
The Possible Role of SARS-CoV-2 in Male Fertility: A Narrative Review
by
 , , , and
, , , and
Claudia Leanza
,
Laura M. Mongioì
*,
Rossella Cannarella
,
Sandro La Vignera
,
Rosita A. Condorelli
and
Aldo E. Calogero
Department of Clinical and Experimental Medicine, University of Catania, Policlinico “G. Rodolico”, Via S. Sofia 78, 95123 Catania, Italy
*
Author to whom correspondence should be addressed.
Endocrines 2022, 3(3), 552-559; https://doi.org/10.3390/endocrines3030046
Submission received: 1 June 2022
/
Revised: 17 August 2022
/
Accepted: 29 August 2022
/
Published: 5 September 2022
(This article belongs to the Section Andrology and Male Sexual Function)
{kind=link}
Abstract
:The spread of severe acute respiratory syndrome—Coronavirus 2 (SARS-CoV-2) around the world has rapidly sparked the interest of the scientific community to discover its implications in human health. Many studies have suggested that SARS-CoV-2 is directly or indirectly involved in the male reproductive tract impairment. Some evidence supports the possible role of the virus in male infertility. Therefore, this review aims to summarize the relationship between the male urogenital tract, male fertility, and the gonadal hormone profile. The testis is one of the organs with the highest expression of the angiotensin-converting enzyme (ACE) 2-receptor that allows the virus to penetrate human cells. Orchitis is a possible clinical manifestation of COVID-19 and testicular damage has been found on autopsy in the testes of patients who died from the disease. SARS-CoV-2 infection can compromise the blood-testis barrier, favoring testicular damage and the production of anti-sperm autoantibodies. Some studies have detected the presence of SARS-CoV-2 in semen and a high percentage of patients with COVID-19 have altered sperm parameters compared to controls. Finally, lower testosterone levels, higher luteinizing hormone (LH) levels, and decreased follicle-stimulating (FSH)/LH and testosterone/LH ratios suggest primary testicular damage. In conclusion, further studies are needed to evaluate the exact mechanisms by which SARS-CoV-2 affects the male reproductive system and fertility and to evaluate the reversibility of its long-term effects.
1. Introduction
Severe acute respiratory syndrome—Coronavirus 2 (SARS-CoV-2) —is a pathogenic coronavirus that caused the pandemic of the acute respiratory disease called COVID-19. According to World Health Organization (WHO) epidemiological data (2 August 2022), 583,238,204 cases of COVID-19 have been registered in the world, with 6,422,235 deaths, and 553,818,416 patients recovered (https://www.worldometers.info/coronavirus/, accessed on 2 August 2022).
SARS-CoV2 can affect various organs and systems [1]. Even the gonadal function can be involved in the infection, and this may impair fertility. In this regard, some molecular characteristics of SARS-CoV-2 suggest its presence in the male reproductive system and this, together with mechanisms of hormonal nature, could cause infertility. However, data on the presence of SARS-CoV-2 in the seminal fluid of infected patients and the effects on sperm parameters are few and controversial [2].
In this review, we summarize all the possible mechanisms through which the virus can affect the male reproductive system and, therefore, male fertility.
1.1. Angiotensin-Converting Enzyme Receptor 2 and Testis
It is widely known that the angiotensin-converting enzyme (ACE) 2 receptor is used by SARS-CoV-2 to penetrate human cells [3]. It is also known that COVID-19 appears to have a higher mortality rate in men due to a possible sex-dependent susceptibility that may result from a higher ACE2 expression in men [4]. In this regard, Meng-Yuan Li and colleagues analyzed ACE2 expression in different human tissues and found that the kidney, thyroid, heart, adipose tissue, small intestine, and testis have the highest level of ACE2 expression [5]. These findings suggest that SARS-CoV-2 can affect other human tissues in addition to the lungs, including the testis. An immunohistochemical study showed that ACE2 is also expressed in both seminiferous tubules and Leydig cells [6]. This outcome has been confirmed by Wang and colleagues who showed the presence of ACE2 in spermatogonia and Leydig and Sertoli cells [7]. Shen and colleagues showed that Sertoli cells are the highest ACE2 mRNA positive cluster by a scRNA-seq analysis on human testicular cells. The ACE2 mRNA has also been found in spermatogonia stem cells and Leydig cells [8]. The same study showed a higher positive rate of ACE2 in testes of infertile patients than in those of fertile men. These findings suggest that SARS-CoV-2 may cause male infertility through an ACE2-related pathway and, on the other hand, that infertile men could be more susceptible to developing COVID-19. Even an age-related difference in ACE2 mRNA expression has emerged in this study, with a higher positive rate in mid-age than young men [8].
