
Identification of Germline Variants in Patients with Hereditary Cancer Syndromes in Northeast Mexico


 , , ,
, , , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patients’ Groups and Approval from the Ethics Committee
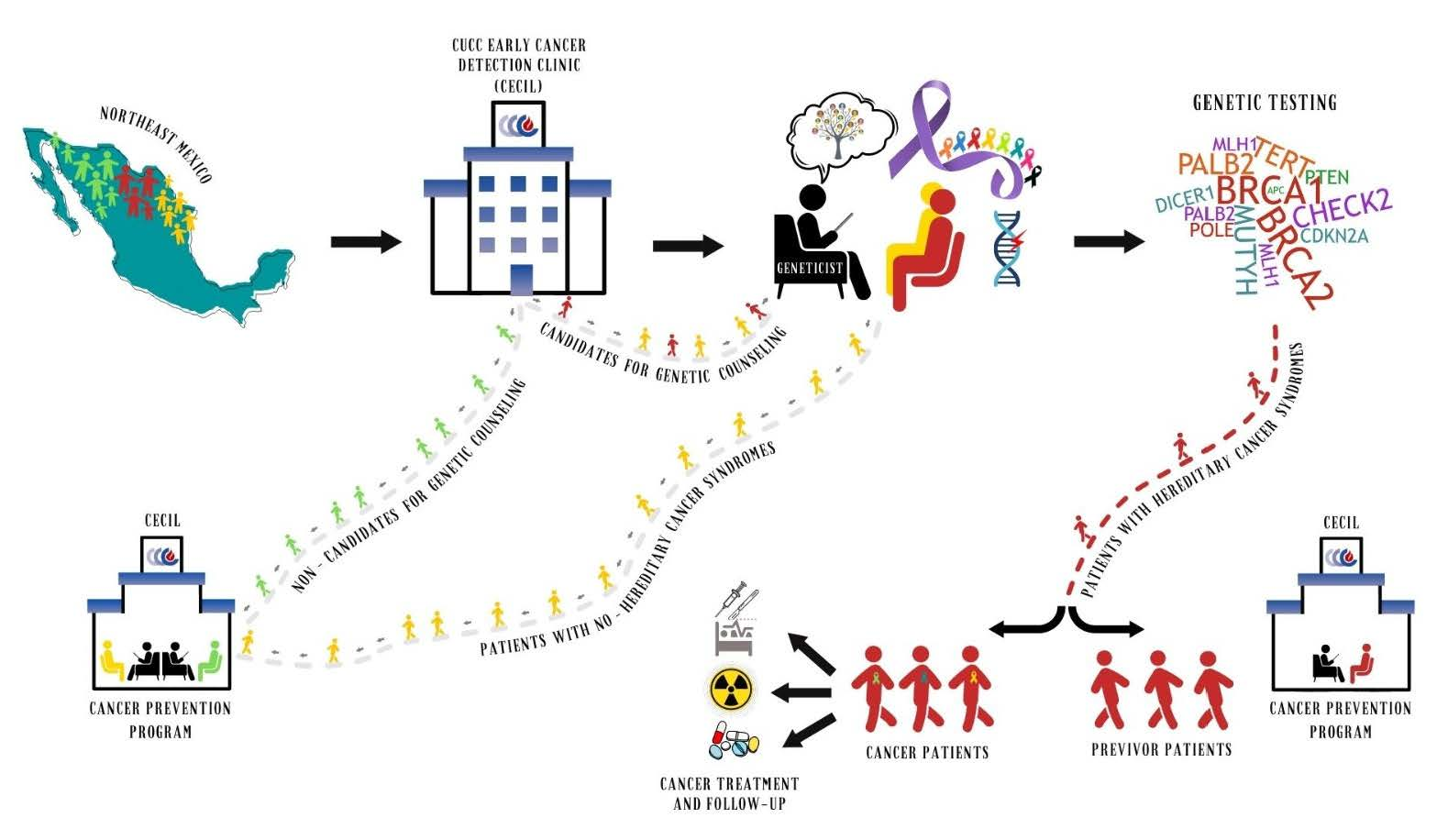
2.2. Algorithm Workflow
2.3. Proband Patients NGS Study
2.4. Genetic Counseling
2.5. Test for Relatives and DNA Extraction
2.6. DNA Sanger Sequencing for Relatives
2.7. Bioinformatics Analysis and Variant Annotation
3. Results
3.1. Patient Description
3.2. Germline Variants
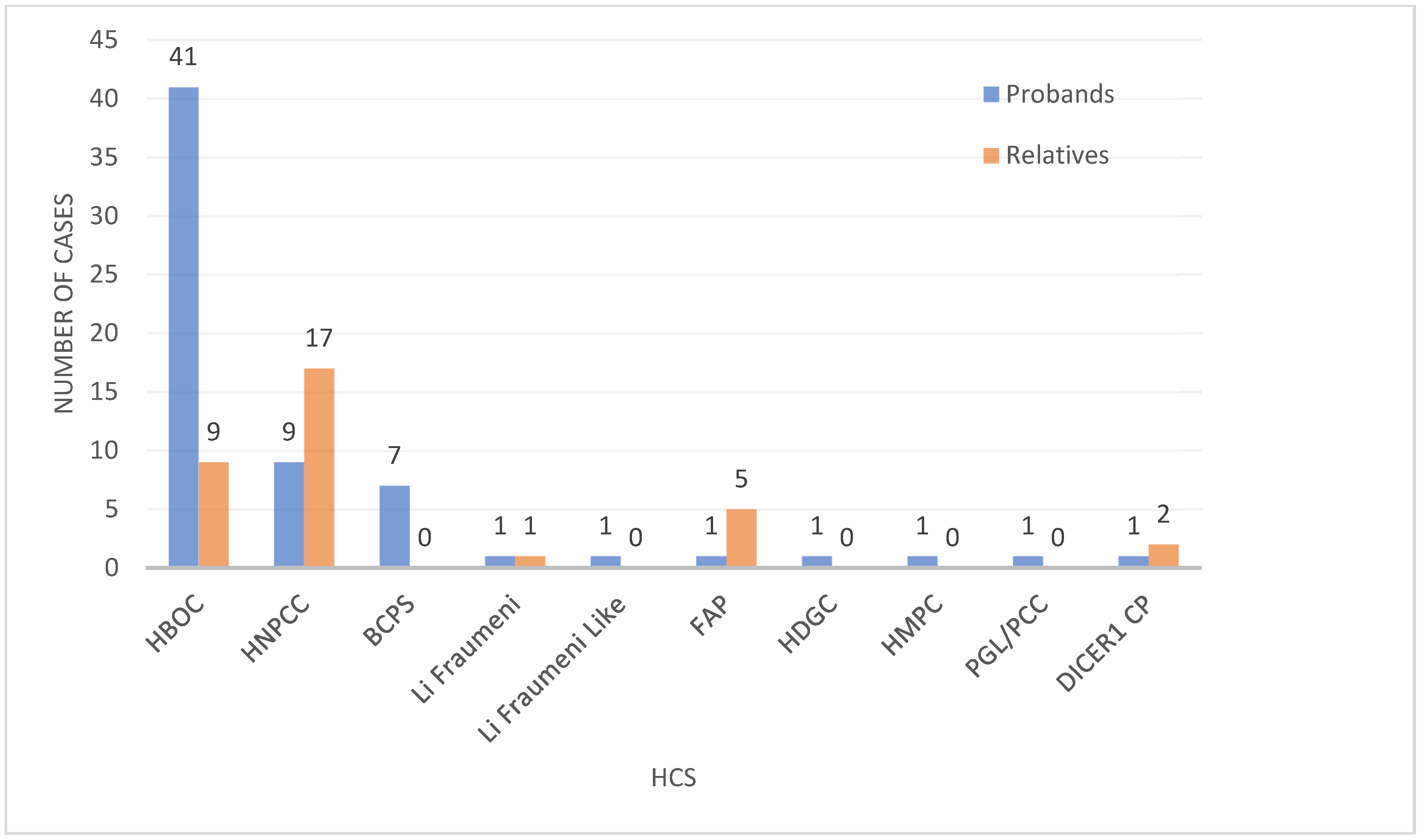
3.3. HCS Frequency
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wagener, R.; Taeubner, J.; Walter, C.; Yasin, L.; Alzoubi, D.; Bartenhagen, C.; Attarbaschi, A.; Classen, C.F.; Kontny, U.; Hauer, J.; et al. Comprehensive germline-genomic and clinical profiling in 160 unselected children and adolescents with cancer. Eur. J. Hum. Genet. 2021, 29, 1301–1311. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, D.E.; Chen, Y.; Jamieson, R.V.; Dalla-Pozza, L.; Byrne, J.A. Investigation of clinically relevant germline variants detected by next-generation sequencing in patients with childhood cancer: A review of the literature. J. Med. Genet. 2018, 55, 785–793. [Google Scholar] [CrossRef] [PubMed]
- Tsaousis, G.N.; Papadopoulou, E.; Apessos, A.; Agiannitopoulos, K.; Pepe, G.; Kampouri, S.; Diamantopoulos, N.; Floros, T.; Iosifidou, R.; Katopodi, O.; et al. Analysis of hereditary cancer syndromes by using a panel of genes: Novel and multiple pathogenic mutations. BMC Cancer 2019, 19, 535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, S.A.; Bradbury, A.; Henderson, V.; Hoskins, K.; Bednar, E.; Arun, B.K. Genetic Counseling and Testing in a Community Setting: Quality, Access, and Efficiency. Am. Soc. Clin. Oncol. Educ. Book 2019, 39, e34–e44. [Google Scholar] [CrossRef]
- Powers, J.; Spielman, K.; Mueller, R.; Batson, M.; Pundock, S.; Arutyunova, A.; Symecko, H.; Domchek, S. Genetic counseling and oncology: Proposed approaches for collaborative care delivery. Can. J. Urol. 2019, 26, 57–59. [Google Scholar]
