

Impact of Daycare Service Interruption during COVID-19 Pandemic on Physical and Mental Functions and Nutrition in Older People with Dementia

Abstract
:1. Background
2. Methods
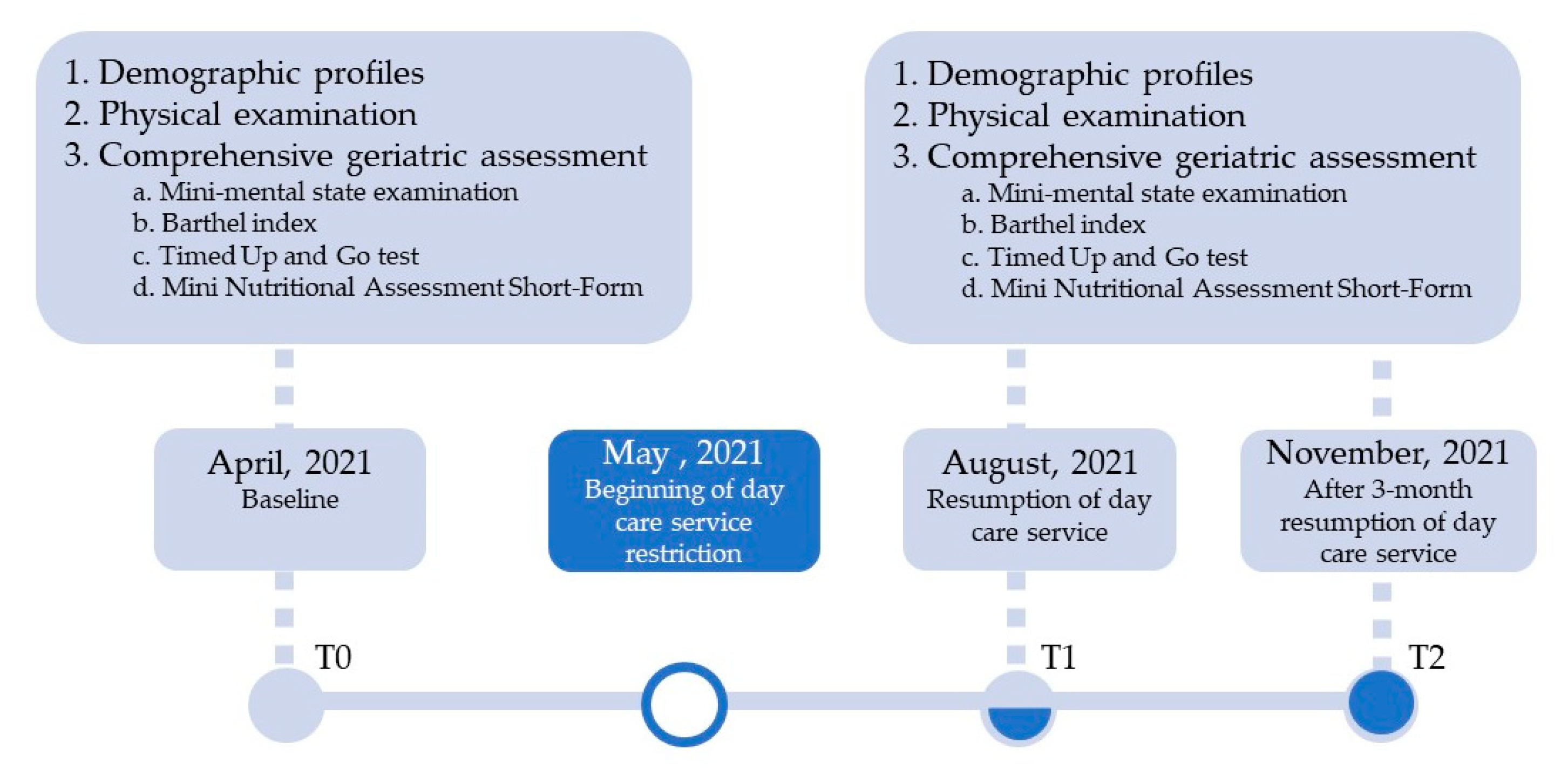
2.1. Study Design
2.2. Recruitment
2.3. Setting
2.4. Measures
2.5. Statistical Analysis
3. Results
3.1. Description of the Study Participants
3.2. Differences in Physical and Cognitive Functions, and Nutritional Status at Baseline, during Restriction and after Resumption of Daycare Services in the COVID-19 Outbreak
3.3. Relevant Factors of Physical and Cognitive Function after Restriction and Resumption of Daycare Services
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guerchet, M.; Prince, M.; Prina, M. Numbers of People with Dementia Worldwide: An Update to the Estimates in the World Alzheimer Report 2015; Alzheimer Disease International: New York, NY, USA, 2020. [Google Scholar]
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.-T.; Prina, M. World Alzheimer Report 2015—The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer Disease International: New York, NY, USA, 2015. [Google Scholar]
- Whatley, M.C.; Siegel, A.L.M.; Schwartz, S.T.; Silaj, K.M.; Castel, A.D. Younger and Older Adults’ Mood and Expectations Regarding Aging During COVID-19. Gerontol. Geriatr. Med. 2020, 6, 259. [Google Scholar] [CrossRef] [PubMed]
- Prynn, J.E.; Kuper, H. Perspectives on Disability and Non-Communicable Diseases in Low- and Middle-Income Countries, with a Focus on Stroke and Dementia. Int. J. Environ. Res. Public Heal. 2019, 16, 3488. [Google Scholar] [CrossRef] [PubMed]
- Avan, A.; Hachinski, V. Stroke and dementia, leading causes of neurological disability and death, potential for prevention. Alzheimer’s Dement. 2021, 17, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; Ismail, Z.; Livingston, G. One third of dementia cases can be prevented within the next 25 years by tackling risk factors. The case “for” and “against”. Alzheimer’s Res. Ther. 2020, 12, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, Y.-H.; Kuo, T.A.; Tai, C.-J.; Lee, S.-S.; Lee, M.-C. Integrated care for dementia in Taiwan: Policy, system and services. J. Hum. Behav. Soc. Env. 2019, 12, S73–S77. [Google Scholar]
- Tsai, C.; Huang, M.; Cheng, C.; Lee, J.; Wang, W.; Huang, L.; Huang, L.; Lee, W.; Sung, P.; Liu, Y.; et al. Determinants of long-term care service use by persons with dementia: A national dementia registry study conducted in Taiwan. Int. J. Geriatr. Psychiatry 2022, 37, 5719. [Google Scholar] [CrossRef]
