
The Use of the Shikani Video-Assisted Intubating Stylet Technique in Patients with Restricted Neck Mobility
 , and
, and
Abstract
:1. Introduction
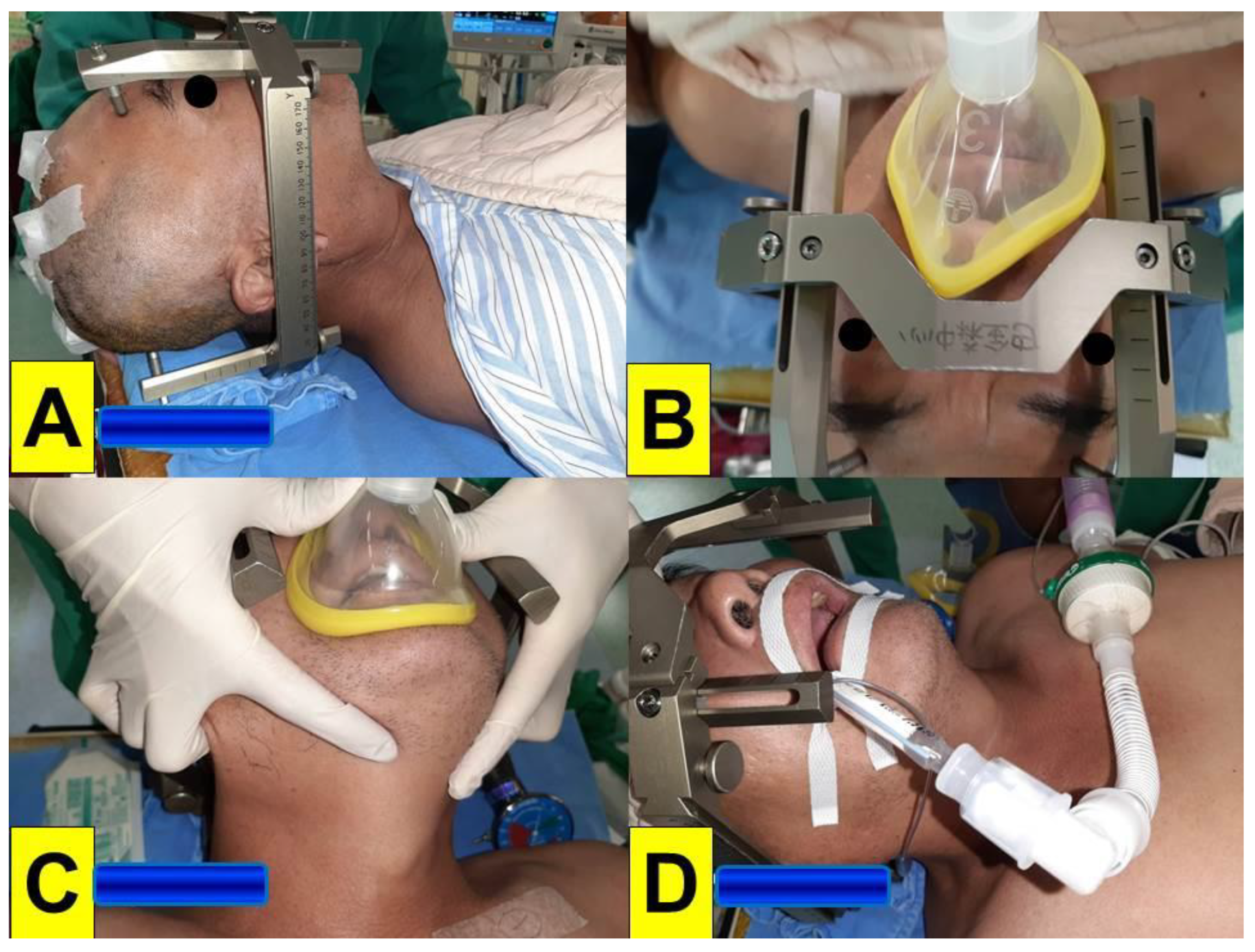
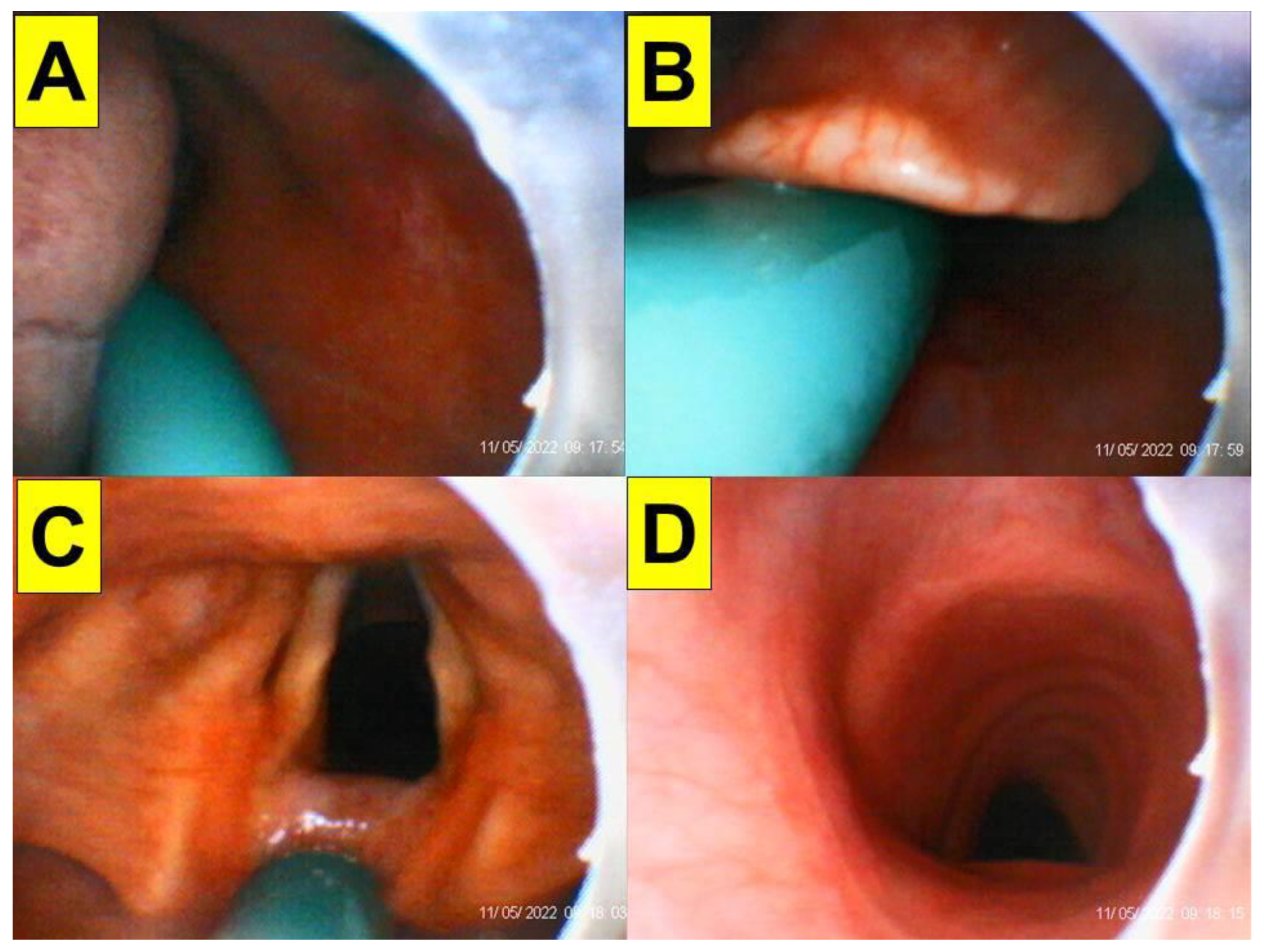
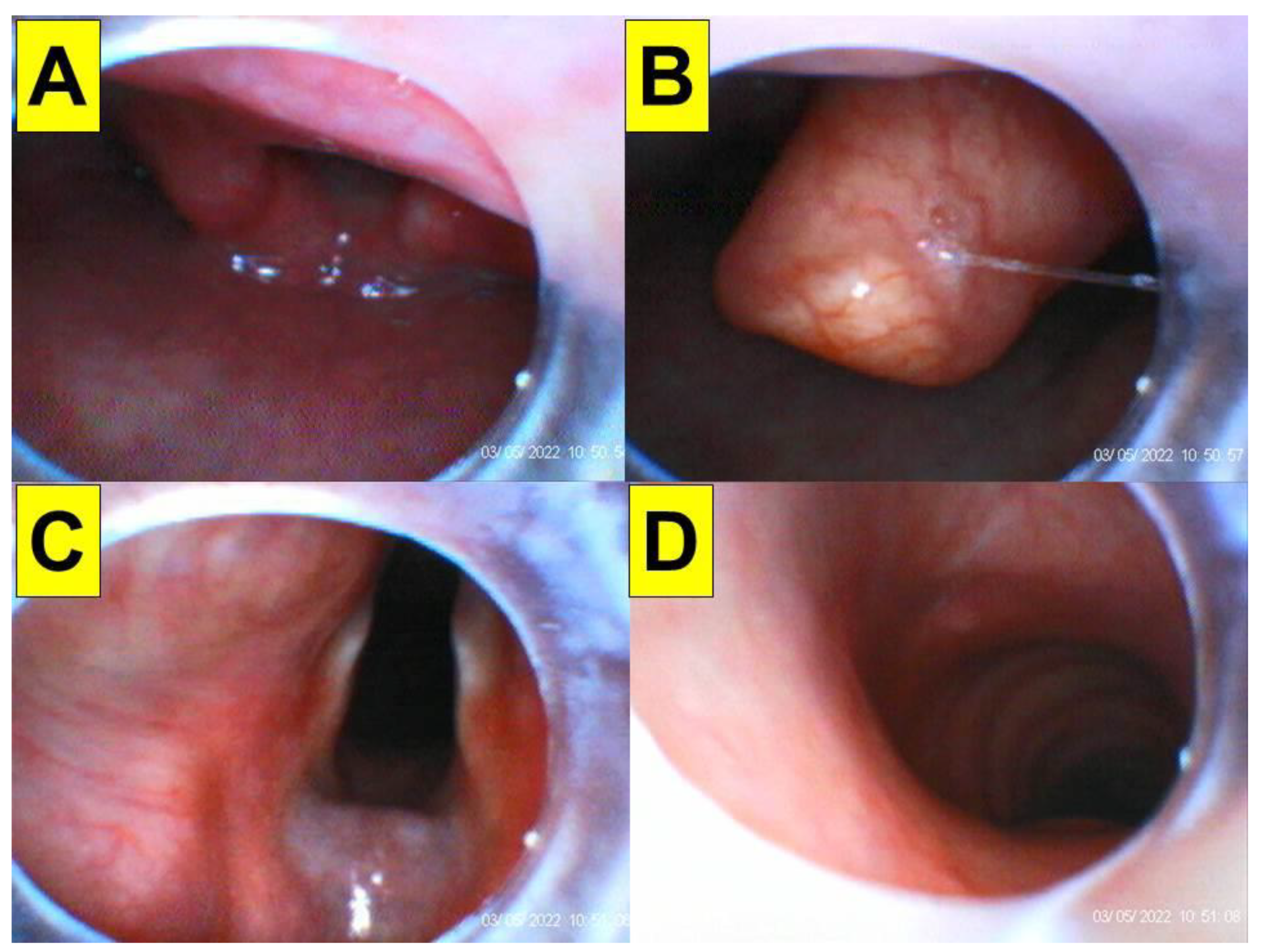
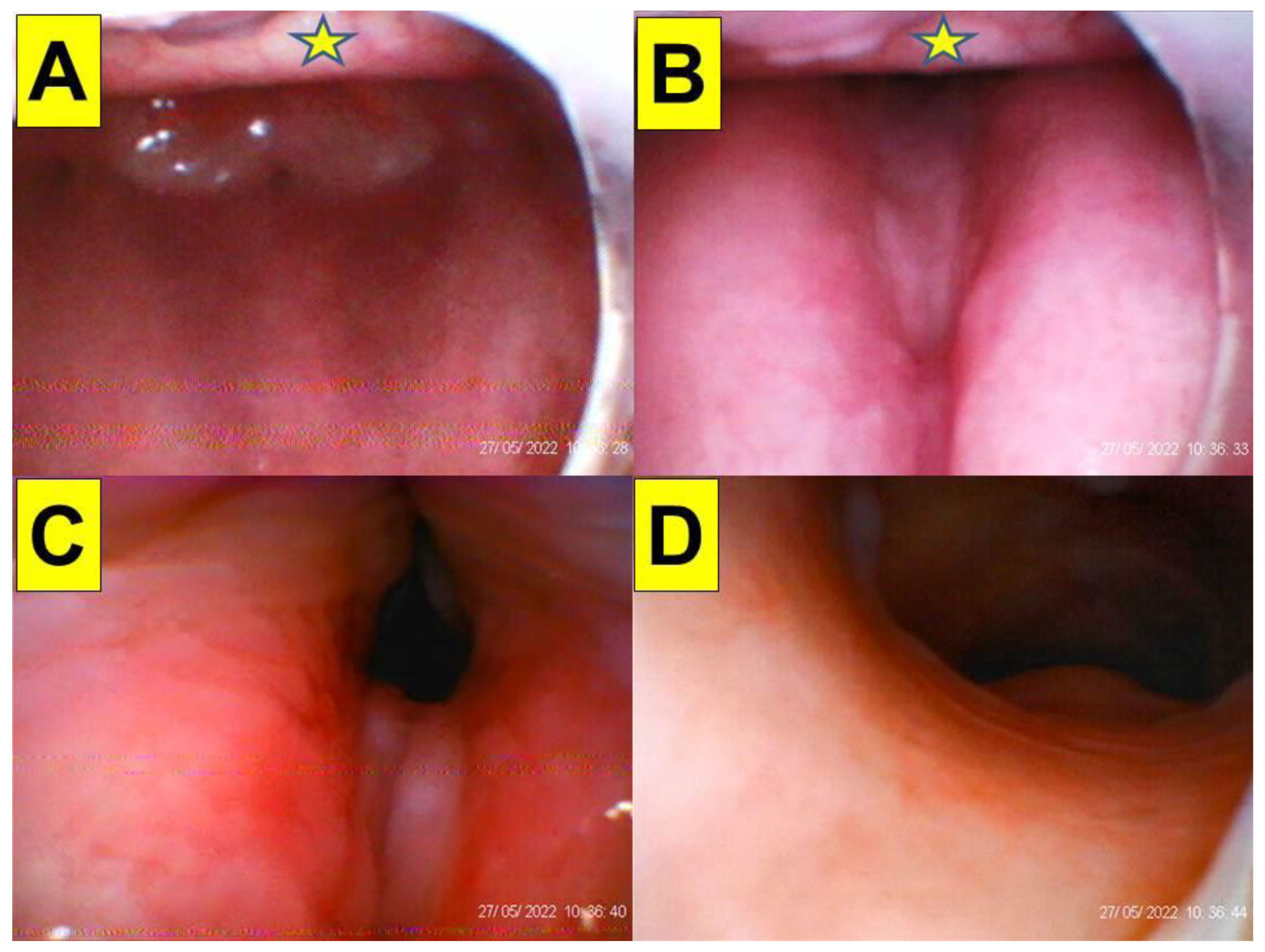
2. Case Presentations
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Austin, N.; Krishnamoorthy, V.; Dagal, A. Airway management in cervical spine injury. Int. J. Crit. Illn. Inj. Sci. 2014, 4, 50–56. [Google Scholar] [CrossRef]
- Law, J.A.; Duggan, L.V.; Asselin, M.; Baker, P.; Crosby, E.; Downey, A.; Hung, O.R.; Kovacs, G.; Lemay, F.; Noppens, R.; et al. Canadian Airway Focus Group updated consensus-based recommendations for management of the difficult airway: Part 2. Planning and implementing safe management of the patient with an anticipated difficult airway. Can. J. Anaesth. 2021, 68, 1405–1436. [Google Scholar] [CrossRef] [PubMed]
- Apfelbaum, J.L.; Hagberg, C.A.; Connis, R.T.; Abdelmalak, B.B.; Agarkar, M.; Dutton, R.P.; Fiadjoe, J.E.; Greif, R.; Klock, P.A.; Mercier, D.; et al. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology 2022, 136, 31–81. [Google Scholar] [CrossRef] [PubMed]
- van Zundert, A.; Stessel, B.; De Ruiter, F.; Giebelen, D.; Weber, E. Video-assisted laryngoscopy: A useful adjunct in endotracheal intubation. Acta Anaesthesiol. Belg. 2007, 58, 129–131. [Google Scholar] [PubMed]
- Vermelis, A.M.; Mateijsen, N.; Giebelen, D.; Meeusen, V.; Wong, D.T.; van Zundert, A.A. Successful use of videolaryngoscopy in an adult patient with acute epiglottitis: A case report. Acta Anaesthesiol. Belg. 2010, 61, 67–70. [Google Scholar] [PubMed]
- Turkstra, T.P.; Pelz, D.M.; Jones, P.M. Cervical spine motion: A fluoroscopic comparison of the AirTraq laryngoscope vs. the Macintosh laryngoscope. Anesthesiology 2009, 111, 97–101. [Google Scholar] [CrossRef]
- Paik, H.; Park, H.P. Randomized crossover trial comparing cervical spine motion during tracheal intubation with a Macintosh laryngoscope vs. a C-MAC D-blade videolaryngoscope in a simulated immobilized cervical spine. BMC Anesthesiol. 2020, 20, 201. [Google Scholar] [CrossRef]
- Saricicek, V.; Mizrak, A.; Gul, R.; Goksu, S.; Cesur, M. GlideScope video laryngoscopy use tracheal intubation in patients with ankylosing spondylitis: A series of four cases and literature review. J. Clin. Monit. Comput. 2014, 28, 169–172. [Google Scholar] [CrossRef]
- Suppan, L.; Tramèr, M.R.; Niquille, M.; Grosgurin, O.; Marti, C. Alternative intubation techniques vs Macintosh laryngoscopy in patients with cervical spine immobilization: Systematic review and meta-analysis of randomized controlled trials. Br. J. Anaesth. 2016, 116, 27–36. [Google Scholar] [CrossRef]
- Singleton, B.N.; Morris, F.K.; Yet, B.; Buggy, D.J.; Perkins, Z.B. Effectiveness of intubation devices in patients with cervical spine immobilisation: A systematic review and network meta-analysis. Br. J. Anaesth. 2021, 126, 1055–1066. [Google Scholar] [CrossRef]
- Kleine-Brueggeney, M.; Greif, R.; Schoettker, P.; Savoldelli, G.L.; Nabecker, S.; Theiler, L.G. Evaluation of six videolaryngoscopes in 720 patients with a simulated difficult airway: A multicentre randomized controlled trial. Br. J. Anaesth. 2016, 116, 670–679. [Google Scholar] [CrossRef]
