
Association between Social Support and Physical Activity in Patients with Coronary Artery Disease: Multiple Mediating Roles of Self-Efficacy and Autonomous Motivation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Ethical Considerations
2.3. Instruments
2.3.1. Sociodemographic and Clinical Characteristics
2.3.2. Social Support
2.3.3. Self-Efficacy
2.3.4. Autonomous Motivation
2.3.5. Physical Activity
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Patients’ Sociodemographic and Clinical Characteristics
3.2. Relationship between Social Support, Self-Efficacy, Autonomous Motivation, and Physical Activity in Patients with CAD
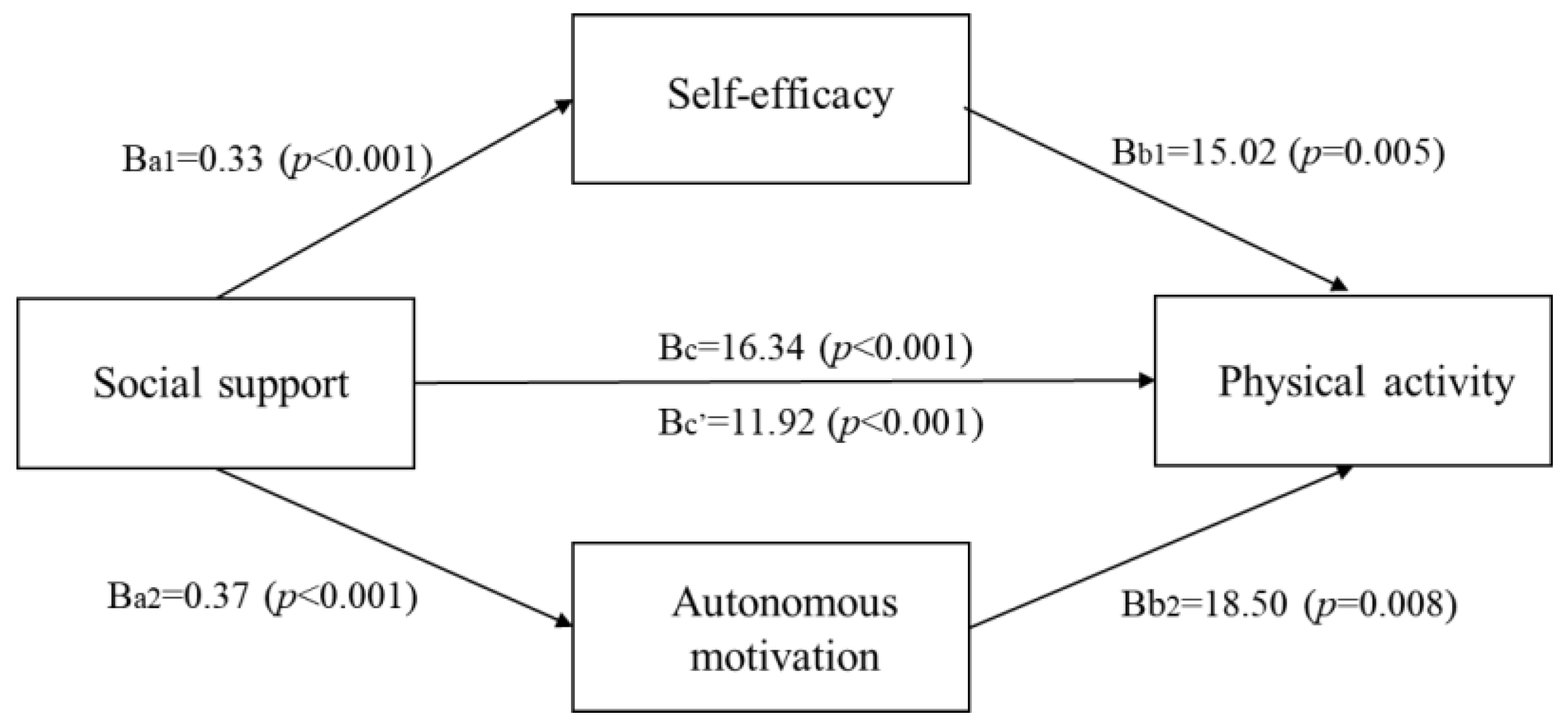
3.3. Multiple Mediating Effects of Self-Efficacy and Autonomous Motivation on the Relationship between Social Support and Physical Activity in Patients with CAD
3.4. Direct and Indirect Effects on Physical Activity in Patients with CAD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ralapanawa, U.; Sivakanesan, R. Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: A narrative review. J. Epidemiol. Glob. Health 2021, 11, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Hashim, M.J.; Mustafa, H.; Baniyas, M.Y.; Al Suwaidi, S.K.B.M.; Al Katheeri, R.; Lootah, S.N.A.H. Global epidemiology of ischemic heart disease: Results from the global burden of disease study. Cureus 2020, 12, e9349. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Service. Press Release on the Health Insurance Treatment Status for Ischemic Heart Disease from 2015 to 2019. Available online: https://www.nhis.or.kr/nhis/together/wbhaea01600m01.do?mode=view&articleNo=10805661 (accessed on 6 October 2021).
