

AI-Supported Comprehensive Detection and Quantification of Biomarkers of Subclinical Widespread Diseases at Chest CT for Preventive Medicine
 , , , , , add
Show full author list
, , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Team
2.2. Training Data
2.3. Algorithm Training
2.3.1. Adipose Tissue and Metabolic Imaging
2.3.2. Cardiovascular Comorbidities
2.3.3. Pulmonal Parenchyma Abnormalities
2.3.4. Pulmonary Nodules
2.3.5. Osteoporosis
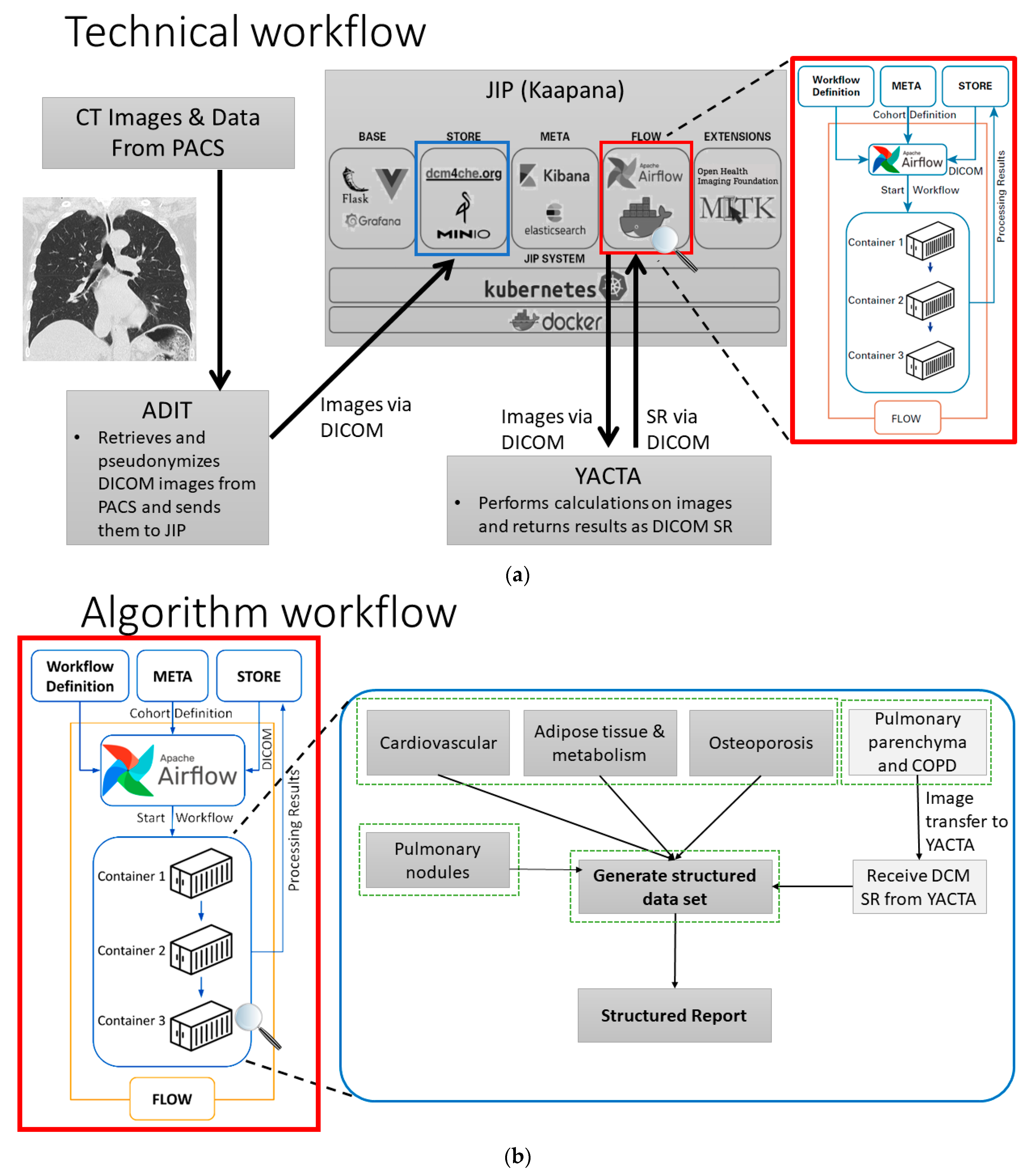
2.4. Technical Set-Up

{kind=link}
{kind=link}
{kind=link}
| Comorbidity | Parameter |
|---|---|
| Adipose tissue and metabolism | |
| Cardiovascular |
|
| Pulmonary parenchyma and COPD | |
| Pulmonary nodule |
|
| Osteoporosis |
|
3. Results
3.1. Workflow
3.2. Output
3.2.1. Example No. 1 ‘TAVI Patient’
3.2.2. Example No. 2 ‘COPD Patient’
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khan, M.S.; Samman Tahhan, A.; Vaduganathan, M.; Greene, S.J.; Alrohaibani, A.; Anker, S.D.; Vardeny, O.; Fonarow, G.C.; Butler, J. Trends in Prevalence of Comorbidities in Heart Failure Clinical Trials. Eur. J. Heart Fail. 2020, 22, 1032–1042. [Google Scholar] [CrossRef] [PubMed]
- Kopf, S.; Groener, J.B.; Kender, Z.; Fleming, T.; Brune, M.; Riedinger, C.; Volk, N.; Herpel, E.; Pesta, D.; Szendrödi, J.; et al. Breathlessness and Restrictive Lung Disease: An Important Diabetes-Related Feature in Patients with Type 2 Diabetes. Respir. Int. Rev. Thorac. Dis. 2018, 96, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. Obesity Management Task Force of the European Association for the Study of Obesity European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef]
- Hoffmann, U.; Massaro, J.M.; Fox, C.S.; Manders, E.; O’Donnell, C.J. Defining Normal Distributions of Coronary Artery Calcium in Women and Men (from the Framingham Heart Study). Am. J. Cardiol. 2008, 102, 1136–1141.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atsou, K.; Chouaid, C.; Hejblum, G. Variability of the Chronic Obstructive Pulmonary Disease Key Epidemiological Data in Europe: Systematic Review. BMC Med. 2011, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 8 August 2022).
