Extremity Exercise Program in Breast Cancer Survivors Suffering from Chemotherapy-Induced Peripheral Neuropathy: A Feasibility Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Extremity Exercise Program
2.3. Sample Size Calculation
2.4. Outcome Measures
2.4.1. Safety and Feasibility
2.4.2. Clinician-Assessed CIPN
2.4.3. Participant-Reported CIPN
3. Data Analysis
4. Results
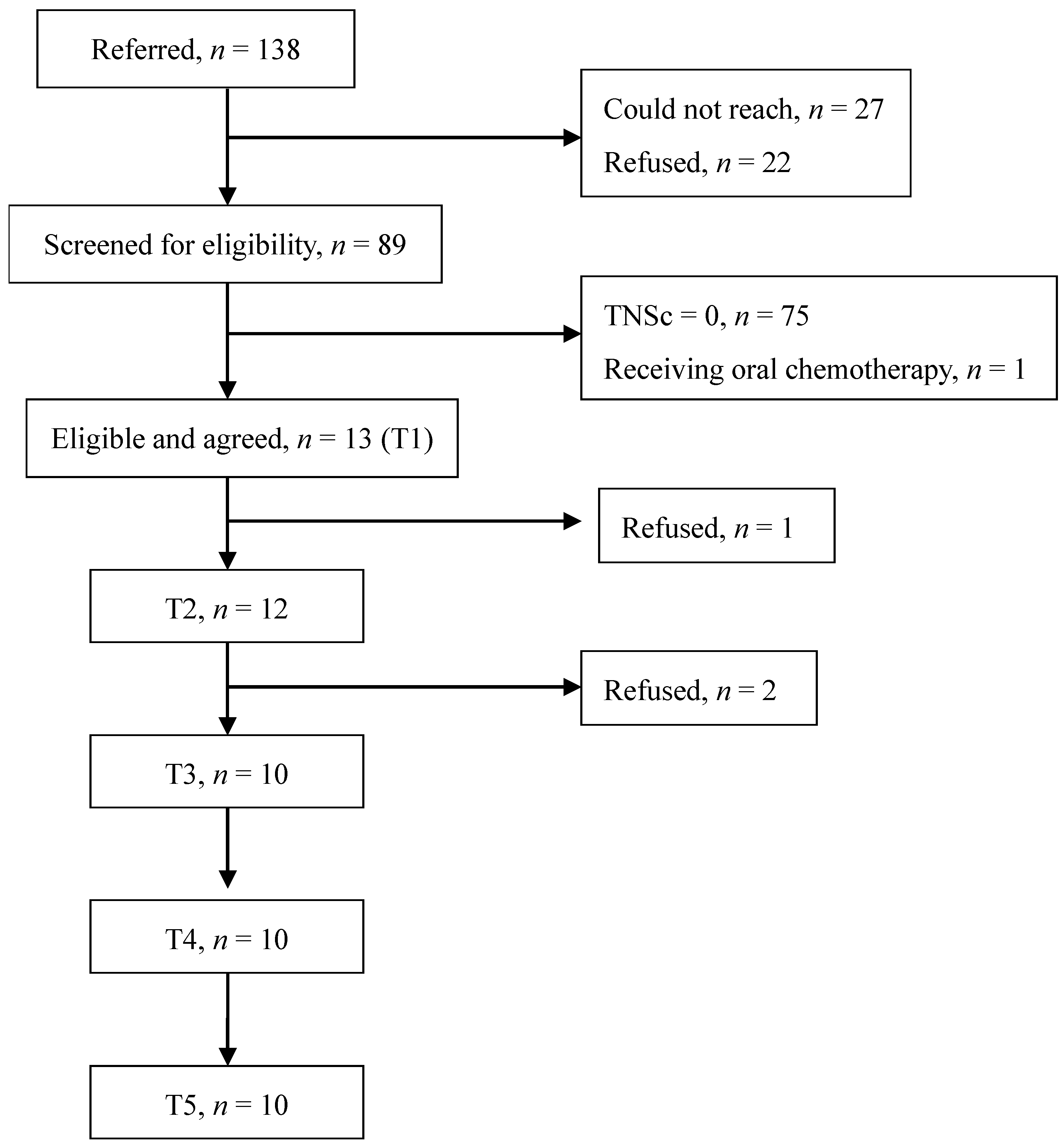
4.1. Recruitment and Follow-Up
4.2. Sample Characteristics, Safety, Adherence, and Retention
4.3. Participant Experience
4.4. Clinician-Assessed and Patient-Reported CIPN
5. Discussion
5.1. Strengths and Weaknesses
5.2. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Administration, Ministry of Health and Welfare. Cancer Registry Annual Report 2020. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=269&pid=13498 (accessed on 20 July 2021).
