
Predominance of the Rare EGFR Mutation p.L861Q in Tunisian Patients with Non-Small Cell Lung Carcinoma

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Samples
2.2. DNA Extraction and PCR Amplification
2.3. Pyrosequencing Analysis
2.4. Statistical Analysis
3. Results
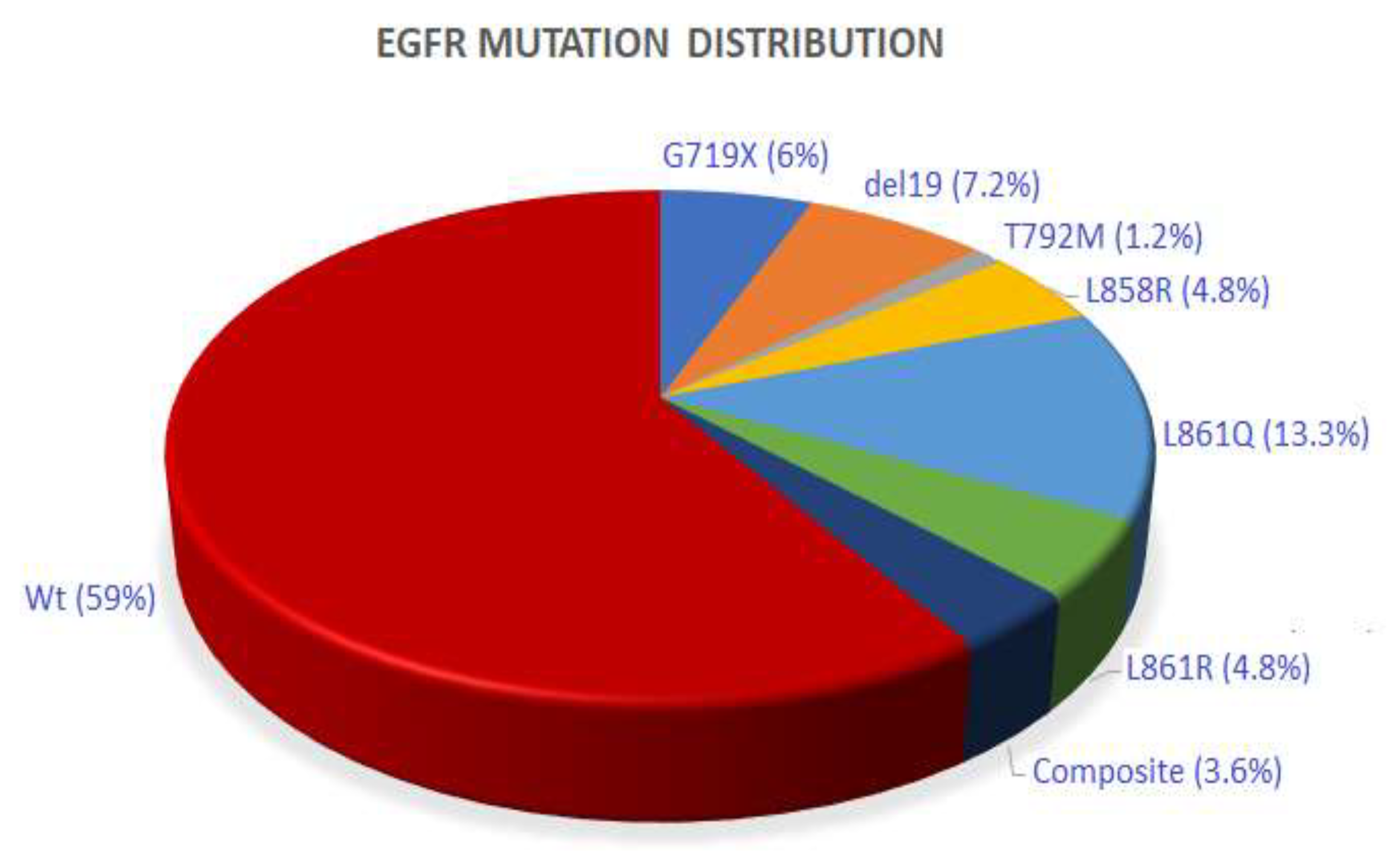
3.1. EGFR and BRAF Mutation Analysis
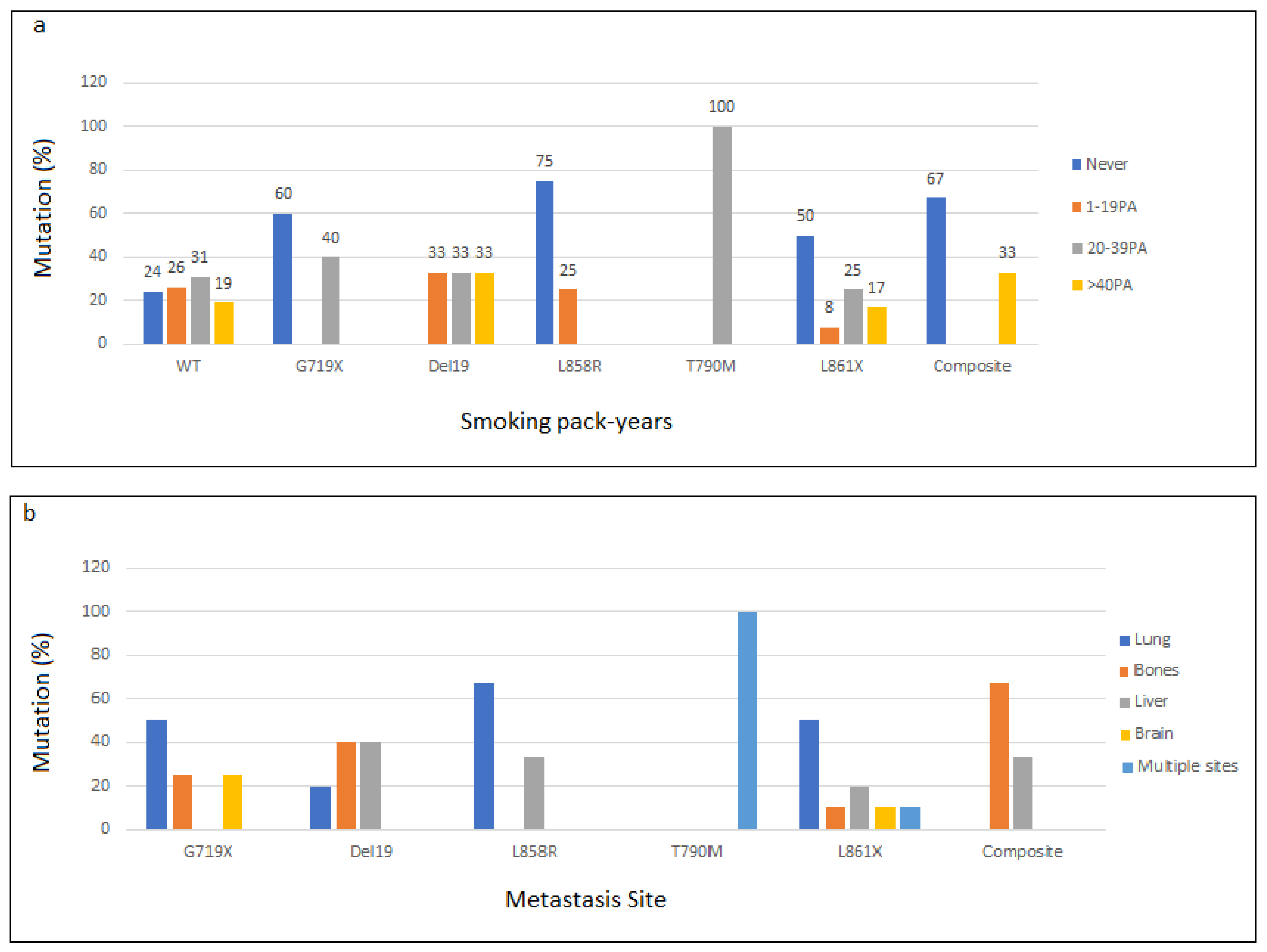
3.2. EGFR Mutations and Clinicopathological Features
3.3. EGFR and BRAF Mutations and Therapy

4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| EGFR | Epithelial Growth Factor Receptor |
| TKI | Tyrosine Kinase Inhibitors |
| NSCLC | Non-Small-Cell Lung Carcinoma |
| FFPE | Formalin-Fixed Paraffin-Embedded |
| ErbB2 | Erb-B2 Receptor Tyrosine Kinase 2 |
| MAPK | Mitogen-Activated Protein Kinases |
| WHO | World Health Organization |
| PA | pack years |
| IHC | Immunohistochemistry |
| Wt | Wild type |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ayed, H.; Hsairi, M.; Yaich, S.; Feki, H.; Jedidi, R.; Karray, J.; Kassis, M.; Damak, J. National Burden of Cancers in Tunisia: A Disability Adjusted Life—Year Approach. Dr. Sulaiman Al Habib Med. J. 2020, 2, 115–122. [Google Scholar] [CrossRef]
- Casal-Mouriño, A.; Ruano-Ravina, A.; Lorenzo-González, M.; Rodríguez-Martínez, Á.; Giraldo-Osorio, A.; Varela-Lema, L.; Pereiro-Brea, T.; Barros-Dios, J.M.; Valdés-Cuadrado, L.; Pérez-Ríos, M. Epidemiology of stage III lung cancer: Frequency, diagnostic characteristics, and survival. Transl. Lung Cancer Res. 2021, 10, 506–518. [Google Scholar] [CrossRef] [PubMed]
- Rusch, V.; Baselga, J.; Cordon-Cardo, C.; Orazem, J.; Zaman, M.; Hoda, S.; McIntosh, J.; Kurie, J.; Dmitrovsky, E. Differential expression of the epidermal growth factor receptor and its ligands in primary non-small cell lung cancers and adjacent benign lung. Cancer Res. 1993, 53 (Suppl. 10), 2379–2385. [Google Scholar] [PubMed]
- Rusch, V.; Klimstra, D.; Venkatraman, E.; Pisters, P.W.; Langenfeld, J.; Dmitrovsky, E. Overexpression of the epidermal growth factor receptor and its ligand transforming growth factor alpha is frequent in resectable non-small cell lung cancer but does not predict tumor progression. Clin. Cancer Res. 1997, 3, 515–522. [Google Scholar]
- Brabender, J.; Danenberg, K.D.; Metzger, R.; Schneider, P.M.; Park, J.; Salonga, D.; Hölscher, A.H.; Danenberg, P.V. Epidermal growth factor receptor and HER2-neu mRNA expression in non-small cell lung cancer Is correlated with survival. Clin. Cancer Res. 2001, 7, 1850–1855. [Google Scholar] [PubMed]