- Lin, C.-F.; Wu, J.-J.; Huang, Y.-H.; Ju, L.-Y.; Lin, S.-Y.; Chou, Y.-C.; Lin, C.-S. Impact of day care services on physical and cognitive functions in old people with dementia in a medical center in central Taiwan. Heal. Qual. Life Outcomes 2021, 19, 1–8. [Google Scholar] [CrossRef]
- Hsu, H.-C.; Chen, C.-F. LTC 2.0: The 2017 reform of home- and community-based long-term care in Taiwan. Heal. Policy 2019, 123, 912–916. [Google Scholar] [CrossRef]
- Chen, C.-F.; Fu, T.-H. Policies and Transformation of Taiwan’s Long-Term Care System. Ann. Geriatr. Med. Res. 2020, 24, 187–194. [Google Scholar] [CrossRef]
- Ma, J.M.; Moriarty, J. Examining day centre provision for older people in the UK using the Equality Act 2010: Findings of a scoping review. Heal. Soc. Care Community 2013, 22, 352–360. [Google Scholar] [CrossRef]
- Ellen, M.E.; DeMaio, B.P.; Lange, A.; Wilson, M.G. Adult Day Center Programs and Their Associated Outcomes on Clients, Caregivers, and the Health System: A Scoping Review. Gerontologist 2017, 57, e85–e94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mossello, E.; Caleri, V.; Razzi, E.; Di Bari, M.; Cantini, C.; Tonon, E.; Lopilato, E.; Marini, M.; Simoni, D.; Cavallini, M.C.; et al. Day Care for older dementia patients: Favorable effects on behavioral and psychological symptoms and caregiver stress. Int. J. Geriatr. Psychiatry 2008, 23, 1066–1072. [Google Scholar] [CrossRef] [PubMed]
- Kukreti, S.; Lu, M.-Y.; Lin, Y.-H.; Strong, C.; Lin, C.-Y.; Ko, N.-Y.; Chen, P.-L.; Ko, W.-C. Willingness of Taiwan’s Healthcare Workers and Outpatients to Vaccinate against COVID-19 during a Period without Community Outbreaks. Vaccines 2021, 9, 246. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.-Y.; Pakpour, A.H. The Association Between Health Status and Insomnia, Mental Health, and Preventive Behaviors: The Mediating Role of Fear of COVID-19. Gerontol. Geriatr. Med. 2020, 6, 6081. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.-W.; Cheng, Y. Policy actions to alleviate psychosocial impacts of COVID-19 pandemic: Experiences from Taiwan. Soc. Heal. Behav. 2020, 3, 72. [Google Scholar] [CrossRef]
- Okely, J.A.; Corley, J.; Welstead, M.; Taylor, A.M.; Page, D.; Skarabela, B.; Redmond, P.; Cox, S.R.; Russ, T.C. Change in Physical Activity, Sleep Quality, and Psychosocial Variables during COVID-19 Lockdown: Evidence from the Lothian Birth Cohort 1936. Int. J. Environ. Res. Public Heal. 2020, 18, 210. [Google Scholar] [CrossRef]
- Webb, L. COVID-19 lockdown: A perfect storm for older people’s mental health. J. Psychiatr. Ment. Health Nurs. 2021, 28, 300. [Google Scholar] [CrossRef]
- Covassin, N.; Singh, P. Sleep Duration and Cardiovascular Disease Risk: Epidemiologic and Experimental Evidence Sleep Med. Clin. 2016, 11, 81–89. [Google Scholar] [CrossRef]