- MacMahon, H.; Austin, J.H.M.; Gamsu, G.; Herold, C.J.; Jett, J.R.; Naidich, D.P.; Patz, E.F.; Swensen, S.J. Fleischner Society Guidelines for Management of Small Pulmonary Nodules Detected on CT Scans: A Statement from the Fleischner Society. Radiology 2005, 237, 395–400. [Google Scholar] [CrossRef] [Green Version]
- MacMahon, H.; Naidich, D.P.; Goo, J.M.; Lee, K.S.; Leung, A.N.C.; Mayo, J.R.; Mehta, A.C.; Ohno, Y.; Powell, C.A.; Prokop, M.; et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology 2017, 284, 228–243. [Google Scholar] [CrossRef] [Green Version]
- Löffler, M.T.; Jacob, A.; Valentinitsch, A.; Rienmüller, A.; Zimmer, C.; Ryang, Y.-M.; Baum, T.; Kirschke, J.S. Improved Prediction of Incident Vertebral Fractures Using Opportunistic QCT Compared to DXA. Eur. Radiol. 2019, 29, 4980–4989. [Google Scholar] [CrossRef] [Green Version]
- Cosman, F.; de Beur, S.J.; LeBoff, M.S.; Lewiecki, E.M.; Tanner, B.; Randall, S.; Lindsay, R.; National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporos. Int. 2014, 25, 2359–2381. [Google Scholar] [CrossRef] [Green Version]
- Doğan, N.; Varlibaş, Z.N.; Erpolat, O.P. Radiological Report: Expectations of Clinicians. Diagn. Interv. Radiol. Ank. Turk. 2010, 16, 179–185. [Google Scholar] [CrossRef] [Green Version]
- Eberhardt, S.C.; Heilbrun, M.E. Radiology Report Value Equation. Radiographics 2018, 38, 1888–1896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruparel, M.; Quaife, S.L.; Dickson, J.L.; Horst, C.; Burke, S.; Taylor, M.; Ahmed, A.; Shaw, P.; Soo, M.-J.; Nair, A.; et al. Evaluation of Cardiovascular Risk in a Lung Cancer Screening Cohort. Thorax 2019, 74, 1140–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howe, T.E.; Shea, B.; Dawson, L.J.; Downie, F.; Murray, A.; Ross, C.; Harbour, R.T.; Caldwell, L.M.; Creed, G. Exercise for Preventing and Treating Osteoporosis in Postmenopausal Women. Cochrane Database Syst. Rev. 2011, CD000333. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Kokkinos, P.; Nyelin, E. Physical Activity, Cardiorespiratory Fitness, and the Metabolic Syndrome. Nutrients 2019, 11, 1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bovolini, A.; Garcia, J.; Andrade, M.A.; Duarte, J.A. Metabolic Syndrome Pathophysiology and Predisposing Factors. Int. J. Sport. Med. 2021, 42, 199–214. [Google Scholar] [CrossRef] [PubMed]
- Scoditti, E.; Massaro, M.; Garbarino, S.; Toraldo, D.M. Role of Diet in Chronic Obstructive Pulmonary Disease Prevention and Treatment. Nutrients 2019, 11, 1357. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Cabello, A.; Ara, I.; González-Agüero, A.; Casajús, J.A.; Vicente-Rodríguez, G. Effects of Training on Bone Mass in Older Adults: A Systematic Review. Sport. Med. Auckl. N. Z. 2012, 42, 301–325. [Google Scholar] [CrossRef]
- Camacho, P.M.; Petak, S.M.; Binkley, N.; Diab, D.L.; Eldeiry, L.S.; Farooki, A.; Harris, S.T.; Hurley, D.L.; Kelly, J.; Lewiecki, E.M.; et al. American Association of Clinical Endocrinologists/ American College of Endocrinology Clinical Practice Guidlines for the Diagnosis and Treatment of Postmenopausal Osteoporosis—2020 Update. Endocr. Pract. 2020, 26, 1–46. [Google Scholar] [CrossRef]
- Faiza, Z.; Sharman, T. Thoracic Aorta Aneurysm. StatPearls 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554567/ (accessed on 18 October 2022).