- Arteaga, C. ErbB-targeted therapeutic approaches in human cancer. Exp. Cell Res. 2003, 284, 122–130. [Google Scholar] [CrossRef]
- Hirsch, F.R.; Scagliotti, G.V.; Langer, C.J.; Varella-Garcia, M.; Franklin, W.A. Epidermal growth factor family of receptors in preneoplasia and lung cancer: Perspectives for targeted therapies. Lung Cancer 2003, 41 (Suppl. 1), 29–42. [Google Scholar] [CrossRef]
- Guo, G.; Gong, K.; Wohlfeld, B.; Hatanpaa, K.J.; Zhao, D.; Habib, A.A. Ligand-Independent EGFR Signaling. Cancer Res. 2015, 75, 3436–3441. [Google Scholar] [CrossRef] [Green Version]
- Tsao, A.S.; Tang, X.M.; Sabloff, B.; Xiao, L.; Shigematsu, H.; Roth, J.; Spitz, M.; Hong, W.K.; Gazdar, A.; Wistuba, I. Clinicopathologic characteristics of the EGFR gene mutation in non-small cell lung cancer. J. Thorac. Oncol. 2006, 1, 231–239. [Google Scholar] [CrossRef] [Green Version]
- Shigematsu, H.; Gazdar, A.F. Somatic mutations of epidermal growth factor receptor signaling pathway in lung cancers. Int. J. Cancer 2006, 118, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Nan, X.; Xie, C.; Yu, X.; Liu, J. EGFR TKI as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer. Oncotarget 2017, 8, 75712–75726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shigematsu, H.; Lin, L.; Takahashi, T.; Nomura, M.; Suzuki, M.; Wistuba, I.I.; Fong, K.M.; Lee, H.; Toyooka, S.; Shimizu, N.; et al. Clinical and biological features associated with epidermal growth factor receptor gene mutations in lung cancers. J. Natl. Cancer Inst. 2005, 97, 339–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvo, E.; Baselga, J. Ethnic differences in response to epidermal growth factor receptor tyrosine kinase inhibitors. J. Clin. Oncol. 2006, 24, 2158–2163. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.V.; Bell, D.W.; Settleman, J.; Haber, D.A. Epidermal growth factor receptor mutations in lung cancer. Nat. Rev. Cancer 2007, 7, 169–181. [Google Scholar] [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Spanish Lung Cancer Group in collaboration with Groupe Français de Pneumo-Cancérologie and Associazione Italiana Oncologia Toracica. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar]
- Zhou, C.; Wu, Y.L.; Chen, G.; Feng, J.; Liu, X.Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef]
