
Phenotypic Impact of Rare Potentially Damaging Copy Number Variation in Obsessive-Compulsive Disorder and Chronic Tic Disorders

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. CNV Identification
2.3. Severity of OCD Symptoms
2.4. Psychiatric Co-Occurring Conditions
2.5. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Genetic Findings
3.3. Co-Occurring Psychiatric Conditions in the Probands
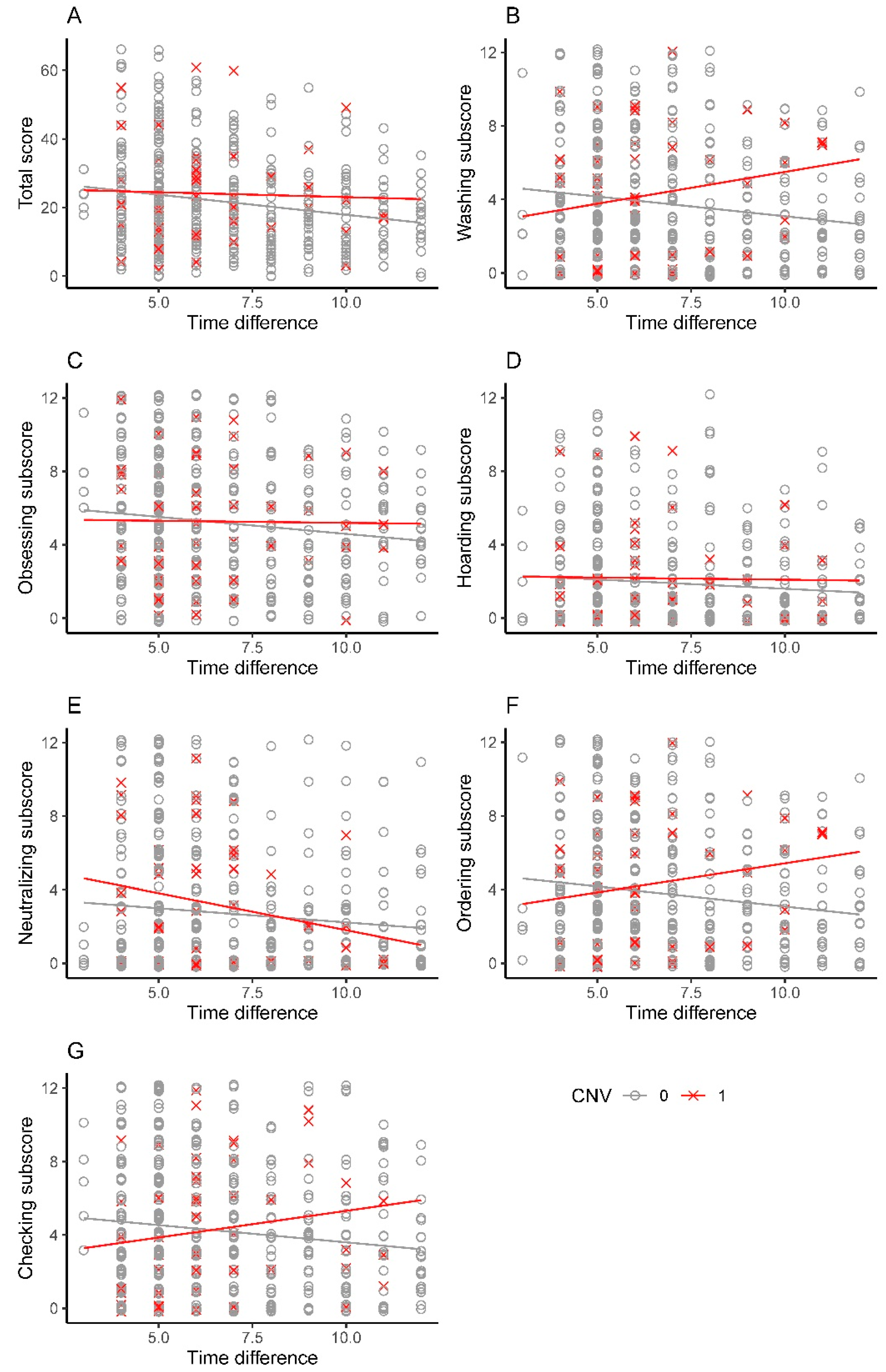
3.4. Severity of OCD among Carriers of pdCNV
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mahjani, B.; Bey, K.; Boberg, J.; Burton, C. Genetics of obsessive-compulsive disorder. Psychol. Med. 2021, 51, 2247–2259. [Google Scholar] [CrossRef] [PubMed]
- Anholt, G.E.; Aderka, I.M.; van Balkom, A.J.L.M.; Smit, J.H.; Schruers, K.; van der Wee, N.J.A.; Eikelenboom, M.; De Luca, V.; van Oppen, P. Age of onset in obsessive-compulsive disorder: Admixture analysis with a large sample. Psychol. Med. 2014, 44, 185–194. [Google Scholar] [CrossRef]
- Geller, D.A. Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatr. Clin. North Am. 2006, 29, 353–370. [Google Scholar] [CrossRef] [PubMed]
- Leckman, J.F.; Denys, D.; Simpson, H.B.; Mataix-Cols, D.; Hollander, E.; Saxena, S.; Miguel, E.C.; Rauch, S.L.; Goodman, W.K.; Phillips, K.A.; et al. Obsessive-compulsive disorder: A review of the diagnostic criteria and possible subtypes and dimensional specifiers for DSM-V. Depress. Anxiety 2010, 27, 507–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, S. Early versus late onset obsessive-compulsive disorder: Evidence for distinct subtypes. Clin. Psychol. Rev. 2011, 31, 1083–1100. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S. Etiology of obsessions and compulsions: A meta-analysis and narrative review of twin studies. Clin. Psychol. Rev. 2011, 31, 1361–1372. [Google Scholar] [CrossRef]
- Ruscio, A.M.; Stein, D.J.; Chiu, W.T.; Kessler, R.C. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol. Psychiatry 2010, 15, 53–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassi, G.; Cecchelli, C.; Mazzocato, G.; Vignozzi, L. Early onset obsessive-compulsive disorder: The biological and clinical phenotype. CNS Spectr. 2021, 27, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hudziak, J.J.; Van Beijsterveldt, C.E.M.; Althoff, R.R.; Stanger, C.; Rettew, D.C.; Nelson, E.C.; Todd, R.D.; Bartels, M.; Boomsma, D.I. Genetic and environmental contributions to the Child Behavior Checklist Obsessive-Compulsive Scale: A cross-cultural twin study. Arch. Gen. Psychiatry 2004, 61, 608–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolton, D.; Rijsdijk, F.; Eley, T.C.; O’Connor, T.G.; Briskman, J.; Perrin, S. Normative childhood repetitive routines and obsessive compulsive symptomatology in 6-year-old twins. J. Child. Psychol. Psychiatry 2009, 50, 1139–1146. [Google Scholar] [CrossRef]