- Zajączkowska, R.; Kocot-Kępska, M.; Leppert, W.; Wrzosek, A.; Mika, J.; Wordliczek, J. Mechanisms of Chemotherapy-Induced Peripheral Neuropathy. Int. J. Mol. Sci. 2019, 20, 1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.J.; Chan, Y.N.; Jheng, Y.W.; Wu, C.J.; Lin, M.W.; Tseng, L.M.; Tsai, Y.F.; Liu, L.C. Chemotherapy-induced Peripheral Neuropathy in Newly Diagnosed Breast Cancer Survivors Treated with Taxane: A Prospective Longitudinal Study. Support Care Cancer 2021, 29, 2959–2971. [Google Scholar] [CrossRef] [PubMed]
- Rivera, D.R.; Ganz, P.A.; Weyrich, M.S.; Bandos, H.; Melnikow, J. Chemotherapy-Associated Peripheral Neuropathy in Patients With Early-Stage Breast Cancer: A Systematic Review. J. Natl. Cancer Inst. 2018, 110, djx140. [Google Scholar] [CrossRef] [Green Version]
- Flatters, S.J.L.; Dougherty, P.M.; Colvin, L.A. Clinical and Preclinical Perspectives on Chemotherapy-Induced Peripheral Neuropathy (CIPN): A Narrative Review. BJA Br. J. Anaesth. 2017, 119, 737–749. [Google Scholar] [CrossRef] [Green Version]
- McNeish, B.L.; Richardson, J.K.; Whitney, D.G. Chemotherapy Induced Peripheral Neuropathy Onset Increases the Early Risk for Depression and Anxiety in Breast Cancer Survivors. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Monfort, S.M.; Pan, X.; Patrick, R.; Ramaswamy, B.; Wesolowski, R.; Naughton, M.J.; Loprinzi, C.L.; Chaudhari, A.M.; Lustberg, M.B. Gait, Balance, and Patient-reported Outcomes During Taxane-based Chemotherapy in Early-stage Breast Cancer Patients. Breast Cancer Res. Treat. 2017, 164, 69–77. [Google Scholar] [CrossRef]
- Chan, Y.N.; Jheng, Y.W.; Wang, Y.J. Chemotherapy-induced Peripheral Neurotoxicity as a Risk Factor for Poor Sleep Quality in Breast Cancer Survivors Treated with Docetaxel. Asia Pac. J. Oncol. Nurs. 2021, 8, 68. [Google Scholar] [CrossRef]
- Bonhof, C.; Trompetter, H.; Vreugdenhil, G.; van de Poll-Franse, L.; Mols, F. Painful and Non-painful Chemotherapy-induced Peripheral Neuropathy and Quality of Life in Colorectal Cancer Survivors: Results from the Population-based PROFILES Registry. Supportive Care Cancer 2020, 28, 5933–5941. [Google Scholar] [CrossRef]
- Loprinzi, C.L.; Lacchetti, C.; Bleeker, J.; Cavaletti, G.; Chauhan, C.; Hertz, D.L.; Kelley, M.R.; Lavino, A.; Lustberg, M.B.; Paice, J.A.; et al. Prevention and Management of Chemotherapy-Induced Peripheral Neuropathy in Survivors of Adult Cancers: ASCO Guideline Update. J. Clin. Oncol. 2020, 38, 3325–3348. [Google Scholar] [CrossRef]
- Li, Y.; Lustberg, M.B.; Hu, S. Emerging Pharmacological and Non-Pharmacological Therapeutics for Prevention and Treatment of Chemotherapy-Induced Peripheral Neuropathy. Cancers 2021, 13, 766. [Google Scholar] [CrossRef] [PubMed]
- Tofthagen, C.; Visovsky, C.; Berry, D.L. Strength and Balance Training for Adults with Peripheral Neuropathy and High Risk of Fall: Current Evidence and Implications for Future Research. Oncol. Nurs. Forum 2012, 39, E416–E424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanay, M.A.L.; Armes, J.; Moss-Morris, R.; Rafferty, A.M.; Robert, G. A Systematic Review of Behavioural and Exercise Interventions for the Prevention and Management of Chemotherapy-induced Peripheral Neuropathy Symptoms. J. Cancer Surviv. 2021, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Kaohsiung Municipan Chinese Medical Hospital. Simple and Health Ten Skilled Hand Exercise. Available online: https://orgws.kcg.gov.tw/001/KcgOrgUploadFiles/UserFiles/%E5%81%A5%E5%BA%B7%E5%8D%81%E5%B7%A7.pdf (accessed on 18 November 2015).
