
Potential Impacts of Interleukin-17A Promoter Polymorphisms on the EGFR Mutation Status and Progression of Non-Small Cell Lung Cancer in Taiwan

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Selection and Specimens
2.2. Genomic DNA Extraction from Tumor Tissues and EGFR Sequencing
2.3. Selection of IL-17A SNPs and Genotyping of IL-17A SNPs from Peripheral Blood
2.4. Cell Culture
2.5. Western Blot Analysis
2.6. DNA Construction and Transient Transfection
2.7. Cell Proliferation and Colony Formation Assays
2.8. Outcome Analysis in Kaplan Meier (KM) Plotter
2.9. Statistical Analysis
3. Results
3.1. General Characteristics of LUAD Patients with the WT or MT EGFR
3.2. Distribution of IL-17A Candidate SNPs (rs8193036, rs8193037, rs2275913, and rs3748067) of LUAD Patients and Their Associations with the EGFR Mutation Status
3.3. Correlations between Polymorphic Genotypes of IL-17A and Clinicopathological Characteristics of LUAD Patients with the WT or MT EGFR
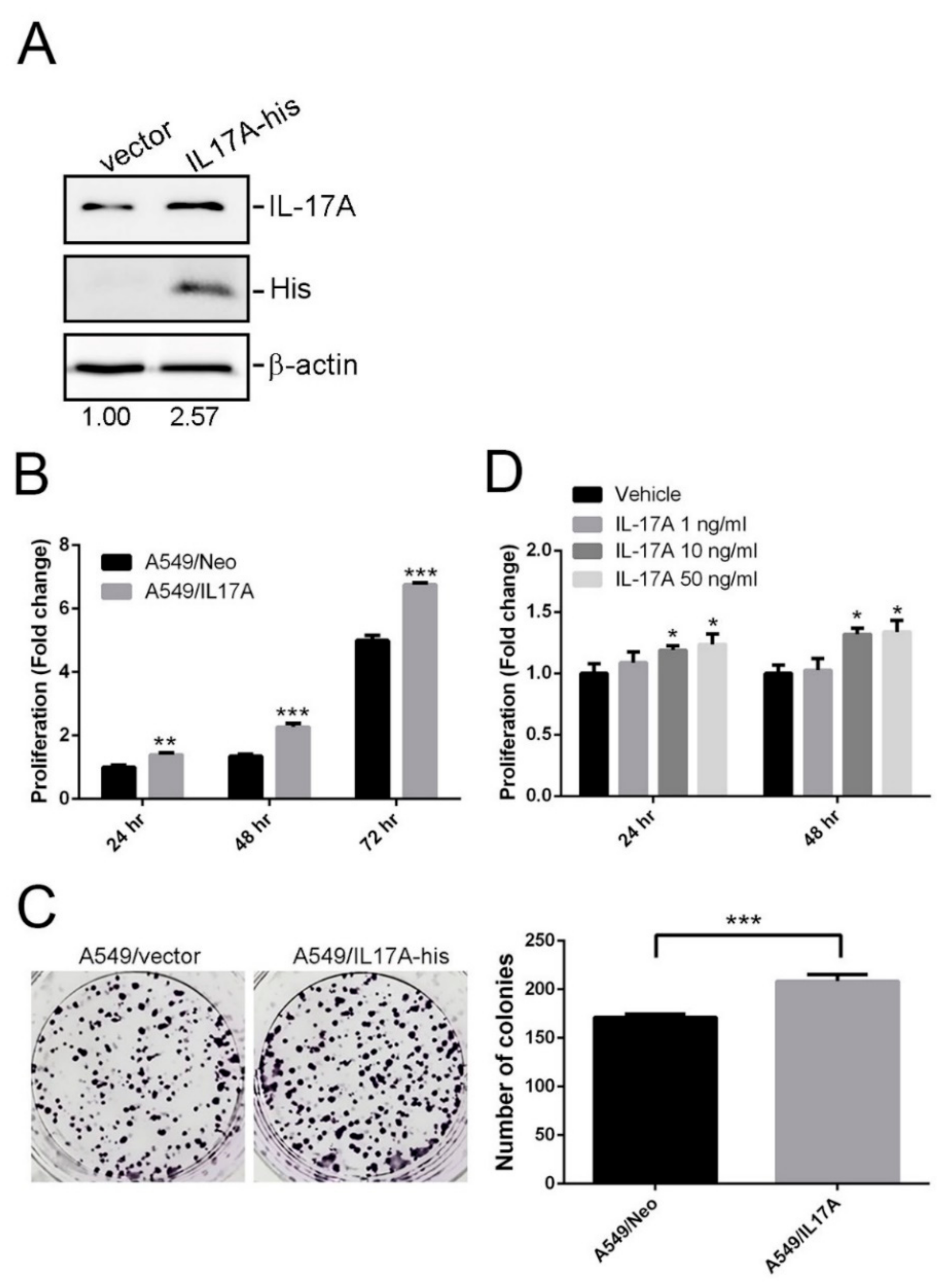
3.4. Effects of IL-17A on Growth of LUAD Cells Harboring WT EGFR and MT KRAS
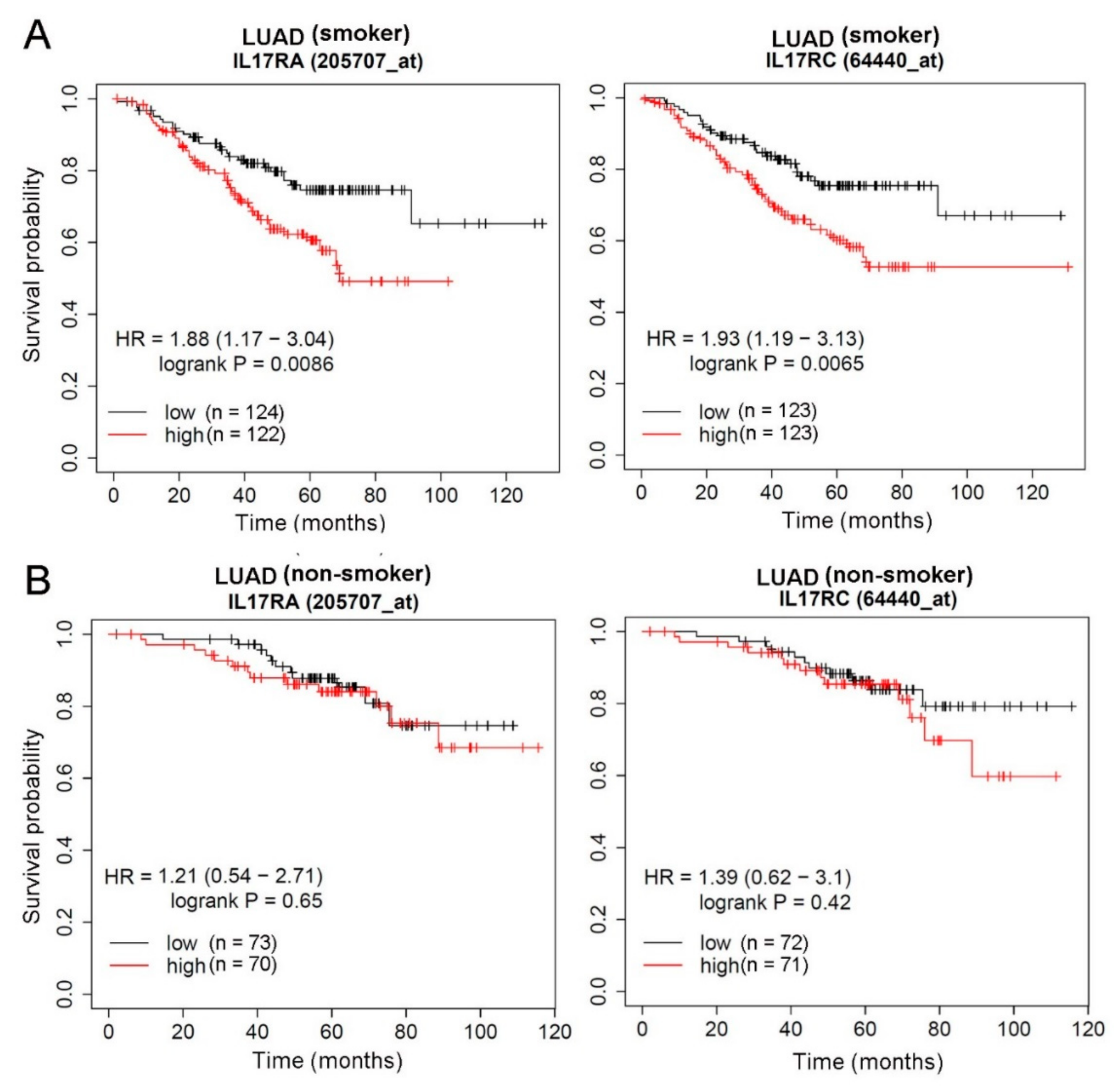
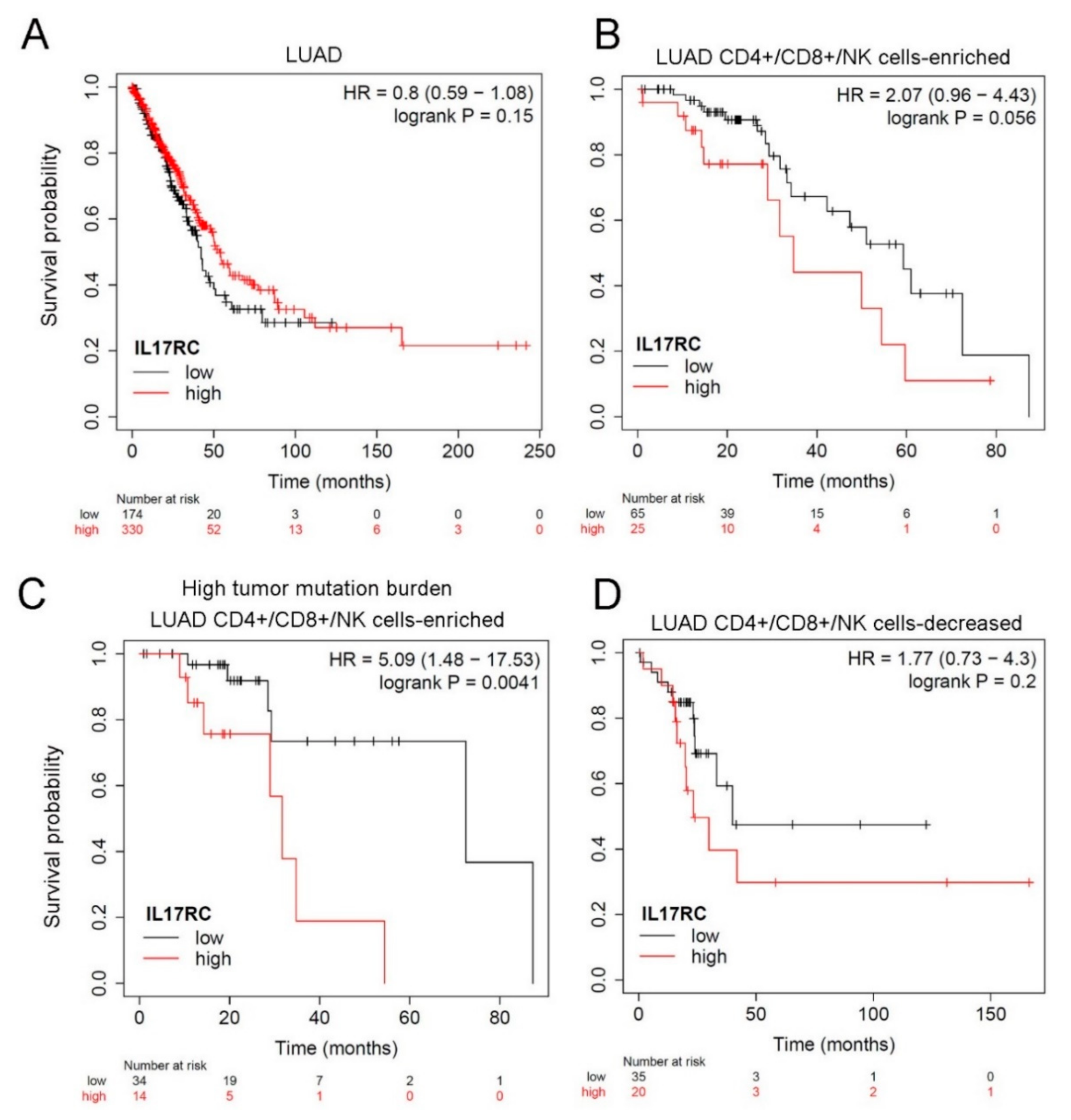
3.5. Prognostic Significance of IL-17 Receptors in LUAD Patients with Different Smoking or EGFR Statuses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Youlden, D.R.; Cramb, S.M.; Baade, P.D. The International Epidemiology of Lung Cancer: Geographical distribution and secular trends. J. Thorac. Oncol. 2008, 3, 819–831. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Wu, Y.L.; Zhou, C.; Hu, C.P.; Feng, J.; Lu, S.; Huang, Y.; Li, W.; Hou, M.; Shi, J.H.; Lee, K.Y.; et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): An open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 213–222. [Google Scholar] [CrossRef]