- Zilhão, N.R.; Smit, D.J.A.; den Braber, A.; Dolan, C.V.; Willemsen, G.; Boomsma, D.I.; Cath, D.C. Genetic and environmental contributions to stability in adult obsessive compulsive behavior. Twin Res. Hum. Genet. 2015, 18, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Halvorsen, M.; Samuels, J.; Wang, Y.; Greenberg, B.D.; Fyer, A.J.; McCracken, J.T.; Geller, D.A.; Knowles, J.A.; Zoghbi, A.W.; Pottinger, T.D.; et al. Exome sequencing in obsessive-compulsive disorder reveals a burden of rare damaging coding variants. Nat. Neurosci. 2021, 24, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Mahjani, B.; Klei, L.; Mattheisen, M.; Halvorsen, M.W.; Reichenberg, A.; Roeder, K.; Pedersen, N.L.; Boberg, J.; de Schipper, E.; Bulik, C.M.; et al. The Genetic Architecture of Obsessive-Compulsive Disorder: Contribution of Liability to OCD From Alleles Across the Frequency Spectrum. Am. J. Psychiatry 2021, 179, 216–225. [Google Scholar] [CrossRef]
- Mahjani, B.; Mahjani, C.G.; Reichenberg, A.; Sandin, S.; Hultman, C.M.; Buxbaum, J.D.; Grice, D.E. OCD Symptom Severity and Comorbid Psychiatric Diagnoses in a Swedish Genetic Epidemiological Obsessive-Compulsive Disorder Cohort. medRxiv 2021. [Google Scholar] [CrossRef]
- Browne, H.A.; Hansen, S.N.; Buxbaum, J.D.; Gair, S.L.; Nissen, J.B.; Nikolajsen, K.H.; Schendel, D.E.; Reichenberg, A.; Parner, E.T.; Grice, D.E. Familial clustering of tic disorders and obsessive-compulsive disorder. JAMA Psychiatry 2015, 72, 359–366. [Google Scholar] [CrossRef] [Green Version]
- do Rosario-Campos, M.C.; Leckman, J.F.; Curi, M.; Quatrano, S.; Katsovitch, L.; Miguel, E.C.; Oauls, D.L. A family study of early-onset obsessive-compulsive disorder. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2005, 136B, 92–97. [Google Scholar] [CrossRef]
- Ivarsson, T.; Melin, K.; Wallin, L. Categorical and dimensional aspects of co-morbidity in obsessive-compulsive disorder (OCD). Eur. Child. Adolesc. Psychiatry 2008, 17, 20–31. [Google Scholar] [CrossRef] [Green Version]
- Nestadt, G.; Di, C.Z.; Riddle, M.A.; Grados, M.A.; Greenberg, B.D.; Fyer, A.J.; McCracken, J.T.; Rauch, S.L.; Murphy, D.L.; Rasmussen, S.A.; et al. Obsessive-compulsive disorder: Subclassification based on co-morbidity. Psychol. Med. 2009, 39, 1491–1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolajsen, K.H.; Nissen, J.B.; Thomsen, P.H. Obsessive-compulsive disorder in children and adolescents: Symptom dimensions in a naturalistic setting. Nord. J. Psychiatry 2011, 65, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Torresan, R.C.; Ramos-Cerqueira, A.T.A.; Shavitt, R.G.; do Rosário, M.C.; de Mathis, M.A.; Miguel, E.C.; Torres, A.R. Symptom dimensions, clinical course and comorbidity in men and women with obsessive-compulsive disorder. Psychiatry Res. 2013, 209, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Mathews, C.A.; Grados, M.A. Familiality of Tourette syndrome, obsessive-compulsive disorder, and attention-deficit/hyperactivity disorder: Heritability analysis in a large sib-pair sample. J. Am. Acad. Child. Adolesc. Psychiatry 2011, 50, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirschtritt, M.E.; Lee, P.C.; Pauls, D.L.; Dion, Y.; Grados, M.A.; Illmann, C.; King, R.A.; Sandor, P.; McMahon, W.M.; Lyon, G.J.; et al. Lifetime prevalence, age of risk, and genetic relationships of comorbid psychiatric disorders in Tourette syndrome. JAMA Psychiatry 2015, 72, 325–333. [Google Scholar] [CrossRef] [Green Version]
