
Collaboration between Psychiatrists and Other Allied Medical Specialists for the Treatment of Delusional Disorders
 , ,
, ,
Abstract
:1. Introduction
Aims
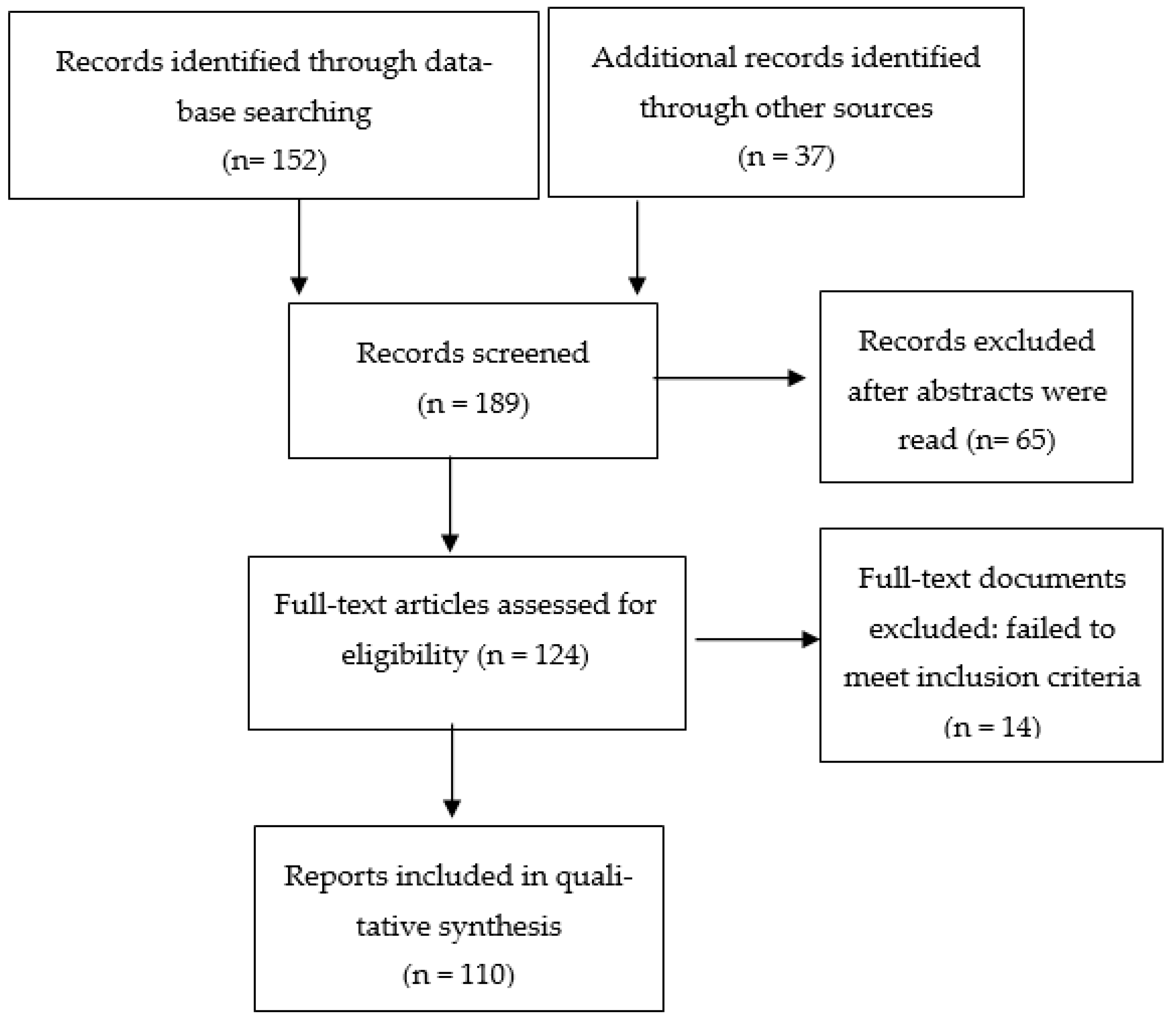
2. Methods
3. Collaboration with Neurologists
3.1. Delusional Disorder Can Precede a Diagnosis of Dementia
3.2. Cognitive Decline Predicts Poor Response to Psychotropic Medications
4. Collaboration with Ophthalmology and Otolaryngology
5. Collaboration with Dermatologists
6. Collaboration with Pain Specialists
7. Collaboration with Gastroenterologists
8. Collaboration with Sleep Specialists
9. Collaboration with Cardiologists
10. Collaboration with Pharmacologists
11. Discussion
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DSM-5, 5th ed.; American Psychiatric Publishing: Arlinghton, VA, USA; Washington, DC, USA, 2013.