- Thorp, A.A.; Owen, N.; Neuhaus, M.; Dunstan, D.W. Sedentary Behaviors and Subsequent Health Outcomes in Adults: A Systematic Review of Longitudinal Studies, 1996–2011. Am. J. Prev. Med. 2011, 41, 207–215. [Google Scholar] [CrossRef]
- Steptoe, A.; Deaton, A.; Stone, A.A. Subjective wellbeing, health, and ageing. Lancet 2014, 385, 640–648. [Google Scholar] [CrossRef]
- Bu, F.; Steptoe, A.; Fancourt, D. Loneliness during a strict lockdown: Trajectories and predictors during the COVID-19 pandemic in 38,217 United Kingdom adults. Soc. Sci. Med. 2020, 265, 113521. [Google Scholar] [CrossRef] [PubMed]
- Tsai, F.-J.; Yang, H.-W.; Lin, C.-P.; Liu, J.Z. Acceptability of COVID-19 Vaccines and Protective Behavior among Adults in Taiwan: Associations between Risk Perception and Willingness to Vaccinate against COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 5579. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.S.; Chong, M.S.; Sahadevan, S. Utility of the Clinical Dementia Rating in Asian Populations. Clin. Med. Res. 2007, 5, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.-B.; Yiao, S.-Y.; Sun, Y.; Lee, H.-J.; Yang, S.-C.; Chiu, M.-J.; Chen, T.-F.; Lin, K.-N.; Tang, L.-Y.; Lin, C.-C.; et al. Comorbidity and dementia: A nationwide survey in Taiwan. PLoS ONE 2017, 12, e0175475. [Google Scholar] [CrossRef]
- Chen, C.C.-H.; Wang, C.; Huang, G.-H. Functional trajectory 6 months posthospitalization: A cohort study of older hospital-ized patients in Taiwan. Nurs. Res. 2008, 57, 93–100. [Google Scholar] [CrossRef]
- Hoyl, M.T.; Alessi, C.A.; Harker, J.O.; Josephson, K.R.; Pietruszka, F.M.; Koelfgen, M.; Mervis, J.R.; Fitten, L.J.; Rubenstein, L. Development and Testing of a Five-Item Version of the Geriatric Depression Scale. J. Am. Geriatr. Soc. 1999, 47, 873–878. [Google Scholar] [CrossRef]
- Chin, W.-C.; Liu, C.-Y.; Lee, C.-P.; Chu, C.-L. Validation of five short versions of the Geriatric Depression Scale in the elder population in Taiwan. Taiwan J. Psychiatr. 2014, 28, 156–163. [Google Scholar]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Lin, C.-F.; Huang, Y.-H.; Ju, L.-Y.; Weng, S.-C.; Lee, Y.-S.; Chou, Y.-Y.; Lin, C.-S.; Lin, S.-Y. Health-Related Quality of Life Measured by EQ-5D in Relation to Hospital Stay and Readmission in Elderly Patients Hospitalized for Acute Illness. Int. J. Environ. Res. Public Heal. 2020, 17, 5333. [Google Scholar] [CrossRef]
- Chen, Y.J.; Dai, Y.T.; Yang, C.T.; Wang, T.J.; Teng, Y.H. A Review and Proposal on Patient Classification in Long-Term Care System; Department of Health for Republic of China: Taipei, Taiwan, 1995.