- Domènech, L.; Cappi, C.; Halvorsen, M. Genetic architecture of Tourette syndrome: Our current understanding. Psychol. Med. 2021, 51, 2201–2209. [Google Scholar] [CrossRef] [PubMed]
- Coe, B.P.; Stessman, H.A.F.; Sulovari, A.; Geisheker, M.R.; Bakken, T.E.; Lake, A.M.; Dougherty, J.D.; Lein, E.S.; Hormozdiari, F.; Bernier, R.A.; et al. Neurodevelopmental disease genes implicated by de novo mutation and copy number variation morbidity. Nat. Genet. 2019, 51, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Zarrei, M.; Burton, C.L.; Engchuan, W.; Young, E.J.; Higginbotham, E.J.; MacDonald, J.R.; Trost, B.; Chan, A.J.S.; Walker, S.; Lamoureux, S.; et al. A large data resource of genomic copy number variation across neurodevelopmental disorders. NPJ Genom. Med. 2019, 4, 26. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.R.; Glessner, J.T.; Coe, B.P.; Li, J.; Mohebnasab, M.; Chang, X.; Connolly, J.; Kao, C.; Wei, Z.; Bradfield, J.; et al. Rare copy number variants in over 100,000 European ancestry subjects reveal multiple disease associations. Nat Commun. 2020, 11, 255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donovan, M.C.; Kirov, G.; Owen, M.J. Phenotypic variations on the theme of CNVs. Nat. Genet. 2008, 40, 1392–1393. [Google Scholar] [CrossRef] [PubMed]
- Delorme, R.; Moreno-De-Luca, D.; Gennetier, A.; Maier, W.; Chaste, P.; Mössner, R.; Grabe, H.J.; Ruhrmann, S.; Falkai, P.; Mouren, M.-C.; et al. Search for copy number variants in chromosomes 15q11-q13 and 22q11.2 in obsessive compulsive disorder. BMC Med. Genet. 2010, 11, 100. [Google Scholar] [CrossRef] [PubMed]
- Walitza, S.; Bové, D.S.; Romanos, M.; Renner, T.; Held, L.; Simons, M.; Wewetzer, C.; Fleischhaker, C.; Remschmidt, H.; Warnke, A.; et al. Pilot study on HTR2A promoter polymorphism, -1438G/A (rs6311) and a nearby copy number variation showed association with onset and severity in early onset obsessive-compulsive disorder. J. Neural. Transm. 2012, 119, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Hooper, S.D.; Johansson, A.C.V.; Tellgren-Roth, C.; Stattin, E.L.; Dahl, N.; Cavelier, L.; Feuk, L. Genome-wide sequencing for the identification of rearrangements associated with Tourette syndrome and obsessive-compulsive disorder. BMC Med. Genet. 2012, 13, 123. [Google Scholar] [CrossRef] [PubMed]