- Maina, G.; Albert, U.; Badà, A.; Bogetto, F. Occurrence and clinical correlates of psychiatric co-morbidity in delusional disorder. Eur. Psychiatry 2001, 16, 222–228. [Google Scholar] [CrossRef]
- de Portugal, E.; Martínez, C.; González, N.; del Amo, V.; Haro, J.M.; Cervilla, J.A. Clinical and cognitive correlates of psychiatric comorbidity in delusional disorder outpatients. Aust. N. Z. J. Psychiatry 2011, 45, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Koyanagi, A.; Veronese, N.; Vancampfort, D.; Solmi, M.; Gaughran, F.; Carvalho, A.F.; Lally, J.; Mitchell, A.J.; Mugisha, J.; et al. Physical multimorbidity and psychosis: Comprehensive cross sectional analysis including 242,952 people across 48 low- and middle-income countries. BMC Med. 2016, 14, 189. [Google Scholar] [CrossRef]
- Singh, R.; Bansal, Y.; Medhi, B.; Kuhad, A. Antipsychotics-induced metabolic alterations: Recounting the mechanistic insights, therapeutic targets and pharmacological alternatives. Eur. J. Pharmacol. 2019, 844, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Carli, M.; Kolachalam, S.; Longoni, B.; Pintaudi, A.; Baldini, M.; Aringhieri, S.; Fasciani, I.; Annibale, P.; Maggio, R.; Scarselli, M. Atypical antipsychotics and metabolic syndrome: From molecular mechanisms to clinical differences. Pharmaceuticals 2021, 14, 238. [Google Scholar] [CrossRef]
- Nordentoft, M.; Plana-Ripoll, O.; Laursen, T.M. Cancer and schizophrenia. Curr. Opin. Psychiatry 2021, 34, 260–265. [Google Scholar] [CrossRef]
- Docherty, M.; Stubbs, B.; Gaughran, F. Strategies to deal with comorbid physical illness in psychosis. Epidemiol. Psychiatr. Sci. 2016, 25, 197–204. [Google Scholar] [CrossRef]
- Hüfner, K.; Frajo-Apor, B.; Hofer, A. Neurology issues in schizophrenia. Curr. Psychiatry Rep. 2015, 17, 32. [Google Scholar] [CrossRef]
- González-Rodríguez, A.; Seeman, M.V.; Guàrdia, A.; Natividad, M.; Marín, M.; Labad, J.; Monreal, J.A. Gynecological health concerns in women with schizophrenia and related disorders: A narrative review of recent studies. Women 2022, 2, 1–14. [Google Scholar] [CrossRef]
- Diaz-Caneja, C.M.; Cervilla, J.A.; Haro, J.M.; Arango, C.; de Portugal, E. Cognition and functionality in delusional disorder. Eur. Psychiatry 2020, 55, 52–60. [Google Scholar] [CrossRef]
- Iezzoni, L.I. Dangers of diagnostic overshadowing. NEJM 2019, 380, 2092–2093. [Google Scholar] [CrossRef] [PubMed]
- Agbayewa, M.O. Earlier psychiatric morbidity in patients with Alzheimer’s disease. J. Am. Geriatr. Soc. 1986, 34, 561–564. [Google Scholar] [CrossRef] [PubMed]
- Leinonen, E.; Santala, M.; Hyötylä, T.; Santala, H.; Eskola, N.; Salokangas, R.K. Elderly patients with major depressive disorder and delusional disorder are at increased risk of subsequent dementia. Nord. J. Psychiatry 2004, 58, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Jellinger, K.A. Morphological basis of Parkinson disease-associated cognitive impairment: An update. J. Neural. Transm. 2022, 129, 977–999. [Google Scholar] [CrossRef]
- Oh, M.; Kim, J.W.; Lee, S.M. Delusional parasitosis as premotor symptom of Parkinson’s disease: A case report. World J. Clin. Cases 2022, 10, 2858–2863. [Google Scholar] [CrossRef] [PubMed]
- Anand, T.V.; Wallace, B.K.; Chase, H.S. Prevalence of potentially harmful multidrug interactions on medication lists of elderly ambulatory patients. BMC Geriatr. 2021, 21, 648. [Google Scholar] [CrossRef]
- Puustinen, J.; Nurminen, J.; Löppönen, M.; Vahlberg, T.; Isoaho, R.; Räihä, I.; Kivelä, S.L. Population-based study. BMC Geriatr. 2011, 11, 70. [Google Scholar]
- Wojt, I.R.; Cairns, R.; Clough, A.J.; Tan, E.C.K. The prevalence and characteristics of psychotropic-related hospitalizations in older people: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2021, 22, 1206–1214.e5. [Google Scholar] [CrossRef]
- Kendler, K.S.; Walsh, D. Schizophreniform disorder, delusional disorder and psychotic disorder not otherwise specified: Clinical features, outcome and familial psychopathology. Acta. Psychiatr. Scand. 1995, 91, 370–378. [Google Scholar] [CrossRef]