- Mitsudomi, T.; Morita, S.; Yatabe, Y.; Negoro, S.; Okamoto, I.; Tsurutani, J.; Seto, T.; Satouchi, M.; Tada, H.; Hirashima, T.; et al. West Japan Oncology Group. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): An open label, randomised phase 3 trial. Lancet Oncol. 2010, 11, 121–128. [Google Scholar] [CrossRef]
- Davies, H.; Bignell, G.R.; Cox, C.; Stephens, P.; Edkins, S.; Clegg, S.; Teague, J.; Woffendin, H.; Garnett, M.J.; Bottomley, W.; et al. Mutations of the BRAF gene in human cancer. Nature 2002, 417, 949–954. [Google Scholar] [CrossRef]
- Pendharkar, D.; Ausekar, B.V.; Gupta, S. Molecular biology of lung cancer-a review. Indian. J. Surg. Oncol. 2013, 4, 120–124. [Google Scholar]
- Sosman, J.A.; Kim, K.B.; Schuchter, L.; Gonzalez, R.; Pavlick, A.C.; Weber, J.S.; McArthur, G.A.; Hutson, T.E.; Moschos, S.J.; Flaherty, K.T.; et al. Survival in BRAF V600-mutant advanced melanoma treated with vemurafenib. N. Engl. J. Med. 2012, 366, 707–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tol, J.; Nagtegaal, I.D.; Punt, C.J. BRAF mutation in metastatic colorectal cancer. N. Engl. J. Med. 2009, 361, 98–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pao, W.; Girard, N. New driver mutations in non-small-cell lung cancer. Lancet Oncol. 2011, 12, 175–180. [Google Scholar] [CrossRef]
- Planchard, D.; Kim, T.M.; Mazieres, J.; Quoix, E.; Riely, G.; Barlesi, F.; Souquet, P.J.; Smit, E.F.; Groen, H.J.; Kelly, R.J.; et al. Dabrafenib in patients with BRAF(V600E)-positive advanced non-small-cell lung cancer: A single-arm, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 642–650. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Smit, E.F.; Groen, H.J.M.; Mazieres, J.; Besse, B.; Helland, Å.; Giannone, V.; D’Amelio, A.M., Jr.; Zhang, P.; Mookerjee, B.; et al. Dabrafenib plus trametinib in patients with previously untreated BRAF V600E -mutant metastatic non-small-cell lung cancer: An open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1307–1316. [Google Scholar] [CrossRef]
- Mraihi, Z.; Ben Amar, J.; Bouacha, H.; Rammeh, S.; Hila, L. EGFR mutation status in Tunisian non-small-cell lung cancer patients evaluated by mutation-specific immunohistochemistry. BMC Pulm. Med. 2018, 18, 132. [Google Scholar] [CrossRef] [Green Version]
- Dhieb, D.; Belguith, I.; Capelli, L.; Chiadini, E.; Canale, M.; Bravaccini, S.; Yangui, I.; Boudawara, O.; Jlidi, R.; Boudawara, T.; et al. Analysis of Genetic Alterations in Tunisian Patients with Lung Adenocarcinoma. Cells 2019, 8, 514. [Google Scholar] [CrossRef] [Green Version]