- McGrath, L.M.; Yu, D.; Marshall, C.; Davis, L.K.; Thiruvahindrapuram, B.; Li, B.; Cappi, C.; Gerber, G.; Wolf, A.; Schroeder, F.A.; et al. Copy number variation in obsessive-compulsive disorder and tourette syndrome: A cross-disorder study. J. Am. Acad. Child. Adolesc. Psychiatry 2014, 53, 910–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cappi, C.; Hounie, A.G.; Mariani, D.B.; Diniz, J.B.; Silva, A.R.T.; Reis, V.N.S.; Busso, A.F.; Silva, A.G.; Fidalgo, F.; Rogatto, S.R.; et al. An inherited small microdeletion at 15q13.3 in a patient with early-onset obsessive-compulsive disorder. PLoS ONE 2014, 9, e110198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gazzellone, M.J.; Zarrei, M.; Burton, C.L.; Walker, S.; Uddin, M.; Shaheen, S.M.; Coste, J.; Rajendram, R.; Schachter, R.J.; Colasanto, M.; et al. Uncovering obsessive-compulsive disorder risk genes in a pediatric cohort by high-resolution analysis of copy number variation. J. Neurodev. Disord. 2016, 8, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grünblatt, E.; Oneda, B.; Ekici, A.B.; Ball, J.; Geissler, J.; Uebe, S.; Romanos, M.; Rauch, A.; Walitza, S. High resolution chromosomal microarray analysis in paediatric obsessive-compulsive disorder. BMC Med. Genom. 2017, 10, 68. [Google Scholar] [CrossRef] [Green Version]
- Jutla, A.; Turner, J.B.; Green Snyder, L.; Chung, W.K.; Veenstra-VanderWeele, J. Psychotic symptoms in 16p11.2 copy-number variant carriers. Autism. Res. 2020, 13, 187–198. [Google Scholar] [CrossRef]
- Huang, A.Y.; Yu, D.; Davis, L.K.; Sul, J.H.; Tsetsos, F.; Ramensky, V.; Zelaya, I.; Ramos, E.M.; Osiecki, L.; Chen, J.A.; et al. Rare Copy Number Variants in NRXN1 and CNTN6 Increase Risk for Tourette Syndrome. Neuron 2017, 94, 1101–1111.e7. [Google Scholar] [CrossRef] [Green Version]
- Nag, A.; Bochukova, E.G.; Kremeyer, B.; Campbell, D.D.; Muller, H.; Valencia-Duarte, A.V.; Cardona, J.; Rivas, I.C.; Mesa, S.C.; Cuartas, M.; et al. CNV analysis in Tourette syndrome implicates large genomic rearrangements in COL8A1 and NRXN1. PLoS ONE 2013, 8, e59061. [Google Scholar]
- Sundaram, S.K.; Huq, A.M.; Wilson, B.J.; Chugani, H.T. Tourette syndrome is associated with recurrent exonic copy number variants. Neurology 2010, 74, 1583–1590. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Mandell, J.D.; Kumar, Y.; Sun, N.; Morris, M.T.; Arbelaez, J.; Nasello, C.; Dong, S.; Duhn, C.; Zhao, X.; et al. De Novo Sequence and Copy Number Variants Are Strongly Associated with Tourette Disorder and Implicate Cell Polarity in Pathogenesis. Cell Rep. 2018, 24, 3441–3454.e12. [Google Scholar] [CrossRef] [Green Version]
- Willsey, A.J.; Fernandez, T.V.; Yu, D.; King, R.A.; Dietrich, A.; Xing, J.; Sanders, S.J.; Mandell, J.D.; Huang, A.Y.; Richer, P.; et al. De Novo Coding Variants Are Strongly Associated with Tourette Disorder. Neuron 2017, 94, 486–499.e9. [Google Scholar] [CrossRef] [Green Version]
- Mahjani, B.; Dellenvall, K.; Grahnat, A.C.S.; Karlsson, G.; Tuuliainen, A.; Reichert, J.; Mahjani, C.G.; Klei, L.; De Rubeis, S.; Reichenberg, A.; et al. Cohort profile: Epidemiology and Genetics of Obsessive-compulsive disorder and chronic tic disorders in Sweden (EGOS). Soc. Psychiatry Psychiatr. Epidemiol. 2020, 55, 1383–1393. [Google Scholar] [CrossRef] [PubMed]