The ACE2 is part of the renin-angiotensin-aldosterone system (RAAS), which plays a role in the male reproductive system, including the regulation of steroidogenesis, spermatogenesis, epididymal contractility, and sperm function [9,10]. Angiotensin II, for example, seems to be involved in sperm motility [11]. The ACE2 catalyzes the generation of angiotensin 1–7 by cleaving the C-terminal amino acid of angiotensin II, suggesting that ACE2 provides a negative feedback regulation on the RAAS [12]. In this regard, an interesting finding is that ACE2-positive spermatogonia in SARS-CoV-2 patients appear to have impaired spermatogenesis [13].
These results also suggest the capacity of SARS-CoV-2 to penetrate within the cells of the male reproductive tract thanks to the presence of ACE2. This may result in spermatogenesis and steroidogenesis impairment, probably through an ACE2-related mechanism.
1.2. Orchitis and Autoimmunity
As SARS-CoV has been shown to cause orchitis [1,14], it can also be hypothesized that SARS-CoV-2 may have a similar effect.
Some authors have reported cases of patients with COVID-19 complaining of an unusual symptom which is testicular pain. La Marca and colleagues, for example, described the case of a 43-year-old patient who presented to the emergency room due to testicular pain that preceded the onset of dyspnea by twelve hours. Testicular ultrasound scan showed a picture of epididymitis [15]. In another study, nearly 11% of patients with COVID-19 had testicular pain or epididymitis-orchitis [16]. At autopsy, three out of six testes of patients who died from COVID-19 showed impaired spermatogenesis. By transmission electron microscopy, they found the virus in the testicular tissue in only one patient and the same sample showed macrophage and leukocyte infiltration on hematoxylin/eosin staining [17]. The presence of SARS-CoV-2 has been reported in the testes of COVID-19 patients associated with impaired spermatogenesis [18].
Li and colleagues suggested an elevated testicular immune response as a cause of impaired sperm parameters and testicular damage. Indeed, they reported edema, interstitial congestion, and red blood cells at the autopsy of testicular and epididymal samples from patients who died from COVID-19. They also found elevated seminal levels of IL-6 and TNF-α. An autoimmune origin of orchitis has been proposed by these authors [19]. The possible mechanism through which SARS-CoV-2 can favor autoimmune orchitis could be the compromise of the blood-testis barrier which normally prevents the passage of molecules and the contact between testicular antigens and the immune system; hence the production of autoantibodies [20]. The compromise of the barrier could derive from the aforementioned involvement of Sertoli cells because it is formed by junctions between these cells [21]. Furthermore, through the autoimmune phenomenon, SARS-CoV-2 infection can promote the production of anti-sperm antibodies (ASA), which are associated with lower sperm concentration and motility [22]. In a study conducted on COVID-19 patients, IgA ASA was found in 65 out of 106 patients (61%), while IgG ASA was less frequently present [23]. The same study showed a strong correlation between sperm abnormalities and the titers of SARS-CoV-2 IgG antibodies against spike 1 and the receptor-binding domain of spike 1, suggesting a possible implication of immune mechanism in the involvement of the male reproductive system during COVID-19 [23]. This hypothesis suggests a possible negative effect of SARS-CoV-2 vaccines on male infertility. Although it is not the aim of our study, it is noteworthy that Corona and colleagues reported a possible positive effect of COVID-19 mRNA vaccines on sperm concentration, whereas no significant effect was found on sperm motility. However, the available data are still too few [24].
Ultimately, we can hypothesize that SARS-CoV-2 can cause testicular damage by both direct and indirect mechanisms.
1.3. SARS-CoV-2 in Semen and Sperm Parameters in COVID-19 Patients
Several viruses have shown their ability to reach the human semen, such as Zika, HIV, and mumps virus [25,26,27]. Conflicting results have emerged from studies that evaluated the presence of SARS-CoV-2 in the semen of infected patients. Some studies did not show the presence of SARS-CoV-2 in semen samples [23,28,29,30]. In contrast, Machado and colleagues found SARS-CoV-2 RNA in one of 15 semen samples on infected patients [31], while Diangeng Li and colleagues showed that 6 out of 38 patients had SARS-CoV-2 in their semen samples. Two of these patients collected the specimen at the acute phase of the infection, while the other four after recovery [32]. A recent review showed that the detection rate of SARS-CoV-2 in semen is inversely related to COVID-19 diagnosis timing. In particular, it was significantly higher in those studies that evaluated samples collected less than 11 days after the diagnosis. Another interesting finding reported by the authors of this review is that the detection rate was higher in low-quality studies. This made them suspect the possibility of semen contamination from respiratory droplets, hands, feces, or urine [24]. Hence, further studies are needed to establish whether SARS-CoV-2 is present in semen, possibly by paying attention to the time between diagnosis of infection/onset of symptoms and semen collection. In this regard, it cannot be excluded that the virus may be present in the acute phase of the disease to disappear later.
