
Eating in the Amazon: Nutritional Status of the Riverine Populations and Possible Nudge Interventions

 ,
,  , , , ,
, , , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Amazonian Riverine Population
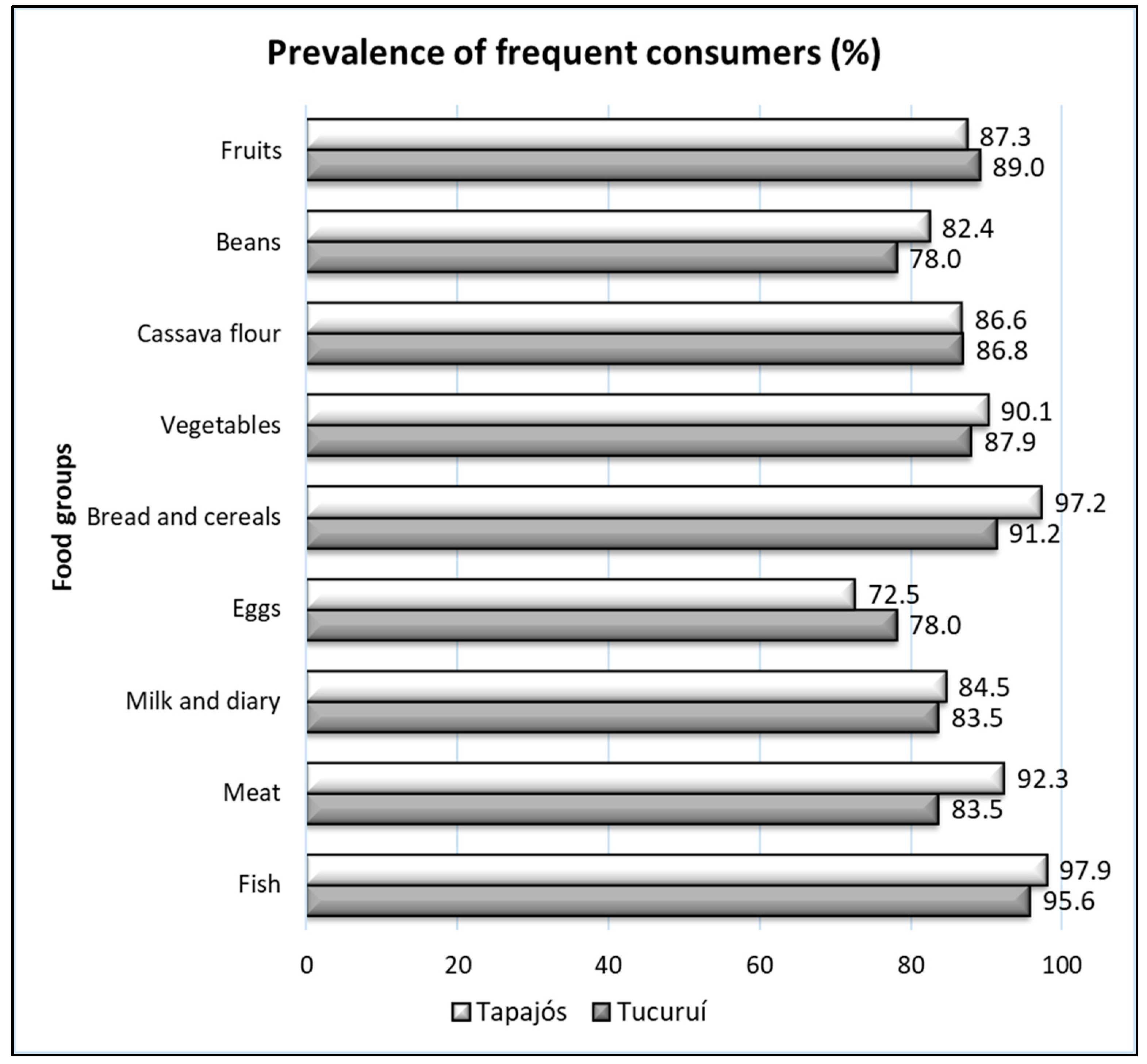
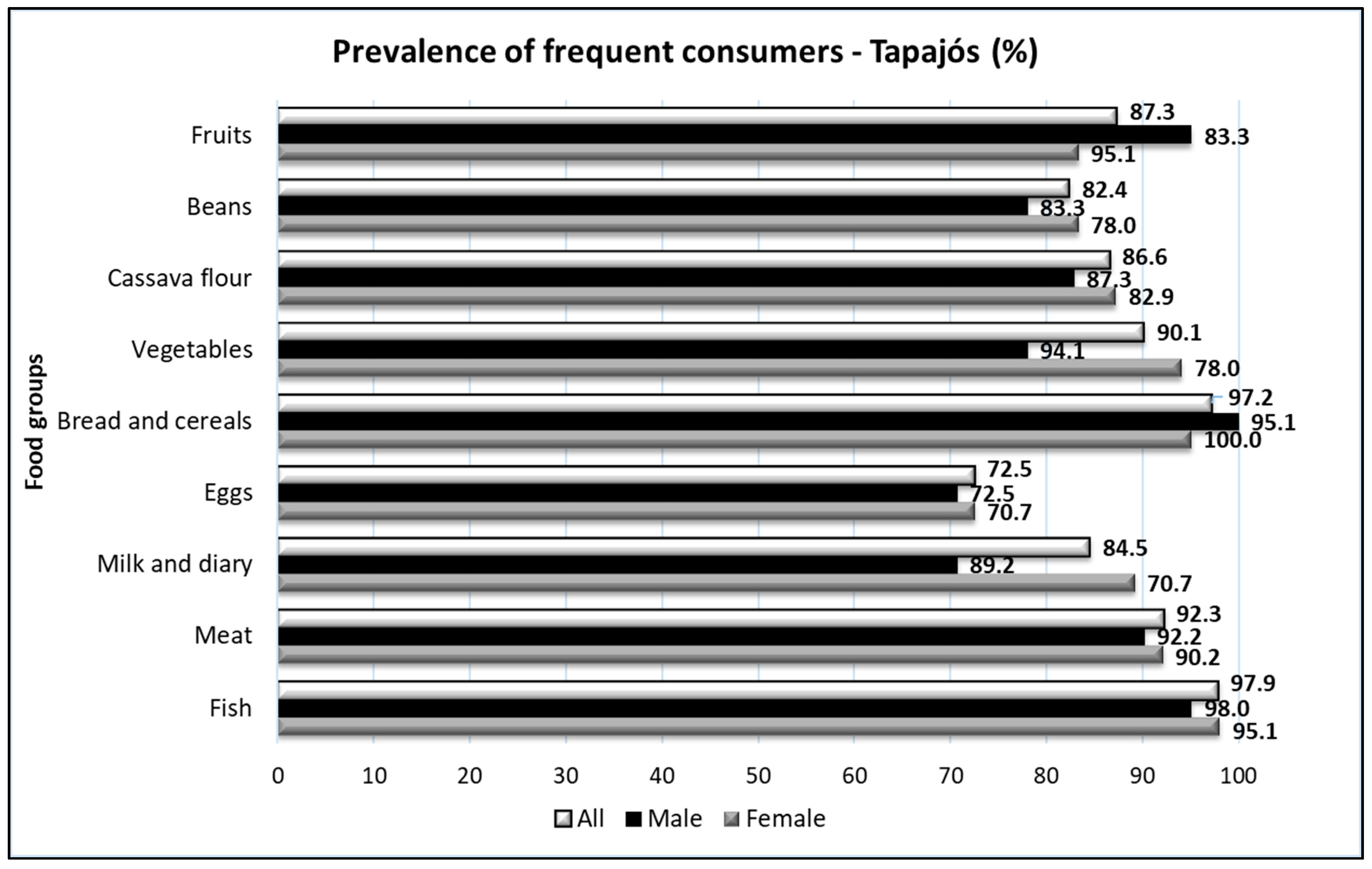
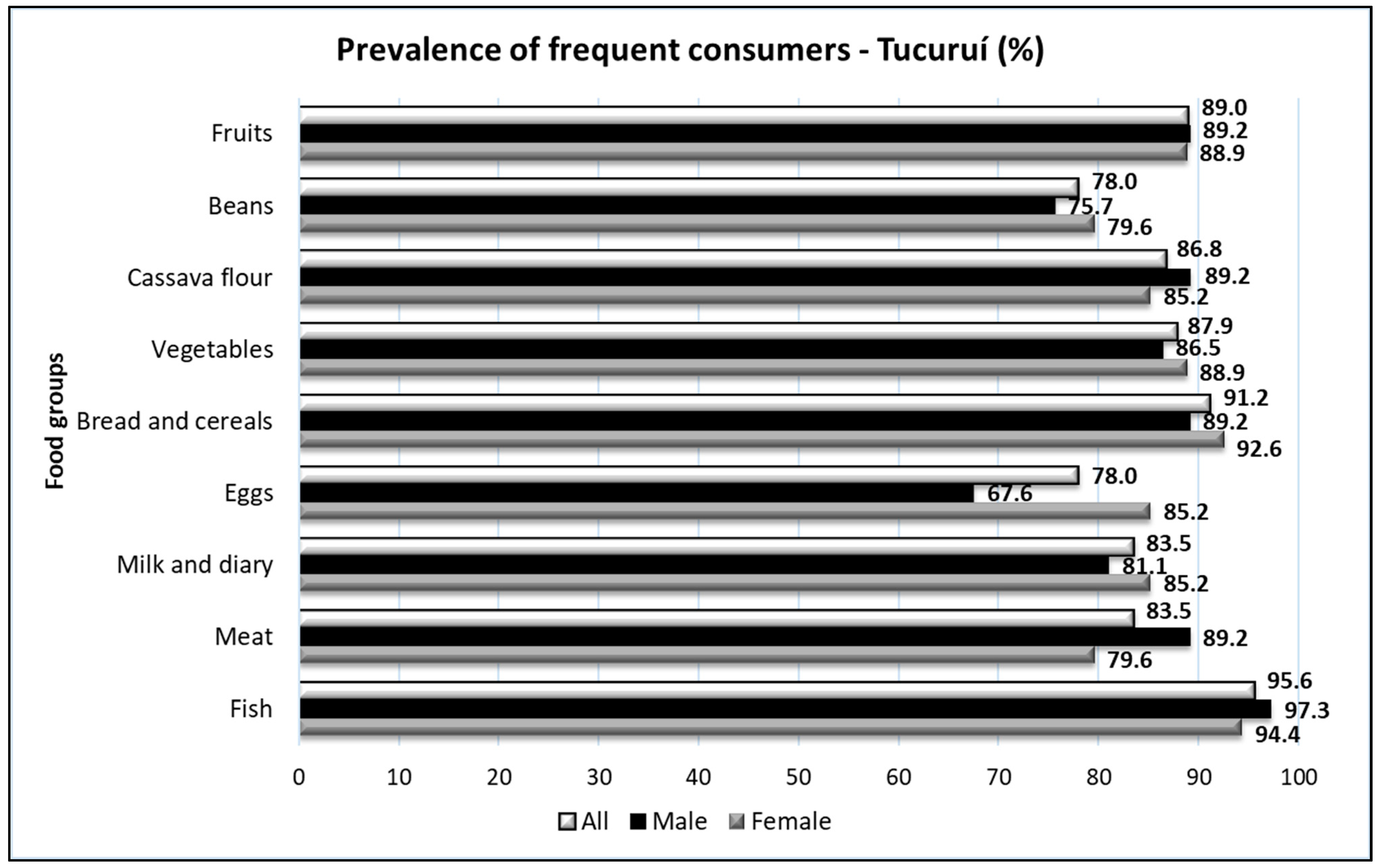
