. Dis. 2021, 39, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Gomi, H.; Takada, T.; Hwang, T.L.; Akazawa, K.; Mori, R.; Endo, I.; Miura, F.; Kiriyama, S.; Matsunaga, N.; Itoi, T.; et al. Updated comprehensive epidemiology, microbiology, and outcomes among patients with acute cholangitis. J. Hepatobiliary Pancreat. Sci. 2017, 24, 310–318. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.-C.; Chang, I.-J.; Lai, Y.-C.; Chen, S.-Y.; Chen, S.-C. Epidemiology and prognostic determinants of patients with bacteremic cholecystitis or cholangitis. Am. J. Gastroenterol. 2007, 102, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Reuken, P.A.; Torres, D.; Baier, M.; Löffler, B.; Lübbert, C.; Lippmann, N.; Stallmach, A.; Bruns, T. Risk factors for multi-drug resistant pathogens and failure of empiric first-line therapy in acute cholangitis. PLoS ONE 2017, 12, e0169900. [Google Scholar]
- Sung, Y.K.; Lee, J.K.; Lee, K.H.; Lee, K.T.; Kang, C.I. The clinical epidemiology and outcomes of bacteremic biliary tract infections caused by antimicrobial-resistant pathogens. Am. J. Gastroenterol. 2012, 107, 473–483. [Google Scholar] [CrossRef]
- Masuda, S.; Koizumi, K.; Uojima, H.; Kimura, K.; Nishino, T.; Tasaki, J.; Ichita, C.; Sasaki, A. Effect of Antibiotic Resistance of Pathogens on Initial Antibiotic Therapy for Patients With Cholangitis. Cureus 2021, 13, e18449. [Google Scholar] [CrossRef] [PubMed]
- Tagashira, Y.; Sakamoto, N.; Isogai, T.; Hikone, M.; Kosaka, A.; Chino, R.; Higuchi, M.; Uehara, Y.; Honda, H. Impact of inadequate initial antimicrobial therapy on mortality in patients with bacteraemic cholangitis: A retrospective cohort study. Clin. Microbiol. Infect. 2017, 23, 740–747. [Google Scholar] [CrossRef] [Green Version]
- Negm, A.A.; Schott, A.; Vonberg, R.P.; Weismueller, T.J.; Schneider, A.S.; Kubicka, S.; Strassburg, C.P.; Manns, M.P.; Suerbaum, S.; Wedemeyer, J.; et al. Routine bile collection for microbiological analysis during cholangiography and its impact on the management of cholangitis. Gastrointest. Endosc. 2010, 72, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Suh, S.W.; Choi, Y.S.; Choi, S.H.; Do, J.H.; Oh, H.C.; Kim, H.J.; Lee, S.E. Antibiotic selection based on microbiology and resistance profiles of bile from gallbladder of patients with acute cholecystitis. Sci. Rep. 2021, 11, 2969. [Google Scholar] [CrossRef]
- Sokal, A.; Sauvanet, A.; Fantin, B.; de Lastours, V. Acute cholangitis: Diagnosis and management. J. Visc. Surg. 2019, 156, 515–525. [Google Scholar] [CrossRef]
- Masadeh, M.; Chandra, S.; Livorsi, D.; Johlin, F.; Silverman, W. Evaluation of biliary bacterial resistance in patients with frequent biliary instrumentation, one size does not fit all. Dig. Dis. Sci. 2018, 63, 3474–3479. [Google Scholar] [CrossRef]
- Kaya, M.; Beştaş, R.; Bacalan, F.; Bacaksız, F.; Arslan, E.G.; Kaplan, M.A. Microbial profile and antibiotic sensitivity pattern in bile cultures from endoscopic retrograde cholangiography patients. World J. Gastroenterol. 2012, 18, 3585–3589. [Google Scholar] [CrossRef]
- Shafagh, S.; Rohani, S.H.; Hajian, A. Biliary infection; distribution of species and antibiogram study. Ann. Med. Surg. 2021, 70, 102822. [Google Scholar] [CrossRef] [PubMed]
- Englesbe, M.J.; Dawes, L.G. Resistant pathogens in biliary obstruction: Importance of cultures to guide antibiotic therapy. HPB 2005, 7, 144–148. [Google Scholar] [CrossRef] [Green Version]
