
Low JAK2 V617F Allele Burden in Ph-Negative Chronic Myeloproliferative Neoplasms Is Associated with Additional CALR or MPL Gene Mutations

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Baxter, E.J.; Scott, L.M.; Campbell, P.J.; East, C.; Fourouclas, N.; Swanton, S.; Vassiliou, G.S.; Bench, A.J.; Boyd, E.M.; Curtin, N.; et al. Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Lancet 2005, 365, 1054–1056. [Google Scholar] [CrossRef]
- Rowley, J.D. Letter: A new consistent chromosomal abnormality in chronic myelogenous leukemia identified by quinacrine fluorescence and Giemsa staining. Nature 1973, 243, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Konopka, J.; Witte, O. Activation of the c-abl oncogene by viral transduction or chromosomal translocation generates altered c-abl proteins with similar in vitro kinase properties. Mol. Cell. Biol. 1985, 5, 204–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, D.J.; Melo, J.V. Cytogenetic and Molecular Genetic Aspects of Chronic Myeloid Leukaemia. Acta Haematol. 2002, 108, 180–202. [Google Scholar] [CrossRef]
- Greiner, J.; Schmitt, M. Current status of peptide vaccines for cancer immunotherapy in malignant myeloid diseases. Memo 2008, 1, 223–226. [Google Scholar] [CrossRef]
- Levine, R.L.; Wadleigh, M.; Cools, J.; Ebert, B.L.; Wernig, G.; Huntly, B.J.; Boggon, T.J.; Wlodarska, I.; Clark, J.J.; Moore, S.; et al. Activating mutation in the tyrosine kinase JAK2 in polycythemia vera, essential thrombocythemia and myeloid metaplasia with myelofibrosis. Cancer Cell 2005, 7, 387–397. [Google Scholar] [CrossRef] [Green Version]
- James, C.E.; Ugo, V.; Le Couédic, J.-P.; Staerk, J.; Delhommeau, F.; Lacout, C.; Garçon, L.; Raslova, H.; Berger, R.; Bennaceur-Griscelli, A.; et al. A unique clonal JAK2 mutation leading to constitutive signaling causes polycythaemia vera. Nature 2005, 434, 1144–1148. [Google Scholar] [CrossRef]