- Statistics Korea. 2019 Annual Report on the Cause of Death Statistics. Available online: http://kostat.go.kr/portal/korea/kor_nw/1/6/2/index.board?bmode=read&bSeq=&aSeq=403046&pageNo=1&rowNum=0&navCount=10&currPg=&searchInfo=&sTarget=title&sTxt= (accessed on 6 October 2021).
- Members, W.C.; Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Zwischenberger, B.A. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e21–e129. [Google Scholar]
- Dai, W.; Long, J.; Cheng, Y.; Chen, Y.; Zhao, S. Elevated plasma lipoprotein (a) levels were associated with increased risk of cardiovascular events in Chinese patients with stable coronary artery disease. Sci. Rep. 2018, 8, 7726. [Google Scholar] [CrossRef] [Green Version]
- Lear, S.A.; Hu, W.; Rangarajan, S.; Gasevic, D.; Leong, D.; Iqbal, R.; Yusuf, S. The effect of physical activity on mortality and cardiovascular disease in 130 000 people from 17 high-income, middle-income, and low-income countries: The PURE study. Lancet 2017, 390, 2643–2654. [Google Scholar] [CrossRef]
- Prabhu, N.V.; Maiya, A.G.; Prabhu, N.S. Impact of cardiac rehabilitation on functional capacity and physical activity after coronary revascularization: A scientific review. Cardiol. Res. Pract. 2020, 2020, 1236968. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.C.; Tsai, J.C.; Liou, Y.M.; Chan, P. Effectiveness of endurance exercise training in patients with coronary artery disease: A meta-analysis of randomised controlled trials. Eur. J. Cardiovasc. Nurs. 2017, 16, 397–408. [Google Scholar] [CrossRef]
- Janssen, V.; De Gucht, V.; Dusseldorp, E.; Maes, S. Lifestyle modification programmes for patients with coronary heart disease: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Prev. Cardiol. 2013, 20, 620–640. [Google Scholar] [CrossRef]
- Aliabad, H.O.; Vafaeinasab, M.; Morowatisharifabad, M.A.; Afshani, S.A.; Firoozabadi, M.G.; Forouzannia, S.K. Maintenance of physical activity and exercise capacity after rehabilitation in coronary heart disease: A randomized controlled trial. Glob. J. Health Sci. 2014, 6, 198–208. [Google Scholar] [CrossRef] [Green Version]
- Eckel, R.H.; Jakicic, J.M.; Ard, J.D.; de Jesus, J.M.; Houston Miller, N.; Hubbard, V.S.; Lee, I.M.; Lichtenstein, A.H.; Loria, C.M.; Millen, B.E.; et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2960–2984. [Google Scholar] [CrossRef] [Green Version]
- Won, M.H.; Son, Y.J. Perceived social support and physical activity among patients with coronary artery disease. West J. Nurs. Res. 2017, 39, 1606–1623. [Google Scholar] [CrossRef] [PubMed]
- Teleki, S.; Zsidó, A.N.; Lénárd, L.; Komócsi, A.; Kiss, E.C.; Tiringer, I. Role of received social support in the physical activity of coronary heart patients. Appl. Psychol. Health Well Being 2021, 14, 44–63. [Google Scholar] [CrossRef] [PubMed]
- Gronewold, J.; Kropp, R.; Lehmann, N.; Schmidt, B.; Weyers, S.; Siegrist, J.; Hermann, D.M. Association of social relationships with incident cardiovascular events and all-cause mortality. Heart 2020, 106, 1317–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Won, M.H.; Kim, O. A Prediction model for physical activity adherence for secondary prevention among patients with coronary artery disease. Korean J. Adult Nurs. 2019, 31, 78–88. [Google Scholar] [CrossRef] [Green Version]