- Isaka, T.; Nakayama, H.; Ito, H.; Yokose, T.; Yamada, K.; Masuda, M. Impact of the epidermal growth factor receptor mutation status on the prognosis of recurrent adenocarcinoma of the lung after curative surgery. BMC Cancer 2018, 18, 959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broderick, P.; Wang, Y.; Vijayakrishnan, J.; Matakidou, A.; Spitz, M.R.; Eisen, T.; Amos, C.I.; Houlston, R.S. Deciphering the impact of common genetic variation on lung cancer risk: A genome-wide association study. Cancer Res. 2009, 69, 6633–6641. [Google Scholar] [CrossRef] [Green Version]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.; Teixeira, A.L.; Coelho, A.; Araújo, A.; Medeiros, R. The role of inflammation in lung cancer. Adv. Exp. Med. Biol. 2014, 816, 1–23. [Google Scholar]
- Bai, L.; Yu, H.; Wang, H.; Su, H.; Zhao, J.; Zhao, Y. Genetic single-nucleotide polymorphisms of inflammation-related factors associated with risk of lung cancer. Med. Oncol. 2013, 30, 414. [Google Scholar] [CrossRef]
- Lim, W.Y.; Chen, Y.; Ali, S.M.; Chuah, K.L.; Eng, P.; Leong, S.S.; Lim, E.; Lim, T.K.; Ng, A.W.; Poh, W.T.; et al. Polymorphisms in inflammatory pathway genes, host factors and lung cancer risk in Chinese female never-smokers. Carcinogenesis 2011, 32, 522–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitiello, G.A.; Miller, G. Targeting the interleukin-17 immune axis for cancer immunotherapy. J. Exp. Med. 2020, 217, e20190456. [Google Scholar] [CrossRef] [PubMed]
- Beringer, A.; Noack, M.; Miossec, P. IL-17 in Chronic Inflammation: From Discovery to Targeting. Trends Mol. Med. 2016, 22, 230–241. [Google Scholar] [CrossRef]
- Zhao, J.; Chen, X.; Herjan, T.; Li, X. The role of interleukin-17 in tumor development and progression. J. Exp. Med. 2020, 217, e20190297. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Hao, K.; Yu, L.; Zhang, X. Serum interleukin-17 as a diagnostic and prognostic marker for non-small cell lung cancer. Biomarkers 2014, 19, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wan, J.; Liu, J.; Xie, W.; Diao, X.; Xu, J.; Zhu, B.; Chen, Z. Increased IL-17-producing cells correlate with poor survival and lymphangiogenesis in NSCLC patients. Lung Cancer 2010, 69, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Cai, G.; Liu, C.; Zhao, J.; Gu, C.; Wu, L.; Hamilton, T.A.; Zhang, C.J.; Ko, J.; Zhu, L.; et al. IL-17R-EGFR axis links wound healing to tumorigenesis in Lrig1(+) stem cells. J. Exp. Med. 2019, 216, 195–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niu, Y.M.; Yuan, H.; Zhou, Y. Interleukin-17 gene polymorphisms contribute to cancer risk. Mediat. Inflamm. 2014, 2014, 128490. [Google Scholar] [CrossRef]
- Kaabachi, W.; Ben Amor, A.; Kaabachi, S.; Rafrafi, A.; Tizaoui, K.; Hamzaoui, K. Interleukin-17A and -17F genes polymorphisms in lung cancer. Cytokine 2014, 66, 23–29. [Google Scholar] [CrossRef]
- Cheng, S.; Shao, Z.; Liu, X.; Guo, L.; Zhang, X.; Na, Q.; Chen, X.; Ma, Y.; Zheng, J.; Song, B.; et al. Interleukin 17A polymorphism elevates gene expression and is associated with increased risk of nonsmall cell lung cancer. DNA Cell Biol. 2015, 34, 63–68. [Google Scholar] [CrossRef]
- Wei, R.; Cao, L.; Pu, H.; Wang, H.; Zheng, Y.; Niu, X.; Weng, X.; Zhang, H.; Favus, M.; Zhang, L.; et al. TERT Polymorphism rs2736100-C Is Associated with EGFR Mutation-Positive Non-Small Cell Lung Cancer. Clin. Cancer Res. 2015, 21, 5173–5180. [Google Scholar] [CrossRef] [Green Version]
- Shiraishi, K.; Okada, Y.; Takahashi, A.; Kamatani, Y.; Momozawa, Y.; Ashikawa, K.; Kunitoh, H.; Matsumoto, S.; Takano, A.; Shimizu, K.; et al. Association of variations in HLA class II and other loci with susceptibility to EGFR-mutated lung adenocarcinoma. Nat. Commun. 2016, 7, 12451. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.L.; Chien, M.H.; Chou, Y.E.; Chang, J.H.; Liu, T.C.; Tsao, T.C.; Chou, M.C.; Yang, S.F. Association of EGFR mutations and HMGB1 genetic polymorphisms in lung adenocarcinoma patients. J. Cancer 2019, 10, 2907–2914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, K.Y.; Chen, H.Y.; Li, K.C.; Kuo, M.L.; Yang, J.C.; Chan, W.K.; Ho, B.C.; Chang, G.C.; Shih, J.Y.; Yu, S.L.; et al. Pretreatment epidermal growth factor receptor (EGFR) T790M mutation predicts shorter EGFR tyrosine kinase inhibitor response duration in patients with non-small-cell lung cancer. J. Clin. Oncol. 2012, 30, 433–440. [Google Scholar] [CrossRef] [Green Version]
- Hsu, K.H.; Ho, C.C.; Hsia, T.C.; Tseng, J.S.; Su, K.Y.; Wu, M.F.; Chiu, K.L.; Yang, T.Y.; Chen, K.C.; Ooi, H.; et al. Identification of five driver gene mutations in patients with treatment-naïve lung adenocarcinoma in Taiwan. PLoS ONE 2015, 10, e0120852. [Google Scholar] [CrossRef] [Green Version]
- He, Y.; Du, Y.; Wei, S.; Shi, J.; Mei, Z.; Qian, L.; Chen, Z.; Jie, Z. IL-17A and IL-17F single nucleotide polymorphisms associated with lung cancer in Chinese population. Clin. Respir. J. 2017, 11, 230–242. [Google Scholar] [CrossRef] [PubMed]
- Ponce-Gallegos, M.A.; Pérez-Rubio, G.; Ambrocio-Ortiz, E.; Partida-Zavala, N.; Hernández-Zenteno, R.; Flores-Trujillo, F.; García-Gómez, L.; Hernández-Pérez, A.; Ramírez-Venegas, A.; Falfán-Valencia, R. Genetic variants in IL17A and serum levels of IL-17A are associated with COPD related to tobacco smoking and biomass burning. Sci. Rep. 2020, 10, 784. [Google Scholar] [CrossRef] [Green Version]
- Tseng, T.H.; Chien, M.H.; Lin, W.L.; Wen, Y.C.; Chow, J.M.; Chen, C.K.; Kuo, T.C.; Lee, W.J. Inhibition of MDA-MB-231 breast cancer cell proliferation and tumor growth by apigenin through induction of G2/M arrest and histone H3 acetylation-mediated p21(WAF1/CIP1) expression. Environ. Toxicol. 2017, 32, 434–444. [Google Scholar] [CrossRef]
- Shigematsu, H.; Lin, L.; Takahashi, T.; Nomura, M.; Suzuki, M.; Wistuba, I.I.; Fong, K.M.; Lee, H.; Toyooka, S.; Shimizu, N.; et al. Clinical and biological features associated with epidermal growth factor receptor gene mutations in lung cancers. J. Natl. Cancer Inst. 2005, 97, 339–346. [Google Scholar] [CrossRef] [Green Version]