- Kralovics, R.; Passamonti, F.; Buser, A.S.; Teo, S.-S.; Tiedt, R.; Passweg, J.R.; Tichelli, A.; Cazzola, M.; Skoda, R.C. A gain-of-function mutation of JAK2 in myeloproliferative disorders. N. Engl. J. Med. 2005, 352, 1779–1790. [Google Scholar] [CrossRef] [Green Version]
- Tefferi, A.; Sirhan, S.; Lasho, T.L.; Schwager, S.M.; Li, C.-Y.; Dingli, D.; Wolanskyj, A.P.; Steensma, D.P.; Mesa, R.; Gilliland, D.G. Concomitant neutrophil JAK2 mutation screening and PRV-1 expression analysis in myeloproliferative disorders and secondary polycythaemia. Br. J. Haematol. 2005, 131, 166–171. [Google Scholar] [CrossRef]
- Tutaeva, V.; Misurin, A.V.; Michiels, J.J.; Rozenberg, J.M.; Sokolova, M.A.; Ivanova, V.L.; Kolosheinova, T.I.; Manakova, T.E.; Levina, A.A.; Semenova, E.A.; et al. Application of PRV-1 mRNA expression level and JAK2V617F mutation for the differentiating between polycytemia vera and secondary erythrocytosis and assessment of treatment by interferon or hydroxyurea. Hematology 2007, 12, 473–479. [Google Scholar] [CrossRef]
- Scott, L.M.; Tong, W.; Levine, R.L.; Scott, M.A.; Beer, P.A.; Stratton, M.R.; Futreal, P.A.; Erber, W.N.; McMullin, M.F.; Harrison, C.N.; et al. JAK2 Exon 12 Mutations in Polycythemia Vera and Idiopathic Erythrocytosis. N. Engl. J. Med. 2007, 356, 459–468. [Google Scholar] [CrossRef] [Green Version]
- Passamonti, F.; Elena, C.; Schnittger, S.; Skoda, R.C.; Green, A.R.; Girodon, F.; Kiladjian, J.J.; McMullin, M.F.; Ruggeri, M.; Besses, C.; et al. Molecular and clinical features of the myeloproliferative neoplasm associated with JAK2 exon 12 mutations. Blood 2011, 117, 2813–2816. [Google Scholar] [CrossRef] [Green Version]
- Pikman, Y.; Lee, B.H.; Mercher, T.; McDowell, E.; Ebert, B.L.; Gozo, M.; Cuker, A.; Wernig, G.; Moore, S.; Galinsky, I.; et al. MPLW515L is a novel somatic activating mutation in myelofibrosis with myeloid metaplasia. PLoS Med. 2006, 3, e270. [Google Scholar] [CrossRef] [Green Version]