- Yang, M.; Kim, J.W. Principles of Genetic Counseling in the Era of Next-Generation Sequencing. Ann. Lab. Med. 2018, 38, 291–295. [Google Scholar] [CrossRef]
- Abacan, M.; Alsubaie, L.; Barlow-Stewart, K.; Caanen, B.; Cordier, C.; Courtney, E.; Davoine, E.; Edwards, J.; Elackatt, N.J.; Gardiner, K.; et al. The Global State of the Genetic Counseling Profession. Eur. J. Hum. Genet. 2019, 27, 183–197. [Google Scholar] [CrossRef] [Green Version]
- Jara-Ettinger, A.C.; Cardenas-Conejo, A.; Huicochea-Montie, J.C.; Araujo-Solis, M.A.J. The lag of genetic counseling in Mexico. Rev. Med. Inst. Mex. Seguro. Soc. 2021, 59, 101–105. [Google Scholar] [CrossRef]
- Yuen, J.; Lee, S.Y.; Courtney, E.; Lim, J.; Soh, H.; Li, S.T.; Chen, Y.; McAllister, M.; Fenwick, E.K.; Ngeow, J. Evaluating empowerment in genetic counseling using patient-reported outcomes. Clin. Genet. 2020, 97, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Lohn, Z.; Fok, A.; Richardson, M.; Derocher, H.; Mung, S.W.; Nuk, J.; Yuson, J.; Jevon, M.; Schrader, K.A.; Sun, S. Large-scale group genetic counseling: Evaluation of a novel service delivery model in a Canadian hereditary cancer clinic. J. Genet. Couns. 2022, 31, 459–469. [Google Scholar] [CrossRef]
- Cohen, S.A.; Gustafson, S.L.; Marvin, M.L.; Riley, B.D.; Uhlmann, W.R.; Liebers, S.B.; Rousseau, J.A. Report from the National Society of Genetic Counselors service delivery model task force: A proposal to define models, components, and modes of referral. J. Genet. Couns. 2012, 21, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Amendola, L.M.; Golden-Grant, K.; Scollon, S. Scaling Genetic Counseling in the Genomics Era. Annu. Rev. Genomics Hum. Genet. 2021, 22, 339–355. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, T.; Tucker, K.; Wakefield, C.E.; Geelan-Small, P.; Macmillan, S.; Taylor, N.; Williams, R. Comparing cancer genetic counselling using telegenetics with in-person and telephone appointments: Results of a partially randomised patient-preference pilot study. J. Telemed. Telecare 2022, ahead of print. 1357633X221112556. [Google Scholar] [CrossRef]