- Chandra, S.; Klair, J.S.; Soota, K.; Livorsi, D.J.; Johlin, F.C. Endoscopic Retrograde Cholangio-Pancreatography-Obtained Bile Culture Can Guide Antibiotic Therapy in Acute Cholangitis. Dig. Dis. 2019, 37, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Melzer, M.; Toner, R.; Lacey, S.; Bettany, E.; Rait, G. Biliary tract infection and bacteraemia: Presentation, structural abnormalities, causative organisms and clinical outcomes. Postgrad Med. J. 2007, 83, 773–776. [Google Scholar] [CrossRef] [Green Version]
- Ortega, M.; Marco, F.; Soriano, A.; Almela, M.; Martínez, J.A.; López, J.; Pitart, C.; Mensa, J. Epidemiology and prognostic determinants of bacteraemic biliary tract infection. J. Antimicrob. Chemother. 2012, 67, 1508–1513. [Google Scholar] [CrossRef]
- Yokoe, M.; Hata, J.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Wakabayashi, G.; Kozaka, K.; Endo, I.; Deziel, D.J.; Miura, F.; et al. Tokyo Guidelines 2018, diagnostic criteria and severity grading of acute cholecystitis (with videos). J. Hepatobiliary Pancreat. Sci. 2018, 25, 41–54. [Google Scholar] [CrossRef]
- Carey, I.M.; Critchley, J.A.; DeWilde, S.; Harris, T.; Hosking, F.J.; Cook, D.G. Risk of infection in type 1 and type 2 diabetes compared with the general population: A matched cohort study. Diabetes Care 2018, 41, 513–521. [Google Scholar] [CrossRef] [Green Version]
- Korbel, L.; Spencer, J.D. Diabetes mellitus and infection: An evaluation of hospital utilization and management costs in the United States. J. Diabetes Complicat. 2015, 29, 192–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casqueiro, J.; Casqueiro, J.; Alves, C. Infections in patients with diabetes mellitus: A review of pathogenesis. Indian J. Endocrinol. Metab. 2012, 16 (Suppl. S1), S27–S36. [Google Scholar] [PubMed]
- Sohouli, M.H.; Fatahi, S.; Sharifi-Zahabi, E.; Santos, H.O.; Tripathi, N.; Lari, A.; Pourrajab, B.; Kord-Varkaneh, H.; Găman, M.A.; Shidfar, F. The Impact of Low Advanced Glycation End Products Diet on Metabolic Risk Factors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2021, 12, 766–776. [Google Scholar] [CrossRef] [PubMed]
- Abu-Ashour, W.; Twells, L.K.; Valcour, J.E.; Gamble, J.M. Diabetes and the occurrence of infection in primary care: A matched cohort study. BMC Infect. Dis. 2018, 18, 67. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71.0. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Kummerow, K.L.; Shelton, J.; Phillips, S.; Holzman, M.D.; Nealon, W.; Beck, W.; Sharp, K.; Poulose, B.K. Predicting complicated choledocholithiasis. J. Surg. Res. 2012, 177, 70–74. [Google Scholar] [CrossRef]
- Mohan, R.; Wei Lynn Goh, S.; Tan, G.W.; Tan, Y.P.; Junnarkar, S.P.; Huey, C.W.T.; Low, J.K.; Shelat, V.G. Validation of Tokyo Guidelines 2007 and Tokyo Guidelines 2013/2018 Criteria for Acute Cholangitis and Predictors of In-Hospital Mortality. Visc. Med. 2021, 37, 434–442. [Google Scholar] [CrossRef]
- Parikh, M.P.; Garg, R.; Chittajallu, V.; Gupta, N.; Sarvepalli, S.; Lopez, R.; Thota, P.N.; Siddiki, H.; Bhatt, A.; Chahal, P.; et al. Trends and risk factors for 30-day readmissions in patients with acute cholangitis: Analysis from the national readmission database. Surg. Endosc. 2021, 35, 223–231. [Google Scholar] [CrossRef]
- García-Alonso, F.J.; de Lucas Gallego, M.; Bonillo Cambrodón, D.; Algaba, A.; de la Poza, G.; Martín-Mateos, R.M.; Bermejo, F. Gallstone-related disease in the elderly: Is there room for improvement? Dig. Dis. Sci. 2015, 60, 1770–1777. [Google Scholar] [CrossRef]