- Pardanani, A.D.; Levine, R.L.; Lasho, T.; Pikman, Y.; Mesa, R.A.; Wadleigh, M.; Steensma, D.P.; Elliott, M.A.; Wolanskyj, A.P.; Hogan, W.J.; et al. MPL515 mutations in myeloproliferative and other myeloid disorders: A study of 1182 patients. Blood 2006, 108, 3472–3476. [Google Scholar] [CrossRef] [Green Version]
- Kröger, N.; Badbaran, A.; Holler, E.; Hahn, J.; Kobbe, G.; Bornhäuser, M.; Reiter, A.; Zabelina, T.; Zander, A.R.; Fehse, B. Monitoring of the JAK2-V617F mutation by highly sensitive quantitative real-time PCR after allogeneic stem cell transplantation in patients with myelofibrosis. Blood 2007, 109, 1316–1321. [Google Scholar] [CrossRef] [Green Version]
- Klampfl, T.; Gisslinger, H.; Harutyunyan, A.S.; Nivarthi, H.; Rumi, E.; Milosevic, J.D.; Them, N.C.; Berg, T.; Gisslinger, B.; Pietra, D.; et al. Somatic Mutations of Calreticulin in Myeloproliferative Neoplasms. N. Engl. J. Med. 2013, 369, 2379–2390. [Google Scholar] [CrossRef] [Green Version]
- Nangalia, J.; Massie, C.; Baxter, E.; Nice, F.; Gundem, G.; Wedge, D.; Avezov, E.; Li, J.; Kollmann, K.; Kent, D.; et al. Somatic CALR Mutations in Myeloproliferative Neoplasms with Nonmutated JAK2. N. Engl. J. Med. 2013, 369, 2391–2405. [Google Scholar] [CrossRef] [Green Version]
- Rumi, E.; Pietra, D.; Ferretti, V.; Klampfl, T.; Harutyunyan, A.S.; Milosevic, J.D.; Them, N.C.; Berg, T.; Elena, C.; Casetti, I.C.; et al. Associazione Italiana per la Ricerca sul Cancro Gruppo Italiano Malattie Mieloproliferative Investigators JAK2 or CALR mutation status defines subtypes of essential thrombocythemia with substantially different clinical course and outcomes. Blood 2014, 123, 1544–1551. [Google Scholar] [CrossRef]