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional Reach: A New Clinical Measure of Balance. J. Gerontol. 1990, 45, M192–M197. [Google Scholar] [CrossRef] [PubMed]
- Weiner, D.K.; Duncan, P.; Chandler, J.; Studenski, S.A. Functional Reach: A Marker of Physical Frailty. J. Am. Geriatr. Soc. 1992, 40, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Wellmon, R. Gait Assessment and Training. In Physical Rehabilitation; Elsevier: Amsterdam, The Netherlands, 2010; ISBN 978-1-4557-3671-3. [Google Scholar]
- Phillips, M.B.; Foley, A.L.; Barnard, R.; Isenring, E.A.; Miller, M.D. Nutritional Screening in Community-Dwelling Older Adults: A Systematic Literature Review. Asia Pac. J. Clin. Nutr. 2010, 19, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.-J.; Tarn, Y.-H.; Hsieh, C.-L.; Liou, W.-S.; Shaw, J.W.; Chiou, X.G. Taiwanese Version of the EQ-5D: Validation in a Representative Sample of the Taiwanese Population. J. Formos. Med Assoc. 2007, 106, 1023–1031. [Google Scholar] [CrossRef]
- Hai, S.; Gao, Q.; Gwee, X.; Chua, D.Q.L.; Yap, K.B.; Ng, T.P. Malnutrition Risk, Physical Function Decline and Disability in Middle-Aged and Older Adults Followed Up in the Singapore Longitudinal Ageing Study. Clin. Interv. Aging 2021, 16, 1527–1539. [Google Scholar] [CrossRef]
- Pigłowska, M.; Guligowska, A.; Kostka, T. Nutritional Status Plays More Important Role in Determining Functional State in Older People Living in the Community than in Nursing Home Residents. Nutrients 2020, 12, 2042. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Rämsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.S.; Charlton, K.E.; Maggio, M.; et al. Frequency of Malnutrition in Older Adults: A Multinational Perspective Using the Mini Nutritional Assessment. J. Am. Geriatr. Soc. 2010, 58, 1734–1738. [Google Scholar] [CrossRef]
- Teramura, A.; Kimura, Y.; Hamada, K.; Ishimoto, Y.; Kawamori, M. COVID-19-Related Lifestyle Changes among Communi-ty-Dwelling Older Adult Day-Care Users: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 256. [Google Scholar] [CrossRef]
- Amagasa, S.; Kojin, H.; Inoue, S. Long-term care and the coronavirus disease 2019 challenge in Japan. J. Gen. Fam. Med. 2020, 21, 292–293. [Google Scholar] [CrossRef]
- Kato, M.; Ono, S.; Seko, H.; Tsukamoto, T.; Kurita, Y.; Kubo, A.; Omote, T.; Omote, S. Trajectories of frailty, physical function, and physical activity levels in elderly patients with heart failure: Impacts of interruption and resumption of outpatient cardiac rehabilitation due to COVID-19. Int. J. Rehabil. Res. Int. Z. Fur Rehabil. Rev. Int. Rech. Readapt. 2021, 44, 200–204. [Google Scholar] [CrossRef]
- Sun, S.; Folarin, A.A.; Ranjan, Y.; Rashid, Z.; Conde, P.; Stewart, C.; Cummins, N.; Matcham, F.; Dalla Costa, G.; Simblett, S.; et al. Using Smartphones and Wearable Devices to Monitor Behavioral Changes During COVID-19. J. Med. Internet Res. 2020, 22, e19992. [Google Scholar] [CrossRef] [PubMed]