- Mezni, F.; Mlika, M.; Boussen, H.; Ghedira, H.; Fenniche, S.; Faten, T.; Loriot, M.A. About molecular profile of lung cancer in Tunisian patients. J. Immunoass. Immunochem. 2018, 39, 99–107. [Google Scholar] [CrossRef]
- Arfaoui Toumi, A.; Blel, A.; Aloui, R.; Zaibi, H.; Ksentinini, M.; Boudaya, M.S.; Znaidi, N.; Zidi, Y.; Aouina, H.; Rammeh Rommani, S. Assessment of EGFR mutation status in Tunisian patients with pulmonary adenocarcinoma. Curr. Res. Transl. Med. 2018, 66, 65–70. [Google Scholar] [CrossRef]
- Graham, R.P.; Treece, A.L.; Lindeman, N.I.; Vasalos, P.; Shan, M.; Jennings, L.J.; Rimm, D.L. Worldwide Frequency of Commonly Detected EGFR Mutations. Arch. Pathol. Lab. Med. 2018, 142, 163–167. [Google Scholar] [CrossRef] [Green Version]
- Melosky, B.; Kambartel, K.; Häntschel, M.; Bennetts, M.; Nickens, D.J.; Brinkmann, J.; Kayser, A.; Moran, M.; Cappuzzo, F. Worldwide Prevalence of Epidermal Growth Factor Receptor Mutations in Non-Small Cell Lung Cancer: A Meta-Analysis. Mol. Diagn. Ther. 2022, 26, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.L.; Yuan, J.Q.; Wang, K.F.; Fu, X.H.; Han, X.R.; Threapleton, D.; Yang, Z.Y.; Mao, C.; Tang, J.L. The prevalence of EGFR mutation in patients with non-small cell lung cancer: A systematic review and meta-analysis. Oncotarget 2016, 7, 78985–78993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Midha, A.; Dearden, S.; McCormack, R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: A systematic review and global map by ethnicity (mutMapII). Am. J. Cancer Res. 2015, 5, 2892–2911. [Google Scholar] [PubMed]
- Benbrahim, Z.; Antonia, T.; Mellas, N. EGFR mutation frequency in Middle East and African non-small cell lung cancer patients: A systematic review and meta-analysis. BMC Cancer 2018, 18, 891. [Google Scholar] [CrossRef] [PubMed]
- Lemine Sow, M.; El Yacoubi, H.; Moukafih, B.; Balde, S.; Akimana, G.; Najem, S.; El Khoyaali, S.; Abahssain, H.; Chaibi, A.; Zeb Khan, S.; et al. Frequency and types of EGFR mutations in Moroccan patients with non-small cell lung cancer. Tumori 2021, 107, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Lahmadi, M.; Beddar, L.; Rouibah, A.L.; Boumegoura, A.; Boufendi, H.; Temim, A.; Nini, A.; Sellam, F.; Satta, D. Analysis of EGFR Mutation Status in Algerian Patients with Non-Small Cell Lung Cancer. Asian Pac. J. Cancer Prev. 2021, 22, 1063–1068. [Google Scholar] [CrossRef]