- Wolanskyj, A.P.; Lasho, T.L.; Schwager, S.M.; McClure, R.F.; Wadleigh, M.; Lee, S.J.; Gilliland, D.G.; Tefferi, A. JAK2 mutation in essential thrombocythaemia: Clinical associations and longterm prognostic relevance. Br. J. Haematol. 2005, 131, 208–213. [Google Scholar] [CrossRef]
- Sandberg, E.M.; Wallace, T.A.; Godeny, M.D.; Linden, D.V.; Sayeski, P.P. JAK2 tyrosine kinase: A true Jak of all trades? Cell Biochem. Biophys. 2004, 41, 207–232. [Google Scholar] [CrossRef]
- Tefferi, A.; Lasho, T.L.; Finke, C.; Belachew, A.A.; Wassie, E.A.; Ketterling, R.P.; Hanson, C.A.; Pardanani, A. Type 1 vs type 2 calreticulin mutations in primary myelofibrosis: Differences in phenotype and prognostic impact. Leukemia 2014, 28, 1568–1570. [Google Scholar] [CrossRef] [PubMed]
- Guglielmelli, P.; Rotunno, G.; Fanelli, T.; Pacilli, A.; Brogi, G.; Calabresi, L.; Pancrazzi, A.; Vannucchi, A.M. Validation of the differential prognostic impact of type 1/type 1-like versus type 2/type 2-like CALR mutations in myelofibrosis. Blood Cancer J. 2015, 5, e360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kisseleva, T.; Bhattacharya, S.; Braunstein, J.; Schindler, C.W. Signaling through the Jak/STAT pathway, recent advances and future challenges. Gene 2002, 285, 1–24. [Google Scholar] [CrossRef]
- Zhao, R.; Xing, S.; Li, Z.; Fu, X.; Li, Q.; Krantz, S.B.; Zhao, Z.J. Identification of an acquired JAK2 mutation in polycythemia vera. J. Biol. Chem. 2005, 280, 22788–22792. [Google Scholar] [CrossRef] [Green Version]
- Staerk, J.; Lacout, C.; Sato, T.; Smith, S.O.; Vainchenker, W.; Constantinescu, S.N. An amphipathic motif at the transmembrane-cytoplasmic junction prevents autonomous activation of the thrombopoietin receptor. Blood 2006, 107, 1864–1871. [Google Scholar] [CrossRef]