- Tseng, C.H.; Chiang, C.J.; Tseng, J.S.; Yang, T.Y.; Hsu, K.H.; Chen, K.C.; Wang, C.L.; Chen, C.Y.; Yen, S.H.; Tsai, C.M.; et al. EGFR mutation, smoking, and gender in advanced lung adenocarcinoma. Oncotarget 2017, 8, 98384–98393. [Google Scholar] [CrossRef] [Green Version]
- Fabre, J.; Giustiniani, J.; Garbar, C.; Antonicelli, F.; Merrouche, Y.; Bensussan, A.; Bagot, M.; Al-Dacak, R. Targeting the Tumor Microenvironment: The Protumor Effects of IL-17 Related to Cancer Type. Int. J. Mol. Sci. 2016, 17, 1433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pallis, A.G.; Syrigos, K.N. Lung cancer in never smokers: Disease characteristics and risk factors. Crit. Rev. Oncol. Hematol. 2013, 88, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Hecht, S.S. Tobacco carcinogens, their biomarkers and tobacco-induced cancer. Nat. Rev. Cancer 2003, 3, 733–744. [Google Scholar] [CrossRef] [PubMed]
- Akbay, E.A.; Koyama, S.; Liu, Y.; Dries, R.; Bufe, L.E.; Silkes, M.; Alam, M.M.; Magee, D.M.; Jones, R.; Jinushi, M.; et al. Interleukin-17A Promotes Lung Tumor Progression through Neutrophil Attraction to Tumor Sites and Mediating Resistance to PD-1 Blockade. J. Thorac. Oncol. 2017, 12, 1268–1279. [Google Scholar] [CrossRef] [Green Version]
- Xie, M.; Cheng, B.; Ding, Y.; Wang, C.; Chen, J. Correlations of IL-17 and NF-κB gene polymorphisms with susceptibility and prognosis in acute respiratory distress syndrome in a chinese population. Biosci. Rep. 2019, 39, BSR20181987. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.; Xu, J.; Huang, Q.; Han, J.; Duan, L.; Fan, J.; Lv, Z.; Guo, M.; Hu, G.; Chen, L.; et al. The Role of Interleukin-17 in Lung Cancer. Mediat. Inflamm. 2016, 2016, 8494079. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; He, D.; Zhao, S.; Wang, H. IL-17A/IL-17RA promotes invasion and activates MMP-2 and MMP-9 expression via p38 MAPK signaling pathway in non-small cell lung cancer. Mol. Cell. Biochem. 2019, 455, 195–206. [Google Scholar] [CrossRef]