- John, T.; Taylor, A.; Wang, H.; Eichinger, C.; Freeman, C.; Ahn, M.J. Uncommon EGFR mutations in non-small-cell lung cancer: A systematic literature review of prevalence and clinical outcomes. Cancer Epidemiol. 2022, 76, 102080. [Google Scholar] [CrossRef]
- Chiu, C.H.; Yang, C.T.; Shih, J.Y.; Huang, M.S.; Su, W.C.; Lai, R.S.; Wang, C.C.; Hsiao, S.H.; Lin, Y.C.; Ho, C.L. Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitor Treatment Response in Advanced Lung Adenocarcinomas with G719X/L861Q/S768I Mutations. J. Thorac. Oncol. 2015, 10, 793–799. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Wang, Z.; Liu, Q.; Wu, G.; Chu, C.; Li, L.; An, L.; Duan, S. Sensitivity analysis of EGFR L861Q mutation to six tyrosine kinase inhibitors. Clin. Transl. Oncol. 2022. accepted. [Google Scholar] [CrossRef]
- Yang, J.C.; Sequist, L.V.; Geater, S.L.; Tsai, C.M.; Mok, T.S.; Schuler, M.; Yamamoto, N.; Yu, C.J.; Ou, S.H.; Zhou, C.; et al. Clinical activity of afatinib in patients with advanced non-small-cell lung cancer harbouring uncommon EGFR mutations: A combined post-hoc analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6. Lancet Oncol. 2015, 16, 830–838. [Google Scholar] [CrossRef]
- Iida, Y.; Kumasawa, F.; Shimizu, T.; Shintani, Y.; Takahashi, N.; Gon, Y. Successful treatment of an elderly patient with an uncommon L861Q epidermal growth factor receptor mutation with low-dose afatinib: A case report. Thorac Cancer 2020, 11, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.Y.; Cho, E.N.; Park, H.S.; Hong, J.Y.; Lim, S.; Youn, J.P.; Hwang, S.Y.; Chang, Y.S. Compound EGFR mutation is frequently detected with co-mutations of actionable genes and associated with poor clinical outcome in lung adenocarcinoma. Cancer Biol. Ther. 2016, 17, 237–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, S.; Canepa, H.M.; Bailey, A.S.; Nakayama, S.; Yamaguchi, N.; Goldstein, M.A.; Huberman, M.S.; Costa, D.B. Compound EGFR mutations and response to EGFR tyrosine kinase inhibitors. J. Thorac. Oncol. 2013, 8, 45–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.Y.; Yu, C.J.; Chang, Y.C.; Yang, C.H.; Shih, J.Y.; Yang, P.C. Effectiveness of tyrosine kinase inhibitors on “uncommon” epidermal growth factor receptor mutations of unknown clinical significance in non-small cell lung cancer. Clin. Cancer Res. 2011, 17, 3812–3821. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Wu, Y.; Wu, F.; Hu, C. Lung adenocarcinoma harboring triple rare EGFR exon18 mutations rapidly developed resistance to multiple therapies. Chemotherapy 2022. accepted. [Google Scholar] [CrossRef]