- Lim, K.-H.; Chang, Y.-C.; Chen, C.G.-S.; Lin, H.-C.; Wang, W.-T.; Chiang, Y.-H.; Cheng, H.-I.; Su, N.-W.; Lin, J.; Chang, M.-C.; et al. Frequent CALR exon 9 alterations in JAK2 V617F-mutated essential thrombocythemia detected by high-resolution melting analysis. Blood Cancer J. 2015, 5, e295. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Tefferi, A.; Vardiman, J.W. Classification and diagnosis of myeloproliferative neoplasms: The 2008 World Health Organization criteria and point-of-care diagnostic algorithms. Leukemia 2008, 22, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SAS Institute Inc. SAS® 9.4; SAS Institute Inc.: Cary, NC, USA, 2016. [Google Scholar]
- Harris, K. ROC Hard? No, ROC Made Easy! In Proceedings of the 2010 SAS Global Forum; GlaxoSmithKline: Brentford, UK, 2010; Available online: http://support.sas.com/resources/papers/proceedings10/222-2010.pdf (accessed on 1 April 2021).
- Ashorobi, D.; Gohari, P. Essential Thrombocytosis; StatPearls: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK539709/ (accessed on 1 April 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index | Mutation Frequency | ODR (Odds Ratio)/p | |
|---|---|---|---|
| JAK2+ | |||
| In cohort | 68.8% (1914/1958) | ||
| Gender | Male | 67.4% (443/657) | ODR = 1.1 (0.9 − 1.35) pFisher = 0.2 |
| Female | 69.5% (874/1257) | ||
| Age | ≤60 years | 66.2% (339/559) | ODR = 1.5 (1.2 − 1.9) pFisher = 0.0001 |
| >60 years | 74.6% (446/598) | ||
| Diagnosis | ET | 53.9% (185/343) | pχ2 < 0.0001 |
| PV | 91.1% (507/555) | ||
| PMF | 60.5% (156/258) | ||
| MPN-U | 61.9% (469/758) | ||
| CALR+ | |||
| In cohort | 22.6% (315/1402) | ||
| Gender | Male | 21.0% (102/485) | ODR = 1.1 (0.9 − 1.5) pFisher = 0.2 |
| Female | 23.2% (213/917) | ||
| Age | ≤60 years | 27.7% (118/426) | ODR = 0.6 (0.4 − 0.8) pFisher < 0.0002 |
| >60 years | 20.2 (197/975) | ||
| Diagnosis | ET | 41.2% (112/272) | pχ2 < 0.0001 |
| PV | 0 | ||
| PMF | 36.9% (79/214) | ||
| MPN-U | 19.8% (124/628) | ||
| MPL+ | |||
| In cohort | 1.7% (23/1364) | ||