As for sperm parameters, Temiz and colleagues reported that patients with COVID-19 had only teratozoospermia but they attributed this abnormality to the fever that affected these patients [33]. Accordingly, the negative impact of fever on sperm parameters has been known for a long time [34]. However, Gilbert and colleagues demonstrated no correlation between the severity of COVID-19 and the presence of fever with sperm characteristics [23]. Pazir et al., compared pre- and post-COVID-19 semen analysis and found that sperm motility and the total motile sperm count were the parameters that showed a significant reduction after mild COVID-19, that is having one of the symptoms of the disease without having lung involvement on chest imaging [35]. In another study, 25% of patients who recovered from COVID-19 were oligo-, crypto-, or azoospermic. The degree of these sperm abnormalities is significantly related to the COVID-19 severity [36]. Li et al., analyzed sperm parameters of 21 patients that had offspring through natural pregnancy (therefore considered fertile males) and observed oligozoospermia in nine of them. Furthermore, the sperm concentration in COVID-19 patients was significantly lower compared with the control group [17]. Another study on COVID-19 patients’ semen samples showed higher levels of ACE2 enzymatic activity, interleukin (IL)-1β, IL-6, IL-8, IL-10, transforming growth factor (TGF)-β, tumor necrosis factor (TNF)-α, interferon (IFN)-α, IFN-γ, reactive oxygen species (ROS), caspase-8, caspase-9, and caspase-3 activity in their seminal plasma. These correlated with impaired semen volume, progressive motility, sperm morphology, sperm concentration, and total sperm count [37]. Best et al., evaluated 30 semen samples with a median duration between the positivity of SARS-CoV-2 and semen collection of 37 days. The median total sperm number was 12.5 million. Five men completed a follow-up by collecting semen after 3 months and the median total sperm count was 18 million [38]. Guo et al., examined 41 semen samples at a median time of 56 days after hospital discharge. They found that sperm concentration and total and progressive motility were significantly reduced if compared with the control group. Twenty-two patients provided a second sample after 29 days from the first one and sperm number and motility increased, suggesting a potential recovery of sperm parameters [39]. Purpura and collaborators conducted a study on seven COVID-19 patients: one patient had severe oligozoospermia (<1 million/mL) and his sperm sample was qRT-PCR positive after 81 days from symptoms onset. The authors attributed the detection of SARS-CoV-2 during the late convalescent phase to the disease severity [40]. A study conducted on 120 Belgian men showed that SARS-CoV2 was not present in any semen sample (neither in the short period: 0–31 days). Their semen analysis showed that about a quarter of them was oligozoospermic, 44.1% had asthenozoospermia, and two thirds had teratozoospermia. Only 24.6% of patients had normal sperm parameters. The authors found out that mean progressive motility had a gradual recovering in time lapse; in fact, it was reduced in 60% of men tested after less than a month after infection, while it was low only in the 28% of men tested after two months. Mean sperm count and total motility, showed to have the same trend of mean progressive motility, while the percentage of men with abnormal morphology did not show substantial differences in the time lapse after COVID-19 infection, settling between 77 and 78%. The same study evaluated sperm DNA fragmentation, finding out that DNA damage was more pronounced within the first month after COVID-19 infection [23]. These data suggest a tendency of COVID-19-related sperm impairment towards reversibility.
Respiratory viral infections, including SARS-CoV-2, are associated with ROS overproduction and, therefore, increased oxidative stress [41]. The ROS impair sperm function by acting at macro and micro levels. The latter includes lipid peroxidation of sperm membranes and intracellular oxidative damage, in particular sperm DNA fragmentation [42], which is a bio-functional sperm parameter that plays a relevant role in fertility by ensuring fertilization, embryo implantation, and development [43].
Finally, Insulin-like factor-3 was found markedly reduced in testicular tissue of COVID-19 patients and even E3 ubiquitin-protein ligase, an important enzyme for spermatogenesis, and dynein regulatory complex subunit-7, essential for sperm motility, was found reduced in COVID-19 patients, suggesting an impairment of spermatogenesis and a possible mechanism of SARS-CoV-2-related sperm damage [44].
In conclusion, different studies have found impaired sperm parameters in patients with COVID-19. Ideally, future studies should be done on patients with COVID-19 that had previously undergone at least one semen analysis to compare pre- and post-COVID sperm parameters. It would also be of interest to understand the mechanism(s) by which spermatogenesis is affected in these patients and to evaluate the reversibility or not of this impairment. Are impaired sperm parameters just a consequence of additional factors, such as fever that increases the testicular temperature causing germinal cells apoptosis? [45]. Could this virus be able to bind spermatozoa making them uncapable to move or to fecundate?