- Kirwan, R.; McCullough, D.; Butler, T.; de Heredia, F.P.; Davies, I.G.; Stewart, C. Sarcopenia during COVID-19 lockdown restrictions: Long-term health effects of short-term muscle loss. GeroScience 2020, 42, 1547–1578. [Google Scholar] [CrossRef]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Otobe, Y.; Suzuki, M.; Koyama, S.; Kikuchi, T.; Kusumi, H.; Arai, H. Letter to the Edi-tor: Recovery of Physical Activity among Older Japanese Adults since the First Wave of the COVID-19 Pandemic. J. Nutr. Health Aging 2020, 24, 1036–1037. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rodríguez, P.; de Bustamante, M.D.; Mollá, S.A.; Arenas, M.C.; Jiménez-Armero, S.; Esclapez, P.L.; González-Espinoza, L.; Boixareu, C.B. Functional, cognitive, and nutritional decline in 435 elderly nursing home residents after the first wave of the COVID-19 Pandemic. Eur. Geriatr. Med. 2021, 12, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Ghanem, J.; Colicchio, B.; Andrès, E.; Geny, B.; Dieterlen, A. Lockdown Effect on Elderly Nutritional Health. J. Clin. Med. 2021, 10, 5052. [Google Scholar] [CrossRef] [PubMed]
- Zamora, E.B.C.; Romero, M.M.; Sahuquillo, M.T.T.; Céspedes, A.A.; Andrés-Petrel, F.; Ballesteros, C.G.; Alfaro, V.S.-F.; López-Bru, R.; López-Utiel, M.; Cifuentes, S.C.; et al. Psychological and Functional Impact of COVID-19 in Long-Term Care Facilities: The COVID-A Study. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2022, 30, 431–443. [Google Scholar] [CrossRef] [PubMed]
- Gareri, P.; Fumagalli, S.; Malara, A.; Mossello, E.; Trevisan, C.; Volpato, S.; Coin, A.; Calsolaro, V.; Bellelli, G.; Del Signore, S.; et al. Management of Older Outpatients during the COVID-19 Pandemic: The GeroCovid Ambulatory Study. Gerontology 2021, 68, 412–417. [Google Scholar] [CrossRef]
- Hörnsten, C.; Littbrand, H.; Boström, G.; Rosendahl, E.; Lundin-Olsson, L.; Nordström, P.; Gustafson, Y.; Lövheim, H. Measurement error of the Mini-Mental State Examination among individuals with dementia that reside in nursing homes. Eur. J. Ageing 2020, 18, 109–115. [Google Scholar] [CrossRef]
- Clark, C.M.; Sheppard, L.; Fillenbaum, G.G.; Galasko, D.; Morris, J.C.; Koss, E.; Mohs, R.; Heyman, A. Variability in Annual Mini-Mental State Examination Score in Patients With Probable Alzheimer Disease: A clinical perspective of data from the Consortium to Establish a Registry for Alzheimer’s. Arch. Neurol. 1999, 56, 857–862. [Google Scholar] [CrossRef]
- Ries, J.D.; Echternach, J.L.; Nof, L.; Blodgett, M.G. Test-Retest Reliability and Minimal Detectable Change Scores for the Timed “Up & Go” Test, the Six-Minute Walk Test, and Gait Speed in People With Alzheimer Disease. Phys. Ther. 2009, 89, 569–579. [Google Scholar] [CrossRef]