- Liu, Q.; Zhou, Q.; Song, M.; Zhao, F.; Yang, J.; Feng, X.; Wang, X.; Li, Y.; Lyu, J. A nomogram for predicting the risk of sepsis in patients with acute cholangitis. J. Int. Med. Res. 2020, 48, 300060519866100. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Wang, L.; Wang, Y.; Wei, W.; Yao, Y.L.; Ling, T.S.; Shen, Y.H.; Zou, X.P. Risk factor analysis of post-ERCP cholangitis: A single-center experience. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Khoury, T.; Sbeit, W. Diabetes mellitus is associated with a higher rate of acute cholangitis among patients with common bile duct stones: A retrospective study. Medicine 2022, 101, e28687. [Google Scholar] [CrossRef] [PubMed]
- Charlier, C.; Fevre, C.; Travier, L.; Cazenave, B.; Bracq-Dieye, H.; Podevin, J.; Assomany, D.; Guilbert, L.; Bossard, C.; Carpentier, F.; et al. Listeria monocytogenes-associated biliary tract infections: A study of 12 consecutive cases and review. Medicine 2014, 93, e105. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.B.; Kim, T.N.; Chung, H.H.; Kim, K.H. Small Gallstone Size and Delayed Cholecystectomy Increase the Risk of Recurrent Pancreatobiliary Complications After Resolved Acute Biliary Pancreatitis. Dig. Dis. Sci. 2017, 62, 777–783. [Google Scholar] [CrossRef]
- Mak, M.H.W.; Low, J.K.; Junnarkar, S.P.; Huey, T.C.W.; Shelat, V.G. A prospective validation of Sepsis-3 guidelines in acute hepatobiliary sepsis: qSOFA lacks sensitivity and SIRS criteria lacks specificity (Cohort Study). Int. J. Surg. 2019, 72, 71–77. [Google Scholar] [CrossRef]
- Sahu, M.K.; Chacko, A.; Dutta, A.K.; Prakash, J.A.J. Microbial profile and antibiotic sensitivity pattern in acute bacterial cholangitis. Indian J. Gastroenterol. 2011, 30, 204–208. [Google Scholar] [CrossRef]
- Jirapinyo, P.; AlSamman, M.A.; Thompson, C.C. Impact of infected stent removal on recurrent cholangitis with time-to-event analysis. Surg. Endosc. 2019, 33, 4109–4115. [Google Scholar] [CrossRef]
- Faillie, J.L.; Yu, O.H.; Yin, H.; Hillaire-Buys, D.; Barkun, A.; Azoulay, L. Association of Bile Duct and Gallbladder Diseases With the Use of Incretin-Based Drugs in Patients With Type 2 Diabetes Mellitus. JAMA Intern Med. 2016, 176, 1474–1481. [Google Scholar] [CrossRef]
- Tan, M.; Schaffalitzky de Muckadell, O.B.; Laursen, S.B. Unchanged mortality in patients with acute cholangitis despite an increase in malignant etiologies—A 25-year epidemiological study. Scand J. Gastroenterol. 2019, 54, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Yeom, D.H.; Oh, H.J.; Son, Y.W.; Kim, T.H. What are the risk factors for acute suppurative cholangitis caused by common bile duct stones? Gut Liver 2010, 4, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Lee, S.H.; Chung, K.H.; Park, J.M.; Lee, B.S.; Paik, W.H.; Park, J.K.; Ryu, J.K.; Kim, Y.T. Risk factors of organ failure in cholangitis with bacteriobilia. World J. Gastroenterol. 2015, 21, 7506–7513. [Google Scholar] [CrossRef]
- Schneider, J.; Hapfelmeier, A.; Thöres, S.; Obermeier, A.; Schulz, C.; Pförringer, D.; Nennstiel, S.; Spinner, C.; Schmid, R.M.; Algül, H.; et al. Mortality Risk for Acute Cholangitis (MAC): A risk prediction model for in-hospital mortality in patients with acute cholangitis. BMC Gastroenterol. 2016, 16, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimura, Y.; Takada, T.; Kawarada, Y.; Nimura, Y.; Hirata, K.; Sekimoto, M.; Yoshida, M.; Mayumi, T.; Wada, K.; Miura, F.; et al. Definitions, pathophysiology, and epidemiology of acute cholangitis and cholecystitis: Tokyo Guidelines. J. Hepatobiliary Pancreat. Surg. 2007, 14, 15–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feingold, K.R.; Anawalt, B.; Boyce, A.; Chrousos, G.; de Herder, W.W.; Dhatariya, K.; Dungan, K.; Hershman, J.M.; Hofland, J. Dyslipidemia in Diabetes. [Updated 10 August 2020]. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. Available online: https://www.ncbi.nlm.nih.gov/books/NBK305900/ (accessed on 1 July 2022).