- Birtwistle, S.B.; Jones, I.; Murphy, R.; Gee, I.; Watson, P.M. Family support for physical activity post-myocardial infarction: A qualitative study exploring the perceptions of cardiac rehabilitation practitioners. Nurs. Health Sci. 2021, 23, 227–236. [Google Scholar] [CrossRef]
- Sanchis-Gomar, F.; Perez-Quilis, C.; Leischik, R.; Lucia, A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann. Transl. Med. 2016, 4, 256. [Google Scholar]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Englewood Cliffs: Prentice-Hall, NJ, USA, 1986. [Google Scholar]
- Mendoza-Vasconez, A.S.; Marquez, B.; Benitez, T.J.; Marcus, B.H. Psychometrics of the self-efficacy for physical activity scale among a Latina women sample. BMC Public Health 2018, 18, 1097. [Google Scholar] [CrossRef]
- Bergström, G.; Börjesson, M.; Schmidt, C. Self-efficacy regarding physical activity is superior to self-assessed activity level, in long-term prediction of cardiovascular events in middle-aged men. BMC Public Health 2015, 15, 820. [Google Scholar] [CrossRef] [Green Version]
- Slovinec D’Angelo, M.E.; Pelletier, L.G.; Reid, R.D.; Huta, V. The roles of self-efficacy and motivation in the prediction of short-and long-term adherence to exercise among patients with coronary heart disease. Health Psychol. 2014, 33, 1344–1354. [Google Scholar] [CrossRef] [Green Version]
- Knittle, K.; De Gucht, V.; Hurkmans, E.; Vlieland, T.V.; Maes, S. Explaining physical activity maintenance after a theory-based intervention among patients with rheumatoid arthritis: Process evaluation of a randomized controlled trial. Arthritis Care Res. 2016, 68, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Ng, J.Y.Y.; Ntoumanis, N.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Duda, J.L.; Williams, G.C. Self-determination theory applied to health contexts. Perspect. Psychol. Sci. 2012, 7, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Hannan, A.L.; Harders, M.P.; Hing, W.; Climstein, M.; Coombes, J.S.; Furness, J. Impact of wearable physical activity monitoring devices with exercise prescription or advice in the maintenance phase of cardiac rehabilitation: Systematic review and meta-analysis. BMC Sports Sci. Med. Rehabil. 2019, 11, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sweet, S.N.; Fortier, M.S.; Strachan, S.M.; Blanchard, C.M.; Boulay, P. Testing a longitudinal integrated self-efficacy and self-determination theory model for physical activity post-cardiac rehabilitation. Health Psychol. Res. 2014, 2, 30–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knapik, A.; Dąbek, J.; Brzęk, A. Kinesiophobia as a problem in adherence to physical activity recommendations in elderly polish patients with coronary artery disease. Patient Prefer. Adherence 2019, 13, 2129–2135. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Liu, H.; Chen, C.; Chang, W.; Ma, Y.; Zhao, C.; Xing, Y. Physical activity and factors affecting its maintenance among patients with coronary heart disease not undergoing cardiac rehabilitation in China. J. Cardiovasc. Nurs. 2020, 35, 558–567. [Google Scholar] [CrossRef]