| Gender | Male | 1.7% (8/474) | ODR = 0.9 (0.4 − 2.4) pFisher = 0.6 |
| Female | 1.7% (15/890) | ||
| Age | ≤60 years | 1.1% (10/914) | ODR = 2.7 (1.2 − 6.2) pFisher = 0.02 |
| >60 years | 2.9% (13/450) | ||
| Diagnosis | ET | 1.5% (4/263) | pχ2 = 0.03 |
| PV | 0 | ||
| PMF | 3.4% (7/205) | ||
| MPN-U | 1.9% (12/609) | ||
| Factor | N | Median, Range | Mean | Standard Deviation | p Fisher | |
|---|---|---|---|---|---|---|
| JAK2+ | ||||||
| Gender | Male | 438 | 29.0 (0.28–100) | 37.1 | 28.6 | |
| Female | 859 | 24.0 (1–100) | 33.8 | 28.9 | p = 0.05 | |
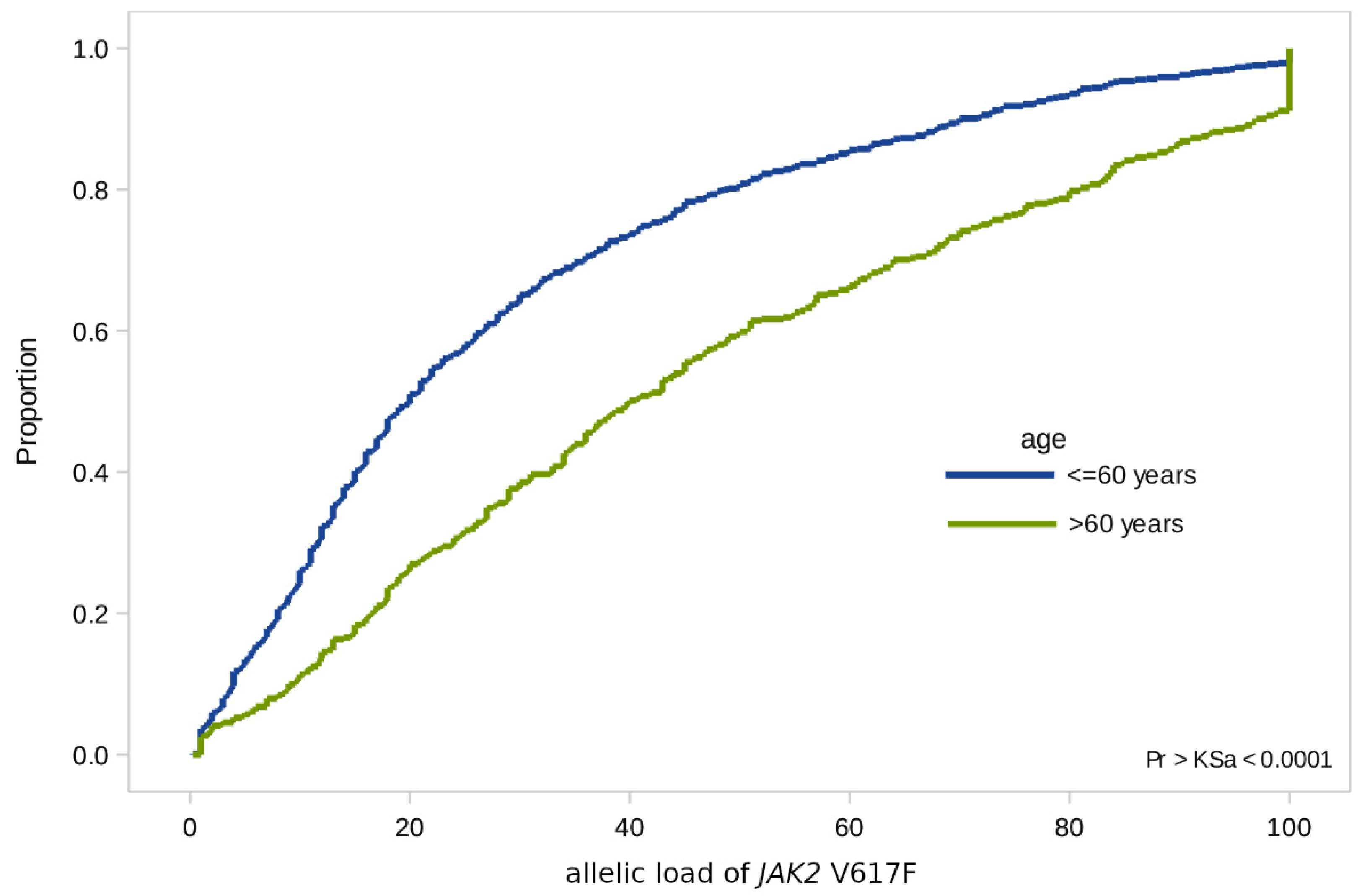
| Age | ≤60 years | 856 | 20.0 (0.28–100) | 28.9 | 25.7 | |
| >60 years | 441 | 40.0 (1–100) | 46.5 | 30.9 | p < 0.0001 | |
| Diagnosis | ET | 182 | 10.8 (1–100) | 14.4 | 13.7 | |
| PV | 497 | 34.0 (1–100) | 41.3 | 28.6 | ||
| PMF | 154 | 43.0 (1–100) | 47.2 | 30.7 | ||
| MPN-U | 464 | 22 (0.28–100) | 32.2 | 28.1 | p < 0.0001 | |
| CALR+ | ||||||
| Gender | Male | 40 | 42.0 (10–54) | 38.7 | 12.9 | |
| Female | 73 | 45.0 (6–96) | 43.4 | 14.1 | p = 0.08 | |
| Age | ≤60 years | 89 | 43.0 (6–96) | 41.5 | 12.9 | |
| >60 years | 24 | 46.0 (8–85) | 42.3 | 16.7 | p = 0.7 | |
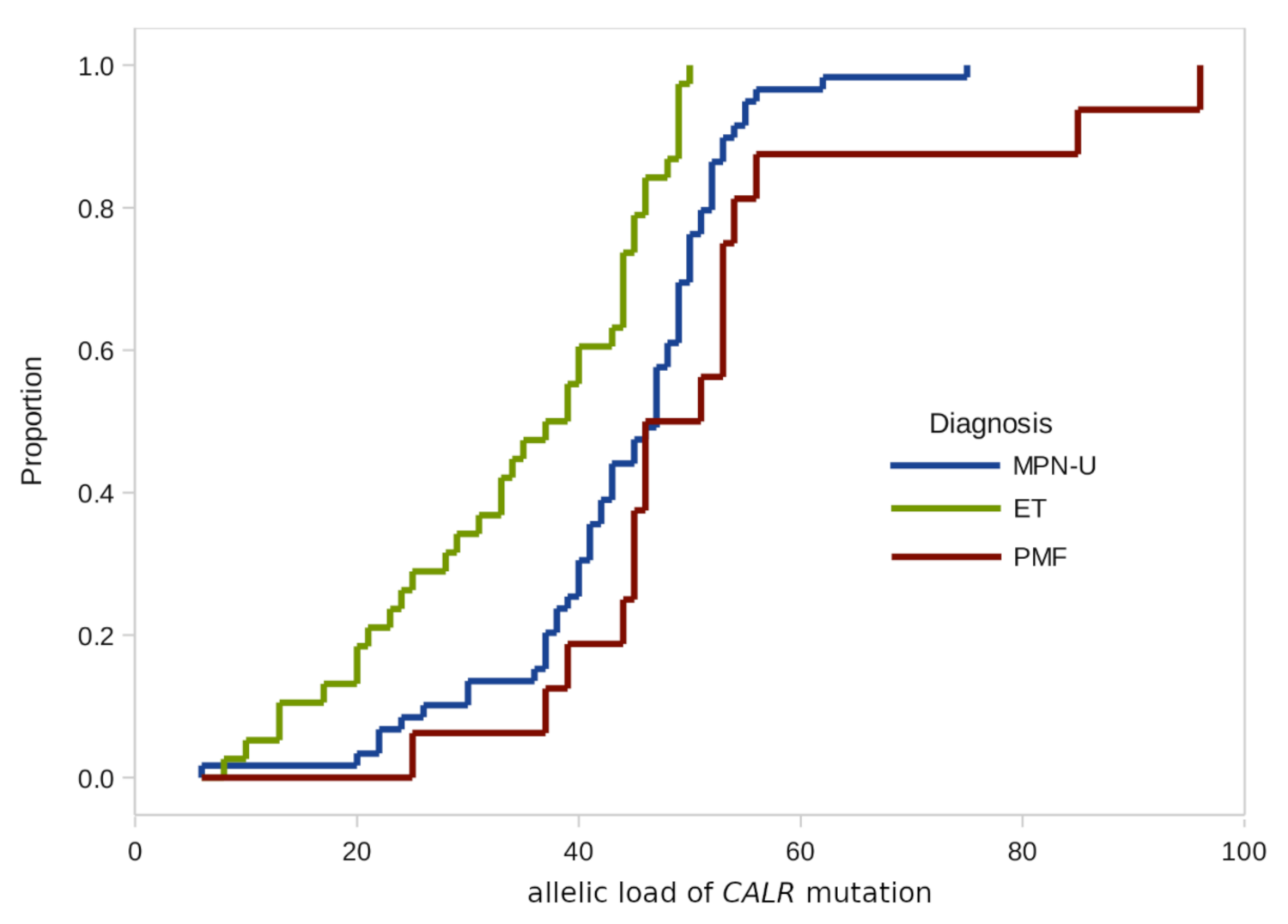
| Diagnosis | ET | 38 | 38.0 (8–50) | 34.5 | 12.1 | |
| PV | 0 | |||||
| PMF | 16 | 48.5 (25–96) | 51.8 | 17.1 | ||
| MPN-U | 59 | 47.0 (6–75) | 43.8 | 11.1 | p < 0.0001 | |
| Criteria | Whole Group (n = 23) | ET (6) | PMF (14) |
|---|---|---|---|
| Age, years, median (range) | 57 (23–86) | 46 (26–61) | 64.5 (23–86) |
| Men:Women | 1:1 (12:11) | 1:1 (3:3) | 5:9 (1:1.8) |
| Diagnosis: ET PMF MPN-U | 6 14 3 | ||
| Red blood cell, ×1012/L | 4.1 (2.9–5.7) | 4.4 (3.5–5.1) | 3.89 (2.9–4.8) |
| Hemoglobin, g/L | 120 (83–166) | 133 (83–154) | 106 (91–142) |
| Platelets, ×109/L | 815 (98–1900) | 1298 (774–1900) | 572 (98–1475) |