- Louhija, U.M.; Martola, J.; Juva, K.; Appelberg, B.G. Brain atrophy in first-episode psychosis of the elderly is associated with cognitive decline. Prim. Care. Companion. CNS Disord. 2021, 23, 20m02865. [Google Scholar] [CrossRef]
- Louhija, U.M.; Saarela, T.; Juva, K.; Appelberg, B. Brain atrophy is a frequent finding in elderly patients with first episode psychosis. Int. Psychogeriatr. 2017, 29, 1925–1929. [Google Scholar] [CrossRef] [PubMed]
- González-Rodríguez, A.; Seeman, M.V.; Izquierdo, E.; Natividad, M.; Guàrdia, A.; Román, E.; Monreal, J.A. Delusional disorder in old age: A hypothesis-driven review of recent work focusing on epidemiology, clinical aspects, and outcomes. Int. J. Environ. Res. Public Health 2022, 19, 7911. [Google Scholar] [CrossRef] [PubMed]
- D’Auria, A.; Wiseman, T.; Varghese, A.; Espiridion, E.D. Refractory delusional parasitosis in a 70-year-old woman. Cureus 2018, 10, e3120. [Google Scholar] [CrossRef] [PubMed]
- Chong, W.W.; Aslani, P.; Chen, T.F. Shared decision-making and interprofessional collaboration in mental healthcare: A qualitative study exploring perceptions of barriers and facilitators. J. Interprof. Care 2013, 27, 373–379. [Google Scholar] [CrossRef]
- Drake, R.E.; Cimpean, D.; Torrey, W.C. Shared decision making in mental health: Prospects for personalized medicine. Dialogues. Clin. Neurosci. 2009, 11, 455–463. [Google Scholar] [CrossRef]
- Velligan, D.I.; Weiden, P.J.; Sajatovic, M.; Scott, J.; Carpenter, D.; Ross, R.; Docherty, J.P. Strategies for addressing adherence problems in patients with serious and persistent mental illness: Recommendations from the expert consensus guidelines. J. Psychiatr. Pract. 2010, 16, 306–324. [Google Scholar] [CrossRef]
- Almeida, O.P.; Ford, A.H.; Hankey, G.J.; Yeap, B.B.; Golledge, J.; Flicker, L. Hearing loss and incident psychosis in later life: The Health in Men Study (HIMS). Int. J. Geriatr. Psychiatry 2019, 34, 408–414. [Google Scholar] [CrossRef]
- Linszen, M.M.; Brouwer, R.M.; Heringa, S.M.; Sommer, I.E. Increased risk of psychosis in patients with hearing impairment: Review and meta-analyses. Neurosci. Biobehav. Rev. 2016, 62, 1–20. [Google Scholar] [CrossRef]
- Porras Segovia, A.; Guerrero Jimenez, M.; Carrillo de Albornoz Calahorro, C.; Cervilla Ballesteros, J. Comorbidity between delusional disorder and sensory deficits. Results from the deliranda case register. Eur. Psychiatry 2016, 33 (Suppl. S1), S144–S145. [Google Scholar] [CrossRef]
- de Portugal, E.; González, N.; Vilaplana, M.; Haro, J.M.; Usall, J.; Cervilla, J.A. An empirical study of psychosocial and clinical correlates of delusional disorder: The DELIREMP study. Rev. Psiquiatr. Salud. Ment. 2009, 2, 72–82. [Google Scholar] [CrossRef]
- Turkson, S.N.; Asamoah, V. Common psychiatric disorders among the elderly attending a general psychiatric outpatient clinic in Accra, Ghana: A five year retrospective study (1989–1993). West Afr. J. Med. 1997, 16, 146–149. [Google Scholar] [PubMed]
- Thakkar, A.; Ooi, K.G.; Assaad, N.; Coroneo, M. Delusional infestation: Are you being bugged? Clin. Ophthalmol. 2015, 9, 967–970. [Google Scholar] [CrossRef] [PubMed]
- Carrión-Expósito, L.; Bancalero-Romero, C.; Hans-Chacón, A.; González-Moreno, J.M.; Baena-Baldomero, A.; Ruiz-Doblado, S. Paranoid delusion of the blind (Sanchís-Banús syndrome). Psiquiatr. Biol. 2012, 19, 95–98. [Google Scholar] [CrossRef]
- Shoham, N.; Lewis, G.; Hayes, J.; McManus, S.; Kiani, R.; Brugha, T.; Bebbington, P.; Cooper, C. Psychotic symptoms and sensory impairment: Findings from the 2014 adult psychiatric morbidity survey. Schizophr. Res. 2020, 215, 357–364. [Google Scholar] [CrossRef]
- Shoham, N.; Eskinazi, M.; Hayes, J.F.; Lewis, G.; Theodorsson, M.; Cooper, C. Associations between psychosis and visual acuity impairment: A systematic review and meta-analysis. Acta. Psychiatr. Scand. 2021, 144, 6–27. [Google Scholar] [CrossRef]