- Shebl, F.M.; Andreotti, G.; Rashid, A.; Gao, Y.T.; Yu, K.; Shen, M.C.; Wang, B.S.; Li, Q.; Han, T.Q.; Zhang, B.H.; et al. Diabetes in relation to biliary tract cancer and stones: A population-based study in Shanghai, China. Br. J. Cancer 2010, 103, 115–119. [Google Scholar] [CrossRef] [Green Version]
- Tan, J.; Kou, J. Advances in Research on the Pathogenesis of Type 2 Diabetes Complicated with Gallstone. Int. J. Clin. Med. 2019, 10, 161–173. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.M.; Yu, C.H.; Chen, H.T.; Shen, Z.; Hu, F.L.; Yuan, X.P.; Xu, G.Q. Study on Helicobacter DNA of Biliary System of Gallstone Disease. Chin. J. Pract. Surg. 2004, 24, 84–87. [Google Scholar]
- Karamanos, E.; Sivrikoz, E.; Beale, E.; Chan, L.; Inaba, K.; Demetriades, D. Effect of Diabetes on Outcomes in Patients Undergoing Emergent Cholecystectomy for Acute Cholecystitis. World J. Surg. 2013, 37, 2257–2264. [Google Scholar] [CrossRef]
- Carrillo-Larco, R.M.; Anza-Ramírez, C.; Saal-Zapata, G.; Villarreal-Zegarra, D.; Zafra-Tanaka, J.H.; Ugarte-Gil, C.; Ugarte-Gil, C.; Bernabé-Ortiz, A. Type 2 diabetes mellitus and antibiotic-resistant infections: A systematic review and meta-analysis. J. Epidemiol. Community Health 2022, 76, 75–84. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| First Author | Year of Publication | Study Design | Country | No. of Participants | Mean Age | Gender | No. of Participants with T2DM | No. of Participants without T2DM | Outcome of AC in pts with DM | Outcome of AC in pts without T2DM | Other Comorbidities |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Kummerow et al. [27] | 2012 | Retrospective study | USA | 123,990 | Uncomplicated CL 56.5 ± 0.36 year AP-60.3 0.40 y | Male/Female | 21.8% of patients with AC had T2DM—20,956 | 20,956 | Third predictor of mortality (OR = 1.14), after complications and alcoholism. | CHF, chronic lung disease, T2DM, HT, obesity, renal failure | |
| Mohan et al. [28] | 2021 | Retrospective study | Singapore | 388 | 75.9 years | Male/Female | Diagnosed in 46.8% of those with a definite diagnosis—100 | 162 | Higher proportion in severe forms (48%), compared to moderate (37.8%) and mild (40.3%) ones (p = 0.197). | ||
| Parikh et al. [29] | 2021 | Retrospective cohort study | USA | Male/Female | Risk of readmission at 30 days is significantly greater in those with T2DM (p = 0.003). | ||||||
| Garcia-Alonso et al. [30] | 2015 | Retrospective study | 491 | 78.8 (71.9–84.7) | 51.7% women | 117 | 374 | After an acute event (AP, AC, cholecystitis) underlined that diabetes was associated more frequent with a non-surgical approach (p = 0.09). | |||
| Liu et al. [31] | 2020 | Retrospective review | USA | 662 | 70.7 +/− 14.7 | Male/Female | 23 | 639 | Diabetes (OR: 10.74, 95% CI: 2.80–70.57) was associated with the risk of sepsis in AC. | ||
| Chen M et al. [32] | 2018 | Retrospective study | China | 110 + 2174 | 74 over 60 years old | 50% females | 256 | 3978 | Risk factor for post-ERCP complications such as AC (p < 0.05). | ||