- Kleine-Brueggeney, M.; Buttenberg, M.; Greif, R.; Nabecker, S.; Theiler, L. Evaluation of three unchannelled videolaryngoscopes and the Macintosh laryngoscope in patients with a simulated difficult airway: A randomised, controlled trial. Anaesthesia 2017, 72, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Kill, C.; Risse, J.; Wallot, P.; Seidl, P.; Steinfeldt, T.; Wulf, H. Videolaryngoscopy with GlideScope reduces cervical spine movement in patients with unsecured cervical spine. J. Emerg. Med. 2013, 44, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Waltl, B.; Melischek, M.; Schuschnig, C.; Kabon, B.; Erlacher, W.; Nasel, C.; Fuchs, M.; Kapral, S. Tracheal intubation and cervical spine excursion: Direct laryngoscopy vs. intubating laryngeal mask. Anaesthesia 2001, 56, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Abramson, S.I.; Holmes, A.A.; Hagberg, C.A. Awake insertion of the Bonfils Retromolar Intubation FiberscopeTM in five patients with anticipated difficult airways. Anesth. Analg. 2008, 106, 1215–1217. [Google Scholar] [CrossRef]
- Rudolph, C.; Schneider, J.P.; Wallenborn, J.; Schaffranietz, L. Movement of the upper cervical spine during laryngoscopy: A comparison of the Bonfils intubation fibrescope and the Macintosh laryngoscope. Anaesthesia 2005, 60, 668–672. [Google Scholar] [CrossRef]
- Wong, D.M.; Prabhu, A.; Chakraborty, S.; Tan, G.; Massicotte, E.M.; Cooper, R. Cervical spine motion during flexible bronchoscopy compared with the Lo-Pro GlideScope®. Br. J. Anaesth. 2009, 102, 424–430. [Google Scholar] [CrossRef]
- Swain, A.; Bhagat, H.; Gupta, V.; Salunke, P.; Panda, N.B.; Sahu, S. Intubating laryngeal mask airway-assisted flexible bronchoscopic intubation is associated with reduced cervical spine motion when compared with C-MAC video laryngoscopy-guided intubation: A prospective randomized cross over Trial. J. Neurosurg. Anesthesiol. 2020, 32, 242–248. [Google Scholar] [CrossRef]
- Agrawal, S.; Salunke, P.; Gupta, S.; Swain, A.; Jangra, K.; Panda, N.; Sahu, S.; Gupta, V.; Bloria, S.; Kataria, K.K.; et al. Fiberoptic bronchoscopy vs. video laryngoscopy guided intubation in patients with craniovertebral junction instability: A cinefluroscopic comparison. Surg. Neurol. Int. 2021, 12, 92. [Google Scholar] [CrossRef]
- Moore, A.; Schricker, T. Awake videolaryngoscopy vs. fiberoptic bronchoscopy. Curr. Opin. Anaesthesiol. 2019, 32, 764–768. [Google Scholar] [CrossRef]
- Alhomary, M.; Ramadan, E.; Curran, E.; Walsh, S.R. Videolaryngoscopy vs. fibreoptic bronchoscopy for awake tracheal intubation: A systematic review and meta-analysis. Anaesthesia 2018, 73, 1151–1161. [Google Scholar] [CrossRef] [PubMed]
- Thong, S.Y.; Wong, T.G. Clinical uses of the Bonfils Retromolar Intubation Fiberscope: A review. Anesth. Analg. 2012, 115, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Hung, O.R.; Pytka, S.; Morris, I.; Murphy, M.; Launcelott, G.; Stevens, S.; MacKay, W.; Stewart, R.D. Clinical trial of a new lightwand device (Trachlight) to intubate the trachea. Anesthesiology 1995, 83, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Shikani, A.H. New “seeing” stylet-scope and method for the management of the difficult airway. Otolaryngol. Head Neck Surg. 1999, 120, 113–116. [Google Scholar] [CrossRef]
- Levitan, R.M. Design rationale and intended use of a short optical stylet for routine fiberoptic augmentation of emergency laryngoscopy. Am. J. Emerg. Med. 2006, 24, 490–495. [Google Scholar] [CrossRef]