- Gampala, S.; Vankeshwaram, V.; Gadula, S.S.P. Is Artificial Intelligence the New Friend for Radiologists? A Review Article. Cureus 2020, 12, e11137. [Google Scholar] [CrossRef]
- McKinney, S.M.; Sieniek, M.; Godbole, V.; Godwin, J.; Antropova, N.; Ashrafian, H.; Back, T.; Chesus, M.; Corrado, G.S.; Darzi, A.; et al. International Evaluation of an AI System for Breast Cancer Screening. Nature 2020, 577, 89–94. [Google Scholar] [CrossRef]
- Loehfelm, T.W. Artificial Intelligence for Quality Improvement in Radiology. Radiol. Clin. N. Am. 2021, 59, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Ranschaert, E.; Topff, L.; Pianykh, O. Optimization of Radiology Workflow with Artificial Intelligence. Radiol. Clin. N. Am. 2021, 59, 955–966. [Google Scholar] [CrossRef] [PubMed]
- Fink, M.A.; Mayer, V.L.; Schneider, T.; Seibold, C.; Stiefelhagen, R.; Kleesiek, J.; Weber, T.F.; Kauczor, H.-U. CT Angiography Clot Burden Score from Data Mining of Structured Reports for Pulmonary Embolism. Radiology 2022, 302, 175–184. [Google Scholar] [CrossRef]
- Alsharif, W.; Qurashi, A. Effectiveness of COVID-19 Diagnosis and Management Tools: A Review. Radiogr. Lond. Engl. 1995 2021, 27, 682–687. [Google Scholar] [CrossRef]
- Rezazade Mehrizi, M.H.; van Ooijen, P.; Homan, M. Applications of Artificial Intelligence (AI) in Diagnostic Radiology: A Technography Study. Eur. Radiol. 2021, 31, 1805–1811. [Google Scholar] [CrossRef] [PubMed]
- Sollmann, N.; Kirschke, J.S.; Kronthaler, S.; Boehm, C.; Dieckmeyer, M.; Vogele, D.; Kloth, C.; Lisson, C.G.; Carballido-Gamio, J.; Link, T.M.; et al. Imaging of the Osteoporotic Spine—Quantitative Approaches in Diagnostics and for the Prediction of the Individual Fracture Risk. ROFO Fortschr. Geb. Rontgenstr. Nukl. 2022, 194, 1088–1099. [Google Scholar] [CrossRef]
- Li, M.D.; Chang, K.; Mei, X.; Bernheim, A.; Chung, M.; Steinberger, S.; Kalpathy-Cramer, J.; Little, B.P. Radiology Implementation Considerations for Artificial Intelligence (AI) Applied to COVID-19, From the AJR Special Series on AI Applications. AJR Am. J. Roentgenol. 2022, 219, 15–23. [Google Scholar] [CrossRef]
- Wolf, I.; Vetter, M.; Wegner, I.; Böttger, T.; Nolden, M.; Schöbinger, M.; Hastenteufel, M.; Kunert, T.; Meinzer, H.-P. The Medical Imaging Interaction Toolkit. Med. Image Anal. 2005, 9, 594–604. [Google Scholar] [CrossRef]
- Heussel, C.P.; Achenbach, T.; Buschsieweke, C.; Kuhnigk, J.; Weinheimer, O.; Hammer, G.; Düber, C.; Kauczor, H.-U. Quantification of pulmonary emphysema in multislice-CT using different software tools. ROFO Fortschr. Geb. Rontgenstr. Nukl. 2006, 178, 987–998. [Google Scholar] [CrossRef]
- Weinheimer, O.; Achenbach, T.; Bletz, C.; Duber, C.; Kauczor, H.U.; Heussel, C.P. About Objective 3-d Analysis of Airway Geometry in Computerized Tomography. IEEE Trans. Med. Imaging 2008, 27, 64–74. [Google Scholar] [CrossRef]
- Konietzke, P.; Wielpütz, M.O.; Wagner, W.L.; Wuennemann, F.; Kauczor, H.-U.; Heussel, C.P.; Eichinger, M.; Eberhardt, R.; Gompelmann, D.; Weinheimer, O. Quantitative CT Detects Progression in COPD Patients with Severe Emphysema in a 3-Month Interval. Eur. Radiol. 2020, 30, 2502–2512. [Google Scholar] [CrossRef] [PubMed]
- Kauczor, H.-U.; Wielpütz, M.O.; Jobst, B.J.; Weinheimer, O.; Gompelmann, D.; Herth, F.J.F.; Heussel, C.P. Computed Tomography Imaging for Novel Therapies of Chronic Obstructive Pulmonary Disease. J. Thorac. Imaging 2019, 34, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Syngo.via—Siemens Healthineers. Available online: https://www.siemens-healthineers.com/medical-imaging-it/syngo-carbon-products/syngovia (accessed on 23 August 2022).
- Fortschrittliche Visualisierung | Philips Healthcare. Available online: https://www.philips.de/healthcare/alle-produkte/klinische-it/advanced-visualization (accessed on 23 August 2022).
- Isensee, F.; Jaeger, P.F.; Kohl, S.A.A.; Petersen, J.; Maier-Hein, K.H. NnU-Net: A Self-Configuring Method for Deep Learning-Based Biomedical Image Segmentation. Nat. Methods 2021, 18, 203–211. [Google Scholar] [CrossRef]
- Isensee, F. NnU-Net. Available online: https://github.com/MIC-DKFZ/nnUNet (accessed on 18 October 2022).