2.2. Identification and Prevalence of Consumers
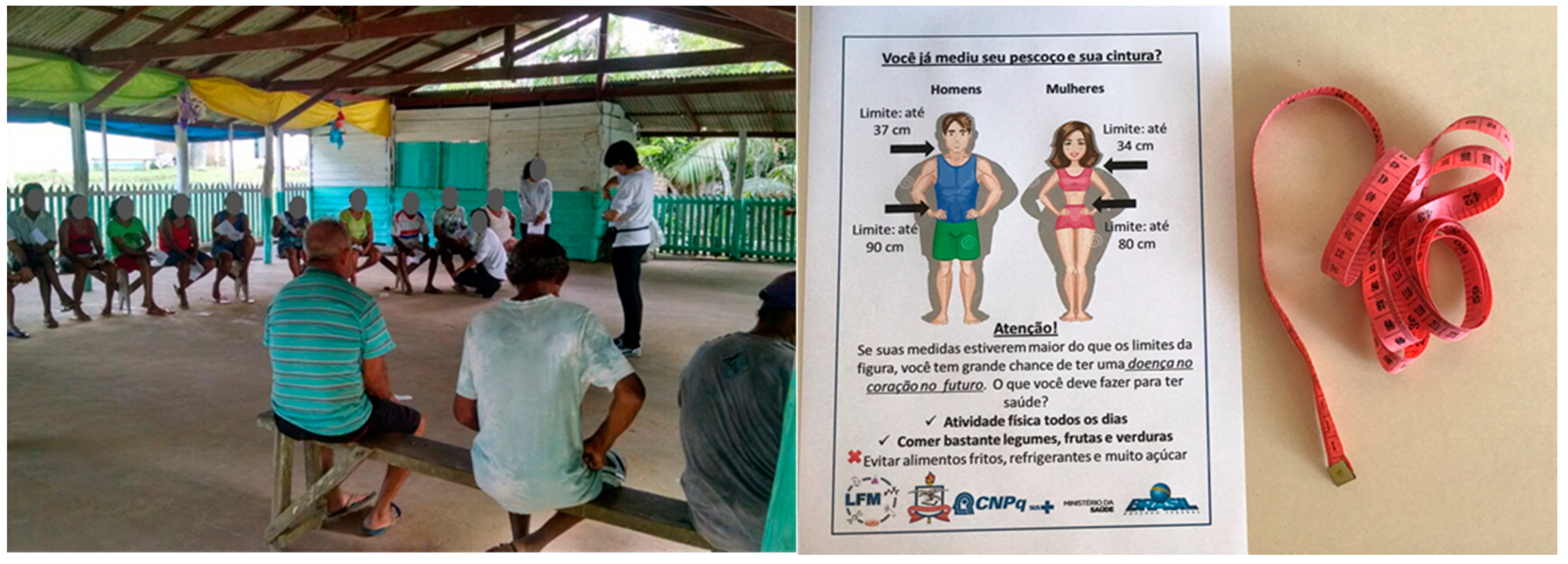
2.3. Anthropometric Evaluation
2.4. Statistical Analysis
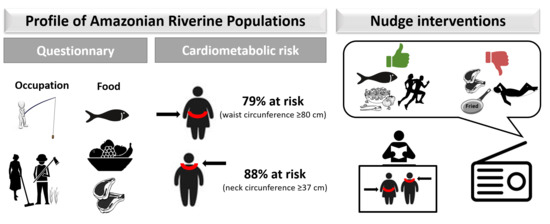
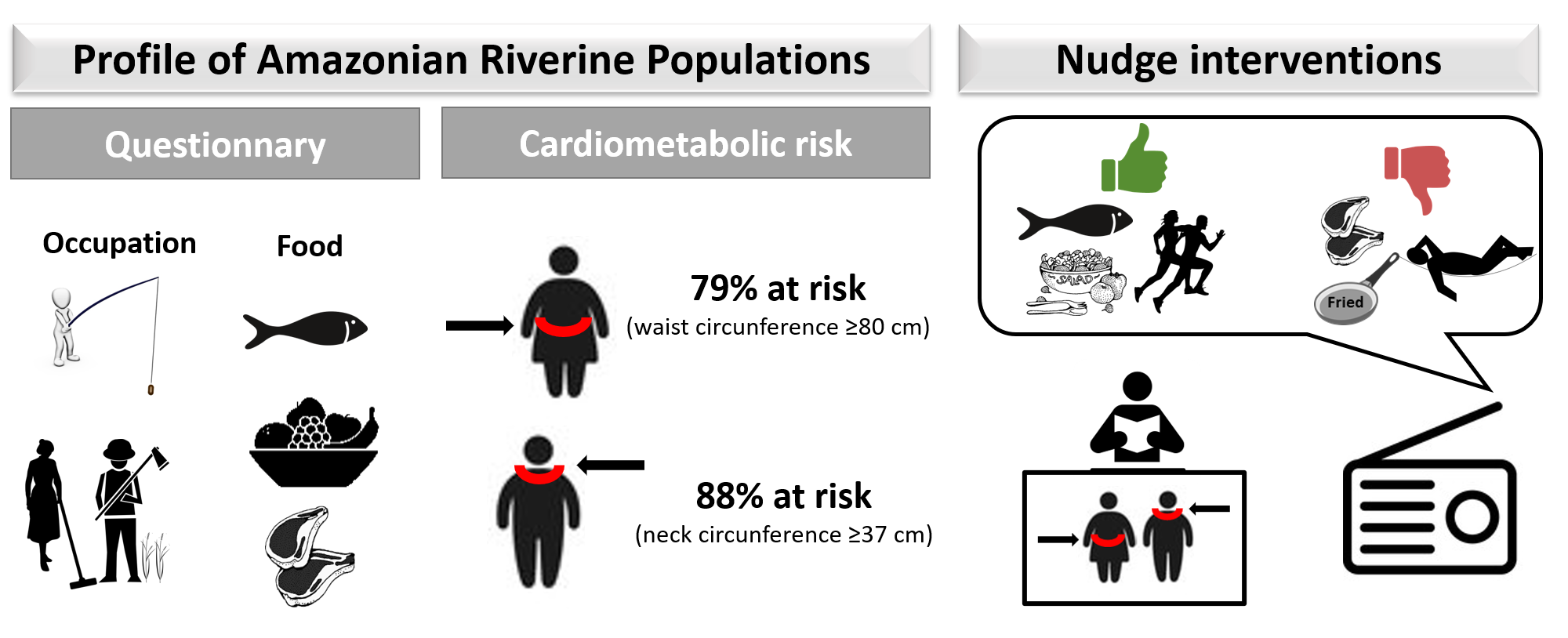
3. Results
4. Discussion
Tailored Behavioral Interventions: Some Possible Nudges Considering Behavior Analysis Principles
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Instituto Brasileiro de Geografia e Estatística (IBGE). Sinopse do censo Demográfico 2010 [Synopsis of the 2010 Census]; IBGE: Rio de Janeiro, Brazil, 2011. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv49230.pdf (accessed on 23 January 2021).
- Instituto de Pesquisa Econômica Aplicada (IPEA). Radar IDHM: Evolução do IDHM e de seus índices Componentes no Período de 2012 a 2017 [IDHM Radar: Evolution of the IDHM and Its Component Indices from 2012 to 2017]; IPEA: Brasilia, Brazil, 2019. Available online: https://www.ipea.gov.br/portal/images/stories/PDFs/livros/livros/190416_rada_IDHM.pdf (accessed on 12 January 2021).