- Turkstra, T.P.; Pelz, D.M.; Shaikh, A.A.; Craen, R.A. Cervical spine motion: A fluoroscopic comparison of Shikani Optical Stylet vs. Macintosh laryngoscope. Can. J. Anaesth. 2007, 54, 441–447. [Google Scholar] [CrossRef]
- Luk, H.N.; Yang, Y.L.; Huang, C.H.; Su, I.M.; Tsai, P.B. Application of plastic sheet barrier and video intubating stylet to protect tracheal intubators during Coronavirus Disease 2019 pandemic: A Taiwan experience. Cell Transpl. 2021, 30, 963689720987527. [Google Scholar] [CrossRef]
- Tsai, P.B.; Luk, H.N. Sheet barrier and intubating stylet. Encyclopedia 2021, 1, 1058–1075. [Google Scholar] [CrossRef]
- Yang, C.P.; Luk, H.N.; Qu, J.Z.; Shikani, A. The use of a video-assisted intubating stylet technique in a critically ill and contagious COVID-19 patient. Healthcare 2022, 10, 388. [Google Scholar] [CrossRef]
- Tsay, P.J.; Yang, C.P.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-assisted intubating stylet technique for difficult intubation: A case series report. Healthcare 2022, 10, 741. [Google Scholar] [CrossRef]
- Houde, B.J.; Williams, S.R.; Cadrin-Chênevert, A.; Guilbert, F.; Drolet, P. A comparison of cervical spine motion during orotracheal intubation with the Trachlight® or the flexible fiberoptic bronchoscope. Anesth. Analg. 2009, 108, 1638–1643. [Google Scholar] [CrossRef] [PubMed]
- Turkstra, T.P.; Craen, R.A.; Pelz, D.M.; Gelb, A.W. Cervical spine motion: A fluoroscopic comparison during intubation with lighted stylet, GlideScope, and Macintosh laryngoscope. Anesth. Analg. 2005, 101, 910–915. [Google Scholar] [CrossRef] [PubMed]
- Nam, K.; Lee, Y.; Park, H.P.; Chung, J.; Yoon, H.K.; Kim, T.K. Cervical spine motion during tracheal intubation using an Optiscope vs. the McGrath videolaryngoscope in patients with simulated cervical immobilization: A prospective randomized crossover study. Anesth. Analg. 2019, 129, 1666–1672. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.K.; Lee, H.C.; Park, J.B.; Oh, H.; Park, H.P. McGrath MAC videolaryngoscope vs. Optiscope video stylet for tracheal intubation in patients with manual inline cervical stabilization: A randomized trial. Anesth. Analg. 2020, 130, 870–878. [Google Scholar] [CrossRef]
- Xu, M.; Li, X.X.; Guo, X.Y.; Wang, J. Shikani Optical Stylet vs. Macintosh laryngoscope for intubation in patients undergoing surgery for cervical spondylosis: A randomized controlled trial. Chin. Med. J. 2017, 130, 297–302. [Google Scholar] [CrossRef]
- Mahrous, R.S.S.; Ahmed, A.M.M. The Shikani Optical Stylet as an alternative to awake fiberoptic intubation in patients at risk of secondary cervical spine injury: A randomized controlled trial. J. Neurosurg. Anesthesiol. 2018, 30, 354–358. [Google Scholar] [CrossRef]
- Phua, D.S.; Mah, C.L.; Wang, C.F. The Shikani Optical Stylet as an alternative to the GlideScope® videolaryngoscope in simulated difficult intubations-a randomised controlled trial. Anaesthesia 2012, 67, 402–406. [Google Scholar] [CrossRef]
- Park, J.W.; An, S.; Park, S.; Nahm, F.S.; Han, S.H.; Kim, J.H. Comparison of a new video intubation stylet and McGrath® MAC video laryngoscope for intubation in an airway manikin with normal airway and cervical spine immobilization scenarios by novice personnel: A randomized crossover study. Biomed. Res. Int. 2021, 2021, 4288367. [Google Scholar] [CrossRef]
- Wang, M.; Ding, R.; Li, Z.; He, M.; Liu, C. Comparison of intubation of Shikani optical stylet and Clarus Video Stylet in patients with cervical spine immobilization. J. Pract. Med. 2017, 24, 3933–3936. [Google Scholar]