| White blood cell, ×109/L | 7.6 (3.41–16) | 8.1 (7.43–16) | 6.6 (3.41–11.63) |
| Splenomegaly, % (number of patients) | 61% (14) | 17 (1) | 79 (11) |
| Risk: | |||
| IPSS Low Intermediate-1 Intermediate-2 High | NA | 4 7 3 0 | |
| IPSET: Low Intermediate High | 0 4 2 | NA | |
| Thrombosis, % (number of patients) | 9% (2) | 33% (2) | - |
| Treatment: | |||
| Hydroxyurea | 16 | 4 | 10 |
| Interferon α 2b | 2 | 1 | 0 |
| Anagrelid | 1 | 1 | 0 |
| Imatinib then Interferon α 2b | 2 | 0 | 2 |
| Observation | 2 | 0 | 2 |
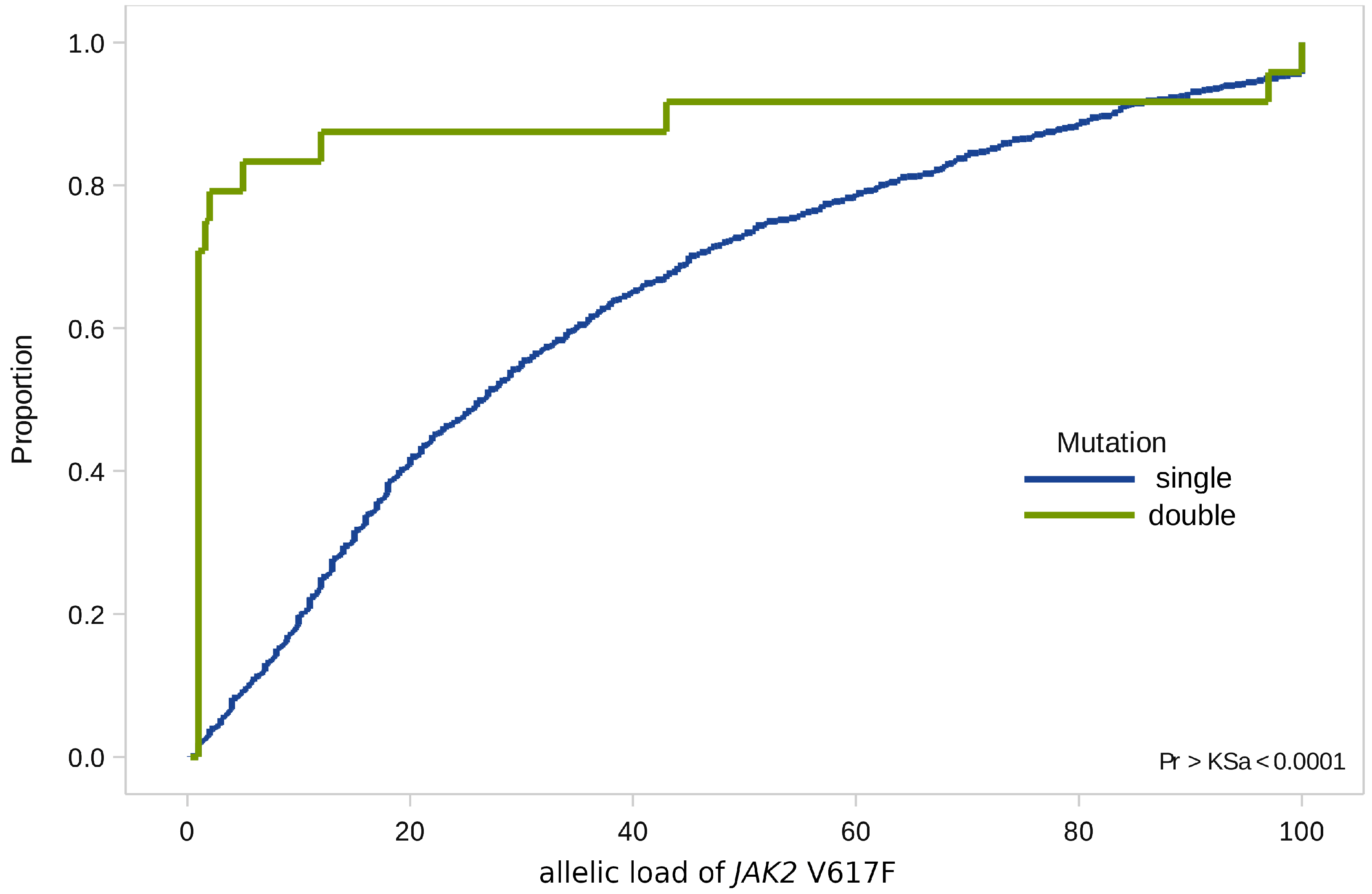
| CALR+ | CALR− | Total | |
|---|---|---|---|
| Allele burden JAK2 ≤ 1% | 16 | 18 | 34 |
| Allele burden JAK2 > 1% | 7 | 753 | 760 |
| Total | 23 | 771 | 794 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makarik, T.V.; Abdullaev, A.O.; Nikulina, E.E.; Treglazova, S.A.; Stepanova, E.E.; Subortseva, I.N.; Kovrigina, A.M.; Melikyan, A.L.; Kulikov, S.M.; Sudarikov, A.B. Low JAK2 V617F Allele Burden in Ph-Negative Chronic Myeloproliferative Neoplasms Is Associated with Additional CALR or MPL Gene Mutations. Genes 2021, 12, 559. https://doi.org/10.3390/genes12040559
Makarik TV, Abdullaev AO, Nikulina EE, Treglazova SA, Stepanova EE, Subortseva IN, Kovrigina AM, Melikyan AL, Kulikov SM, Sudarikov AB. Low JAK2 V617F Allele Burden in Ph-Negative Chronic Myeloproliferative Neoplasms Is Associated with Additional CALR or MPL Gene Mutations. Genes. 2021; 12(4):559. https://doi.org/10.3390/genes12040559
Chicago/Turabian StyleMakarik, Tatiana V., Adhamjon O. Abdullaev, Elena E. Nikulina, Svetlana A. Treglazova, Elena E. Stepanova, Irina N. Subortseva, Alla M. Kovrigina, Anait L. Melikyan, Sergei M. Kulikov, and Andrey B. Sudarikov. 2021. "Low JAK2 V617F Allele Burden in Ph-Negative Chronic Myeloproliferative Neoplasms Is Associated with Additional CALR or MPL Gene Mutations" Genes 12, no. 4: 559. https://doi.org/10.3390/genes12040559