- Sheikine, Y.; Pavlick, D.; Klempner, S.J.; Trabucco, S.E.; Chung, J.H.; Rosenzweig, M.; Wang, K.; Velcheti, V.; Frampton, G.M.; Peled, N. BRAF in Lung Cancers: Analysis of Patient Cases Reveals Recurrent BRAF Mutations, Fusions, Kinase Duplications, and Concurrent Alterations. JCO. Precis. Oncol. 2018, 2, PO.17.00172. [Google Scholar] [CrossRef]
- Litvak, A.M.; Paik, P.K.; Woo, K.M.; Sima, C.S.; Hellmann, M.D.; Arcila, M.E.; Ladanyi, M.; Rudin, C.M.; Kris, M.G.; Riely, G.J. Clinical characteristics and course of 63 patients with BRAF mutant lung cancers. J. Thorac. Oncol. 2014, 9, 1669–1674. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Zhang, L.Q.; Huang, J.F.; Liu, K.; Chuai, Z.R.; Yang, Z.; Wang, Y.X.; Shi, D.C.; Liu, Q.; Huang, Q.; et al. BRAF mutations in patients with non-small cell lung cancer: A systematic review and meta-analysis. PLoS ONE 2014, 9, e101354. [Google Scholar] [CrossRef] [Green Version]
- Cui, G.; Liu, D.; Li, W.; Fu, X.; Liang, Y.; Li, Y.; Shi, W.; Chen, X.; Zhao, S. A meta-analysis of the association between BRAF mutation and nonsmall cell lung cancer. Med. Baltim. 2017, 96, e6552. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Patients’ Characteristics | Number (%) |
|---|---|
| Total | 79 |
| Age (Years) | 69 |
| Median | 59.54 |
| Range | 24–85 |
| Gender | 79 |
| Male | 65 (82.27) |
| Female | 14 (17.72) |
| Smoking history | 69 |
| Never-smoker | 24 (34.78) |
| Former/current smoker | 44 (61.21) |
| Histological Type | 56 |
| Adenocarcinoma | 51 (91.07) |
| epidermoid carcinoma | 4 (7.14) |
| Pleomorphic carcinoma | 1(1.78) |
| Metastasis | 69 |
| Absence | 48 (69.56) |
| Presence | 21 (30.43) |
| Patient | Gender | Age | EGFR Alteration | Metastasis | Smoking History | Therapy | Status | Survival (Months) |
|---|---|---|---|---|---|---|---|---|
| P3 | M | 60 | p.L861Q | Lymph nodes | 30 PA | Chemotherapy | dead | 37 |
| P4 | M | 46 | p.T790M | Liver, Bones | 20 PA | - | - | - |
| P27 | F | 65 | p.L861Q | Lung | No | Chemotherapy + Erlotinib | alive | 40 |
| P34 | M | 72 | p.L861R | No | 25 PA | Chemotherapy | dead | 18 |
| P35 | M | - | p.L861R | No | 30 PA | - | - | - |