- Lin, S.-C.; Lin, K.-H.; Lee, Y.-C.; Peng, H.-Y.; Chiu, E.-C. Test-retest reliability of the Mini Nutritional Assessment and its relationship with quality of life in patients with stroke. PLoS ONE 2019, 14, e0218749. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.M.; Wang, Y.-C.; Lee, C.-H.; Chen, M.-H.; Hsieh, C.-L. A comparison of test–retest reliability and random measurement error of the Barthel Index and modified Barthel Index in patients with chronic stroke. Disabil. Rehabil. 2020, 44, 2099–2103. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-C.; Yu, W.-H.; Hsueh, I.-P.; Chen, S.-S.; Hsieh, C.-L. Test-retest reliability and responsiveness of the Barthel Index-based Supplementary Scales in patients with stroke. Eur. J. Phys. Rehabil. Med. 2017, 53, 710–718. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographic Characteristics | Mean ± SEM | Median (IQR) |
|---|---|---|
| Age (years) | 80.2 ± 2.4 | 81 (74.5–86) |
| Sex, n (%) | ||
| Male | 7 | (41.2%) |
| Female | 10 | (58.8%) |
| Body Mass Index (kg/m2) | 24.2 ± 0.7 | 24.3 (22.8–25.3) |
| Educational level, n (%) | ||
| Illiterate | 2 | (11.8%) |
| Literate | 15 | (88.2%) |
| Marital Status, n (%) | ||
| Married | 6 | (35.3%) |
| Widowed | 10 | (58.8%) |
| Divorced | 1 | (5.9%) |
| Comorbid disease number, n (%) | 3 | (2–4) |
| Comorbidities, n (%) | ||
| Hypertension | 8 | (47.1%) |
| Diabetes mellitus | 5 | (29.4%) |
| Parkinson’s disease | 4 | (23.5%) |
| Cerebrovascular accident | 3 | (17.6%) |
| Cardiovascular diseases | 2 | (11.8%) |
| Long-term care disability level, n (%) | ||
| 2 | 2 | (11.8%) |
| 3 | 1 | (5.9%) |
| 4 | 8 | (47.1%) |
| 5 | 3 | (17.6%) |
| 6 | 3 | (17.6%) |
| Clinical dementia rating, n (%) | ||
| 0.5 | 6 | (35.3%) |
| 1 | 7 | (41.2%) |
| 2 | 3 | (17.6%) |
| 3 | 1 | (5.9%) |
| Baseline | After 3-Month Restriction | After 3-Month Resumption | p Value | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SEM | Median (IQR) | Mean ± SEM | Median (IQR) | Mean ± SEM | Median (IQR) | ||
| Body mass index | 24.2 ± 0.7 | 24.3 (22.8–25.3) | 23.6 ± 0.7 | 23.7 (22.1–25.3) | 23.9 ± 0.7 | 24.2 (22.6–25.1) | 0.215 |
| Mini-mental state examination | 21.9 ± 1.4 | 21.0 (18.5–28.5) | 20.8 ± 1.5 | 19.0 (17.0–27.5) | 20.9 ± 1.4 | 20.0 (17.0–27.0) | 0.019 |
| Five-item geriatric depression scale | 0.1 ± 0.1 | 0 (0–0) | 0.4 ± 0.2 | 0 (0–0.5) | 0.4 ± 0.1 | 0 (0–1.0) | 0.186 |
| Barthel index of activities of daily living | 83.5 ± 3.1 | 85.0 (72.5–95.0) | 82.6 ± 3.3 | 85.0 (70.0–95.0) | 81.5 ± 3.3 | 85.0 (70.0–92.5) | 0.021 |
| Lawton instrumental activities of daily living scale | 2.8 ± 0.4 | 3.0 (1.5–5.0) | 2.8 ± 0.5 | 2.0 (1.5–5.0) | 2.7 ± 0.5 | 2.0 (1.0–5.0) | 0.472 |
| 6 m walking speed | 0.8 ± 0.1 | 0.9 (0.6–0.9) | 0.8 ± 0.1 | 0.9 (0.5–1.1) | 0.8 ± 0.1 | 0.9 (0.6–1.0) | 0.133 |