- Sanders, S.J.; Ercan-Sencicek, A.G.; Hus, V.; Luo, R.; Murtha, M.T.; Moreno-De-Luca, D.; Chu, S.H.; Moreau, M.P.; Gupta, A.R.; Thomson, S.A.; et al. Multiple recurrent de novo CNVs, including duplications of the 7q11.23 Williams syndrome region, are strongly associated with autism. Neuron 2011, 70, 863–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ClinGen Ftp. 2021. Available online: https://ftp.clinicalgenome.org/ (accessed on 6 November 2021).
- DECIPHER v11.10: Mapping the Clinical Genome. 2021. Available online: https://decipher.sanger.ac.uk/disorders/syndromes/list (accessed on 26 February 2022).
- ClinGen Genome Dosage Map. 2021. Available online: https://dosage.clinicalgenome.org/recurrent_region.shtml (accessed on 23 October 2021).
- Mahjani, B.; De Rubeis, S.; Gustavsson Mahjani, C.; Mulhern, M.; Xu, X.; Klei, L.; Satterstrom, F.K.; Fu, J.; Talkowski, M.E.; Reichenberg, A.; et al. Prevalence and phenotypic impact of rare potentially damaging variants in autism spectrum disorder. Mol. Autism. 2021, 12, 65. [Google Scholar] [CrossRef]
- Foa, E.B.; Huppert, J.D.; Leiberg, S.; Langner, R.; Kichic, R.; Hajcak, G.; Salkovskis, P.M. The Obsessive-Compulsive Inventory: Development and validation of a short version. Psychol. Assess. 2002, 14, 485–496. [Google Scholar] [CrossRef]
- Levitas, A.S.; Reid, C.S. Rubinstein-Taybi syndrome and psychiatric disorders. J. Intellect. Disabil. Res. 2002, 42, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Ramalingam, A.; Zhou, X.G.; Fiedler, S.D.; Brawner, S.J.; Joyce, J.M.; Liu, H.Y.; Yu, S. 16p13.11 duplication is a risk factor for a wide spectrum of neuropsychiatric disorders. J. Hum. Genet. 2011, 56, 541–544. [Google Scholar] [CrossRef] [Green Version]
- Bradshaw, N.J.; Ukkola-Vuoti, L.; Pankakoski, M.; Zheutlin, A.B.; Ortega-Alonso, A.; Torniainen-Holm, M.; Sinha, V.; Therman, S.; Paunio, T.; Suvisaari, J.; et al. The NDE1 genomic locus can affect treatment of psychiatric illness through gene expression changes related to microRNA-484. Open Biol. 2017, 7. [Google Scholar] [CrossRef]
- Sinha, V.; Ortega-Alonso, A.; Ukkola-Vuoti, L.; Linnaranta, O.; Zheutlin, A.B.; Torniainen-Holm, M.; Therman, S.; Tuulio-Henriksson, A.; Jylhä, P.; Kaprio, J.; et al. SNP Variants at 16p13.11 Clarify the Role of the NDE1/miR-484 Locus in Major Mental Illness in Finland. Schizophr. Bull Open 2020, 1, sgaa055. Available online: https://academic.oup.com/schizbullopen/article-abstract/1/1/sgaa055/5992279 (accessed on 6 November 2021). [CrossRef]
- Fujitani, M.; Zhang, S.; Fujiki, R.; Fujihara, Y.; Yamashita, T. A chromosome 16p13.11 microduplication causes hyperactivity through dysregulation of miR-484/protocadherin-19 signaling. Mol. Psychiatry 2017, 22, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, N.J.; Hayashi, M.A.F. NDE1 and NDEL1 from genes to (mal)functions: Parallel but distinct roles impacting on neurodevelopmental disorders and psychiatric illness. Cell. Mol. Life Sci. 2017, 74, 1191–1210. [Google Scholar] [CrossRef] [PubMed]