- Kim, J.K.; Kim, J.A.; Kim, C.S.; Ahn, H.J.; Yang, M.K.; Choi, S.J. Comparison of tracheal intubation with the Airway Scope or Clarus Video System in patients with cervical collars. Anaesthesia 2011, 66, 694–698. [Google Scholar] [CrossRef]
- Hung, K.C.; Chang, Y.J.; Chen, I.W.; Lin, C.M.; Liao, S.W.; Chin, J.C.; Chen, J.Y.; Yew, M.; Sun, C.K. Comparison of video-stylet and video-laryngoscope for endotracheal intubation in adults with cervical neck immobilisation: A meta-analysis of randomised controlled trials. Anaesth. Crit. Care Pain Med. 2021, 40, 100965. [Google Scholar] [CrossRef] [PubMed]
- Osborn, I.P.; Naruse, R.; Ferrario, L. Airway management in neurosurgical patients. In Hagberg and Benumof’s Airway Management, 4th ed.; Chapter 40; Elsevier: Philadelphia, PA, USA, 2018; pp. 717–731. [Google Scholar]
- Spiekermann, B.F.; Stone, D.J.; Bogdonoff, D.L.; Yemen, T.A. Airway management in neuroanaesthesia. Can. J. Anaesth. 1996, 43, 820–834. [Google Scholar] [CrossRef] [PubMed]
- Langeron, O.; Semjen, F.; Bourgain, J.L.; Marsac, A.; Cros, A.M. Comparison of the intubating laryngeal mask airway with the fiberoptic intubation in anticipated difficult airway management. Anesthesiology 2001, 94, 968–972. [Google Scholar] [CrossRef] [PubMed]
- Ferson, D.Z.; Rosenblatt, W.H.; Johansen, M.J.; Osborn, I.; Ovassapian, A. Use of the intubating LMA-FastrachTM in 254 patients with difficult-to-manage airways. Anesthesiology 2001, 95, 1175–1181. [Google Scholar] [CrossRef]
- Tang, W.; Wei, P.; Huang, J.; Zhang, N.; Zhou, H.; Zhou, J.; Zheng, Q.; Li, J.; Wang, Z. Nasotracheal intubation-extubation-intubation and asleep-awake-asleep anesthesia technique for deep brain stimulation. BMC Anesthesiol. 2019, 19, 14. [Google Scholar] [CrossRef]
- Brockerville, M.; Unger, Z.; Rowland, N.C.; Sammartino, F.; Manninen, P.H.; Venkatraghavan, L. Airway management with a stereotactic headframe in situ-A mannequin study. J. Neurosurg. Anesthesiol. 2018, 30, 44–48. [Google Scholar] [CrossRef]
- Dalby, T.; Iorio-Morin, C.; Kalia, S.; Venkatraghavan, L.; Dinsmore, M. Airway management with Leksell frame in situ with or without frontal bar: A mannequin study. Can. J. Neurol. Sci. 2022, 49, 579–582. [Google Scholar] [CrossRef]
- Brimacombe, J.; Keller, C.; Künzel, K.H.; Gaber, O.; Boehler, M.; Pühringer, F. Cervical spine motion during airway management: A cinefluoroscopic study of the posteriorly destabilized third cervical vertebrae in human cadavers. Anesth. Analg. 2000, 91, 1274–1278. [Google Scholar] [CrossRef]
- Holmes, M.G.; Dagal, A.; Feinstein, B.A.; Joffe, A.M. Airway management practice in adults with an unstable cervical spine: The Harborview Medical Center experience. Anesth. Analg. 2018, 127, 450–454. [Google Scholar] [CrossRef]
- Seo, K.H.; Kim, K.M.; John, H.; Jun, J.H.; Han, M.; Kim, S. Comparison of C-MAC D-blade videolaryngoscope and McCoy laryngoscope efficacy for nasotracheal intubation in simulated cervical spinal injury: A prospective randomized comparative study. BMC Anesthesiol. 2020, 20, 114. [Google Scholar] [CrossRef]
- Kuo, Y.M.; Lai, H.Y.; Tan, E.C.; Li, Y.S.; Chiang, T.Y.; Huang, S.S.; Huang, W.C.; Chu, Y.C. Cervical spine immobilization does not interfere with nasotracheal intubation performed using GlideScope videolaryngoscopy: A randomized equivalence trial. Sci. Rep. 2022, 12, 4041. [Google Scholar] [CrossRef] [PubMed]