- Ibrahim, M.M. Subcutaneous and Visceral Adipose Tissue: Structural and Functional Differences. Obes. Rev. 2010, 11, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Nattenmüller, J.; Wochner, R.; Muley, T.; Steins, M.; Hummler, S.; Teucher, B.; Wiskemann, J.; Kauczor, H.-U.; Wielpütz, M.O.; Heussel, C.P. Prognostic Impact of CT-Quantified Muscle and Fat Distribution before and after First-Line-Chemotherapy in Lung Cancer Patients. PLoS ONE 2017, 12, e0169136. [Google Scholar] [CrossRef] [PubMed]
- Troschel, F.M.; Jin, Q.; Eichhorn, F.; Muley, T.; Best, T.D.; Leppelmann, K.S.; Yang, C.-F.J.; Troschel, A.S.; Winter, H.; Heußel, C.P.; et al. Sarcopenia on Preoperative Chest Computed Tomography Predicts Cancer-Specific and All-Cause Mortality Following Pneumonectomy for Lung Cancer: A Multicenter Analysis. Cancer Med. 2021, 10, 6677–6686. [Google Scholar] [CrossRef] [PubMed]
- Kullberg, J.; Hedström, A.; Brandberg, J.; Strand, R.; Johansson, L.; Bergström, G.; Ahlström, H. Automated Analysis of Liver Fat, Muscle and Adipose Tissue Distribution from CT Suitable for Large-Scale Studies. Sci. Rep. 2017, 7, 10425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.J.; Liu, J.; Yao, J.; Kanarek, A.; Summers, R.M.; Pickhardt, P.J. Fully Automated Segmentation and Quantification of Visceral and Subcutaneous Fat at Abdominal CT: Application to a Longitudinal Adult Screening Cohort. Br. J. Radiol. 2018, 91, 20170968. [Google Scholar] [CrossRef] [PubMed]
- Nowak, S.; Faron, A.; Luetkens, J.A.; Geißler, H.L.; Praktiknjo, M.; Block, W.; Thomas, D.; Sprinkart, A.M. Fully Automated Segmentation of Connective Tissue Compartments for CT-Based Body Composition Analysis: A Deep Learning Approach. Investig. Radiol. 2020, 55, 357–366. [Google Scholar] [CrossRef]
- Fu, Y.; Ippolito, J.E.; Ludwig, D.R.; Nizamuddin, R.; Li, H.H.; Yang, D. Technical Note: Automatic Segmentation of CT Images for Ventral Body Composition Analysis. Med. Phys. 2020, 47, 5723–5730. [Google Scholar] [CrossRef]
- Irlbeck, T.; Massaro, J.M.; Bamberg, F.; O’Donnell, C.J.; Hoffmann, U.; Fox, C.S. Association between Single-Slice Measurements of Visceral and Abdominal Subcutaneous Adipose Tissue with Volumetric Measurements: The Framingham Heart Study. Int. J. Obes. 2005 2010, 34, 781–787. [Google Scholar] [CrossRef] [Green Version]
- Graffy, P.M.; Sandfort, V.; Summers, R.M.; Pickhardt, P.J. Automated Liver Fat Quantification at Nonenhanced Abdominal CT for Population-Based Steatosis Assessment. Radiology 2019, 293, 334–342. [Google Scholar] [CrossRef]
- Sarwar, A.; Shaw, L.J.; Shapiro, M.D.; Blankstein, R.; Hoffmann, U.; Hoffman, U.; Cury, R.C.; Abbara, S.; Brady, T.J.; Budoff, M.J.; et al. Diagnostic and Prognostic Value of Absence of Coronary Artery Calcification. JACC Cardiovasc. Imaging 2009, 2, 675–688. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, U.; Massaro, J.M.; D’Agostino, R.B.; Kathiresan, S.; Fox, C.S.; O’Donnell, C.J. Cardiovascular Event Prediction and Risk Reclassification by Coronary, Aortic, and Valvular Calcification in the Framingham Heart Study. J. Am. Heart Assoc. 2016, 5, e003144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Criqui, M.H.; Denenberg, J.O.; McClelland, R.L.; Allison, M.A.; Ix, J.H.; Guerci, A.; Cohoon, K.P.; Srikanthan, P.; Watson, K.E.; Wong, N.D. Abdominal Aortic Calcium, Coronary Artery Calcium, and Cardiovascular Morbidity and Mortality in the Multi-Ethnic Study of Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1574–1579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brady, A.R.; Thompson, S.G.; Fowkes, F.G.R.; Greenhalgh, R.M.; Powell, J.T. UK Small Aneurysm Trial Participants Abdominal Aortic Aneurysm Expansion: Risk Factors and Time Intervals for Surveillance. Circulation 2004, 110, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Detrano, R.; Guerci, A.D.; Carr, J.J.; Bild, D.E.; Burke, G.; Folsom, A.R.; Liu, K.; Shea, S.; Szklo, M.; Bluemke, D.A.; et al. Coronary Calcium as a Predictor of Coronary Events in Four Racial or Ethnic Groups. N. Engl. J. Med. 2008, 358, 1336–1345. [Google Scholar] [CrossRef] [Green Version]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M.; Detrano, R. Quantification of Coronary Artery Calcium Using Ultrafast Computed Tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Wolterink, J.M.; Leiner, T.; Takx, R.A.P.; Viergever, M.A.; Isgum, I. Automatic Coronary Calcium Scoring in Non-Contrast-Enhanced ECG-Triggered Cardiac CT with Ambiguity Detection. IEEE Trans. Med. Imaging 2015, 34, 1867–1878. [Google Scholar] [CrossRef] [PubMed]
- Growing a Random Forest with Fuzzy Spatial Features for Fully Automatic Artery-Specific Coronary Calcium Scoring | SpringerLink. Available online: https://link.springer.com/chapter/10.1007/978-3-319-67389-9_4 (accessed on 18 October 2022).