- Isomura, K.; Sidorchuk, A.; Brander, G.; Jernberg, T.; Rück, A.; Song, H.; Valdimarsdóttir, U.A.; Lichtenstein, P.; Larsson, H.; Rück, C.; et al. Risk of specific cardiovascular diseases in obsessive-compulsive disorder. J. Psychiatr. Res. 2021, 135, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Isomura, K.; Brander, G.; Chang, Z.; Kuja-Halkola, R.; Rück, C.; Hellner, C.; Lichtenstein, P.; Larsson, H.; Mataix-Cols, D.; Fernández de la Cruz, L. Metabolic and Cardiovascular Complications in Obsessive-Compulsive Disorder: A Total Population, Sibling Comparison Study With Long-Term Follow-up. Biol. Psychiatry 2018, 84, 324–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allach El Khattabi, L.; Heide, S.; Caberg, J.H.; Andrieux, J.; Doco Fenzy, M.; Vincent-Delorme, C.; Callier, P.; Chantot-Bastaraud, S.; Afenjar, A.; Boute-Benejean, O.; et al. 16p13.11 microduplication in 45 new patients: Refined clinical significance and genotype-phenotype correlations. J. Med. Genet. 2020, 57, 301–307. [Google Scholar] [CrossRef]
- Wat, M.J.; Enciso, V.B.; Wiszniewski, W.; Resnick, T.; Bader, P.; Roeder, E.R.; Freedenberg, D.; Brown, C.; Stankiewicz, P.; Cheung, S.-W.; et al. Recurrent microdeletions of 15q25.2 are associated with increased risk of congenital diaphragmatic hernia, cognitive deficits and possibly Diamond--Blackfan anaemia. J. Med. Genet. 2010, 47, 777–781. [Google Scholar] [CrossRef] [Green Version]
- Cooper, G.M.; Coe, B.P.; Girirajan, S.; Rosenfeld, J.A.; Vu, T.H.; Baker, C.; Williams, C.; Stalker, H.; Hamid, R.; Hannig, V.; et al. A copy number variation morbidity map of developmental delay. Nat. Genet. 2011, 43, 838–846. [Google Scholar] [CrossRef] [Green Version]
- Stein, D.J.; Costa, D.L.C.; Lochner, C.; Miguel, E.C.; Reddy, Y.C.J.; Shavitt, R.G.; van den Heuvel, O.A.; Simpson, H.B. Obsessive-compulsive disorder. Nat. Rev. Dis. Prim. 2019, 5, 52. [Google Scholar] [CrossRef] [Green Version]
- Ferentinos, P.; Preti, A.; Veroniki, A.A.; Pitsalidis, K.G.; Theofilidis, A.T.; Antoniou, A.; Fountoulakis, K.N. Comorbidity of obsessive-compulsive disorder in bipolar spectrum disorders: Systematic review and meta-analysis of its prevalence. J. Affect. Disord. 2020, 263, 193–208. [Google Scholar] [CrossRef]


{kind=link}
| Total (n, %) | Average Diagnosis Age (SD) | Diagnosed < 18 (% of Total) | Diagnosed ≥ 18 (% of Total) | |
|---|---|---|---|---|
| OCD Probands | 993 1 | 21.9 (7.0) | 311 (31%) | 681 (69%) |
| Female | 623 (63%) 2 | 22.0 (6.8) | 178 (29%) | 444 (71%) |
| Male | 370 (37%) 2 | 21.5 (7.4) | 133 (36%) | 237 (64%) |
| CTD Probands | 217 3 | 17.5 (6.9) | 149 (69%) | 67 (31%) |
| Female | 77 (36%) | 17.0 (6.7) | 49 (64%) | 27 (36%) |
| Male | 140 (64%) | 17.8 (7.1) | 100 (71%) | 40 (29%) |