- Robitaille, A.; Williams, S.R.; Tremblay, M.H.; Guilbert, F.; Thériault, M.; Drolet, P. Cervical spine motion during tracheal intubation with manual in-line stabilization: Direct laryngoscopy vs. GlideScope® videolaryngoscopy. Anesth. Analg. 2008, 106, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, R.; Kamata, K.; Hamada, K.; Sessler, D.I.; Ozaki, M. Airway scope and StyletScope for tracheal intubation in a simulated difficult airway. Anesth. Analg. 2009, 108, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.C.; Lee, J.S.; Lee, Y.W.; Chang, C.H. Comparison of the laryngeal view during intubation using Airtraq and Macintosh laryngoscopes in patients with cervical spine immobilization and mouth opening limitation. Korean J. Anesthesiol. 2010, 59, 314–318. [Google Scholar] [CrossRef]
- Gill, N.; Purohit, S.; Kalra, P.; Lall, T.; Khare, A. Comparison of hemodynamic responses to intubation: Flexible fiberoptic bronchoscope vs. McCoy laryngoscope in presence of rigid cervical collar simulating cervical immobilization for traumatic cervical spine. Anesth. Essays Res. 2015, 9, 337–342. [Google Scholar] [CrossRef]
- Bathory, I.; Frascarolo, P.; Kern, C.; Schoettker, P. Evaluation of the GlideScope® for tracheal intubation in patients with cervical spine immobilisation by a semi-rigid collar. Anaesthesia 2009, 64, 1337–1341. [Google Scholar] [CrossRef]
- Kim, D.H.; Yoo, J.Y.; Ha, S.Y.; Chae, Y.J. Comparison of the paediatric blade of the Pentax-AWS and Ovassapian airway in fibreoptic tracheal intubation in patients with limited mouth opening and cervical spine immobilization by a semi-rigid neck collar: A randomized controlled trial. Br. J. Anaesth. 2017, 119, 993–999. [Google Scholar] [CrossRef]
- Maharaj, C.H.; Buckley, E.; Harte, B.H.; Laffey, J.G. Endotracheal intubation in patients with cervical spine immobilization: A comparison of Macintosh and Airtraq laryngoscopes. Anesthesiology 2007, 107, 53–59. [Google Scholar] [CrossRef]
- McElwain, J.; Laffey, J.G. Comparison of the C-MAC®, Airtraq®, and Macintosh laryngoscopes in patients undergoing tracheal intubation with cervical spine immobilization. Br. J. Anaesth. 2011, 107, 258–264. [Google Scholar] [CrossRef]
- Joseph, J.; Sequeira, T.; Upadya, M. Comparison of the use of McCoy and TruView EVO2 laryngoscopes in patients with cervical spine immobilization. Saudi J. Anaesth. 2012, 6, 248–253. [Google Scholar] [CrossRef]
- Kim, Y.J.; Hur, C.; Yoon, H.K.; Lee, H.C.; Park, H.P.; Oh, H. Effects of external laryngeal manipulation on cervical spine motion during videolaryngoscopic intubation under manual in-line stabilization: A randomized crossover trial. J. Clin. Med. 2021, 10, 2931. [Google Scholar] [CrossRef] [PubMed]
- Vijayakumar, V.; Rao, S.; Shetty, N. A Comparison of Macintosh and Airtraq laryngoscopes for endotracheal intubation in adult patients with cervical spine immobilization using manual in line axial stabilization: A prospective randomized study. J. Neurosurg. Anesthesiol. 2016, 28, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Varshney, P.; Ahmed, S.M.; Siddiqui, O.A.; Nadeem, A.; Ajmal, P.M. A comparative evaluation of Airtraq and Hansraj video laryngoscopes in patients undergoing tracheal intubation with cervical spine immobilization-A randomized prospective study. J. Anaesthesiol. Clin. Pharmacol. 2021, 37, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Liu, E.H.; Goy, R.W.; Tan, B.H.; Asai, T. Tracheal intubation with videolaryngoscopes in patients with cervical spine immobilization: A randomized trial of the Airway Scope® and the GlideScope®. Br. J. Anaesth. 2009, 103, 446–451. [Google Scholar] [CrossRef]