- Zeleznik, R.; Foldyna, B.; Eslami, P.; Weiss, J.; Alexander, I.; Taron, J.; Parmar, C.; Alvi, R.M.; Banerji, D.; Uno, M.; et al. Deep Convolutional Neural Networks to Predict Cardiovascular Risk from Computed Tomography. Nat. Commun. 2021, 12, 715. [Google Scholar] [CrossRef] [PubMed]
- Eng, D.; Chute, C.; Khandwala, N.; Rajpurkar, P.; Long, J.; Shleifer, S.; Khalaf, M.H.; Sandhu, A.T.; Rodriguez, F.; Maron, D.J.; et al. Automated Coronary Calcium Scoring Using Deep Learning with Multicenter External Validation. NPJ Digit. Med. 2021, 4, 88. [Google Scholar] [CrossRef] [PubMed]
- Galbán, C.J.; Han, M.K.; Boes, J.L.; Chughtai, K.A.; Meyer, C.R.; Johnson, T.D.; Galbán, S.; Rehemtulla, A.; Kazerooni, E.A.; Martinez, F.J.; et al. Computed Tomography-Based Biomarker Provides Unique Signature for Diagnosis of COPD Phenotypes and Disease Progression. Nat. Med. 2012, 18, 1711–1715. [Google Scholar] [CrossRef]
- Weinheimer, O.; Wielpütz, M.O.; Konietzke, P.; Heussel, C.P.; Kauczor, H.-U.; Brochhausen, C.; Hollemann, D.; Savage, D.; Galbán, C.J.; Robinson, T.E. Fully Automated Lobe-Based Airway Taper Index Calculation in a Low Dose MDCT CF Study over 4 Time-Points; Styner, M.A., Angelini, E.D., Eds.; spie digital library: Orlando, FL, USA; p. 101330U.
- Wielpütz, M.O.; Eichinger, M.; Weinheimer, O.; Ley, S.; Mall, M.A.; Wiebel, M.; Bischoff, A.; Kauczor, H.-U.; Heußel, C.P.; Puderbach, M. Automatic Airway Analysis on Multidetector Computed Tomography in Cystic Fibrosis: Correlation with Pulmonary Function Testing. J. Thorac. Imaging 2013, 28, 104–113. [Google Scholar] [CrossRef] [Green Version]
- Wielpütz, M.O.; Weinheimer, O.; Eichinger, M.; Wiebel, M.; Biederer, J.; Kauczor, H.-U.; Heußel, C.P.; Mall, M.A.; Puderbach, M. Pulmonary Emphysema in Cystic Fibrosis Detected by Densitometry on Chest Multidetector Computed Tomography. PLoS ONE 2013, 8, e73142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Jiang, B.; Zhang, L.; Greuter, M.J.W.; de Bock, G.H.; Zhang, H.; Xie, X. Lung Nodule Detectability of Artificial Intelligence-Assisted CT Image Reading in Lung Cancer Screening. Curr. Med. Imaging 2022, 18, 327–334. [Google Scholar] [CrossRef]
- Baumgartner, M.; Jäger, P.F.; Isensee, F.; Maier-Hein, K.H. NnDetection: A Self-Configuring Method for Medical Object Detection. In Medical Image Computing and Computer Assisted Intervention—MICCAI 2021; de Bruijne, M., Cattin, P.C., Cotin, S., Padoy, N., Speidel, S., Zheng, Y., Essert, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 530–539. [Google Scholar]
- Baumgartner, M. What Is NnDetection? Available online: https://github.com/MIC-DKFZ/nnDetection (accessed on 18 October 2022).
- Cao, H.; Liu, H.; Song, E.; Ma, G.; Xu, X.; Jin, R.; Liu, T.; Hung, C.-C. A Two-Stage Convolutional Neural Networks for Lung Nodule Detection. IEEE J. Biomed. Health Inform. 2020, 24, 2006–2015. [Google Scholar] [CrossRef]
- Liu, J.; Cao, L.; Akin, O.; Tian, Y. 3DFPN-HS$$^2$$: 3D Feature Pyramid Network Based High Sensitivity and Specificity Pulmonary Nodule Detection. In Medical Image Computing and Computer Assisted Intervention—MICCAI 2019; Shen, D., Liu, T., Peters, T.M., Staib, L.H., Essert, C., Zhou, S., Yap, P.-T., Khan, A., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 513–521. [Google Scholar]
- S4ND: Single-Shot Single-Scale Lung Nodule Detection | SpringerLink. Available online: https://link.springer.com/chapter/10.1007/978-3-030-00934-2_88 (accessed on 18 October 2022).
- Towards Accurate Pulmonary Nodule Detection by Representing Nodules as Points with High-Resolution Network | IEEE Journals & Magazine | IEEE Xplore. Available online: https://ieeexplore.ieee.org/document/9174981/ (accessed on 18 October 2022).