| Khoury and Sbeit [33] | 2022 | Retrospective study | Israel | 101 + 586 | 77.7 ± 13.6 | 47.5% females | 53 (52.5) in group A (CL with AC) and 213 (36.3) in group B (CL without AC) (p = 0.001) | 48 in group A and 373 in group B | Associated with AC development (OR 1.92, p = 0.002). | ||
| Charlier et al. [34] | 2014 | Retrospective study | France | 20 | 69 | 50% female | 3 | 17 | Recurrence in 1 patient needing 6 weeks amoxicillin and 2 drainages f/b cure in 2 yrs. Cure in other 2 pts. | ||
| Kim et al. [35] | 2017 | Retrospective study | Republic of Korea | 290 | 66.8 ± 16.0 | 53.1% female | 52 | 238 | CBD-related complications (AP, CL or AC) (p = 0.334). | ||
| Mak et al. [36] | 2019 | Prospective study | Singapore | 124 | 64.5 | 39.5% female | 34 (7%) | 90 | Severe cases with admission in high-dependency units (HDU) (p = 0.003). | ||
| Sahu MK et al. [37] | 2011 | Retrospective and prospective study | India | 185 | 51.3 ± 13.4 | 55.1% male | 25 (13.5%) | 160 | Not mentioned as paper is about need for a change in empirical antibiotic policy for AC. | Not mentioned. | |
| Jirapinyo et al. [38] | 2019 | Retrospective cohort | USA | 182 | 64 | 49% female | 55 (30%) | 127 | Not mentioned as paper is about stent exchange at the time of AC, which was more effective in preventing recurrence. | Absence of T2DM did not decrease the risk of disease recurrence. | HT |
| Faillie J et al. [39] | 2016 | Comparative study | Canada | 71369 | GLP-1 analogous 57.1 years DPP-4 inhibitors 65.1 years Others 62.3 years | Male/Female | 71369 | None | This study assessed AC and other gallbladder diseases as a complication from noninsulin antidiabetic drugs, mainly: GLP-1 analogues and DPP-4 inhibitors not as a complication from DM itself. Total of 853 were hospitalized for gallbladder disease. | Null | Null |
| Tan M et al. [40] | 2019 | Epidemiological study | Denmark | 755 | 72 ± 9 | Male/Female | 176 (29 had complications) | 579 | All of them having AC. | All of them having AC. | AMI, cancer, CVA, CHF, connective tissue disorder, dementia, HIV 1, liver disease, metastatic cancer, paraplegia, PUD, PVD, pulmonary disease, renal disease, severe liver disease. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cozma, M.-A.; Dobrică, E.-C.; Shah, P.; Shellah, D.; Găman, M.-A.; Diaconu, C.C. Implications of Type 2 Diabetes Mellitus in Patients with Acute Cholangitis: A Systematic Review of Current Literature. Healthcare 2022, 10, 2196. https://doi.org/10.3390/healthcare10112196
Cozma M-A, Dobrică E-C, Shah P, Shellah D, Găman M-A, Diaconu CC. Implications of Type 2 Diabetes Mellitus in Patients with Acute Cholangitis: A Systematic Review of Current Literature. Healthcare. 2022; 10(11):2196. https://doi.org/10.3390/healthcare10112196
Chicago/Turabian StyleCozma, Matei-Alexandru, Elena-Codruta Dobrică, Purva Shah, Duha Shellah, Mihnea-Alexandru Găman, and Camelia Cristina Diaconu. 2022. "Implications of Type 2 Diabetes Mellitus in Patients with Acute Cholangitis: A Systematic Review of Current Literature" Healthcare 10, no. 11: 2196. https://doi.org/10.3390/healthcare10112196