- Crespo-Lopez, M.E.; Augusto-Oliveira, M.; Lopes-Araujo, A.; Santos-Sacramento, L.; Yuki Takeda, P.; Macchi, B.M.; do Nascimento, J.L.M.; Maia, C.S.F.; Lima, R.R.; Arrifano, G.P. Mercury: What can we learn from the Amazon? Environ. Int. 2021, 146, 106223. [Google Scholar] [CrossRef]
- Santos-Sacramento, L.; Arrifano, G.P.; Lopes-Araujo, A.; Augusto-Oliveira, M.; Albuquerque-Santos, R.; Takeda, P.Y.; Souza-Monteiro, J.R.; Macchi, B.M.; do Nascimento, J.L.M.; Lima, R.R.; et al. Human neurotoxicity of mercury in the Amazon: A scoping review with insights and critical considerations. Ecotoxicol. Environ. Saf. 2021, 208, 111686. [Google Scholar] [CrossRef]
- Berzas Nevado, J.J.; Rodriguez Martin-Doimeadios, R.C.; Guzman Bernardo, F.J.; Jimenez Moreno, M.; Herculano, A.M.; do Nascimento, J.L.; Crespo-Lopez, M.E. Mercury in the Tapajos River basin, Brazilian Amazon: A review. Environ. Int. 2010, 36, 593–608. [Google Scholar] [CrossRef] [PubMed]
- Fillion, M.; Mergler, D.; Sousa Passos, C.J.; Larribe, F.; Lemire, M.; Guimaraes, J.R. A preliminary study of mercury exposure and blood pressure in the Brazilian Amazon. Environ. Health 2006, 5, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piperata, B.A. Nutritional status of Ribeirinhos in Brazil and the nutrition transition. Am. J. Phys. Anthropol. 2007, 133, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Piperata, B.A.; Spence, J.E.; Da-Gloria, P.; Hubbe, M. The nutrition transition in amazonia: Rapid economic change and its impact on growth and development in Ribeirinhos. Am. J. Phys. Anthropol. 2011, 146, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. Nutrition Transition and the Global Diabetes Epidemic. Curr. Diab. Rep. 2015, 15, 64. [Google Scholar] [CrossRef] [PubMed]
- Arrifano, G.P.F.; Alvarez-Leite, J.I.; Souza-Monteiro, J.R.; Augusto-Oliveira, M.; Paraense, R.; Macchi, B.M.; Pinto, A.; Oria, R.B.; do Nascimento, J.L.M.; Crespo-Lopez, M.E. In the Heart of the Amazon: Noncommunicable Diseases and Apolipoprotein E4 Genotype in the Riverine Population. Int. J. Environ. Res. Public Health 2018, 15, 1957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Physical Status: The Use and Interpretation of Anthropometry—Report of a WHO Expert Committee; Thecnical Report Series No. 854; WHO: Geneva, Switherland, 1995; Available online: http://www.who.int/childgrowth/publications/physical_status/en/index.html (accessed on 15 February 2021).
- Thaler, R.H.; Sunstein, C.R. Nudge: Improving Decisions about Health, Wealth, and Happiness; Yale University Press: New Haven, CT, USA, 2008. [Google Scholar]
- Skinner, B.F. Science and Human Behavior; Free Press: New York, NY, USA, 1953. [Google Scholar]
- Skinner, B.F. Selection by consequences. Science 1981, 213, 501–504. [Google Scholar] [CrossRef] [Green Version]
- Arno, A.; Thomas, S. The efficacy of nudge theory strategies in influencing adult dietary behaviour: A systematic review and meta-analysis. BMC Public Health 2016, 16, 676. [Google Scholar] [CrossRef] [Green Version]
- Damgaard, M.T.; Nielsen, H.S. Nudging in education. Econ. Educ. Rev. 2018, 64, 313–342. [Google Scholar] [CrossRef]
- Ebert, P.; Freibichler, W. Nudge management: Applying behavioural science to increase knowledge worker productivity. J. Organ. Des. 2017, 6, 1–6. [Google Scholar] [CrossRef]
- Forberger, S.; Reisch, L.; Kampfmann, T.; Zeeb, H. Nudging to move: A scoping review of the use of choice architecture interventions to promote physical activity in the general population. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 77. [Google Scholar] [CrossRef] [Green Version]
- Graffeo, M.; Ritov, I.; Bonini, N.; Hadjichristidis, C. To make people save energy tell them what others do but also who they are: A preliminary study. Front. Psychol. 2015, 6, 1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korn, L.; Betsch, C.; Bohm, R.; Meier, N.W. Social nudging: The effect of social feedback interventions on vaccine uptake. Health Psychol. 2018, 37, 1045–1054. [Google Scholar] [CrossRef] [PubMed]
- Thaler, R.H.; Benartzi, S. Save More Tomorrow™: Using Behavioral Economics to Increase Employee Saving. J. Political Econ. 2004, 112, S164–S187. [Google Scholar] [CrossRef]
- Sunstein, C. Nudges that fail. Behav. Public Policy 2017, 1, 4–25. [Google Scholar] [CrossRef]
- Simon, C.; Tagliabue, M. Feeding the behavioral revolution: Contributions of behavior analysis to nudging and vice versa. J. Behav. Econ. Policy 2018, 2, 91–97. [Google Scholar]
- Passos, C.J.; Mergler, D.; Gaspar, E.; Morais, S.; Lucotte, M.; Larribe, F.; Davidson, R.; de Grosbois, S. Eating tropical fruit reduces mercury exposure from fish consumption in the Brazilian Amazon. Environ. Res. 2003, 93, 123–130. [Google Scholar] [CrossRef]
- Arrifano, G.P.F.; Martin-Doimeadios, R.C.R.; Jimenez-Moreno, M.; Ramirez-Mateos, V.; da Silva, N.F.S.; Souza-Monteiro, J.R.; Augusto-Oliveira, M.; Paraense, R.S.O.; Macchi, B.M.; do Nascimento, J.L.M.; et al. Large-scale projects in the amazon and human exposure to mercury: The case-study of the Tucurui Dam. Ecotoxicol. Environ. Saf. 2018, 147, 299–305. [Google Scholar] [CrossRef]
- Arrifano, G.P.F.; Martin-Doimeadios, R.C.R.; Jimenez-Moreno, M.; Fernandez-Trujillo, S.; Augusto-Oliveira, M.; Souza-Monteiro, J.R.; Macchi, B.M.; Alvarez-Leite, J.I.; do Nascimento, J.L.M.; Amador, M.T.; et al. Genetic Susceptibility to Neurodegeneration in Amazon: Apolipoprotein E Genotyping in Vulnerable Populations Exposed to Mercury. Front. Genet. 2018, 9, 285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Body Mass Index—BMI. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 12 April 2021).