| Probands with pdCNV (%) | Probands with pdCNV and Diagnosed < 18 (% Diagnosed < 18) | Probands with pdCNV and Diagnosed ≥ 18 (% Diagnosed ≥ 18) | |
|---|---|---|---|
| OCD Probands | 86 (9%) | 27 (9%) | 59 (9%) |
| Female | 51 (8%) | 15 (8%) | 36 (8%) |
| Male | 35 (9%) | 12 (9%) | 23 (10%) |
| CTD Probands | 18 (8%) | 13 (9%) | 5 (7%) |
| Female | 8 (10%) | 6 (12%) | 2 (7%) |
| Male | 10 (7%) | 7 (7%) | 3 (8%) |
| ID | Sex | Chromosomal Disorder | OCD, Diagnosis Age | CTD, Diagnosis Age | Co-Occurring Psychiatric Conditions |
|---|---|---|---|---|---|
| 1 | Female | 16p13.3 deletion (includes CREBBP) | Yes, 44 | No | Bipolar disorder |
| 2 | Female | 22q11.2 deletion (Velo-cardio-facial syndrome/DiGeorge syndrome; proximal, A-D; includes TBX1) | Yes, 34 | No | None |
| 3 | Female | 16p13.11 deletion (BP2-BP3; includes MYH11) | No | Yes, 15 | None |
| 4 | Female | 16p11.2 deletion (proximal, BP4-BP5; includes TBX6) | Yes, 24 | No | Major depression, bulimia nervosa, specific (isolated) phobias |
| 5 | Male | 15q25.2 deletion (LCR B-C, proximal) | Yes, 14 | Yes, 14 | Asperger’s syndrome |
| 6 | Male | 1q21.1 deletion (BP3-BP4, distal; includes GJA5) | Yes, 23 | No | None |
| 7 | Female | 17q12 duplication (RCAD syndrome; includes HNF1B) | No, 24 | Yes | Agoraphobia with panic disorder |
| 8 | Male | 22q11.2 duplication (DGS/VCFS; proximal, A-D; includes TBX1) | Yes, 18 | No | None |
| 9 | Male | 5q35 duplication (Sotos syndrome; includes NSD1) | Yes, 17 | No | ADHD, Asperger’s syndrome |
| 10 | Female | Xq28 duplication (int22h1/int22h2-flanked; includes RAB39B) | Yes, 31 | No | Specific (isolated) phobias |
| 11 | Female | Xq28 duplication (int22h1/int22h2-flanked; includes RAB39B) | Yes, 13 | No | None |
| 12 * | Female | 16p13.11 recurrent microduplication (neurocognitive disorder susceptibility locus) | Yes, 23 | No | Major depression, bulimia nervosa |
| 13 * | Male | 16p13.11 recurrent microduplication (neurocognitive disorder susceptibility locus) | Yes, 33 | No | None |
| Co-Occurring Psychiatric Condition | OCD Probands 1 | CTD Probands 2 | OCD with CTD Probands | |||
|---|---|---|---|---|---|---|
| Total (%) 3 | With pdCNV (%) 4 | Total (%) 3 | With pdCNV (%) 4 | Total (%) 3 | With pdCNV (%) 4 | |
| ADHD | 69 (7%) | 6 (9%) | 58 (27%) | 3 (5%) | 32 (35%) | 2 (6%) |
| Anxiety disorders 5 | 216 (22%) | 15 (7%) | 29 (13%) | 3 (10%) | 18 (20%) | 1 (5%) |
| ASD | 48 (5%) | 7 (15%) | 26 (12%) | 5 (19%) | 14 (15%) | 3 (21%) |
| Bipolar disorder | 32 (3%) | 4 (13%) | 3 (1%) | 0 (0%) | 2 (2%) | 0 (0%) |
| Borderline personality disorder | 19 (2%) | 0 (0%) | 1 (<1%) | - | 1 (1%) | 0 (0%) |
| Eating disorders | 49 (5%) | 3 (6%) | 5 (2%) | 0 (0%) | 3 (3%) | 0 (0%) |
| Major depression | 199 (20%) | 13 (7%) | 36 (17%) | 3 (8%) | 22 (24%) | 2 (9%) |
| Schizophrenia | 8 (<1%) | 0 (0%) | 0 (0%) | - | 0 (0%) | - |
| All Probands | Diagnosed < 18 | Diagnosed ≥ 18 | ||||
|---|---|---|---|---|---|---|