- Thewissen, V.; Myin-Germeys, I.; Bentall, R.; de Graaf, R.; Vollebergh, W.; van Os, J. Hearing impairment and psychosis revisited. Schizophr. Res. 2005, 76, 99–103. [Google Scholar] [CrossRef]
- Silverstein, S.M.; Keane, B.P.; Corlett, P.R. Oculomics in Schizophrenia Research. Schizophr. Bull. 2021, 47, 577–579. [Google Scholar] [CrossRef]
- Marschall, T.M.; Brederoo, S.G.; Ćurčić-Blake, B.; Sommer, I.E.C. Deafferentation as a cause of hallucinations. Curr. Opin. Psychiatry 2020, 33, 206–211. [Google Scholar] [CrossRef]
- Collerton, D.; Perry, E.; McKeith, I. Why people see things that are not here: A novel Perception and Attention Deficit model for recurrent complex visual hallucinations. Behav. Brain Sci. 2005, 28, 737–757. [Google Scholar] [CrossRef]
- Noblett, J.; Roberts, E. The importance of not jumping to conclusions: Syphilis as an organic cause of neurological, psychiatric and endocrine presentations. BMJ Case Rep. 2015, 2015, bcr2014207900. [Google Scholar] [CrossRef] [PubMed]
- Wagner-Jauregg, J. The history of the malaria treatment of general paralysis. 1946. Am. J. Psychiatry 1994, 151 (Suppl. S6), 231–235. [Google Scholar] [PubMed]
- Nevin, R.L.; Croft, A.M. Psychiatric effects of malaria and anti-malarial drugs: Historical and modern perspectives. Malar. J. 2016, 15, 332. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, P.P.; Borkakati, R.N.; Saikia, D.K. A review on Ekbom syndrome. J. Entomol. Zool. Stud. 2019, 7, 894–900. [Google Scholar]
- Mumcuoglu, K.Y.; Leibovici, V.; Reuveni, I.; Bonne, O. Delusional parasitosis: Diagnosis and treatment. Isr. Med. Assoc. J. 2018, 20, 456–460. [Google Scholar]
- Manschreck, T.C. Delusional disorder: The recognition and management of paranoia. J. Clin. Psychiatry 1996, 57 (Suppl. S3), 32–38. [Google Scholar] [PubMed]
- Reszke, R.; Pacan, P.; Reich, A.; Szepietowski, J.C. Delusional infestation in clinical practice over a period of two decades. Postepy. Dermatol. Alergol. 2021, 38, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Alonso, B.; Álvarez-Artero, E.; Martínez-Goñi, R.; Almeida, H.; Casado-Espada, N.M.; Jaén-Sánchez, N.; Velasco-Tirado, V.; Belhassen-García, M.; Pérez-Arellano, J.L. Delusional parasitosis. A multicenter retrospective study in Spanish infectious disease services. Enferm. Infecc. Microbiol. Clin. 2021, 39, 223–228. [Google Scholar] [CrossRef]
- Torales, J.; García, O.; Barrios, I.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A.; Jafferany, M. Delusional infestation: Clinical presentations, diagnosis, and management. J. Cosmet. Dermatol. 2020, 19, 3183–3188. [Google Scholar] [CrossRef]
- Todd, S.; Squire, S.B.; Bartlett, R.; Lepping, P. Delusional infestation managed in a combined tropical medicine and psychiatry clinic. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 18–23. [Google Scholar] [CrossRef]
- Lee, C.S.; Accordino, R.; Howard, J.; Koo, J. Psychopharmacology in dermatology. Dermatol. Ther. 2008, 21, 69–82. [Google Scholar] [CrossRef]
- Seeman, M.V. Skin and hair conditions in women with schizophrenia and related disorders. Women’s Health Res. 2018, 2, 14–28. [Google Scholar]
- González-Rodríguez, A.; Molina-Andreu, O.; Penadés, R.; Garriga, M.; Pons, A.; Catalán, R.; Bernardo, M. Delusional disorder over the reproductive life span: The potential influence of menopause on the clinical course. Schizophr. Res. Treat. 2015, 2015, 979605. [Google Scholar] [CrossRef] [PubMed]
- Delacerda, A.; Reichenberg, J.S.; Magid, M. Successful treatment of patients previously labeled as having “delusions of parasitosis” with antidepressant therapy. J. Drugs Dermatol. 2012, 11, 1506–1507. [Google Scholar]
- Gupta, M.A.; Vujcic, B.; Pur, D.R.; Gupta, A.K. Use of antipsychotic drugs in dermatology. Clin. Dermatol. 2018, 36, 765–773. [Google Scholar] [CrossRef]
- McPhie, M.L.; Kirchhof, M.G. A systematic review of antipsychotic agents for primary delusional infestation. J. Dermatolog. Treat. 2022, 33, 709–721. [Google Scholar] [CrossRef] [PubMed]