| P36 | M | 50 | p.E746_A750del/p.L861R | Bones | 40 PA | Erlotinib | alive | 15 |
| P37 | M | 60 | p.G719S | Brain | No | Chemotherapy | dead | 35 |
| P40 | M | 72 | p.G719A | Lung | No | - | - | - |
| P42 | M | 63 | p.E746_A750del | Bones | 60 PA | Chemotherapy | alive | 17 |
| P104 | M | - | p.L861Q | - | 20 PA | - | - | - |
| P105 | M | - | p.E746_A750del | Liver | 40 PA | - | - | - |
| P106 | F | - | p.E746_S752>V/p.S768I | Bones | No | - | - | - |
| P109 | F | - | p.E746_T751>I | Bones | 10 PA | - | - | - |
| P112 | M | - | p.L861R | Brain | 50 PA | - | - | - |
| P117 | F | - | p.L747_T751del | Bones | 15 PA | - | - | - |
| P120 | M | 66 | p.G719A/p. L861Q | Liver | No | - | - | - |
| P121 | M | 51 | p.L858R | Lung | No | - | - | - |
| P125 | M | 54 | p.E746_A750del | Lung | 30 PA | - | - | - |
| P128 | M | p.L858R | Liver | No | - | - | - | |
| P134 | M | 67 | p.L861Q | No | No | - | - | - |
| P135 | M | 54 | p.G719C | No | 40 PA | - | - | - |
| P136 | M | 76 | p.E746_A750del | No | 20 PA | Surgery | alive | 7 |
| P137 | F | 63 | p. L861Q | No | No | - | - | |
| P139 | M | 64 | p. G719C | Adrenal | 40 PA | Chemotherapy | alive | 18 |
| P140 | M | 66 | p. L861Q | Bones | Unknown | Chemotherapy + Erlotinib | dead | 1 |
| P145 | M | 59 | p.L858R | No | 50 PA | * | dead | 3 |
| P146 | F | 48 | p.G719A | Bones | No | * | dead | 4 |
| P148 | F | 70 | p. L861Q | No | No | - | - | - |
| P149 | F | 60 | p. L861R | No | No | Erlotinib | alive | 3 |
| P150 | M | 62 | p. L861Q | No | No | - | - | - |
| P156 | M | 62 | p. L861Q | Liver | 40 PA | - | - | - |
| P157 | M | 54 | p. L861Q | Liver | No | Erlotinib | alive | 2 |
| P158 | M | 56 | p. L861Q | Liver | 30 PA | - | - | - |
| P160 | F | 75 | p. L858R | Bones | No | Erlotinib | alive | 2 |
| Clinical Feature | Overall | Mutation (%) | Wt (%) | p-Value | |
|---|---|---|---|---|---|
| Gender | M | 65 (82.27) | 24 (36.9) | 41 (63.1) | 0.019 |
| F | 14 (17.72) | 10 (71.4) | 4 (28.6) | ||
| Age | <60 | 26 (32.91) | 10 (38.5) | 16 (61.5) | 0.307 |
| >60 | 33 (41.7) | 16 (48.5) | 17 (51.5) | ||
| Unknown | 20 (25.31) | 8 (40) | 12 (60) | ||
| Smoking History | Smoker | 45 (56.6) | 15 (33.3) | 30 (66.7) | 0.008 |
| Non-smoker | 24 (31.3) | 16 (61.5) | 10 (38.5) | ||
| Unknown | 10 (12) | 3 (30%) | 7 (70%) | ||
| Histological subtype | Adenocarcinoma | 51 (64.55) | 21 (41.2) | 30 (58.8) | 0.646 |
| Other subtypes | 5 (6.32) | 4 (80) | 1 (20) | ||
| Unknown | 23 (29.11) | 9 (39.1) | 14 (60.9) | ||