1.4. Sex Hormone Levels
Another element that supports the effect of SARS-CoV-2 on male gonadal function is the evidence of altered levels of sex hormones in patients with COVID-19. Studies have shown low testosterone levels, high luteinizing hormone (LH) levels, and decreased testosterone/LH and follicle stimulating hormone (FSH)/LH ratios, suggesting primary testicular damage and, in particular, in the Leydigian compartment [46,47,48,49]. Ma and colleagues reported a relationship between decreased testosterone/LH ratio and the clinical characteristics of patients with COVID-19. In particular, they found a negative correlation between the testosterone/LH ratio and C-reactive protein levels [49], the increase of which is observed in patients with severe COVID-19 [50]. Kadihasanoglu and colleagues affirmed that more serious COVID-19 provokes a greater reduction of serum testosterone levels and prolongs the hospitalization length [48]. Another repercussion of COVID-19 seems to be erectile dysfunction [45]. Low testosterone levels could explain this disorder in these patients, even though erectile dysfunction could arise from a COVID-induced endothelial dysfunction [45].
2. Conclusions
The literature shows that SARS-CoV-2 could cause male infertility (Figure 1). However, further studies are needed to better understand the mechanism by which the virus affects testicular function and whether this effect is reversible or not. It is known that SARS-CoV-2 can reach the testis. This is demonstrated by the presence of SARS-CoV2 RNA in the testis and semen of COVID-19 patients. In this regard, further studies are needed to understand where the virus is exactly localized, if it is just in suspension or it binds to spermatozoa, if it is able to replicate and how long it could survive in semen.
SARS-CoV-2 may cause orchitis and testicular damage by direct and indirect mechanisms. The finding that patients with COVID-19 have hypotestosteronemia and high levels of LH adds further evidence for primary testicular damage involving the Leydig cells. Finally, studies have shown that COVID-19 patients have a higher percentage of impaired sperm parameters and, in particular, morphology, motility, and concentration.
Author Contributions
Conceptualization: L.M.M., C.L., A.E.C.; Investigation: C.L.; Methodology: C.L., L.M.M.; Supervision: R.C., S.L.V., R.A.C.; Validation: A.E.C., S.L.V.; R.A.C., R.C.; Visualization: A.E.C., S.L.V.; R.A.C., R.C.; Writing—original draft: C.L., L.M.M.; Writing—review & editing: A.E.C., S.L.V.; R.A.C., R.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
References
- Mongioì, L.M.; Barbagallo, F.; Condorelli, R.A.; Cannarella, R.; Aversa, A.; La Vignera, S.; Calogero, A.E. Possible long-term endocrine-metabolic complications in COVID-19: Lesson from the SARS model. Endocrine 2020, 68, 467–470. [Google Scholar] [CrossRef] [PubMed]
- Verrienti, P.; Cito, G.; Di Maida, F.; Tellini, R.; Cocci, A.; Minervini, A.; Natali, A. The impact of COVID-19 on the male genital tract: A qualitative literature review of sexual transmission and fertility implications. Clin. Exp. Reprod. Med. 2022, 49, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Chen, P.; Wang, J.; Feng, J.; Zhou, H.; Li, X.; Zhong, W.; Hao, P. Evolution of the novel coronavirus from the ongoing Wuhan outbreak and modeling of its spike protein for risk of human transmission. Sci. China Life Sci. 2020, 63, 457–460. [Google Scholar] [CrossRef]