- Cuppari, L. Nutrição Clínica no Adulto [Clinical Nutrition in Adults], 4th ed.; Manole: Barueri, SP, Brazil, 2014. [Google Scholar]
- Aswathappa, J.; Garg, S.; Kutty, K.; Shankar, V. Neck circumference as an anthropometric measure of obesity in diabetics. North. Am. J. Med. Sci. 2013, 5, 28–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, W.Y.; Yang, C.Y.; Shih, S.R.; Hsieh, H.J.; Hung, C.S.; Chiu, F.C.; Lin, M.S.; Liu, P.H.; Hua, C.H.; Hsein, Y.C.; et al. Measurement of Waist Circumference: Midabdominal or iliac crest? Diabetes Care 2013, 36, 1660–1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Waist Circumference and Waist–Hip Ratio: Report of a WHO Expert Consultation; WHO: Geneva, Switzerland, 2008; Available online: https://apps.who.int/iris/rest/bitstreams/53079/retrieve (accessed on 12 February 2021).
- Madden, A.M.; Smith, S. Body composition and morphological assessment of nutritional status in adults: A review of anthropometric variables. J. Hum. Nutr Diet. 2016, 29, 7–25. [Google Scholar] [CrossRef]
- De Paula Fonseca Arrifano, G.; Del Carmen Rodriguez Martin-Doimeadios, R.; Jimenez-Moreno, M.; Augusto-Oliveira, M.; Rogerio Souza-Monteiro, J.; Paraense, R.; Rodrigues Machado, C.; Farina, M.; Macchi, B.; do Nascimento, J.L.M.; et al. Assessing mercury intoxication in isolated/remote populations: Increased S100B mRNA in blood in exposed riverine inhabitants of the Amazon. Neurotoxicology 2018, 68, 151–158. [Google Scholar] [CrossRef]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist circumference as a vital sign in clinical practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef]
- Hallwass, G.; Silvano, R.A.M. Patterns of selectiveness in the Amazonian freshwater fisheries: Implications for management. J. Environ. Plan. Manag. 2016, 59, 1537–1559. [Google Scholar] [CrossRef]
- Adams, C.; Murrieta, R.S.S.; Sanches, R.A. Agricultura e alimentação em populações ribeirinhas das várzeas do Amazonas: Novas perspectivas [Agriculture and diet among riverine populations of the Amazonian floodplains: New perspectives]. Ambiente Soc. 2005, 8, 65–86. [Google Scholar] [CrossRef] [Green Version]
- Bôas, L.M.S.; Oliveira, D.C. A saúde nas comunidades ribeirinhas da região Norte brasileira: Revisão sistemática da literatura [Health in the riverine communities of North Brazilian region: Systematic literature review]. Investig. Qual. Saúde 2016, 2, 1386–1395. Available online: https://proceedings.ciaiq.org/index.php/ciaiq2016/article/view/896 (accessed on 10 January 2021).
- World Health Organization (WHO). Noncommunicable Diseases (NCD) Country Profiles; WHO: Geneva, Switzerland, 2014; Available online: http://apps.who.int/iris/bitstream/handle/10665/274512/9789241514620-eng.pdf (accessed on 12 February 2021).
- Brasil Ministerio da Saúde. Vigitel Brasil 2019: Vigilância de Fatores de Risco e Proteção Para Doenças crônicas por Inquérito Telefoônico [Surveillance of Risk and Protective Factors for Chronic Diseases by Telephone Survey]; Ministerio da Saúde: Brasília, Brazil, 2020. Available online: https://portalarquivos.saude.gov.br/images/pdf/2020/April/27/vigitel-brasil-2019-vigilancia-fatores-risco.pdf (accessed on 12 February 2021).