| Metastasis | Presence | 48 (60.75) | 26 (54.2) | 22 (45.8) | 0.044 |
| Absence | 21 (26.58) | 6 (28.6) | 15 (71.4) | ||
| Unknown | 10 (12) | 2 (20) | 8 (80) | ||
| Patient | EGFR Alteration | Therapy | Response to Therapy Protocol | Status | Survival (Months) |
|---|---|---|---|---|---|
| P3 | p.L861Q | Chemotherapy | Good response to chemotherapy then metastasis | died | 37 |
| P27 | p.L861Q | Chemotherapy + Erlotinib | Complete remission | alive | 40 |
| P34 | p.L861R | Chemotherapy | Bad response to chemotherapy | died | 18 |
| P36 | p.E746_A750del/p.L861R | Erlotinib | 63% tumor regression then resumption of tumor progression | alive | 15 |
| P37 | p.G719S | Chemotherapy | Bad response to chemotherapy | died | 35 |
| P42 | p.E746_A750del | Chemotherapy | Good response to chemotherapy | alive | 17 |
| P136 | p.E746_A750del | Surgery | No treatment | alive | 7 |
| P139 | p. G719C | Chemotherapy | Good response to chemotherapy | alive | 18 |
| P140 | p. L861Q | Chemotherapy + Erlotinib | Chemotherapy then 2 weeks of erlotinib, died of interstitial lung disease | died | 1 |
| P149 | p. L861R | Erlotinib | Treated for 1 month | alive | 3 |
| P157 | p. L861Q | Erlotinib | Treated for 2 months | alive | 2 |
| P160 | p. L858R | Erlotinib | Treated for 1 month and 2 weeks | alive | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdelmaksoud-Dammak, R.; Ammous-Boukhris, N.; Saadallah-Kallel, A.; Charfi, S.; Khemiri, S.; Khemakhem, R.; Kallel, N.; Ben Kridis-Rejeb, W.; Sallemi-Boudawara, T.; Khanfir, A.; et al. Predominance of the Rare EGFR Mutation p.L861Q in Tunisian Patients with Non-Small Cell Lung Carcinoma. Genes 2022, 13, 1499. https://doi.org/10.3390/genes13081499
Abdelmaksoud-Dammak R, Ammous-Boukhris N, Saadallah-Kallel A, Charfi S, Khemiri S, Khemakhem R, Kallel N, Ben Kridis-Rejeb W, Sallemi-Boudawara T, Khanfir A, et al. Predominance of the Rare EGFR Mutation p.L861Q in Tunisian Patients with Non-Small Cell Lung Carcinoma. Genes. 2022; 13(8):1499. https://doi.org/10.3390/genes13081499
Chicago/Turabian StyleAbdelmaksoud-Dammak, Rania, Nihel Ammous-Boukhris, Amèna Saadallah-Kallel, Slim Charfi, Souhir Khemiri, Rim Khemakhem, Nesrin Kallel, Wala Ben Kridis-Rejeb, Tahya Sallemi-Boudawara, Afef Khanfir, and et al. 2022. "Predominance of the Rare EGFR Mutation p.L861Q in Tunisian Patients with Non-Small Cell Lung Carcinoma" Genes 13, no. 8: 1499. https://doi.org/10.3390/genes13081499