- Armato, S.G.; McLennan, G.; Bidaut, L.; McNitt-Gray, M.F.; Meyer, C.R.; Reeves, A.P.; Zhao, B.; Aberle, D.R.; Henschke, C.I.; Hoffman, E.A.; et al. The Lung Image Database Consortium (LIDC) and Image Database Resource Initiative (IDRI): A Completed Reference Database of Lung Nodules on CT Scans. Med. Phys. 2011, 38, 915–931. [Google Scholar] [CrossRef] [Green Version]
- Schreuder, A.; Scholten, E.T.; van Ginneken, B.; Jacobs, C. Artificial Intelligence for Detection and Characterization of Pulmonary Nodules in Lung Cancer CT Screening: Ready for Practice? Transl. Lung Cancer Res. 2021, 10, 2378–2388. [Google Scholar] [CrossRef]
- Ciompi, F.; Chung, K.; van Riel, S.J.; Setio, A.A.A.; Gerke, P.K.; Jacobs, C.; Scholten, E.T.; Schaefer-Prokop, C.; Wille, M.M.W.; Marchianò, A.; et al. Towards Automatic Pulmonary Nodule Management in Lung Cancer Screening with Deep Learning. Sci. Rep. 2017, 7, 46479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekuboyina, A.; Kukačka, J.; Kirschke, J.S.; Menze, B.H.; Valentinitsch, A. Attention-Driven Deep Learning for Pathological Spine Segmentation. In Computational Methods and Clinical Applications in Musculoskeletal Imaging; Glocker, B., Yao, J., Vrtovec, T., Frangi, A., Zheng, G., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 108–119. [Google Scholar]
- Janssens, R.; Zeng, G.; Zheng, G. Fully Automatic Segmentation of Lumbar Vertebrae from CT Images Using Cascaded 3D Fully Convolutional Networks. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; pp. 893–897. [Google Scholar]
- Lessmann, N.; van Ginneken, B.; Išgum, I. Iterative Convolutional Neural Networks for Automatic Vertebra Identification and Segmentation in CT Images. In the Medical Imaging 2018: Image Processing; SPIE: Bellingham WC, USA, 2018; Volume 10574, pp. 39–44. [Google Scholar]
- Payer, C.; Štern, D.; Bischof, H.; Urschler, M. Coarse to Fine Vertebrae Localization and Segmentation with SpatialConfiguration-Net and U-Net. In Proceedings of the 15th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications, Valletta, Malta, 27–29 February; SCITEPRESS—Science and Technology Publications: Valletta, Malta, 2020; pp. 124–133. [Google Scholar]
- Sekuboyina, A.; Husseini, M.E.; Bayat, A.; Löffler, M.; Liebl, H.; Li, H.; Tetteh, G.; Kukačka, J.; Payer, C.; Štern, D.; et al. VerSe: A Vertebrae Labelling and Segmentation Benchmark for Multi-Detector CT Images. Med. Image Anal. 2021, 73, 102166. [Google Scholar] [CrossRef] [PubMed]
- Scherer, J.; Nolden, M.; Kleesiek, J.; Metzger, J.; Kades, K.; Schneider, V.; Bach, M.; Sedlaczek, O.; Bucher, A.M.; Vogl, T.J.; et al. Joint Imaging Platform for Federated Clinical Data Analytics. JCO Clin. Cancer Inform. 2020, 4, 1027–1038. [Google Scholar] [CrossRef]
- Schlamp, K. GitHub—Radexperts/Adit: ADIT (Automated DICOM Transfer). Available online: https://github.com/radexperts/adit (accessed on 24 August 2022).
- Pickhardt, P.J.; Graffy, P.M.; Reeder, S.B.; Hernando, D.; Li, K. Quantification of Liver Fat Content with Unenhanced MDCT: Phantom and Clinical Correlation With MRI Proton Density Fat Fraction. AJR Am. J. Roentgenol. 2018, 211, W151–W157. [Google Scholar] [CrossRef]
- O’Connor, S.D.; Graffy, P.M.; Zea, R.; Pickhardt, P.J. Does Nonenhanced CT-Based Quantification of Abdominal Aortic Calcification Outperform the Framingham Risk Score in Predicting Cardiovascular Events in Asymptomatic Adults? Radiology 2019, 290, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Han, D.; Kuronuma, K.; Rozanski, A.; Budoff, M.J.; Miedema, M.D.; Nasir, K.; Shaw, L.J.; Rumberger, J.A.; Gransar, H.; Blumenthal, R.S.; et al. Implication of Thoracic Aortic Calcification over Coronary Calcium Score Regarding the 2018 ACC/AHA Multisociety Cholesterol Guideline: Results from the CAC Consortium. Am. J. Prev. Cardiol. 2021, 8, 100232. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 73, e285–e350. [Google Scholar] [CrossRef]
- Rumberger, J.A. Coronary Artery Calcium Scanning Using Computed Tomography: Clinical Recommendations for Cardiac Risk Assessment and Treatment. Semin. Ultrasound. CT MR 2008, 29, 223–229. [Google Scholar] [CrossRef]
- Grydeland, T.B.; Dirksen, A.; Coxson, H.O.; Pillai, S.G.; Sharma, S.; Eide, G.E.; Gulsvik, A.; Bakke, P.S. Quantitative Computed Tomography: Emphysema and Airway Wall Thickness by Sex, Age and Smoking. Eur. Respir. J. 2009, 34, 858–865. [Google Scholar] [CrossRef] [Green Version]