| Total | Carriers of pdCNV (%) | Total | Carriers of pdCNV (%) | Total | Carriers of pdCNV (%) | |
| OCD probands without CTD | ||||||
| No co-occurring psychiatric condition | 578 | 52 (9%) | 174 | 17 (10%) | 404 | 35 (9%) |
| At least one co-occurring psychiatric condition | 324 | 26 (8%) | 78 | 4 (5%) | 246 | 22 (9%) |
| CTD probands without OCD | ||||||
| No psychiatric co-occurring psychiatric condition | 78 | 6 (8%) | 50 | 3 (6%) | 28 | 3 (11%) |
| At least one co-occurring psychiatric condition | 48 | 4 (8%) | 29 | 3 (10%) | 19 | 1 (5%) |
| Phenotypes | OCD Probands | CTD Probands | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| ADHD | 0.97 | (0.36,2.16) | 0.94 | 0.54 | (0.12,1.71) | 0.34 |
| Anxiety disorders | 0.75 | (0.41,1.30) | 0.33 | 1.26 | (0.28,4.18) | 0.74 |
| ASD | 1.80 | (0.71,3.98) | 0.17 | 3.46 | (1.02,10.30) | 0.03 * |
| Bipolar disorder | 1.30 | (0.31,3.82) | 0.67 | - | - | - |
| Eating disorders | 0.71 | (0.17,2.04) | 0.58 | - | - | - |
| Major depression | 0.70 | (0.36,1.24) | 0.25 | 0.99 | (0.22,3.22) | 0.99 |
| Intercept | pdCNV | TimeD | Sex | pdCNV × TimeD | Marginal Mean without pdCNV n = 502 | Marginal Means with pdCNV n = 49 | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean | 95% CI | Mean | 95% CI | ||||||
| Total score | 28.2 * | −4.6 | −1.2 * | 2.1 | 0.99 | 21.5 | (20.3,22.7) | 23.6 | (19.8,27.4) |
| Washing | 5.5 * | 1.3 | −0.3 * | 0.8 * | −0.08 | 3.8 | (3.5,4.1) | 4.6 | (3.6,5.6) |
| Obsessing | 6.4 * | −1.2 | −0.2 * | 0.2 | 0.2 | 3.8 | (3.5,4.1) | 4.6 | (3.6,5.6) |
| Hoarding | 2.7 * | −0.2 | −0.1 * | −0.2 | 0.1 | 2.0 | (1.7,2.2) | 2.2 | (1.5,2.9) |
| Ordering | 4.8 * | −3.2* | −0.2 * | 0.6 * | 0.6 * | 3.7 | (3.4,4.0) | 4.2 | (3.2,5.1) |
| Checking | 5.2 * | −3.3* | −0.2 * | 0.5 | 0.5 * | 4.2 | (3.8,4.4) | 4.2 | (3.3,5.2) |
| Neutralizing | 3.7 * | 2.0 | −0.2 * | 0.2 | −0.2 | 2.7 | (2.4,3.0) | 3.1 | (2.1,4.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahjani, B.; Birnbaum, R.; Buxbaum Grice, A.; Cappi, C.; Jung, S.; Avila, M.N.; Reichenberg, A.; Sandin, S.; Hultman, C.M.; Buxbaum, J.D.; et al. Phenotypic Impact of Rare Potentially Damaging Copy Number Variation in Obsessive-Compulsive Disorder and Chronic Tic Disorders. Genes 2022, 13, 1796. https://doi.org/10.3390/genes13101796
Mahjani B, Birnbaum R, Buxbaum Grice A, Cappi C, Jung S, Avila MN, Reichenberg A, Sandin S, Hultman CM, Buxbaum JD, et al. Phenotypic Impact of Rare Potentially Damaging Copy Number Variation in Obsessive-Compulsive Disorder and Chronic Tic Disorders. Genes. 2022; 13(10):1796. https://doi.org/10.3390/genes13101796
Chicago/Turabian StyleMahjani, Behrang, Rebecca Birnbaum, Ariela Buxbaum Grice, Carolina Cappi, Seulgi Jung, Marina Natividad Avila, Abraham Reichenberg, Sven Sandin, Christina M. Hultman, Joseph D. Buxbaum, and et al. 2022. "Phenotypic Impact of Rare Potentially Damaging Copy Number Variation in Obsessive-Compulsive Disorder and Chronic Tic Disorders" Genes 13, no. 10: 1796. https://doi.org/10.3390/genes13101796