- Lolkema, M.P.; Gadellaa-van Hooijdonk, C.G.; Bredenoord, A.L.; Kapitein, P.; Roach, N.; Cuppen, E.; Knoers, N.V.; Voest, E.E. Ethical, legal, and counseling challenges surrounding the return of genetic results in oncology. J. Clin. Oncol. 2013, 31, 1842–1848. [Google Scholar] [CrossRef] [PubMed]
- Bucio, D.; Ormond, K.E.; Hernandez, D.; Bustamante, C.D.; Lopez Pineda, A. A genetic counseling needs assessment of Mexico. Mol. Genet. Genomic Med. 2019, 7, e668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valdespino-Gomez, V.M.; Valdespino-Castillo, V.E. Usefulness of the oncogenetic molecular counselling in adults whith familial cancer. Rev. Med. Inst. Mex. Seguro Soc. 2016, 54, 364–374. [Google Scholar]
- Childers, K.K.; Maggard-Gibbons, M.; Macinko, J.; Childers, C.P. National Distribution of Cancer Genetic Testing in the United States: Evidence for a Gender Disparity in Hereditary Breast and Ovarian Cancer. JAMA Oncol. 2018, 4, 876–879. [Google Scholar] [CrossRef]
- Daly, M.B.; Pal, T.; Berry, M.P.; Buys, S.S.; Dickson, P.; Domchek, S.M.; Elkhanany, A.; Friedman, S.; Goggins, M.; Hutton, M.L.; et al. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2021, 19, 77–102. [Google Scholar] [CrossRef]
- Padilla-Raygoza, N.; Monroy-Torres, R.; Sandoval-Salazar, C.; Vera-Becerra, L.E.; Patino-Lopez, M.E.; de Lourdes Garcia-Campos, M.; Campos, V.B.; Del Carmen Ortega Jimenez, M.; Del Carmen Delgado-Sandoval, S.; Ramirez-Gomez, X.S.; et al. Cancer prevention programmes in Mexico: Are we doing enough? Ecancermedicalscience 2020, 14, 997. [Google Scholar] [CrossRef]
- Rychlik, W. OLIGO 7 primer analysis software. Methods Mol. Biol. 2007, 402, 35–60. [Google Scholar] [CrossRef]
- Li, M.M.; Datto, M.; Duncavage, E.J.; Kulkarni, S.; Lindeman, N.I.; Roy, S.; Tsimberidou, A.M.; Vnencak-Jones, C.L.; Wolff, D.J.; Younes, A.; et al. Standards and Guidelines for the Interpretation and Reporting of Sequence Variants in Cancer: A Joint Consensus Recommendation of the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists. J. Mol. Diagn. 2017, 19, 4–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef] [PubMed]