- Sinha, R.; Ray, B.R.; Sharma, A.; Pandey, R.K.; Punj, J.; Darlong, V.; Trikha, A. Comparison of the C-MAC video laryngoscope size 2 Macintosh blade with size 2 C-MAC D-blade for laryngoscopy and endotracheal intubation in children with simulated cervical spine injury: A prospective randomized crossover study. J. Anaesthesiol. Clin. Pharmacol. 2019, 35, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Chandy, J.; Pillai, R.; Mathew, A.; Philip, A.V.; George, S.P.; Sahajanandan, R. A randomized clinical trial comparing the King Vision (channeled blade) and the CMAC (D blade) videolaryngoscopes in patients with cervical spine immobilization. J. Anaesthesiol. Clin. Pharmacol. 2021, 37, 604–609. [Google Scholar] [CrossRef]
- Malik, M.A.; Maharaj, C.H.; Harte, B.H.; Laffey, J.G. Comparison of Macintosh, Truview EVO2®, Glidescope®, and Airwayscope® laryngoscope use in patients with cervical spine immobilization. Br. J. Anaesth. 2008, 101, 723–730. [Google Scholar] [CrossRef]
- Malik, M.A.; Subramaniam, R.; Churasia, S.; Maharaj, C.H.; Harte, B.H.; Laffey, J.G. Tracheal intubation in patients with cervical spine immobilization: A comparison of the Airwayscope®, LMA CTrach®, and the Macintosh laryngoscopes. Br. J. Anaesth. 2009, 102, 654–661. [Google Scholar] [CrossRef]
- Enomoto, Y.; Asai, T.; Arai, T.; Kamishima, K.; Okuda, Y. Pentax-AWS, a new videolaryngoscope, is more effective than the Macintosh laryngoscope for tracheal intubation in patients with restricted neck movements: A randomized comparative study. Br. J. Anaesth. 2008, 100, 544–548. [Google Scholar] [CrossRef]
- Aoi, Y.; Inagawa, G.; Hashimoto, K.; Tashima, H.; Tsuboi, S.; Takahata, T.; Nakamura, K.; Goto, T. Airway scope laryngoscopy under manual inline stabilization and cervical collar immobilization: A crossover in vivo cinefluoroscopic study. J. Trauma 2011, 71, 32–36. [Google Scholar] [CrossRef]
- Yoo, J.Y.; Park, S.Y.; Kim, J.Y.; Kim, M.; Haam, S.J.; Kim, D.H. Comparison of the McGrath videolaryngoscope and the Macintosh laryngoscope for double lumen endobronchial tube intubation in patients with manual in-line stabilization: A randomized controlled trial. Medicine 2018, 97, e0081. [Google Scholar] [CrossRef] [PubMed]
- Roh, G.U.; Kwak, H.J.; Lee, K.C.; Lee, S.Y.; Kim, J.Y. Randomized comparison of McGrath MAC videolaryngoscope, Pentax Airway Scope, and Macintosh direct laryngoscope for nasotracheal intubation in patients with manual in-line stabilization. Can. J. Anaesth. 2019, 66, 1213–1220. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.H.; Cheng, C.P.; Chiu, Y.L.; Hsu, Y.C.; Hu, M.H.; Huang, G.S. Two head positions for orotracheal intubation with the trachway videolight intubating stylet with manual in-line stabilization: A randomized controlled trial. Medicine 2020, 99, e19645. [Google Scholar] [CrossRef] [PubMed]