- Assyov, Y.; Gateva, A.; Tsakova, A.; Kamenov, Z. A comparison of the clinical usefulness of neck circumference and waist circumference in individuals with severe obesity. Endocr. Res. 2017, 42, 6–14. [Google Scholar] [CrossRef]
- Browder, J.O.; Godfrey, B.J. Rainforest Cities, Urbanization, Development, and Globalization of the Brazilian Amazon; Columbia University Press: New York, NY, USA, 1997. [Google Scholar]
- Goodarzi, M.O. Genetics of obesity: What genetic association studies have taught us about the biology of obesity and its complications. Lancet Diabetes Endocrinol. 2018, 6, 223–236. [Google Scholar] [CrossRef]
- Staiano, A.E.; Broyles, S.T.; Gupta, A.K.; Katzmarzyk, P.T. Ethnic and sex differences in visceral, subcutaneous, and total body fat in children and adolescents. Obesity 2013, 21, 1251–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadekar, T.; Dudeja, P.; Basu, I.; Vashisht, S.; Mukherji, S. Correlation of visceral body fat with waist-hip ratio, waist circumference and body mass index in healthy adults: A cross sectional study. Med. J. Armed Forces India 2020, 76, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Küçük, U.; Küçük, H.O.; Cüce, F.; Balta, S. Relationship between neck circumference and epicardial fat thickness in a healthy male population. Arq. Bras. Cardiol. 2016, 107, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Rabkin, S.W. Epicardial fat: Properties, function and relationship to obesity. Obes. Rev. 2007, 8, 253–261. [Google Scholar] [CrossRef]
- Iacobellis, G.; Barbaro, G. The double role of epicardial adipose tissue as pro- and anti-inflammatory organ. Horm. Metab. Res. 2008, 40, 442–445. [Google Scholar] [CrossRef]
- Preis, S.R.; Massaro, J.M.; Hoffmann, U.; D’Agostino, R.B., Sr.; Levy, D.; Robins, S.J.; Meigs, J.B.; Vasan, R.S.; O’Donnell, C.J.; Fox, C.S. Neck circumference as a novel measure of cardiometabolic risk: The Framingham Heart study. J. Clin. Endocrinol. Metab. 2010, 95, 3701–3710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, Y.; Wan, X.; Li, X.; Jin, E.; Li, X. Neck circumference and future cardiovascular events in a high-risk population--A prospective cohort study. Lipids Health Dis. 2016, 15, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desnoyers, M.; Gilbert, K.; Rousseau, G. Cardioprotective Effects of Omega-3 Polyunsaturated Fatty Acids: Dichotomy between Experimental and Clinical Studies. Mar. Drugs 2018, 16, 234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez Martin-Doimeadios, R.C.; Berzas Nevado, J.J.; Guzman Bernardo, F.J.; Jimenez Moreno, M.; Arrifano, G.P.; Herculano, A.M.; do Nascimento, J.L.; Crespo-Lopez, M.E. Comparative study of mercury speciation in commercial fishes of the Brazilian Amazon. Environ. Sci. Pollut. Res. Int. 2014, 21, 7466–7479. [Google Scholar] [CrossRef]
- Daneshmand, R.; Kurl, S.; Tuomainen, T.P.; Virtanen, J.K. Associations of serum n-3 and n-6 PUFA and hair mercury with the risk of incident stroke in men: The Kuopio Ischaemic Heart Disease Risk Factor Study (KIHD). Br. J. Nutr. 2016, 115, 1851–1859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genchi, G.; Sinicropi, M.S.; Carocci, A.; Lauria, G.; Catalano, A. Mercury Exposure and Heart Diseases. Int. J. Environ. Res. Public Health 2017, 14, 74. [Google Scholar] [CrossRef] [Green Version]
- Camelo Ldo, V.; de Figueiredo, R.C.; Oliveira-Campos, M.; Giatti, L.; Barreto, S.M. Healthy behavior patterns and levels of schooling in Brazil: Time trend from 2008 to 2013. Cien. Saude Colet. 2016, 21, 1011–1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arrifano, G.P.F.; Lichtenstein, M.P.; Souza-Monteiro, J.R.; Farina, M.; Rogez, H.; Carvalho, J.C.T.; Sunol, C.; Crespo-Lopez, M.E. Clarified Acai (Euterpe oleracea) Juice as an Anticonvulsant Agent: In Vitro Mechanistic Study of GABAergic Targets. Oxid. Med. Cell Longev. 2018, 2018, 2678089. [Google Scholar] [CrossRef] [Green Version]
- Crespo-Lopez, M.E.; Soares, E.S.; Macchi, B.M.; Santos-Sacramento, L.; Takeda, P.Y.; Lopes-Araujo, A.; Paraense, R.S.O.; Souza-Monteiro, J.R.; Augusto-Oliveira, M.; Luz, D.A.; et al. Towards Therapeutic Alternatives for Mercury Neurotoxicity in the Amazon: Unraveling the Pre-Clinical Effects of the Superfruit Acai (Euterpe oleracea, Mart.) as Juice for Human Consumption. Nutrients 2019, 11, 2585. [Google Scholar] [CrossRef] [Green Version]