- Heussel, C.P.; Herth, F.J.F.; Kappes, J.; Hantusch, R.; Hartlieb, S.; Weinheimer, O.; Kauczor, H.U.; Eberhardt, R. Fully Automatic Quantitative Assessment of Emphysema in Computed Tomography: Comparison with Pulmonary Function Testing and Normal Values. Eur. Radiol. 2009, 19, 2391–2402. [Google Scholar] [CrossRef]
- Do, T.D.; Skornitzke, S.; Merle, U.; Kittel, M.; Hofbaur, S.; Melzig, C.; Kauczor, H.-U.; Wielpütz, M.O.; Weinheimer, O. COVID-19 Pneumonia: Prediction of Patient Outcome by CT-Based Quantitative Lung Parenchyma Analysis Combined with Laboratory Parameters. PLoS ONE 2022, 17, e0271787. [Google Scholar] [CrossRef]
- McKee, B.J.; Regis, S.M.; McKee, A.B.; Flacke, S.; Wald, C. Performance of ACR Lung-RADS in a Clinical CT Lung Screening Program. J. Am. Coll. Radiol. JACR 2015, 12, 273–276. [Google Scholar] [CrossRef]
- van Hamersvelt, R.W.; Schilham, A.M.R.; Engelke, K.; den Harder, A.M.; de Keizer, B.; Verhaar, H.J.; Leiner, T.; de Jong, P.A.; Willemink, M.J. Accuracy of Bone Mineral Density Quantification Using Dual-Layer Spectral Detector CT: A Phantom Study. Eur. Radiol. 2017, 27, 4351–4359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Li, X.; Li, J.; Jiao, X.; Jia, X.; Zhang, X.; Fan, G.; Yang, J.; Guo, J. The Accuracy of Bone Mineral Density Measurement Using Dual-Energy Spectral CT and Quantitative CT: A Comparative Phantom Study. Clin. Radiol. 2020, 75, 320.e9–320.e15. [Google Scholar] [CrossRef] [PubMed]
- Kalender, W.A.; Suess, C. A New Calibration Phantom for Quantitative Computed Tomography. Med. Phys. 1987, 14, 863–866. [Google Scholar] [CrossRef]
- Hendrickson, N.R.; Pickhardt, P.J.; Del Rio, A.M.; Rosas, H.G.; Anderson, P.A. Bone Mineral Density T-Scores Derived from CT Attenuation Numbers (Hounsfield Units): Clinical Utility and Correlation with Dual-Energy X-Ray Absorptiometry. Iowa Orthop. J. 2018, 38, 25–31. [Google Scholar]
- Nasir, K.; Cainzos-Achirica, M. Role of Coronary Artery Calcium Score in the Primary Prevention of Cardiovascular Disease. BMJ 2021, 373, n776. [Google Scholar] [CrossRef]
- Chen, Z.; Qureshi, A.R.; Ripsweden, J.; Wennberg, L.; Heimburger, O.; Lindholm, B.; Barany, P.; Haarhaus, M.; Brismar, T.B.; Stenvinkel, P. Vertebral Bone Density Associates with Coronary Artery Calcification and Is an Independent Predictor of Poor Outcome in End-Stage Renal Disease Patients. Bone 2016, 92, 50–57. [Google Scholar] [CrossRef]
- Chuang, T.-L.; Chuang, M.-H.; Koo, M.; Lin, C.-H.; Wang, Y.-F. Association of Bone Mineral Density and Trabecular Bone Score with Cardiovascular Disease. Tzu-Chi Med. J. 2020, 32, 234–239. [Google Scholar] [CrossRef]
- Ahmadi, N.; Mao, S.S.; Hajsadeghi, F.; Arnold, B.; Kiramijyan, S.; Gao, Y.; Flores, F.; Azen, S.; Budoff, M. The Relation of Low Levels of Bone Mineral Density with Coronary Artery Calcium and Mortality. Osteoporos. Int. 2018, 29, 1609–1616. [Google Scholar] [CrossRef]
- Teng, Z.; Zhu, Y.; Teng, Y.; Long, Q.; Hao, Q.; Yu, X.; Yang, L.; Lv, Y.; Liu, J.; Zeng, Y.; et al. The Analysis of Osteosarcopenia as a Risk Factor for Fractures, Mortality, and Falls. Osteoporos. Int. 2021, 32, 2173–2183. [Google Scholar] [CrossRef]
- Salech, F.; Marquez, C.; Lera, L.; Angel, B.; Saguez, R.; Albala, C. Osteosarcopenia Predicts Falls, Fractures, and Mortality in Chilean Community-Dwelling Older Adults. J. Am. Med. Dir. Assoc. 2021, 22, 853–858. [Google Scholar] [CrossRef]
- Inoue, T.; Maeda, K.; Nagano, A.; Shimizu, A.; Ueshima, J.; Murotani, K.; Sato, K.; Hotta, K.; Morishita, S.; Tsubaki, A. Related Factors and Clinical Outcomes of Osteosarcopenia: A Narrative Review. Nutrients 2021, 13, 291. [Google Scholar] [CrossRef] [PubMed]
- Kahnert, K.; Jörres, R.A.; Kauczor, H.-U.; Biederer, J.; Jobst, B.; Alter, P.; Biertz, F.; Mertsch, P.; Lucke, T.; Lutter, J.I.; et al. Relationship between Clinical and Radiological Signs of Bronchiectasis in COPD Patients: Results from COSYCONET. Respir. Med. 2020, 172, 106117. [Google Scholar] [CrossRef] [PubMed]
- Karch, A.; Vogelmeier, C.; Welte, T.; Bals, R.; Kauczor, H.-U.; Biederer, J.; Heinrich, J.; Schulz, H.; Gläser, S.; Holle, R.; et al. The German COPD Cohort COSYCONET: Aims, Methods and Descriptive Analysis of the Study Population at Baseline. Respir. Med. 2016, 114, 27–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, N.; Motsch, E.; Trotter, A.; Heussel, C.P.; Dienemann, H.; Schnabel, P.A.; Kauczor, H.-U.; Maldonado, S.G.; Miller, A.B.; Kaaks, R.; et al. Lung Cancer Mortality Reduction by LDCT Screening-Results from the Randomized German LUSI Trial. Int. J. Cancer 2020, 146, 1503–1513. [Google Scholar] [CrossRef] [PubMed]