- Hollander, E.; Allen, A.; Kwon, J.; Aronowitz, B.; Schmeidler, J.; Wong, C.; Simeon, D. Clomipramine vs desipramine crossover trial in body dysmorphic disorder: Selective efficacy of a serotonin reuptake inhibitor in imagined ugliness. Arch. Gen. Psychiatry 1999, 56, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Kawakatsu, S.; Nadaoka, T.; Okuyama, N.; Otani, K. Clomipramine treatment of delusional disorder, somatic type. Int. Clin. Psychopharmacol. 1999, 14, 181–183. [Google Scholar] [CrossRef]
- Comardelle, N.; Edinoff, A.; Fort, J. Delusions of glass under skin: An unusual case of somatic-type delusional disorder treated with olanzapine. Health Psychol. Res. 2022, 10, 35500. [Google Scholar] [CrossRef]
- Singh, A.R.; Veale, D. Understanding and treating body dysmorphic disorder. Ind. J. Psychiatry 2019, 61 (Suppl. S1), S131–S135. [Google Scholar]
- Seale, L.; Gaulding, J.V.; Porto, D.; Prabhakar, D.; Kerr, H. Implementation of a psychodermatology clinic at a major health system in Detroit. Intern. J. Women’s Dermatol. 2018, 4, 227–229. [Google Scholar] [CrossRef]
- Katz, J.; Rosenbloom, B.N.; Fashler, S. Chronic pain, psychopathology, and DSM-V somatic symptom disorder. Can. J. Psychiatry 2015, 60, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Karakuş, İ.H.; Bulut, N.S. Oral cenesthopathy superimposed on burning mouth syndrome treated with aripiprazole: A case report with a phenomenological overview. Gerodontology 2021, 38, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Watanabe, M.; Takao, C.; Hong, C.; Liu, Z.; Suga, T.; Tu, T.T.H.; Sakamoto, J.; Umezaki, Y.; Yoshikawa, T.; et al. Clinical characteristics of predominantly unilateral oral cenesthopathy with and without neurovascular contact. Front. Neurol. 2021, 12, 744561. [Google Scholar] [CrossRef]
- Uezato, A.; Yamamoto, N.; Kurumaji, A.; Toriihara, A.; Umezaki, Y.; Toyofuku, A.; Nishikawa, T. Improvement of asymmetrical temporal blood flow in refractory oral somatic delusion after successful electroconvulsive therapy. J. ECT 2012, 28, 50–51. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Kawakatsu, S.; Komatani, A.; Okuyama, N.; Otani, K. Possible association between delusional disorder, somatic type and reduced regional cerebral blood flow. Prog. Neuropsychopharmacol. Biol. Psychiatry 1999, 23, 353–357. [Google Scholar] [CrossRef]
- Gerdle, B.; Åkerblom, S.; Brodda Jansen, G.; Enthoven, P.; Ernberg, M.; Dong, H.J.; Stålnacke, B.M.; Äng, B.O.; Boersma, K. Who benefits from multimodal rehabilitation—An exploration of pain, psychological distress, and life impacts in over 35,000 chronic pain patients identified in the Swedish Quality Registry for Pain Rehabilitation. J. Pain. Res. 2019, 12, 891–908. [Google Scholar] [CrossRef] [Green Version]
- Ukai, K.; Kimura, H.; Arao, M.; Aleksic, B.; Yamauchi, A.; Ishihara, R.; Iritani, S.; Kurita, K.; Ozaki, N. Effectiveness of low-dose milnacipran for a patient suffering from pain disorder with delusional disorder (somatic type) in the orofacial region. Psychogeriatrics 2013, 13, 99–102. [Google Scholar] [CrossRef]
- Tabbalat, R.R.; Cal, N.V.; Mayigegowda, K.K.; Desilets, D.J. Two cases of gastrointestinal delusional parasitosis presenting as folie á deux. ACG Case Rep. J. 2019, 6, e00183. [Google Scholar] [CrossRef]
- Stein, L.L.; Jesudian, A.B. Acute liver injury with severe coagulopathy in marasmus caused by a somatic delusional disorder. Case Rep. Hepatol. 2011, 2011, 176894. [Google Scholar] [CrossRef]
- Geka, A.E.; Venetis, C.; Apatangelos, D.; Kalimeris, S.; Psarra, V.; Drakonakis, N.; Doulgeraki, G.; Evangelatou, R.; Garnetas, C. Delusional disorder with severe weight loss. Eur. Psychiatry 2011, 26 (Suppl. S1), 1720. [Google Scholar] [CrossRef]
- Talley, N.J. What Causes Functional Gastrointestinal Disorders? A Proposed Disease Model. Am. J. Gastroenterol. 2020, 115, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Thylur, D.S.; Goldsmith, D.R. Brick by Brick: Building a Transdiagnostic Understanding of Inflammation in Psychiatry. Harv. Rev. Psychiatry 2022, 30, 40–53. [Google Scholar] [CrossRef] [PubMed]