- Williams, G.C.; Freedman, Z.R.; Deci, E.L. Supporting autonomy to motivate patients with diabetes for glucose control. Diabetes Care 1998, 21, 1644–1651. [Google Scholar] [CrossRef]
- Hickey, M.L.; Owen, S.V.; Froman, R.D. Instrument development: Cardiac diet and exercise self-efficacy. Nurs. Res. 1992, 41, 347–351. [Google Scholar]
- Xu, L.; Ryu, S.; Goong, H. Gender differences in predictors of health behaviors modification among patients with cardiovascular disease. J. Korea Contents Assoc. 2015, 15, 280–289. [Google Scholar] [CrossRef]
- Levesque, C.S.; Williams, G.C.; Elliot, D.; Pickering, M.A.; Bodenhamer, B.; Finley, P.J. Validating the theoretical structure of the Treatment Self-Regulation Questionnaire (TSRQ) across three different health behaviors. Health Educ. Res. 2007, 22, 691–702. [Google Scholar] [CrossRef]
- Armstrong, T.; Bull, F. Development of the World Health Organization global physical activity questionnaire (GPAQ). J. Public Health 2006, 14, 6–70. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Won, M.H. Mediating effect of physical activity in the relationship between depressive symptoms and health-related quality of life in patients with coronary artery disease: The 2016 nationwide community health survey in Korea. Korean J. Adult Nurs. 2019, 31, 691–700. [Google Scholar] [CrossRef]
- Lu, M.; Xia, H.; Ma, J.; Lin, Y.; Zhang, X.; Shen, Y.; Hravnak, M. Relationship between adherence to secondary prevention and health literacy, self-efficacy and disease knowledge among patients with coronary artery disease in China. Eur. J. Cardiovasc. Nurs. 2020, 19, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Klompstra, L.; Jaarsma, T.; Strömberg, A.; Evangelista, L.S.; van der Wal, M.H.; HF-Wii Study Team. Exercise motivation and self-efficacy vary among patients with heart failure–An explorative analysis using data from the HF-Wii Study. Patient Prefer. Adherence 2021, 15, 2353–2362. [Google Scholar] [CrossRef] [PubMed]
- Siegmund, L.A.; Ahmed, H.M.; Crawford, M.T.; Bena, J.F. Feasibility of a Facebook intervention for exercise motivation and cardiac rehabilitation adherence: Study protocol. JMIR Res. Protoc. 2017, 6, e162. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Category | n (%) | PA (MET-In/Week) Mean ± SD | t or F | p |
|---|---|---|---|---|---|
| Age (years) | <65 | 88 (46.3) | 1357.88 ± 1136.57 | 1.08 | 0.28 |
| ≥65 | 102 (53.7) | 1191.62 ± 977.18 | |||
| Gender | Men | 104 (54.7) | 1199.62 ± 632.43 | 5.36 | <0.001 |
| Women | 86 (45.3) | 632.43 ± 43 | |||
| Education level | ≦Middle school | 77 (40.5) | 526.46 ± 59.99 | 14.05 | <0.001 |
| High school | 75 (39.5) | 1208.43 ± 139.53 | |||
| ≥College | 38 (20.0) | 1488.26 ± 1202.96 | |||
| Living arrangement | Alone | 40 (21.1) | 1090.85 ± 867.83 | −1.2 | 0.231 |
| With family | 150 (78.9) | 1316.04 ± 1096.55 | |||
| Employment | No | 96 (50.5) | 1109.38 ± 955.22 | 2.07 | 0.039 |
| Yes | 94 (49.5) | 1126.52 ± 114.97 | |||
| BMI (kg/m2) | Underweight (<18.5) | 32 (16.8) | 1044.12 ± 1162.65 | 3.69 | 0.013 |
| Normal (18.5–22.9) | 48 (25.3) | 1191.86 ± 162.19 | |||
| Overweight (23–24.9) | 52 (27.4) | 923.19 ± 130.55 | |||
| Obesity (≥25) | 58 (30.5) | 861.39 ± 117.29 | |||
| Periods since diagnosed | <1 | 100 (52.6) | 1183.86 ± 967.65 | −1.16 | 0.244 |
| (years) | ≥1 | 90 (47.4) | 1362.82 ± 1141.25 | ||