- McKusick-Nathans Institute of Genetic Medicine Online Mendelian Inheritance in Man, OMIM. Available online: https://omim.org/ (accessed on 24 June 2022).
- Boulyjenkov, V. The role of the World Health Organization in promoting medical genetics in Latin America. Community Genet. 2004, 7, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Douglas, M.P.; Lin, G.A.; Trosman, J.R.; Phillips, K.A. Hereditary cancer panel testing challenges and solutions for the latinx community: Costs, access, and variants. J. Community Genet. 2022, 13, 75–80. [Google Scholar] [CrossRef]
- Penchaszadeh, V.B. Genetic services in Latin America. Community Genet. 2004, 7, 65–69. [Google Scholar] [CrossRef]
- Marques-de-Faria, A.P.; Ferraz, V.E.; Acosta, A.X.; Brunoni, D. Clinical genetics in developing countries: The case of Brazil. Community Genet. 2004, 7, 95–105. [Google Scholar] [CrossRef]
- Garza-Rodriguez, M.L.; Trevino, V.; Perez-Maya, A.A.; Rodriguez-Gutierrez, H.F.; Gonzalez-Escamilla, M.; Elizondo-Riojas, M.A.; Ramirez-Correa, G.A.; Vidal-Gutierrez, O.; Burciaga-Flores, C.H.; Perez-Ibave, D.C. Identification of a Novel Pathogenic Rearrangement Variant of the APC Gene Associated with a Variable Spectrum of Familial Cancer. Diagnostics 2021, 11, 411. [Google Scholar] [CrossRef]
- Fragoso-Ontiveros, V.; Velazquez-Aragon, J.A.; Nunez-Martinez, P.M.; de la Luz Mejia-Aguayo, M.; Vidal-Millan, S.; Pedroza-Torres, A.; Sanchez-Contreras, Y.; Ramirez-Otero, M.A.; Muniz-Mendoza, R.; Dominguez-Ortiz, J.; et al. Mexican BRCA1 founder mutation: Shortening the gap in genetic assessment for hereditary breast and ovarian cancer patients. PLoS ONE 2019, 14, e0222709. [Google Scholar] [CrossRef] [PubMed]
- Herzog, J.S.; Chavarri-Guerra, Y.; Castillo, D.; Abugattas, J.; Villarreal-Garza, C.; Sand, S.; Clague-Dehart, J.; Alvarez-Gomez, R.M.; Wegman-Ostrosky, T.; Mohar, A.; et al. Genetic epidemiology of BRCA1- and BRCA2-associated cancer across Latin America. NPJ Breast Cancer 2021, 7, 107. [Google Scholar] [CrossRef]