- La Vignera, S.; Cannarella, R.; Condorelli, R.A.; Torre, F.; Aversa, A.; Calogero, A.E. Sex-Specific SARS-CoV-2 Mortality: Among Hormone-Modulated ACE2 Expression, Risk of Venous Thromboembolism and Hypovitaminosis D. Int. J. Mol. Sci. 2020, 21, 2948. [Google Scholar] [CrossRef]
- Li, M.Y.; Li, L.; Zhang, Y.; Wang, X.S. Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect. Dis. Poverty 2020, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Zhou, B.; Zhang, L.; Balaji, K.S.; Wei, C.; Liu, X.; Chen, H.; Peng, J.; Fu, J. Expressions and significances of the angiotensin-converting enzyme 2 gene, the receptor of SARS-CoV-2 for COVID-19. Mol. Biol. Rep. 2020, 47, 4383–4392. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Xu, X. scRNA-seq Profiling of Human Testes Reveals the Presence of the ACE2 Receptor, a Target for SARS-CoV-2 Infection in Spermatogonia, Leydig and Sertoli Cells. Cells 2020, 9, 920. [Google Scholar] [CrossRef] [PubMed]
- Qio Shen, Q.; Xiao, X.; Aierken, A.; Yue, W.; Wu, X.; Liao, M.; Hua, J. The ACE2 expression in Sertoli cells and germ cells may cause male reproductive disorder after SARS-CoV-2 infection. J. Cell Mol. Med. 2020, 24, 9472–9477. [Google Scholar] [CrossRef]
- Seymen, C.M. The other side of COVID-19 pandemic: Effects on male fertility. J. Med. Virol. 2021, 93, 1396–1402. [Google Scholar] [CrossRef]
- Reis, A.B.; Araújo, F.C.; Pereira, V.M.; Dos Reis, A.M.; Santos, R.A.; Reis, F.M. Angiotensin (1-7) and its receptor Mas are expressed in the human testis: Implications for male infertility. J. Mol. Histol. 2010, 41, 75–80. [Google Scholar] [CrossRef]
- Gianzo, M.; Muñoa-Hoyos, I.; Urizar-Arenaza, I.; Larreategui, Z.; Quintana, F.; Garrido, N.; Subirán, N.; Irazusta, J. Angiotensin II type 2 receptor is expressed in human sperm cells and is involved in sperm motility. Fertil. Steril. 2016, 105, 608–616. [Google Scholar] [CrossRef]
- Harmer, D.; Gilbert, M.; Borman, R.; Clark, K.L. Quantitative mRNA expression profiling of ACE 2, a novel homologue of angiotensin converting enzyme. FEBS Lett. 2002, 4, 532. [Google Scholar] [CrossRef]
- Fan, C.; Li, K.; Ding, Y.; Lu, W.L.; Wang, J. ACE2 expression in kidney and testis may cause kidney and testis damage after 2019-nCoV infection. MedRxiv 2020. [Google Scholar] [CrossRef]
- Xu, J.; Qi, L.; Chi, X.; Yang, J.; Wei, X.; Gong, E.; Peh, S.; Gu, J. Orchitis: A complication of severe acute respiratory syndrome (SARS). Biol. Reprod. 2006, 74, 410–416. [Google Scholar] [CrossRef]
- La Marca, A.; Busani, S.; Donno, V.; Guaraldi, G.; Ligabue, G.; Girardis, M. Testicular pain as an unusual presentation of COVID-19: A brief review of SARS-CoV-2 and the testis. Reprod. Biomed. Online 2020, 41, 903–906. [Google Scholar] [CrossRef]
- Ediz, C.; Tavukcu, H.H.; Akan, S.; Kizilkan, Y.E.; Alcin, A.; Oz, K.; Yilmaz, O. Is there any association of COVID-19 with testicular pain and epididymo-orchitis? Int. J. Clin. Pract. 2021, 75, e13753. [Google Scholar] [CrossRef]