| LVEF (%) | <40 | 28 (14.7) | 863.65 ± 74.33 | 18.12 | <0.001 |
| 41–49 | 75 (39.5) | 933.71 ± 1109.87 | |||
| ≥50 | 87 (42.8) | 1759.92 ± 1135.70 | |||
| PCI | No | 55 (28.9) | 1127.50 ± 152.03 | −6.8 | <0.001 |
| Yes | 135 (71.1) | 893.11 ± 703.35 | |||
| Number of chronic | 1 | 87 (45.8) | 1755.77 ± 1165.30 | 21.05 | <0.001 |
| diseases | 2 | 64 (33.7) | 913.25 ± 755.74 | ||
| ≥3 | 39 (20.5) | 765.12 ± 702.54 | |||
| Prescribed cardiac | Aspirin, yes | 131 (67.5) | 1288.27 ± 1088.01 | 0.495 | 0.622 |
| medications | Clopidogrel, yes | 163 (84.0) | 1278.99 ± 1035.46 | 0.5 | 0.615 |
| Lipid-lowering agents, yes | 172 (88.7) | 1261.65 ± 1085.12 | −0.03 | 0.978 | |
| ACEI or ARB, yes | 98 (50.5) | 1237.83 ± 1019.46 | −0.39 | 0.691 | |
| Beta blocker, yes | 79 (40.7) | 1352.96 ± 959.90 | 0.99 | 0.32 |
| Variables | Mean ± SD | 1 | 2 | 3 |
|---|---|---|---|---|
| r (p) | r (p) | r (p) | ||
| 1. Social support | 81.94 ± 14.34 | 1 | ||
| 2. Self-efficacy | 45.90 ± 14.28 | 0.40 (<0.001) | 1 | |
| 3. Autonomy motivation | 42.30 ± 10.45 | 0.61 (<0.001) | 0.39 (<0.001) | 1 |
| 4. Physical activity (MET-in/week) | 1268.63 ± 1054.43 | 0.53 (<0.001) | 0.48 (<0.001) | 0.54 (<0.001) |
| Path | Variables | B | SE | t | p | 95% CI | Adj. R2 | F (p) | |
|---|---|---|---|---|---|---|---|---|---|
| LL | UL | ||||||||
| a1 | Social support → Self-efficacy | 0.33 | 0.07 | 4.67 | <0.001 | 0.19 | 0.47 | 0.217 | 6.27 (<0.001) |
| a2 | Social support → Autonomous motivation | 0.37 | 0.04 | 8.87 | <0.001 | 0.29 | 0.46 | 0.459 | 19.20 (<0.001) |
| c | Social support → Physical activity | 16.34 | 4.89 | 3.34 | 0.001 | 6.68 | 25.99 | 0.541 | 21.11 (<0.001) |
| b1 | Self-efficacy → Physical activity | 15.02 | 4.25 | 3.53 | 0.005 | 6.62 | 23.41 | ||
| b2 | Autonomous motivation → Physical activity | 18.50 | 6.99 | 2.64 | 0.008 | 4.69 | 32.31 | ||
| Variables | Direct Effect | Indirect Effect | ||||||
|---|---|---|---|---|---|---|---|---|
| B | Boot SE | 95% CI | B | Boot SE | 95% CI | |||
| Boot LLCI | Boot ULCI | Boot LLCI | Boot ULCI | |||||
| Social support → Physical activity (c) | 16.34 | 4.97 | 6.88 | 26.39 | ||||
| Social support → Self-efficacy → Physical activity (a1b1) | 4.92 | 1.78 | 1.89 | 8.78 | ||||
| Social support → Autonomous motivation → Physical activity (a2b2) | 7 | 2.68 | 1.69 | 12.37 | ||||
| Total (c′) | 11.92 | 3.15 | 5.82 | 18.3 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, N.-S.; Won, M.-H. Association between Social Support and Physical Activity in Patients with Coronary Artery Disease: Multiple Mediating Roles of Self-Efficacy and Autonomous Motivation. Healthcare 2022, 10, 425. https://doi.org/10.3390/healthcare10030425
Han N-S, Won M-H. Association between Social Support and Physical Activity in Patients with Coronary Artery Disease: Multiple Mediating Roles of Self-Efficacy and Autonomous Motivation. Healthcare. 2022; 10(3):425. https://doi.org/10.3390/healthcare10030425
Chicago/Turabian StyleHan, Nam-Sin, and Mi-Hwa Won. 2022. "Association between Social Support and Physical Activity in Patients with Coronary Artery Disease: Multiple Mediating Roles of Self-Efficacy and Autonomous Motivation" Healthcare 10, no. 3: 425. https://doi.org/10.3390/healthcare10030425