- Wisham, L.H.; Abramson, A.S.; Ebel, A. Value of Exercise in Peripheral Arterial Disease. JAMA J. Am. Med. Assoc. 1953, 153, 10–12. [Google Scholar] [CrossRef]
- Radhika, J.; Poomalai, G.; Nalini, S.; Revathi, R. Effectiveness of Buerger-Allen Exercise on Lower Extremity Perfusion and Peripheral Neuropathy Symptoms Among Patients with Diabetes Mellitus. Iran J. Nurs. Midwifery Res. 2020, 25, 291. [Google Scholar] [CrossRef]
- Von Ah, D.; Brown, C.G.; Brown, S.J.; Bryant, A.L.; Davies, M.; Dodd, M.; Ferrell, B.; Hammer, M.; Knobf, M.T.; Knoop, T.J. Research Agenda of the Oncology Nursing Society: 2019–2022. Oncol. Nurs. Forum 2019, 46, 654–669. [Google Scholar] [CrossRef]
- Sim, J. Should Treatment Effects be Estimated in Pilot and Feasibility Studies? Pilot Feasibility Stud. 2019, 5, 107. [Google Scholar] [CrossRef]
- Cavaletti, G.; Jann, S.; Pace, A.; Plasmati, R.; Siciliano, G.; Briani, C.; Cocito, D.; Padua, L.; Ghiglione, E.; Manicone, M. Multi-center Assessment of the Total Neuropathy Score for Chemotherapy-induced Peripheral Neurotoxicity. J. Peripher. Nerv. Syst. 2006, 11, 135–141. [Google Scholar] [CrossRef]
- Cavaletti, G.; Cornblath, D.; Merkies, I.; Postma, T.; Rossi, E.; Frigeni, B.; Alberti, P.; Bruna, J.; Velasco, R.; Argyriou, A. The Chemotherapy-induced Peripheral Neuropathy Outcome Measures Standardization Study: From Consensus to the First Validity and Reliability Findings. Ann. Oncol. 2013, 24, 454–462. [Google Scholar] [CrossRef]
- Chan, Y.N.; Jheng, Y.W.; Wang, P.J.; Chen, C.Y.; Lin, M.W.; Wang, Y.J. Taxane-Induced Peripheral Neuropathy: Objective and Subjective Comparison Between Paclitaxel and Docetaxel in Patients with Breast Cancer. Clin. J. Oncol. Nurs. 2019, 23, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Weimer, L.H.; Wang, A.; Kranwinkel, G.; Brafman, L.; Fuentes, D.; Awad, D.; Crew, K.D. Association Between Patient Reported Outcomes and Quantitative Sensory Tests for Measuring Long-term Neurotoxicity in Breast Cancer Survivors Treated with Adjuvant Paclitaxel Chemotherapy. Breast Cancer Res. Treat. 2011, 125, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Zanville, N.R.; Nudelman, K.N.; Smith, D.J.; Von Ah, D.; McDonald, B.C.; Champion, V.L.; Saykin, A.J. Evaluating the Impact of Chemotherapy-induced Peripheral Neuropathy Symptoms (CIPN-sx) on Perceived Ability to Work in Breast Cancer Survivors during the Frrst Year Post-treatment. Supportive Care Cancer 2016, 24, 4779–4789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portenoy, R.; for the ID Pain Steering Committee. Development and Testing of a Neuropathic Pain Screening Questionnaire: ID Pain. Curr. Med. Res. Opin. 2006, 22, 1555–1565. [Google Scholar] [CrossRef]
- Chan, A.; Wong, S.; Chen, P.; Tsoi, T.; Lam, J.; Ip, W.; Wong, C.; Wong, L.; Mok, V. Validation Study of the Chinese Identification Pain Questionnaire for Neuropathic Pain. Hong Kong Med. J. 2011, 17, 297–300. [Google Scholar]
- Wilkie, D.; Lovejoy, N.; Dodd, M.; Tesler, M. Cancer Pain Intensity Measurement: Concurrent Validity of Three Tools—Finger Dynamometer, Pain Intensity Number Scale, Visual Analogue Scale. Hosp. J. 1990, 6, 1–13. [Google Scholar] [CrossRef]