- Huang, Q.; Du, J.; Fan, J.; Lv, Z.; Qian, X.; Zhang, X.; Han, J.; Chen, C.; Wu, F.; Jin, Y. The effect of proinflammatory cytokines on IL-17RA expression in NSCLC. Med. Oncol. 2014, 31, 144. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Subject Characteristic | Total (N = 277) | Wild Type (N = 109) | Mutation Type (N = 168) | p Value |
|---|---|---|---|---|
| Age, n (%) | ||||
| Mean ± SD (years) | 65.60 ± 13.46 | 65.45 ± 13.34 | 65.69 ± 13.58 | 0.885 |
| Gender, n (%) | ||||
| Male | 125 (45.1%) | 65 (59.6%) | 60 (35.7%) | <0.001 |
| Female | 152 (54.9%) | 44 (40.4%) | 108 (64.3%) | |
| Cigarette smoking, n (%) | ||||
| Non-smoker | 179 (64.6%) | 49 (45.0%) | 130 (77.4%) | <0.001 |
| Ever-smoker | 98 (35.4%) | 60 (55.0%) | 38 (22.6%) | |
| Cancer stage, n (%) | ||||
| I or II | 72 (26.0%) | 25 (22.9%) | 47 (28.0%) | 0.350 |
| III or IV | 205 (74.0%) | 84 (77.1%) | 121 (72.0%) | |
| Tumor T status, n (%) | ||||
| T1 or T2 | 166 (59.9%) | 59 (54.1%) | 107 (63.7%) | 0.113 |
| T3 or T4 | 111 (40.1%) | 50 (45.9%) | 61 (36.3%) | |
| Lymph node status, n (%) | ||||
| Negative | 81 (29.2%) | 28 (25.7%) | 53 (31.5%) | 0.295 |
| Positive | 196 (70.8%) | 81 (74.3%) | 115 (68.5%) | |
| Distant metastasis, n (%) | ||||
| Negative | 133 (48.0%) | 53 (48.6%) | 80 (47.6%) | 0.870 |
| Positive | 144 (52.0%) | 56 (51.4%) | 88 (52.4%) | |
| Cell differentiation, n (%) | ||||
| Good/Moderate | 245 (88.4%) | 87 (79.8%) | 158 (94.0%) | <0.001 |
| Poor | 32 (11.6%) | 22 (20.2%) | 10 (6.0%) |
| Genotype SNP | Wild Type (N = 60) | Mutated Type (N = 38) | AOR (95% CI) | p Value |
|---|---|---|---|---|
| rs8193036 | ||||
| CC | 36 (60.0%) | 19 (50.0%) | 1.00 | |