- González Maldonado, S.; Hynes, L.C.; Motsch, E.; Heussel, C.-P.; Kauczor, H.-U.; Robbins, H.A.; Delorme, S.; Kaaks, R. Validation of Multivariable Lung Cancer Risk Prediction Models for the Personalized Assignment of Optimal Screening Frequency: A Retrospective Analysis of Data from the German Lung Cancer Screening Intervention Trial (LUSI). Transl. Lung Cancer Res. 2021, 10, 1305–1317. [Google Scholar] [CrossRef] [PubMed]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chassagnon, G.; Vakalopoulou, M.; Paragios, N.; Revel, M.-P. Artificial Intelligence Applications for Thoracic Imaging. Eur. J. Radiol. 2020, 123, 108774. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Summers, R.M. Clinical Artificial Intelligence Applications in Radiology: Chest and Abdomen. Radiol. Clin. N. Am. 2021, 59, 987–1002. [Google Scholar] [CrossRef]
- Hwang, E.J.; Park, C.M. Clinical Implementation of Deep Learning in Thoracic Radiology: Potential Applications and Challenges. Korean J. Radiol. 2020, 21, 511–525. [Google Scholar] [CrossRef] [Green Version]
- Fischer, A.M.; Yacoub, B.; Savage, R.H.; Martinez, J.D.; Wichmann, J.L.; Sahbaee, P.; Grbic, S.; Varga-Szemes, A.; Schoepf, U.J. Machine Learning/Deep Neuronal Network: Routine Application in Chest Computed Tomography and Workflow Considerations. J. Thorac. Imaging 2020, 35 (Supply 1), S21–S27. [Google Scholar] [CrossRef]
- AI-Rad Companion. Available online: https://www.siemens-healthineers.com/digital-health-solutions/digital-solutions-overview/clinical-decision-support/ai-rad-companion (accessed on 23 August 2022).
- Pickhardt, P.J.; Graffy, P.M.; Perez, A.A.; Lubner, M.G.; Elton, D.C.; Summers, R.M. Opportunistic Screening at Abdominal CT: Use of Automated Body Composition Biomarkers for Added Cardiometabolic Value. RadioGraphics 2021, 41, 524–542. [Google Scholar] [CrossRef] [PubMed]
- Telenga, E.D.; Oudkerk, M.; van Ooijen, P.M.; Vliegenthart, R.; Ten Hacken, N.H.; Postma, D.S.; van den Berge, M. Airway wall thickness on HRCT scans decreases with age and increases with smoking. BMC Pulm Med. 2017, 17, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, D.; Klein, E.; Friedman, J.; Gransar, H.; Achenbach, S.; Al-Mallah, M.H.; Budoff, M.J.; Cademartiri, F.; Maffei, E.; Callister, T.Q.; et al. Prognostic significance of subtle coronary calcification in patients with zero coronary artery calcium score: From the CONFIRM registry. Atherosclerosis 2020, 309, 33–38. [Google Scholar] [CrossRef] [PubMed]



| Comorbidity | Results | Conclusion |
|---|---|---|
| Adipose tissue and metabolism |
|
|
| Pulmonary nodules |
|
|
| Pulmonal parenchyma abnormalities (COPD) |
|
|
| Cardiovascular comorbidities |
|
|
| Osteoporosis |
|
|
| Comorbidity | Results | Conclusion |
|---|---|---|
| Adipose tissue and metabolism |
|
|
| Pulmonary nodules |
| |
| Pulmonal parenchyma abnormalities (COPD) |
|
|
| Cardiovascular comorbidities |
|
|
| Osteoporosis |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palm, V.; Norajitra, T.; von Stackelberg, O.; Heussel, C.P.; Skornitzke, S.; Weinheimer, O.; Kopytova, T.; Klein, A.; Almeida, S.D.; Baumgartner, M.; et al. AI-Supported Comprehensive Detection and Quantification of Biomarkers of Subclinical Widespread Diseases at Chest CT for Preventive Medicine. Healthcare 2022, 10, 2166. https://doi.org/10.3390/healthcare10112166
Palm V, Norajitra T, von Stackelberg O, Heussel CP, Skornitzke S, Weinheimer O, Kopytova T, Klein A, Almeida SD, Baumgartner M, et al. AI-Supported Comprehensive Detection and Quantification of Biomarkers of Subclinical Widespread Diseases at Chest CT for Preventive Medicine. Healthcare. 2022; 10(11):2166. https://doi.org/10.3390/healthcare10112166
Chicago/Turabian StylePalm, Viktoria, Tobias Norajitra, Oyunbileg von Stackelberg, Claus P. Heussel, Stephan Skornitzke, Oliver Weinheimer, Taisiya Kopytova, Andre Klein, Silvia D. Almeida, Michael Baumgartner, and et al. 2022. "AI-Supported Comprehensive Detection and Quantification of Biomarkers of Subclinical Widespread Diseases at Chest CT for Preventive Medicine" Healthcare 10, no. 11: 2166. https://doi.org/10.3390/healthcare10112166