- Madziala, M.; Smereka, J.; Dabrowski, M.; Leung, S.; Ruetzler, K.; Szarpak, L. A comparison of McGrath MAC® and standard direct laryngoscopy in simulated immobilized cervical spine pediatric intubation: A manikin study. Eur. J. Pediatr. 2017, 176, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.W.; Kim, J.A.; Jung, H.J.; Kim, W.H. Tracheal intubation with a McGrath® Series 5 video laryngoscope by novice personnel in a cervical-immobilized manikin. J. Emerg. Med. 2016, 50, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Smereka, J.; Ladny, J.R.; Naylor, A.; Ruetzler, K.; Szarpak, L. C-MAC compared with direct laryngoscopy for intubation in patients with cervical spine immobilization: A manikin trial. Am. J. Emerg. Med. 2017, 35, 1142–1146. [Google Scholar] [CrossRef] [PubMed]
- Jain, D.; Dhankar, M.; Wig, J.; Jain, A. Comparison of the conventional CMAC and the D-blade CMAC with the direct laryngoscopes in simulated cervical spine injury-a manikin study. Braz. J. Anesthesiol. 2014, 64, 269–274. [Google Scholar] [CrossRef]
- Karczewska, K.; Szarpak, L.; Smereka, J.; Dabrowski, M.; Ladny, J.R.; Wieczorek, W.; Robak, O.; Frass, M.; Ahuja, S.; Ruetzler, K. ET-View compared to direct laryngoscopy in patients with immobilized cervical spine by unexperienced physicians: A randomized crossover manikin trial. Anaesthesiol. Intensive Ther. 2017, 49, 274–282. [Google Scholar] [CrossRef]
- Gawlowski, P.; Smereka, J.; Madziala, M.; Cohen, B.; Ruetzler, K.; Szarpak, L. Comparison of the ETView Single Lumen and Macintosh laryngoscopes for endotracheal intubation in an airway manikin with immobilized cervical spine by novice paramedics: A randomized crossover manikin trial. Medicine 2017, 96, e5873. [Google Scholar] [CrossRef]
- Pius, J.; Noppens, R.R. Learning curve and performance in simulated difficult airway for the novel C-MAC® video-stylet and C-MAC® Macintosh video laryngoscope: A prospective randomized manikin trial. PLoS ONE 2020, 15, e0242154. [Google Scholar] [CrossRef]
- Nair, S.M.; Menon, G.D.; George, M.; Issac, E.; Bhaskaran, R. Comparison of performance characteristics of C-MAC video, McCoy, and Macintosh laryngoscopes in elective cervical spine surgery. J. Anaesthesiol. Clin. Pharmacol. 2021, 37, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Bharti, N.; Arora, S.; Panda, N.B. A comparison of McCoy, TruView, and Macintosh laryngoscopes for tracheal intubation in patients with immobilized cervical spine. Saudi J. Anaesth. 2014, 8, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Desai, D.J. Tracheal intubation with King Vision video laryngoscope in patients with cervical spine instability-Comparison of straight vs. curved reinforced endotracheal tubes. Indian J. Anaesth. 2021, 65, 650–655. [Google Scholar] [CrossRef]
- Shravanalakshmi, D.; Bidkar, P.U.; Narmadalakshmi, K.; Lata, S.; Mishra, S.K.; Adinarayanan, S. Comparison of intubation success and glottic visualization using King Vision and C-MAC videolaryngoscopes in patients with cervical spine injuries with cervical immobilization: A randomized clinical trial. Surg. Neurol. Int. 2017, 8, 19. [Google Scholar] [CrossRef] [PubMed]
- Jakhar, R.; Saigal, D.; Kale, S.; Aggarwal, S. Comparison of videolaryngoscope and intubating laryngeal mask airway for tracheal intubation with manual-in-line stabilization in patients undergoing cervical spine surgery. Anesth. Essays Res. 2020, 14, 485–491. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DL | VL | FOB | VS | |
|---|---|---|---|---|
| Using a rigid cervical collar to simulate a difficult airway in patients | ||||
| Koh [55] | − | + | ||
| Gill [56] | − | + | ||
| Paik [7] | − | + | ||
| Kleine-Brueggeney [11] | + | |||