- Jensen, M.P. The Validity and Reliability of Pain Measures in Adults with Cancer. J. Pain 2003, 4, 2–21. [Google Scholar] [CrossRef]
- Bowen, D.J.; Kreuter, M.; Spring, B.; Cofta-Woerpel, L.; Linnan, L.; Weiner, D.; Bakken, S.; Kaplan, C.P.; Squiers, L.; Fabrizio, C. How We Design Feasibility Studies. Am. J. Prev. Med. 2009, 36, 452–457. [Google Scholar] [CrossRef] [Green Version]
- Cavaletti, G.; Cornblath, D.R.; Merkies, I.S.; Postma, T.J.; Rossi, E.; Alberti, P.; Gonzalez, C.D.; Bruna, J.; Argyriou, A.A.; Briani, C.; et al. Patients’ and physicians’ interpretation of chemotherapy-induced peripheral neurotoxicity. J. Peripher. Nerv. Syst. 2019, 24, 111–119. [Google Scholar] [CrossRef] [Green Version]
- Seretny, M.; Currie, G.L.; Sena, E.S.; Ramnarine, S.; Grant, R.; MacLeod, M.R.; Colvin, L.A.; Fallon, M. Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Pain 2014, 155, 2461–2470. [Google Scholar] [CrossRef] [Green Version]
- Kanzawa-Lee, G.A.; Larson, J.L.; Resnicow, K.; Smith, E.M.L. Exercise Effects on Chemotherapy-induced Peripheral Neuropathy: A Comprehensive Integrative Review. Cancer Nurs. 2020, 43, E172–E185. [Google Scholar] [CrossRef] [PubMed]
- Ganz, P.A.; Land, S.R.; Antonio, C.; Zheng, P.; Yothers, G.; Petersen, L.; Wickerham, D.L.; Wolmark, N.; Ko, C.Y. Cancer Survivorship Research: The Challenge of Recruiting Adult Long Term Cancer Survivors from a Cooperative Clinical Trials Group. J. Cancer Surviv. 2009, 3, 137–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleckner, I.R.; Kamen, C.; Gewandter, J.S.; Mohile, N.A.; Heckler, C.E.; Culakova, E.; Fung, C.; Janelsins, M.C.; Asare, M.; Lin, P.-J. Effects of Exercise During Chemotherapy on Chemotherapy-induced Peripheral Neuropathy: A Multicenter, Randomized Controlled Trial. Supportive Care Cancer 2018, 26, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Bao, T.; Zhi, I.; Baser, R.; Hooper, M.; Chen, C.; Piulson, L.; Li, Q.S.; Galantino, M.L.; Blinder, V.; Robson, M. Yoga for Chemotherapy-induced Peripheral Neuropathy and Fall Risk: A Randomized Controlled Trial. JNCI Cancer Spectr. 2020, 4, pkaa048. [Google Scholar] [CrossRef]
- Hatlevoll, I.; Oldervoll, L.M.; Wibe, A.; Stene, G.; Stafne, S.N.; Hofsli, E. Physical Exercise During Adjuvant Chemotherapy for Colorectal Cancer—A Non-randomized Feasibility Study. Supportive Care Cancer 2021, 29, 2993–3008. [Google Scholar] [CrossRef]
- McCrary, J.M.; Goldstein, D.; Sandler, C.X.; Barry, B.K.; Marthick, M.; Timmins, H.C.; Li, T.; Horvath, L.; Grimison, P.; Park, S.B. Exercise-based Rehabilitation for Cancer Survivors with Chemotherapy-induced Peripheral Neuropathy. Supportive Care Cancer 2019, 27, 3849–3857. [Google Scholar] [CrossRef] [PubMed]
- Berthelot, J.-M.; Nizard, J.; Maugars, Y. The Negative Hawthorne Effect: Explaining Pain Overexpression. Jt. Bone Spine 2019, 86, 445–449. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Mean, SD | n | % |
|---|---|---|---|