| CT | 18 (30.0%) | 12 (31.6%) | 1.675 (0.628~4.469) | 0.303 |
| TT | 6 (10.0%) | 7 (18.4%) | 3.125 (0.842~11.590) | 0.088 |
| CT + TT | 24 (40.0%) | 19 (50.0%) | 2.023 (0.837~4.890) | 0.117 |
| rs8193037 | ||||
| GG | 44 (73.3%) | 35 (92.1%) | 1.00 | |
| GA | 15 (25.0%) | 3 (7.9%) | 0.225 (0.056~0.900) | 0.035 * |
| AA | 1 (1.7%) | 0 (0.0%) | --- | --- |
| GA + AA | 16 (26.7%) | 3 (7.9%) | 0.222 (0.056~0.885) | 0.033 * |
| rs2275913 | ||||
| GG | 23 (38.3%) | 8 (21.1%) | 1.00 | |
| GA | 23 (38.3%) | 19 (50.0%) | 2.021 (0.712~5.742) | 0.186 |
| AA | 14 (23.4%) | 11 (28.9%) | 1.523 (0.450~5.154) | 0.499 |
| GA + AA | 37 (61.7%) | 30 (78.9%) | 1.839 (0.689~4.911) | 0.224 |
| rs3748067 | ||||
| CC | 49 (81.7%) | 32 (84.2%) | 1.00 | |
| CT | 10 (16.7%) | 6 (15.8%) | 0.811 (0.258~2.550) | 0.720 |
| TT | 1 (1.6%) | 0 (0.0%) | --- | --- |
| CT + TT | 11 (18.3%) | 6 (15.8%) | 0.721 (0.234~2.223) | 0.569 |
| rs763780 | ||||
| TT | 40 (66.7%) | 27 (71.1%) | 1.00 | |
| TC | 15 (25.0%) | 10 (26.3%) | 0.941 (0.343~2.586) | 0.906 |
| CC | 5 (8.3%) | 1 (2.6%) | 0.411 (0.042~3.999) | 0.444 |
| TC + CC | 20 (33.3%) | 11 (28.9%) | 0.824 (0.319~2.124) | 0.688 |
| Genotype SNP | CC (N = 153) | CT or TT (N = 124) | AOR (95% CI) | p Value |
|---|---|---|---|---|
| Stage | ||||
| I or II | 48 (31.4%) | 24 (19.4%) | 1.00 | 0.020 * |
| III or IV | 105 (68.6%) | 100 (80.6%) | 1.976 (1.114~3.506) | |
| Tumor T status | ||||
| T1 or T2 | 91 (59.5%) | 75 (60.5%) | 1.00 | 0.813 |
| T3 or T4 | 62 (40.5%) | 49 (39.5%) | 0.942 (0.574~1.545) | |
| Lymph node metastasis | ||||
| Negative | 49 (32.0%) | 32 (25.8%) | 1.00 | 0.249 |
| Positive | 104 (68.0%) | 92 (74.2%) | 1.372 (0.801~2.348) | |
| Distant metastasis | ||||
| Negative | 73 (47.7%) | 60 (48.4%) | 1.00 | 0.846 |
| Positive | 80 (52.3%) | 64 (51.6%) | 0.953 (0.586~1.550) | |
| Cell differentiation | ||||
| Good/Moderate | 131 (85.6%) | 114 (91.9%) | 1.00 | 0.122 |
| Poor | 22 (14.4%) | 10 (8.1%) | 0.527 (0.234~1.187) |