- Zayas-Villanueva, O.A.; Campos-Acevedo, L.D.; Lugo-Trampe, J.J.; Hernandez-Barajas, D.; Gonzalez-Guerrero, J.F.; Noriega-Iriondo, M.F.; Ramirez-Sanchez, I.A.; Martinez-de-Villarreal, L.E. Analysis of the pathogenic variants of BRCA1 and BRCA2 using next-generation sequencing in women with familial breast cancer: A case-control study. BMC Cancer 2019, 19, 722. [Google Scholar] [CrossRef] [Green Version]
- Rubi-Castellanos, R.; Martinez-Cortes, G.; Munoz-Valle, J.F.; Gonzalez-Martin, A.; Cerda-Flores, R.M.; Anaya-Palafox, M.; Rangel-Villalobos, H. Pre-Hispanic Mesoamerican demography approximates the present-day ancestry of Mestizos throughout the territory of Mexico. Am. J. Phys. Anthropol. 2009, 139, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Penchaszadeh, V.B.; Beiguelman, B. Medical genetic services in Latin America: Report of a meeting of experts. Rev. Panam. Salud Publica 1998, 3, 409–420. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Flores, J.; Zuniga-Chiquette, F.; Rubi-Castellanos, R.; Alvarez-Miranda, J.L.; Zetina-Hernandez, A.; Martinez-Sevilla, V.M.; Gonzalez-Andrade, F.; Corach, D.; Vullo, C.; Alvarez, J.C.; et al. Admixture and genetic relationships of Mexican Mestizos regarding Latin American and Caribbean populations based on 13 CODIS-STRs. Homo 2015, 66, 44–59. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Cortes, G.; Salazar-Flores, J.; Haro-Guerrero, J.; Rubi-Castellanos, R.; Velarde-Felix, J.S.; Munoz-Valle, J.F.; Lopez-Casamichana, M.; Carrillo-Tapia, E.; Canseco-Avila, L.M.; Bravi, C.M.; et al. Maternal admixture and population structure in Mexican-Mestizos based on mtDNA haplogroups. Am. J. Phys. Anthropol. 2013, 151, 526–537. [Google Scholar] [CrossRef] [PubMed]
- ClinVar. National Library of Medicine. NM_007294.4(BRCA1):c.3113A>C (p.Glu1038Ala) AND Breast and/or Ovarian Cancer. Available online: https://www.ncbi.nlm.nih.gov/clinvar/120833734/ (accessed on 6 January 2023).