| Age (42~65 years) | 50.08, 5.79 | ||
| BMI (18.8~29.7 kg/m2) | 24.78, 3.50 | ||
| Length since diagnosis (9.1~37.9 months) | 24.11, 8.97 | ||
| Marital status | |||
| Single | 2 | 15.4 | |
| Married | 11 | 84.6 | |
| Children | |||
| No | 2 | 15.4 | |
| Yes | 11 | 84.6 | |
| Education level | |||
| High school | 2 | 15.4 | |
| College and above | 11 | 84.6 | |
| Working status | |||
| Not working | 6 | 46.2 | |
| Full time | 6 | 46.2 | |
| Part time | 1 | 7.7 | |
| Household income | |||
| Below average | 11 | 84.6 | |
| Above average | 2 | 14.4 | |
| Religion belief | |||
| Non | 1 | 7.7 | |
| Yes | 12 | 92.3 | |
| Menopausal status | |||
| Pre- | 1 | 7.7 | |
| Post- | 12 | 92.3 | |
| Comorbidity | |||
| Non | 9 | 69.2 | |
| Yes | 4 | 30.8 | |
| Family history of cancer | |||
| No | 7 | 53.8 | |
| Yes | 6 | 46.2 | |
| Regular exercise | |||
| No | 1 | 7.7 | |
| Yes | 12 | 92.3 | |
| Experience of fall | |||
| No | 10 | 76.9 | |
| Yes | 3 | 23.1 | |
| Cancer stage | |||
| I | 2 | 15.4 | |
| II | 2 | 15.4 | |
| III | 5 | 38.4 | |
| Unknown | 4 | 30.8 | |
| Node status | |||
| Negative | 7 | 53.8 | |
| Positive | 6 | 46.2 | |
| Gene-subtypes | |||
| Triple negative | 5 | 38.4 | |
| Her-2+, ER+ | 4 | 30.8 | |
| Her-2+, ER− | 1 | 7.7 | |
| Her-2−, ER+ | 3 | 23.1 | |
| Surgery | |||
| BCS | 8 | 61.5 | |
| Total mastectomy | 5 | 38.5 |
| Aspects | Quotations from Participant’s Feedback |
|---|---|
| Acceptability | “This exercise program is easy to perform. I feel confident to do it.” “I believe that I will keep doing this exercise even after the four-week intervention. It’s really helpful that I even want to do it more.” “I feel comfortable and relaxed when doing Ten Skilled Hand Exercise outdoors or during commuting to work.” |
| Demand | “This is what I really needed to ease my CIPN symptoms.” “It is easy for me to do and does relieve my pain in extremity.” “The Ten Skilled Hand Exercise is exactly suitable for me to manage my numb fingers.” |
| Implementation | “It is hard for me to achieve the exercise goal because I had to work on weekdays.” “I have to sit on the bar table to do Burger Allen Exercise because my bed is too low to do this. It is inconvenient and complicate to do Burger Allen Exercise because I have to move from bed to bar table and back to bed.” “Due to the complexity of this exercise program, I have to do it with an iPad or on a television.” |
| Practicality | “After doing this exercise for one week, I feel my CIPN symptoms improved.” “When I do this extremity exercise program, I can feel the blood flow is going to the extremities. After doing the program, I can really feel the CIPN symptoms improved.” “I can feel the numbness is improving, thanks to this extremity exercise program. It is practical and takes no effort to perform.” “I do really experience the benefit of the exercise and want to do more Ten Skilled Hand Exercise and some more movements in toes of Burger Allen exercise during commuting to work or home.” |
| Measure | T1 (n = 13) | T2 (n = 12) | T3 (n = 10) | T4 (n = 10) | T5 (n = 10) |
|---|---|---|---|---|---|