| Timed up-and-go test | 25.0 ± 9.2 | 12.8 (10.5–19.4) | 31.0 ± 13.4 | 16.3 (11.8–21.0) | 26.1 ± 9.6 | 13.4 (11.5–19.5) | 0.047 |
| Functional reach test | 22.9 ± 1.7 | 22.3 (17.9–26.8) | 20.8 ± 1.7 | 19.4 (15.7–24.6) | 22.3 ± 1.7 | 20.9 (18.4–24.8) | 0.368 |
| Mini nutritional assessment short form | 12.5 ± 0.3 | 13.0 (12.0–13.0) | 11.4 ± 0.4 | 12.0 (10.5–12.0) | 12.4 ± 0.3 | 13.0 (11.5–13.0) | 0.001 |
| EQ-5D utility index | 0.805 ± 0.051 | 0.877 (0.625–1) | 0.798 ± 0.052 | 0.756 (0.61–1) | 0.817 ± 0.046 | 0.833 (0.625–1) | 0.268 |
| EQ-visual analogue scale | 83.9 ± 3.1 | 85.0 (75–95) | 82.5 ± 3.6 | 85.0 (77.5–95) | 86.4 ± 3.4 | 90.0 (77.5–99.0) | 0.463 |
| After 3-Month Restriction | After 3-Month Resumption | |||||||
|---|---|---|---|---|---|---|---|---|
| Timed Up-and-Go Test | Mini Nutritional Assessment Short-Form | Timed Up-and-Go test | Mini Nutritional Assessment Short-Form | |||||
| rs | p Value | rs | p Value | rs | p Value | rs | p Value | |
| Baseline parameters of CGA | ||||||||
| Body mass index | −0.10 | 0.701 | 0.30 | 0.243 | −0.01 | 0.978 | 0.73 | 0.001 |
| Mini-mental state examination | −0.15 | 0.565 | 0.09 | 0.745 | −0.28 | 0.271 | 0.18 | 0.484 |
| Five-item geriatric depression scale | −0.10 | 0.697 | −0.32 | 0.205 | −0.31 | 0.232 | −0.46 | 0.065 |
| Barthel index of activities of daily living | −0.61 | 0.009 | 0.26 | 0.321 | −0.66 | 0.004 | 0.48 | 0.051 |
| Lawton instrumental activities of daily living scale | −0.54 | 0.025 | 0.01 | 0.955 | −0.75 | 0.001 | 0.13 | 0.615 |
| 6 m walking speed | −0.84 | <0.001 | −0.22 | 0.386 | −0.70 | 0.002 | −0.05 | 0.834 |
| Functional reach test | −0.40 | 0.124 | 0.49 | 0.056 | −0.48 | 0.057 | 0.02 | 0.943 |
| EQ-5D utility index | −0.60 | 0.011 | 0.26 | 0.319 | −0.55 | 0.023 | 0.24 | 0.349 |
| EQ-visual analogue scale | −0.74 | 0.001 | 0.08 | 0.761 | −0.63 | 0.007 | −0.20 | 0.436 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.-S.; Lin, C.-F.; Kuo, F.-H.; Chou, Y.-C.; Lin, S.-Y. Impact of Daycare Service Interruption during COVID-19 Pandemic on Physical and Mental Functions and Nutrition in Older People with Dementia. Healthcare 2022, 10, 1744. https://doi.org/10.3390/healthcare10091744
Wang Y-S, Lin C-F, Kuo F-H, Chou Y-C, Lin S-Y. Impact of Daycare Service Interruption during COVID-19 Pandemic on Physical and Mental Functions and Nutrition in Older People with Dementia. Healthcare. 2022; 10(9):1744. https://doi.org/10.3390/healthcare10091744
Chicago/Turabian StyleWang, Ya-Shin, Cheng-Fu Lin, Fu-Hsuan Kuo, Ying-Chyi Chou, and Shih-Yi Lin. 2022. "Impact of Daycare Service Interruption during COVID-19 Pandemic on Physical and Mental Functions and Nutrition in Older People with Dementia" Healthcare 10, no. 9: 1744. https://doi.org/10.3390/healthcare10091744