- Achua, J.K.; Chu, K.Y.; Ibrahim, E.; Khodamoradi, K.; Delma, K.S.; Iakymenko, O.A.; Kryvenko, O.N.; Arora, H.; Ramasamy, R. Histopathology and Ultrastructural Findings of Fatal COVID-19 Infections on Testis. World J. Mens Health 2021, 39, 65–74. [Google Scholar] [CrossRef]
- Ma, X.; Guan, C.; Chen, R.; Wang, Y.; Feng, S.; Wang, R.; Qu, G.; Zhao, S.; Wang, F.; Wang, X.; et al. Pathological and molecular examinations of postmortem testis biopsies reveal SARS-CoV-2 infection in the testis and spermatogenesis damage in COVID-19 patients. Cell Mol. Immunol. 2021, 18, 487–489. [Google Scholar] [CrossRef]
- Li, H.; Xiao, X.; Zhang, J.; Zafar, M.I.; Wu, C.; Long, Y.; Lu, W.; Pan, F.; Meng, T.; Zhao, K.; et al. Impaired spermatogenesis in COVID-19 patients. EClinicalMedicine 2020, 28, 100604. [Google Scholar] [CrossRef] [PubMed]
- Mital, P.; Hinton, B.T.; Dufour, J.M. The blood-testis and blood-epididymis barriers are more than just their tight junctions. Biol. Reprod. 2011, 84, 851–858. [Google Scholar] [CrossRef] [Green Version]
- Mruk, D.D.; Cheng, C.Y. The Mammalian Blood-Testis Barrier: Its Biology and Regulation. Endocr. Rev. 2015, 36, 564–591. [Google Scholar] [CrossRef] [PubMed]
- Cui, D.; Han, G.; Shang, Y.; Liu, C.; Xia, L.; Li, L.; Yi, S. Antisperm antibodies in infertile men and their effect on semen parameters: A systematic review and meta-analysis. Clin. Chim. Acta 2015, 444, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.G.; Bosmans, E.; Reumers, J.; Donders, F.; Jonckheere, J.; Salembier, G.; Stern, N.; Jacquemyn, Y.; Ombelet, W.; Depuydt, C.E. Sperm quality and absence of SARS-CoV-2 RNA in semen after COVID-19 infection: A prospective, observational study and validation of the Sperm COVID test. Fertil. Steril. 2022, 117, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Corona, G.; Vena, W.; Pizzocaro, A.; Pallotti, F.; Paoli, D.; Rastrelli, G.; Baldi, E.; Cilloni, N.; Gacci, M.; Semeraro, F.; et al. Andrological effects of SARS-Cov-2 infection: A systematic review and meta-analysis. J. Endocrinol. Investig. 2022, 9, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Salam, A.P.; Horby, P.W. The Breadth of Viruses in Human Semen. Emerg. Infect. Dis. 2017, 23, 1922–1924. [Google Scholar]
- Gupta, P.; Leroux, C.; Patterson, B.K.; Kingsley, L.; Rinaldo, C.; Ding, M.; Chen, Y.; Kulka, K.; Buchanan, W.; McKeon, B.; et al. Human immunodeficiency virus type 1 shedding pattern in semen correlates with the compartmentalization of viral Quasi species between blood and semen. J. Infect. Dis. 2000, 182, 79–87. [Google Scholar] [CrossRef]
- Rubin, S.; Eckhaus, M.; Rennick, L.J.; Bamford, C.G.; Duprex, W.P. Molecular biology, pathogenesis and pathology of mumps virus. J. Pathol. 2015, 235, 242–252. [Google Scholar] [CrossRef]
- Guo, L.; Zhao, S.; Li, W.; Wang, Y.; Li, L.; Jiang, S.; Ren, W.; Yuan, Q.; Zhang, F.; Kong, F.; et al. Absence of SARS-CoV-2 in semen of a COVID-19 patient cohort. Andrology 2021, 9, 42–47. [Google Scholar] [CrossRef]
- Ruan, Y.; Hu, B.; Liu, Z.; Liu, K.; Jiang, H.; Li, H.; Li, R.; Luan, Y.; Liu, X.; Yu, G.; et al. No detection of SARS-CoV-2 from urine, expressed prostatic secretions, and semen in 74 recovered COVID-19 male patients: A perspective and urogenital evaluation. Andrology 2021, 9, 99–106. [Google Scholar] [CrossRef]