| Variable Score | Mean, SD | Mean, SD | Mean, SD | Mean, SD | Mean, SD |
| TNSc | 5.23, 3.06 | 6.67, 2.23 | 4.80, 2.78 | 4.70, 3.77 | 4.30, 3.65 |
| Sensory CIPN | 3.92, 2.87 | 5.08, 1.44 | 3.20, 1.93 | 3.80, 3.05 | 3.40, 3.13 |
| Motor CIPN | 1.31, 1.25 | 1.58, 1.38 | 1.40, 1.26 | 0.90, 0.99 | 0.80, 1.03 |
| Autonomic CIPN | 0, 0 | 0, 0 | 0.20, 0.63 | 0, 0 | 1.00, 0.32 |
| Sensory symptoms | 0.54, 0.78 | 0.92, 1.08 | 0.10, 0.32 | 0.30, 0.68 | 0.10, 0.32 |
| Motor symptoms | 0, 0 | 0.08, 0.29 | 0.20, 0.42 | 0.11, 0.33 | 0.10, 0.32 |
| Pin sensitivity | 2.08, 1.50 | 2.58, 1.38 | 1.50, 1.51 | 2.00, 1.89 | 1.90, 1.91 |
| Vibration sensitivity | 1.31, 1.55 | 1.58, 1.44 | 1.60, 1.71 | 1.50, 1.65 | 1.40, 1.71 |
| Muscle strength | 0.23, 0.60 | 0.17, 0.39 | 0.20, 0.42 | 0.10, 0.32 | 0, 0 |
| DTR | 1.08, 1.19 | 1.33, 1.30 | 1.00, 1.16 | 0.70, 0.95 | 0.70, 0.95 |
| NTX-13 | 40.00, 6.58 | 39.67, 6.67 | 43.10, 8.60 | 44.78, 6.22 | 45.56, 6.31 |
| ID-pain | 1.00, 1.47 | 0.92, 1.38 | 0.40, 1.65 | −0.10, 1.29 | −0.22, 1.30 |
| Pain VAS | 30.19, 29.76 | 15.46, 29.45 | 15.56, 27.89 | 13.89, 24.47 | 3.89, 11.67 |
| TNSc | Sensory CIPN | Motor CIPN | NTX−13 | ID−pain | Pain VAS | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | Wald X2 | B | SE | Wald X2 | B | SE | Wald X2 | B | SE | Wald X2 | B | SE | Wald X2 | B | SE | Wald X2 | |
| Intercept | 5.23 | 0.82 | 40.36 *** | 3.92 | 0.68 | 33.61 *** | 1.31 | 0.32 | 16.85 *** | 40.00 | 1.75 | 43.44 *** | 1.00 | 0.38 | 7.04 ** | 30.18 | 7.41 | 16.57 *** |
| T5 | −0.93 | 1.25 | 0.56 | −0.52 | 1.03 | 0.26 | −0.51 | 0.48 | 1.10 | 4.50 | 1.28 | 12.31 *** | −1.22 | 0.59 | 4.30 * | −26.29 | 11.05 | 5.67 * |
| T4 | −0.53 | 1.25 | 0.18 | −0.12 | 1.03 | 0.01 | −0.41 | 0.48 | 0.71 | 3.72 | 0.86 | 18.82 *** | −1.10 | 0.57 | 3.70 | −16.29 | 11.05 | 2.17 |
| T3 | −0.43 | 1.25 | 0.12 | −0.72 | 1.03 | 0.50 | 0.09 | 0.48 | 0.04 | 2.47 | 1.46 | 2.88 | −0.60 | 0.57 | 1.10 | −14.63 | 11.05 | 1.75 |
| T2 | 1.44 | 1.19 | 1.46 | 1.17 | 0.98 | 1.41 | 0.28 | 0.46 | 0.36 | −0.26 | 1.23 | 0.05 | −0.08 | 0.54 | 0.02 | −14.73 | 10.45 | 1.97 |
| T1 | 0 | 0 | 0 | 0 | 0 | 0 | ||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-J.; Chan, Y.-N.; Yen, L.-Y.; Chen, Y.-H.; Lo, C.; Tseng, L.-M.; Wang, Y.-J. Extremity Exercise Program in Breast Cancer Survivors Suffering from Chemotherapy-Induced Peripheral Neuropathy: A Feasibility Pilot Study. Healthcare 2022, 10, 688. https://doi.org/10.3390/healthcare10040688
Wu C-J, Chan Y-N, Yen L-Y, Chen Y-H, Lo C, Tseng L-M, Wang Y-J. Extremity Exercise Program in Breast Cancer Survivors Suffering from Chemotherapy-Induced Peripheral Neuropathy: A Feasibility Pilot Study. Healthcare. 2022; 10(4):688. https://doi.org/10.3390/healthcare10040688
Chicago/Turabian StyleWu, Chih-Jung, Ya-Ning Chan, Li-Yu Yen, Yun-Hen Chen, Chyi Lo, Ling-Ming Tseng, and Ya-Jung Wang. 2022. "Extremity Exercise Program in Breast Cancer Survivors Suffering from Chemotherapy-Induced Peripheral Neuropathy: A Feasibility Pilot Study" Healthcare 10, no. 4: 688. https://doi.org/10.3390/healthcare10040688