- Kwong, A.; Shin, V.Y.; Ho, C.Y.S.; Khalid, A.; Au, C.H.; Chan, K.K.L.; Ngan, H.Y.S.; Chan, T.L.; Ma, E.S.K. Germline PALB2 Mutation in High-Risk Chinese Breast and/or Ovarian Cancer Patients. Cancers 2021, 13, 4195. [Google Scholar] [CrossRef]
- Kuusisto, K.M.; Bebel, A.; Vihinen, M.; Schleutker, J.; Sallinen, S.L. Screening for BRCA1, BRCA2, CHEK2, PALB2, BRIP1, RAD50, and CDH1 mutations in high-risk Finnish BRCA1/2-founder mutation-negative breast and/or ovarian cancer individuals. Breast Cancer Res. 2011, 13, R20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubard Gault, M.; Mandelker, D.; DeLair, D.; Stewart, C.R.; Kemel, Y.; Sheehan, M.R.; Siegel, B.; Kennedy, J.; Marcell, V.; Arnold, A.; et al. Germline SDHA mutations in children and adults with cancer. Cold Spring Harb. Mol. Case Stud. 2018, 4, a002584. [Google Scholar] [CrossRef] [Green Version]
- Soerjomataram, I.; Bray, F. Planning for tomorrow: Global cancer incidence and the role of prevention 2020–2070. Nat. Rev. Clin. Oncol. 2021, 18, 663–672. [Google Scholar] [CrossRef]
- Williams, K.P.; Mullan, P.B.; Todem, D. Moving from theory to practice: Implementing the Kin Keeper Cancer Prevention Model. Health Educ. Res. 2009, 24, 343–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zonderman, A.B.; Ejiogu, N.; Norbeck, J.; Evans, M.K. The influence of health disparities on targeting cancer prevention efforts. Am. J. Prev. Med. 2014, 46, S87–S97. [Google Scholar] [CrossRef] [Green Version]
- Britt, K.L.; Cuzick, J.; Phillips, K.A. Key steps for effective breast cancer prevention. Nat. Rev. Cancer 2020, 20, 417–436. [Google Scholar] [CrossRef] [PubMed]
- DuBard, C.A.; Gizlice, Z. Language spoken and differences in health status, access to care, and receipt of preventive services among US Hispanics. Am. J. Public Health 2008, 98, 2021–2028. [Google Scholar] [CrossRef] [PubMed]
- Allain, D.C. Genetic counseling and testing for common hereditary breast cancer syndromes: A paper from the 2007 William Beaumont hospital symposium on molecular pathology. J. Mol. Diagn. 2008, 10, 383–395. [Google Scholar] [CrossRef] [Green Version]
- Kofman-Alfaro, S.; Zenteno, J.C. Genetic services in Mexico City. Community Genet. 2004, 7, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Gobierno de Nuevo Leon, Mexico. Cobertura Universal Contra el Cáncer de Mama. Available online: https://www.nl.gob.mx/campanas/cobertura-universal-contra-el-cancer-de-mama (accessed on 11 January 2022).



{kind=link}
{kind=link}
{kind=link}
| Cancer Distribution | n (%) |
|---|---|
| Breast (total) Breast (Unilateral) Breast (Bilateral) Breast (Bilateral) & Pancreas Breast & Pancreas Breast and Ovarian | 95 (78.51) 82 (86.31) 8 (8.42) 1 (1.05) 1 (1.95) 3 (3.15) |
| Ovarian (total) Ovarian (unilateral) Ovarian, Kidney and Pseudomyxoma | 10 (8.26) 9 (90) 1 (10) |
| Colon | 8 (6.61) |
| Melanoma, Breast, and Cervical | 1 (0.82) |
| Endometrial | 3 (2.47) |
| Sarcoma (total) Sarcoma Sarcoma and Thyroid | 2 (1.65) 1 (50) 1 (50) |
| Medulloblastoma and Kidney | 1 (0.82) |
| Hemangioendothelioma | 1 (0.82) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Ibave, D.C.; Garza-Rodríguez, M.L.; Noriega-Iriondo, M.F.; Flores-Moreno, S.M.; González-Geroniz, M.I.; Espinoza-Velazco, A.; Castruita-Ávila, A.L.; Alcorta-Núñez, F.; Zayas-Villanueva, O.A.; González-Guerrero, J.F.; et al. Identification of Germline Variants in Patients with Hereditary Cancer Syndromes in Northeast Mexico. Genes 2023, 14, 341. https://doi.org/10.3390/genes14020341
Pérez-Ibave DC, Garza-Rodríguez ML, Noriega-Iriondo MF, Flores-Moreno SM, González-Geroniz MI, Espinoza-Velazco A, Castruita-Ávila AL, Alcorta-Núñez F, Zayas-Villanueva OA, González-Guerrero JF, et al. Identification of Germline Variants in Patients with Hereditary Cancer Syndromes in Northeast Mexico. Genes. 2023; 14(2):341. https://doi.org/10.3390/genes14020341
Chicago/Turabian StylePérez-Ibave, Diana Cristina, María Lourdes Garza-Rodríguez, María Fernanda Noriega-Iriondo, Sonia María Flores-Moreno, Manuel Ismael González-Geroniz, Absalon Espinoza-Velazco, Ana Lilia Castruita-Ávila, Fernando Alcorta-Núñez, Omar Alejandro Zayas-Villanueva, Juan Francisco González-Guerrero, and et al. 2023. "Identification of Germline Variants in Patients with Hereditary Cancer Syndromes in Northeast Mexico" Genes 14, no. 2: 341. https://doi.org/10.3390/genes14020341