- Pan, F.; Xiao, X.; Guo, J.; Song, Y.; Li, H.; Patel, D.P.; Spivak, A.M.; Alukal, J.P.; Zhang, X.; Xiong, C.; et al. No evidence of severe acute respiratory syndrome-coronavirus 2 in semen of males recovering from coronavirus disease 2019. Fertil. Steril. 2020, 113, 1135–1139. [Google Scholar] [CrossRef]
- Machado, B.; Barcelos Barra, G.; Scherzer, N.; Massey, J.; Dos Santos Luz, H.; Henrique Jacomo, R.; Herinques Santa Rita, T.; Davis, R. Presence of SARS-CoV-2 RNA in Semen-Cohort Study in the United States COVID-19 Positive Patients. Infect. Dis. Rep. 2021, 13, 12. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Jin, M.; Bao, P.; Zhao, W.; Zhang, S. Clinical Characteristics and Results of Semen Tests among Men with Coronavirus Disease 2019. JAMA Netw Open 2020, 3, e208292. [Google Scholar] [CrossRef] [PubMed]
- Temiz, M.Z.; Dincer, M.M.; Hacibey, I.; Yazar, R.O.; Celik, C.; Kucuk, S.H.; Alkurt, G.; Doganay, L.; Yuruk, E.; Muslumanoglu, A.Y. Investigation of SARS-CoV-2 in semen samples and the effects of COVID-19 on male sexual health by using semen analysis and serum male hormone profile: A cross-sectional, pilot study. Andrologia 2021, 53, e13912. [Google Scholar] [CrossRef]
- Carlsen, E.; Andersson, A.M.; Petersen, J.H.; Skakkebaek, N.E. History of febrile illness and variation in semen quality. Hum. Reprod. 2003, 18, 2089–2092. [Google Scholar] [CrossRef]
- Pazir, Y.; Eroglu, T.; Kose, A.; Bulut, T.B.; Genc, C.; Kadihasanoglu, M. Impaired semen parameters in patients with confirmed SARS-CoV-2 infection: A prospective cohort study. Andrologia 2021, 53, e14157. [Google Scholar] [CrossRef]
- Gacci, M.; Coppi, M.; Baldi, E.; Sebastianelli, A.; Zaccaro, C.; Morselli, S.; Pecoraro, A.; Manera, A.; Nicoletti, R.; Liaci, A.; et al. Semen impairment and occurrence of SARS-CoV-2 virus in semen after recovery from COVID-19. Hum. Reprod. 2021, 36, 1520–1529. [Google Scholar] [CrossRef]
- Hajizadeh Maleki, B.; Tartibian, B. COVID-19 and male reproductive function: A prospective, longitudinal cohort study. Reproduction 2021, 161, 319–331. [Google Scholar] [CrossRef]
- Best, J.C.; Kuchakulla, M.; Khodamoradi, K.; Lima, T.F.N.; Frech, F.S.; Achua, J.; Rosete, O.; Mora, B.; Arora, H.; Ibrahim, E.; et al. Evaluation of SARS-CoV-2 in Human Semen and Effect on Total Sperm Number: A Prospective Observational Study. World J. Mens Health 2021, 39, 489–495. [Google Scholar] [CrossRef]
- Guo, T.H.; Sang, M.Y.; Bai, S.; Ma, H.; Wan, Y.Y.; Jiang, X.H.; Zhang, Y.W.; Xu, B.; Chen, H.; Zheng, X.Y.; et al. Semen parameters in men recovered from COVID-19. Asian J. Androl. 2021, 23, 479–483. [Google Scholar]
- Purpura, L.J.; Alukal, J.; Chong, A.M.; Liu, L.; Cantos, A.; Shah, J.; Medrano, N.; Chang, J.Y.; Tsuji, M.; Mohri, H.; et al. SARS-CoV-2 RNA Shedding in Semen and Oligozoospermia of Patient with Severe Coronavirus Disease 11 Weeks after Infection. Emerg. Infect. Dis. 2022, 28, 196–200. [Google Scholar] [CrossRef]
- Delgado-Roche, L.; Mesta, F. Oxidative Stress as Key Player in Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) Infection. Arch. Med. Res. 2020, 51, 384–387. [Google Scholar] [CrossRef]
- Sengupta, P.; Dutta, S. Does SARS-CoV-2 infection cause sperm DNA fragmentation? Possible link with oxidative stress. Eur. J. Contracept. Reprod. Health Care 2020, 25, 405–406. [Google Scholar] [CrossRef]