- Shiina, T.; Hosomichi, K.; Inoko, H.; Kulski, J.K. The HLA genomic loci map: Expression, interaction, diversity and disease. J. Hum. Genet. 2009, 54, 15–39. [Google Scholar] [CrossRef] [PubMed]
- Corvin, A.; Morris, D.W. Genome-wide association studies: Findings at the major histocompatibility complex locus in psychosis. Biol. Psychiatry 2014, 75, 276–283. [Google Scholar] [CrossRef]
- Debnath, M.; Das, S.K.; Bera, N.K.; Nayak, C.R.; Chaudhuri, T.K. Genetic associations between delusional disorder and paranoid schizophrenia: A novel etiologic approach. Can. J. Psychiatry 2006, 51, 342–349. [Google Scholar] [CrossRef]
- Debnath, M.; Das, S.K.; Bera, N.K.; Nayak, C.R.; Chaudhuri, T.K. A study of HLA-linked genes in a monosymptomatic psychotic disorder in an Indian Bengali population. Can. J. Psychiatry 2005, 50, 269–274. [Google Scholar] [CrossRef]
- Solmi, M.; Murru, A.; Pacchiarotti, I.; Undurraga, J.; Veronese, N.; Fornaro, M.; Stubbs, B.; Monaco, F.; Vieta, E.; Seeman, M.V.; et al. Safety, tolerability, and risks associated with first- and second-generation antipsychotics: A state-of-the-art clinical review. Ther. Clin. Risk Manag. 2017, 13, 757–777. [Google Scholar] [CrossRef]
- González-Rodríguez, A.; Labad, J.; Seeman, M.V. Sleep disturbances in patients with persistent delusions: Prevalence, clinical associations, and therapeutic strategies. Clocks Sleep 2020, 2, 399–415. [Google Scholar] [CrossRef]
- González-Rodríguez, A.; Haba-Rubio, J.; Usall, J.; Natividad, M.; Soria, V.; Labad, J.; Monreal, J.A. Hormone targets for the treatment of sleep disorders in postmenopausal women with schizophrenia: A narrative review. Clocks Sleep 2022, 4, 52–65. [Google Scholar] [CrossRef]
- Canellas, F.; Lin, L.; Julià, M.R.; Clemente, A.; Vives-Bauza, C.; Ollila, H.M.; Hong, S.C.; Arboleya, S.M.; Einen, M.A.; Faraco, J.; et al. Dual cases of type 1 narcolepsy with schizophrenia and other psychotic disorders. J. Clin. Sleep Med. 2014, 10, 1011–1018. [Google Scholar] [CrossRef]
- Basu, A.; Kundu, S.; Khurana, H. Olanzapine-induced restless leg syndrome: A case report and review of literature. Indian J. Pharmacol. 2014, 46, 450–452. [Google Scholar] [CrossRef] [PubMed]
- Seeman, M.V. Why are women prone to restless legs syndrome? Int. J. Environ. Res. Public Health 2020, 17, 368. [Google Scholar] [CrossRef] [PubMed]
- Seeman, M.V. Diagnosis and treatment of sleep apnoea in women with schizophrenia. J. Ment. Health 2014, 23, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Giles, J.J.; Ling, I.; McArdle, N.; Bucks, R.S.; Cadby, G.; Singh, B.; Morgan, V.A.; Gabriel, L.; Waters, F. Obstructive Sleep Apnea is treatable with Continuous Positive Airway Pressure in people with schizophrenia and other psychotic disorders. Schizophr. Bull. 2022, 48, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Bottlender, R.; Möller, H.J. Negative symptoms due to sleep apnea syndrome in a patient with a delusional disorder. Eur. Psychiatry 1999, 14, 352. [Google Scholar] [CrossRef]
- Oh, H.Y.; Singh, F.; Koyanagi, A.; Jameson, N.; Schiffman, J.; DeVylder, J. Sleep disturbances are associated with psychotic experiences: Findings from the National Comorbidity Survey Replication. Schizophr. Res. 2016, 171, 74–78. [Google Scholar] [CrossRef]
- Regestein, Q.R.; Reich, P. A sleep clinic within a general hospital psychiatry service. Gen. Hosp. Psychiatry 1980, 2, 112–117. [Google Scholar] [CrossRef]
- Dahale, A.B.; Hemendra, S.; Chaturvedi, S.K. Need for Sleep Clinics in Psychiatric Practice. Indian J. Sleep Med. 2012, 7, 1–5. [Google Scholar] [CrossRef]
- Ward, M.; Druss, B. The epidemiology of diabetes in psychotic disorders. Lancet Psychiatry 2015, 2, 431–451. [Google Scholar] [CrossRef]