- Souza-Monteiro, J.R.; Arrifano, G.P.F.; Queiroz, A.; Mello, B.S.F.; Custodio, C.S.; Macedo, D.S.; Hamoy, M.; Paraense, R.S.O.; Bittencourt, L.O.; Lima, R.R.; et al. Antidepressant and Antiaging Effects of Acai (Euterpe oleracea Mart.) in Mice. Oxid. Med. Cell Longev. 2019, 2019, 3614960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souza-Monteiro, J.R.; Hamoy, M.; Santana-Coelho, D.; Arrifano, G.P.; Paraense, R.S.; Costa-Malaquias, A.; Mendonca, J.R.; da Silva, R.F.; Monteiro, W.S.; Rogez, H.; et al. Anticonvulsant properties of Euterpe oleracea in mice. Neurochem. Int. 2015, 90, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Micha, R.; Michas, G.; Lajous, M.; Mozaffarian, D. Processing of meats and cardiovascular risk: Time to focus on preservatives. BMC Med. 2013, 11, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, A.K.; Cole-Lewis, H.; Bernhardt, J.M. Mobile text messaging for health: A systematic review of reviews. Annu. Rev. Public Health 2015, 36, 393–415. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BMI (kg/m²) | WC (cm) at CVD Risk | WHR at CVD Risk | NC (cm) at CVD Risk | |
|---|---|---|---|---|
| <8.5 | Underweight | ≥80 (female) | >0.85 (female) | >34 (female) |
| 18.5–24.9 | Normal Weight | ≥90 (male) | >1.0 (male) | >37 (male) |
| 25.0–29.9 | Pre-obesity | |||
| 30.0–34.9 | Obesity I | |||
| 35.0–39.9 | Obesity II | |||
| ≥40 | Obesity III | |||
| Characteristics | Total | Tapajós | Tucuruí | P (Tap vs. Tuc) | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||
| Gender | Male | 78 | 41 | 29 | 37 | 41 | 0.065 a |
| Female | 156 | 102 | 71 | 54 | 59 | ||
| Total | 234 | 143 | 100 | 91 | 100 | ||
| Age | 44 (31–50) | 40 (30–49) | 47 (37–51) | 0.014 b | |||
| Weight (kg) | 65.6 (56.6–75.2) | 65.6 (56.2–75.0) | 65.6 (56.7–76.0) | 0.908 b | |||
| Height (cm) | 157 (151–164) | 157 (152–164) | 157 (150–166) | 0.902 b | |||
| BMI | 25.8 (23.0–29.7) | 25.8 (22.9–29.5) | 25.5 (23.0–30.1) | 0.992 b | |||
| WC (cm) | 90.5 ± 11.9 | 90.3 ± 11.9 | 90.6 ± 11.8 | 0.838 c | |||
| HC (cm) | 101 (96–107) | 101 (95–107) | 102 (96–107) | 0.913 b | |||
| WHR | 0.90 (0.84–0.94) | 0.89 (0.84–0.94) | 0.90 (0.84–0.95) | 0.855 b | |||
| NC (cm) | 36 (34–39) | 37 (34–39) | 36 (34–40) | 0.919 b | |||
| Prevalence (and Number of Participants) According to BMI | ||||||
|---|---|---|---|---|---|---|
| Status | Male | Female | Total | |||
| Tapajós | Tucuruí | Tapajós | Tucuruí | Tapajós | Tucuruí | |
| Underweight | 5% (2) | 3% (1) | 2% (2) | 0% (0) | 3% (4) | 1% (1) |
| Normal Weight | 39% (16) | 35% (13) | 41% (42) | 48% (26) | 40% (57) | 43% (39) |
| Pre-obesity/Obesity | 56% (23) | 62% (23) | 57% (58) | 52% (28) | 57% (82) | 56% (51) |
| Total | 100% (41) | 100% (37) | 100% (102) | 100% (54) | 100% (143) | 100% (91) |
| Prevalence (and Number of Participants) According to BMI in Pre-Obesity/Obesity | ||||||
|---|---|---|---|---|---|---|
| Male | Female | Total | ||||
| Tapajós | Tucuruí | Tapajós | Tucuruí | Tapajós | Tucuruí | |
| Pre-Obesity | 87% (20) | 60.9% (14) | 53.4% (31) | 50% (14) | 63% (52) | 54.9% (28) |
| Obesity I | 13% (3) | 34.8% (8) | 32.8% (19) | 35.7% (10) | 27.2% (22) | 35.3% (18) |
| Obesity II | 0% (0) | 0% (0) | 12.1% (7) | 14.3% (4) | 8.6% (7) | 7.8% (4) |
| Obesity III | 0% (0) | 4.3% (1) | 1.7% (1) | 0% (0) | 1.2% (1) | 2% (1) |
| Total | 100% (23) | 100% (23) | 100% (58) | 100% (28) | 100% (82) | 100% (51) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machado, C.L.R.; Crespo-Lopez, M.E.; Augusto-Oliveira, M.; Arrifano, G.d.P.; Macchi, B.d.M.; Lopes-Araújo, A.; Santos-Sacramento, L.; Souza-Monteiro, J.R.; Alvarez-Leite, J.I.; Souza, C.B.A.d. Eating in the Amazon: Nutritional Status of the Riverine Populations and Possible Nudge Interventions. Foods 2021, 10, 1015. https://doi.org/10.3390/foods10051015
Machado CLR, Crespo-Lopez ME, Augusto-Oliveira M, Arrifano GdP, Macchi BdM, Lopes-Araújo A, Santos-Sacramento L, Souza-Monteiro JR, Alvarez-Leite JI, Souza CBAd. Eating in the Amazon: Nutritional Status of the Riverine Populations and Possible Nudge Interventions. Foods. 2021; 10(5):1015. https://doi.org/10.3390/foods10051015
Chicago/Turabian StyleMachado, Camila Lorena Rodrigues, Maria Elena Crespo-Lopez, Marcus Augusto-Oliveira, Gabriela de Paula Arrifano, Barbarella de Matos Macchi, Amanda Lopes-Araújo, Letícia Santos-Sacramento, José Rogério Souza-Monteiro, Jacqueline Isaura Alvarez-Leite, and Carlos Barbosa Alves de Souza. 2021. "Eating in the Amazon: Nutritional Status of the Riverine Populations and Possible Nudge Interventions" Foods 10, no. 5: 1015. https://doi.org/10.3390/foods10051015