- Condorelli, R.A.; La Vignera, S.; Barbagallo, F.; Alamo, A.; Mongioì, L.M.; Cannarella, R.; Aversa, A.; Calogero, A.E. Bio-Functional Sperm Parameters: Does Age Matter? Front. Endocrinol. 2020, 11, 558374. [Google Scholar] [CrossRef]
- Banihani, S.A. Human semen quality as affected by SARS-CoV-2 infection: An up-to-date review. Andrologia 2022, 54, e14295. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Hulme, J.; Tran, H.D.; Vo, T.K.; Vo, G.V. The potential impact of COVID-19 on male reproductive health. J. Endocrinol. Investig. 2022, 45, 1483–1495. [Google Scholar] [CrossRef]
- Haghpanah, A.; Masjedi, F.; Alborzi, S.; Hosseinpour, A.; Dehghani, A.; Malekmakan, L.; Roozbeh, J. Potential mechanisms of SARS-CoV-2 action on male gonadal function and fertility: Current status and future prospects. Andrologia 2021, 53, e13883. [Google Scholar] [CrossRef]
- Salonia, A.; Pontillo, M.; Capogrosso, P.; Gregori, S.; Tassara, M.; Boeri, L.; Carenzi, C.; Abbate, C.; Cignoli, D.; Ferrara, A.M.; et al. Severely low testosterone in males with COVID-19: A case-control study. Andrology 2021, 9, 1043–1052. [Google Scholar] [CrossRef]
- Kadihasanoglu, M.; Aktas, S.; Yardimci, E.; Aral, H.; Kadioglu, A. SARS-CoV-2 Pneumonia Affects Male Reproductive Hormone Levels: A Prospective, Cohort Study. J. Sex. Med. 2021, 18, 256–264. [Google Scholar] [CrossRef]
- Ma, L.; Xie, W.; Li, D.; Shi, L.; Ye, G.; Mao, Y.; Xiong, Y.; Sun, H.; Zheng, F.; Chen, Z.; et al. Evaluation of sex-related hormones and semen characteristics in reproductive-aged male COVID-19 patients. J. Med. Virol. 2021, 93, 456–462. [Google Scholar] [CrossRef]
- Tan, C.; Huang, Y.; Shi, F.; Tan, K.; Ma, Q.; Chen, Y.; Jiang, X.; Li, X. C-reactive protein correlates with computed tomographic findings and predicts severe COVID-19 early. J. Med. Virol. 2020, 92, 856–862. [Google Scholar] [CrossRef] [Green Version]
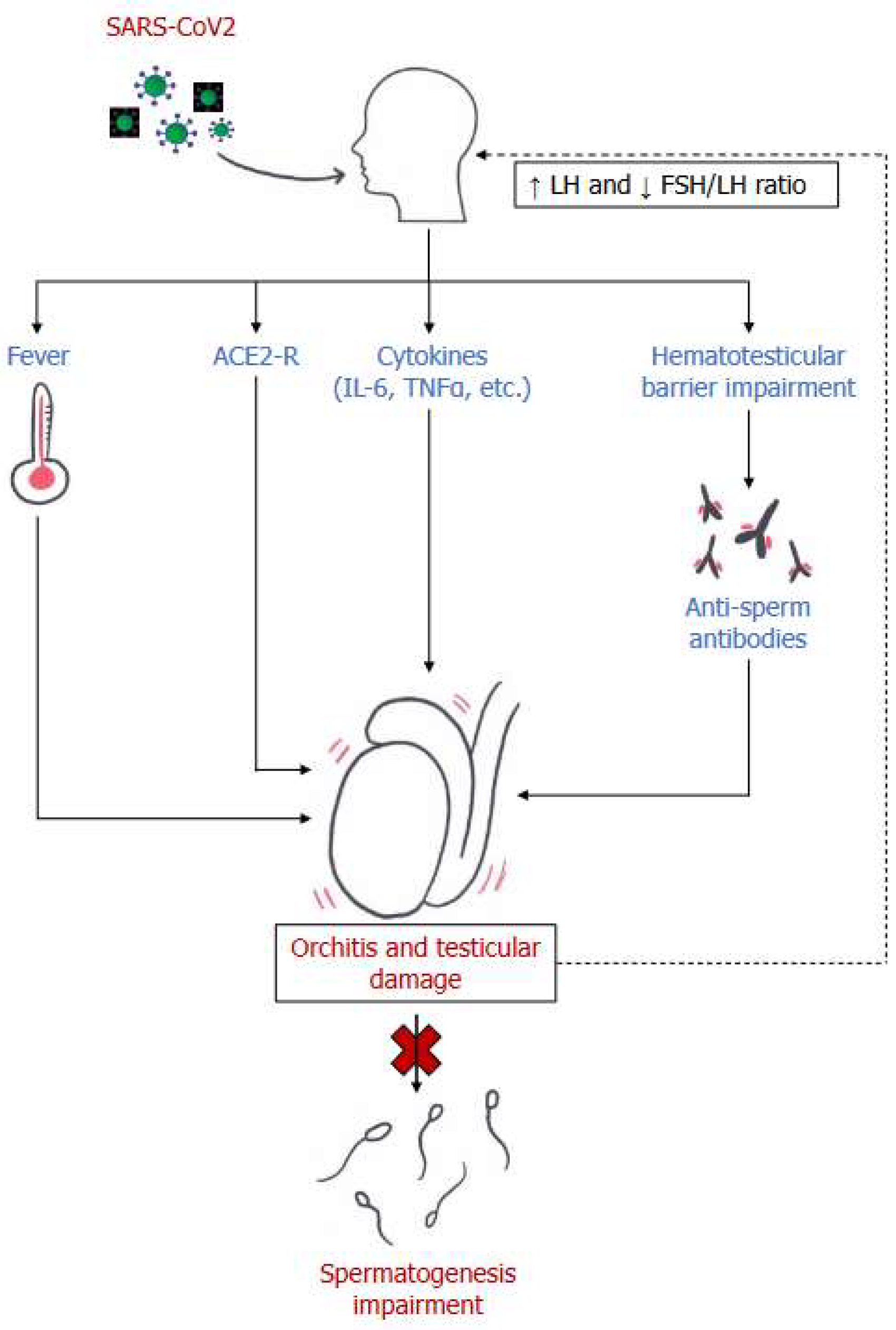
Figure 1.
Main mechanisms of male reproductive system damage in SARS-CoV2 infection. LH= luteinizing hormone; FSH: follicle stimulating hormone; ACE2-R= Angiotensin-converting enzyme receptor 2; IL-6= Interleukin 6; TNF-α= Tumor Necrosis Factor α.
Figure 1.
Main mechanisms of male reproductive system damage in SARS-CoV2 infection. LH= luteinizing hormone; FSH: follicle stimulating hormone; ACE2-R= Angiotensin-converting enzyme receptor 2; IL-6= Interleukin 6; TNF-α= Tumor Necrosis Factor α.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Leanza, C.; Mongioì, L.M.; Cannarella, R.; La Vignera, S.; Condorelli, R.A.; Calogero, A.E. The Possible Role of SARS-CoV-2 in Male Fertility: A Narrative Review. Endocrines 2022, 3, 552-559. https://doi.org/10.3390/endocrines3030046
AMA Style
Leanza C, Mongioì LM, Cannarella R, La Vignera S, Condorelli RA, Calogero AE. The Possible Role of SARS-CoV-2 in Male Fertility: A Narrative Review. Endocrines. 2022; 3(3):552-559. https://doi.org/10.3390/endocrines3030046
Chicago/Turabian StyleLeanza, Claudia, Laura M. Mongioì, Rossella Cannarella, Sandro La Vignera, Rosita A. Condorelli, and Aldo E. Calogero. 2022. "The Possible Role of SARS-CoV-2 in Male Fertility: A Narrative Review" Endocrines 3, no. 3: 552-559. https://doi.org/10.3390/endocrines3030046