- Foley, D.L.; Mackinnon, A.; Morgan, V.A.; Watts, G.F.; Castle, D.J.; Waterreus, A.; Galletly, C.A. Common familial risk factors for schizophrenia and diabetes mellitus. Aust. N. Z. J. Psychiatry 2016, 50, 488–494. [Google Scholar] [CrossRef]
- Eriksson, S.V.; Osbu, V.; Olsson, E.; Edman, G. Treatment of cardiovascular risk factors in patients with serious mental disorders. Eur. Heart. J. 2013, 34 (Suppl. S1), P2534. [Google Scholar] [CrossRef]
- Ösby, U.; Olsson, E.; Edman, G.; Hilding, A.; Eriksson, S.V.; Östenson, C.G. Psychotic disorder is an independent risk factor for increased fasting glucose and waist circumference. Nordic J. Psychiatry 2014, 68, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Howell, S.; Yarovova, E.; Khwanda, A.; Rosen, S.D. Cardiovascular effects of psychotic illnesses and antipsychotic therapy. Heart 2019, 105, 1852–1859. [Google Scholar] [CrossRef] [PubMed]
- Hadlandsmyth, K.; Rosenbaum, D.L.; Craft, J.M.; Gervino, E.V.; White, K.S. Health care utilisation in patients with non-cardiac chest pain: A longitudinal analysis of chest pain, anxiety and interoceptive fear. Psychol. Health 2013, 28, 849–861. [Google Scholar] [CrossRef] [PubMed]
- Sobański, J.A.; Klasa, K.; Popiołek, L.; Rutkowski, K.; Dembińska, E.; Mielimąka, M.; Cyranka, K.; Müldner-Nieckowski, Ł.; Smiatek-Mazgaj, B.; Rodziński, P. Complaints of neurotic patients that are of interest for a cardiologist. Kardiol. Pol. 2015, 73, 1114–1121. [Google Scholar] [CrossRef]
- Hocaoglu, C.; Gulec, M.Y.; Durmus, I. Psychiatric comorbidity in patients with chest pain without a cardiac etiology. Isr. J. Psychiatry Relat. Sci. 2008, 45, 49–54. [Google Scholar]
- Rozanski, A.; Blumenthal, J.A.; Davidson, K.W.; Saab, P.G.; Kubzansky, L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: The emerging field of behavioral cardiology. J. Am. Coll. Cardiol. 2005, 45, 637–651. [Google Scholar] [CrossRef] [Green Version]
- Siepmann, M.; Kirch, W. Psychosomatic aspects of cardiac arrhythmias. Med. Klin. 2010, 105, 479–484. [Google Scholar] [CrossRef]
- Seeman, M.V. Pseudocyesis, delusional pregnancy, and psychosis: The birth of a delusion. World J. Clin. Cases 2014, 2, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Manjunatha, N.; Saddichha, S. Delusion of pregnancy associated with antipsychotic induced metabolic syndrome. World J. Biol. Psychiatry 2009, 10, 669–670. [Google Scholar] [CrossRef]
- Arbus, C.; Clement, J.P.; Bougerol, T.; Fremont, P.; Lancrenon, S.; Camus, V. Health management of older persons with chronically medicated psychotic disorders: The results of a survey in France. Int. Psychogeriatr. 2012, 24, 496–502. [Google Scholar] [CrossRef] [PubMed]
- González-Rodríguez, A.; Guàrdia, A.; Álvarez Pedrero, A.; Betriu, M.; Cobo, J.; Sanz, N.; Acebillo, S.; Monreal, J.A.; Palao-Vidal, D.; Labad, J. Monitoring of antipsychotic plasma levels in the assessment of poor response and nonadherence to antipsychotics in delusional disorder. Eur. Psychiatry 2021, 64 (Suppl. S1), S158. [Google Scholar] [CrossRef]
- Silva, H.; Jerez, S.; Ramirez, A.; Renteria, P.; Aravena, N.; Salazar, D.; Labarca, R. Effects of pimozide on the psychopathology of delusional disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 1998, 22, 331–340. [Google Scholar] [CrossRef]
- Herbel, B.L.; Stelmach, H. Involuntary medication treatment for competency restoration of 22 defendants with delusional disorder. J. Am. Acad. Psychiatry Law 2007, 35, 47–59. [Google Scholar] [PubMed]
- Strauss, M.; Heinritz, W.; Hegerl, U.; Kopf, A. Risperidone intoxication in a patient with a genetic predisposition as “poor [non]metabolizer”. Psychiatr. Prax. 2010, 37, 199–201. [Google Scholar]
- Arranz, M.J.; Gonzalez-Rodriguez, A.; Perez-Blanco, J.; Penadés, R.; Gutierrez, B.; Ibañez, L.; Arias, B.; Brunet, M.; Cervilla, J.; Salazar, J.; et al. A pharmacogenetic intervention for the improvement of the safety profile of antipsychotic treatments. Transl. Psychiatry 2019, 9, 177. [Google Scholar] [CrossRef]