| Genotype SNP | CC (N = 63) | CT or TT (N = 46) | AOR (95% CI) | p Value |
|---|---|---|---|---|
| Stage | ||||
| I or II | 20 (31.7%) | 5 (10.9%) | 1.00 | 0.016 * |
| III or IV | 43 (68.3%) | 41 (89.1%) | 4.175 (1.312~13.285) | |
| Tumor T status | ||||
| T1 or T2 | 34 (54.0%) | 25 (54.3%) | 1.00 | 0.691 |
| T3 or T4 | 29 (46.0%) | 21 (45.7%) | 0.849 (0.377~1.908) | |
| Lymph node metastasis | ||||
| Negative | 21 (33.3%) | 7 (15.2%) | 1.00 | 0.049 * |
| Positive | 42 (66.7%) | 39 (84.8%) | 2.839 (1.005~8.018) | |
| Distant metastasis | ||||
| Negative | 34 (54.0%) | 19 (41.3%) | 1.00 | 0.273 |
| Positive | 29 (46.0%) | 27 (58.7%) | 1.587 (0.696-3.620) | |
| Cell differentiation | ||||
| Good/Moderate | 48 (76.2%) | 39 (84.8%) | 1.00 | 0.271 |
| Poor | 15 (23.8%) | 7 (15.2%) | 0.553 (0.192-1.590) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.-L.; Lai, T.-C.; Wang, Y.-C.; Shih, P.-C.; Yang, Y.-C.; Tsao, T.C.-Y.; Liu, T.-C.; Wen, Y.-C.; Chang, L.-C.; Yang, S.-F.; et al. Potential Impacts of Interleukin-17A Promoter Polymorphisms on the EGFR Mutation Status and Progression of Non-Small Cell Lung Cancer in Taiwan. Genes 2021, 12, 427. https://doi.org/10.3390/genes12030427
Lee K-L, Lai T-C, Wang Y-C, Shih P-C, Yang Y-C, Tsao TC-Y, Liu T-C, Wen Y-C, Chang L-C, Yang S-F, et al. Potential Impacts of Interleukin-17A Promoter Polymorphisms on the EGFR Mutation Status and Progression of Non-Small Cell Lung Cancer in Taiwan. Genes. 2021; 12(3):427. https://doi.org/10.3390/genes12030427
Chicago/Turabian StyleLee, Kai-Ling, Tsung-Ching Lai, Yao-Chen Wang, Pei-Chun Shih, Yi-Chieh Yang, Thomas Chang-Yao Tsao, Tu-Chen Liu, Yu-Ching Wen, Lun-Ching Chang, Shun-Fa Yang, and et al. 2021. "Potential Impacts of Interleukin-17A Promoter Polymorphisms on the EGFR Mutation Status and Progression of Non-Small Cell Lung Cancer in Taiwan" Genes 12, no. 3: 427. https://doi.org/10.3390/genes12030427