| Kleine-Brueggeney [12] | − | + | ||
| Bathory [57] | − | + | ||
| Seo [51] | − | + | ||
| Kim [58] | + | |||
| Nam [33] | − | + | ||
| Phua [37] | − | + | ||
| Kim [40] | − | + | ||
| Using manual in-line axial cervical spine stabilization to simulate a difficult airway in patients | ||||
| Turkstra [6] | − | + | ||
| Maharaj [59] | − | + | ||
| Houde [31] | + | + | ||
| McElwain [60] | − | + | ||
| Joseph [61] | − | + | ||
| Kim [62] | + | |||
| Robitaille [53] | − | + | ||
| Vijayakumar [63] | − | + | ||
| Varshney [64] | + | |||
| Liu [65] | + | |||
| Sinha [66] | + | |||
| Chandy [67] | + | |||
| Malik [68] | − | + | ||
| Malik [69] | − | + | ||
| Enomoto [70] | − | + | ||
| Aoi [71] | + | |||
| Yoo [72] | − | + | ||
| Roh [73] | − | + | ||
| Chan [74] | + | |||
| Turkstra [32] | − | + | ||
| Using a rigid cervical collar/manual in-line stabilization to simulate a difficult airway in mannequins | ||||
| Park [38] | − | + | ||
| Madziala [75] | − | + | ||
| Choi [76] | − | + | ||
| Smereka [77] | − | + | ||
| Jain [78] | − | + | ||
| Karczewska [79] | − | + | ||
| Gawlowski [80] | − | + | ||
| Pius [81] | − | + | ||
| Cervical spines injuries patients in the real world | ||||
| Yoon [34] | + | − | ||
| Xu [35] | − | + | ||
| Mahrous [36] | + | + | ||
| Wang [39] | + | |||
| Nair [82] | − | + | ||
| Bharti [83] | − | + | ||
| Patel [84] | + | |||
| Shravanalakshmi [85] | + | |||
| Jakhar [86] | + | |||
| Kuo [52] | + | |||
| Shih [this paper] | + | |||
| DL | VL | SGD | FOB (Awake) | VS | |
|---|---|---|---|---|---|
| Need patient’s cooperation | − | − | − | + | − |
| Allow neurologic exam before/after intubation | − | − | − | + | − |
| Require wide mouth opening | + | + | − | − | − |
| Possible difficult laryngoscopy | + | + | − | − | − |
| Always better laryngeal visualization | − | + | − | + | + |
| Operator’s skill/experience demanded | + | − | − | + | − |
| High first-attempt success rate | − | + | + | + | + |
| High overall success rate | − | + | + | + | + |
| Fast intubation/easiness | − | + | + | − | + |
| Blood/secretion may obscure the camera view, and suction is required | − | + | − | + | + |
| Often require an adjunctive tool (e.g., GEB) | + | + | − | − | − |
| Jaw-thrust is a helpful maneuver | − | − | − | − | + |
| Dental/soft tissue injuries | + | + | − | − | − |
| Autonomic stimulation | + | + | − | − | − |
| Risk of pulmonary aspiration under RSI | + | + | + | − | + |
| Availability/affordability | + | − | + | − | − |
| For routine use | + | + | − | + | + |
| Speedy preparedness, easy maintenance | + | + | + | − | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shih, T.-L.; Koay, K.-P.; Hu, C.-Y.; Luk, H.-N.; Qu, J.Z.; Shikani, A. The Use of the Shikani Video-Assisted Intubating Stylet Technique in Patients with Restricted Neck Mobility. Healthcare 2022, 10, 1688. https://doi.org/10.3390/healthcare10091688
Shih T-L, Koay K-P, Hu C-Y, Luk H-N, Qu JZ, Shikani A. The Use of the Shikani Video-Assisted Intubating Stylet Technique in Patients with Restricted Neck Mobility. Healthcare. 2022; 10(9):1688. https://doi.org/10.3390/healthcare10091688
Chicago/Turabian StyleShih, Tung-Lin, Ker-Ping Koay, Ching-Yuan Hu, Hsiang-Ning Luk, Jason Zhensheng Qu, and Alan Shikani. 2022. "The Use of the Shikani Video-Assisted Intubating Stylet Technique in Patients with Restricted Neck Mobility" Healthcare 10, no. 9: 1688. https://doi.org/10.3390/healthcare10091688