- Walden, L.M.; Brandl, E.J.; Tiwari, A.K.; Cheema, S.; Freeman, N.; Braganza, N.; Kennedy, J.L.; Müller, D.J. Genetic testing for CYP2D6 and CYP2C19 suggests improved outcome for antidepressant and antipsychotic medication. Psychiatry Res. 2019, 279, 111–115. [Google Scholar] [CrossRef]
- González-Rodríguez, A.; Molina-Andreu, O.; Penadés, R.; Bernardo, M.; Catalán, R. Effectiveness of long-acting injectable antipsychotics in delusional disorders with nonprominent hallucinations and without hallucinations. Int. Clin. Psychopharmacol. 2014, 29, 177–180. [Google Scholar] [CrossRef]
- Firth, J.; Siddiqi, N.; Koyanagi, A.I.; Siskind, D.; Rosenbaum, S.; Galletly, C.; Allan, S.; Caneo, C.; Carney, R.; Carvalho, A.F.; et al. The lancet psychiatry commission: A blueprint for protecting physical health in people with mental illness. Lancet Psychiatry 2019, 6, 675–712. [Google Scholar] [CrossRef]
- Cho, H.L. Can intersectionality help lead to more accurate diagnosis? Am. J. Bioeth. 2019, 19, 37–39. [Google Scholar] [CrossRef]
- Seeman, M.V.; Gordon, A. A pain consultation clinic for women. Can. Med. Assoc. J. 1998, 159, 382–384. [Google Scholar]
- Gautam, S.; Gautam, M.; Jain, A.; Yadav, K. Overview of practice of Consultation-Liaison Psychiatry. Indian J. Psychiatry 2022, 64 (Suppl. S2), S201–S210. [Google Scholar] [CrossRef] [PubMed]
- Kelly, B.J.; Perkins, D.A.; Fuller, J.D.; Parker, S.M. Shared care in mental illness: A rapid review to inform implementation. Int. J. Ment. Health Syst. 2011, 5, 31. [Google Scholar] [CrossRef] [PubMed]
- Smulevich, A.B.; Lvov, A.N.; Romanov, D.V. Hypochondriasis Circumscripta: A neglected concept with important implications in psychodermatology. Acta. Derm. Venereol. 2016, 96, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Druss, B.G.; Rohrbaugh, R.M.; Levinson, C.M.; Rosenheck, R.A. Integrated medical care for patients with serious psychiatric illness: A randomized trial. Arch. Gen. Psychiatry 2001, 58, 861–868. [Google Scholar] [CrossRef]


{kind=link}
| Specialty | How Psychiatry Can Help Other Specialties | How Other Doctors Can Help Psychiatry |
|---|---|---|
| Neurology | DD can precede the onset of Parkinson’s disease and other dementias | Investigation of cognitive defects and brain structure helps predict Rx response |
| Ophthalmology and Otorhinolaryngology | Sensory impairments May have psychological bases | Rx of deafness and blindness reduces DD symptoms |
| Dermatology | Skin disease may be self-inflicted | Early referral to psychiatry improves outcome |
| Pain specialty | Chronic pain benefits from psychiatric Rx | Specialized pain Rx helps somatic type DD |
| Gastroenterology | Psychosis and inflammatory disease often co-exist | DD may show evidence of G.I. inflammation and auto-immunity |
| Sleep Units | Rx of psychotic symptoms & changes in antipsychotic regimens improve sleep disorders | Sleep apnoea needs to be ruled out in DD patients with negative symptoms |
| Cardiology | Trauma may precede chest pain and arrhythmias | Antipsychotic selection may need cardiological input |
| Pharmacology | Reporting adverse drug effects spurs the synthesis of better drugs | Experts help in testing for harmful drug-drug interactions |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Rodríguez, A.; Monreal, J.A.; Natividad, M.; Seeman, M.V. Collaboration between Psychiatrists and Other Allied Medical Specialists for the Treatment of Delusional Disorders. Healthcare 2022, 10, 1729. https://doi.org/10.3390/healthcare10091729
González-Rodríguez A, Monreal JA, Natividad M, Seeman MV. Collaboration between Psychiatrists and Other Allied Medical Specialists for the Treatment of Delusional Disorders. Healthcare. 2022; 10(9):1729. https://doi.org/10.3390/healthcare10091729
Chicago/Turabian StyleGonzález-Rodríguez, Alexandre, José Antonio Monreal, Mentxu Natividad, and Mary V. Seeman. 2022. "Collaboration between Psychiatrists and Other Allied Medical Specialists for the Treatment of Delusional Disorders" Healthcare 10, no. 9: 1729. https://doi.org/10.3390/healthcare10091729