Plasma Levels of Cytokines (IL-10, IFN-γ and TNF-α) in Multidrug Resistant Tuberculosis and Drug Responsive Tuberculosis Patients in Ghana

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Subjects and Sample Collection
2.2. Plasma Level Measurement of Cytokines (TNF-α, IFN-γ and IL-10)
2.3. Statistical Analysis
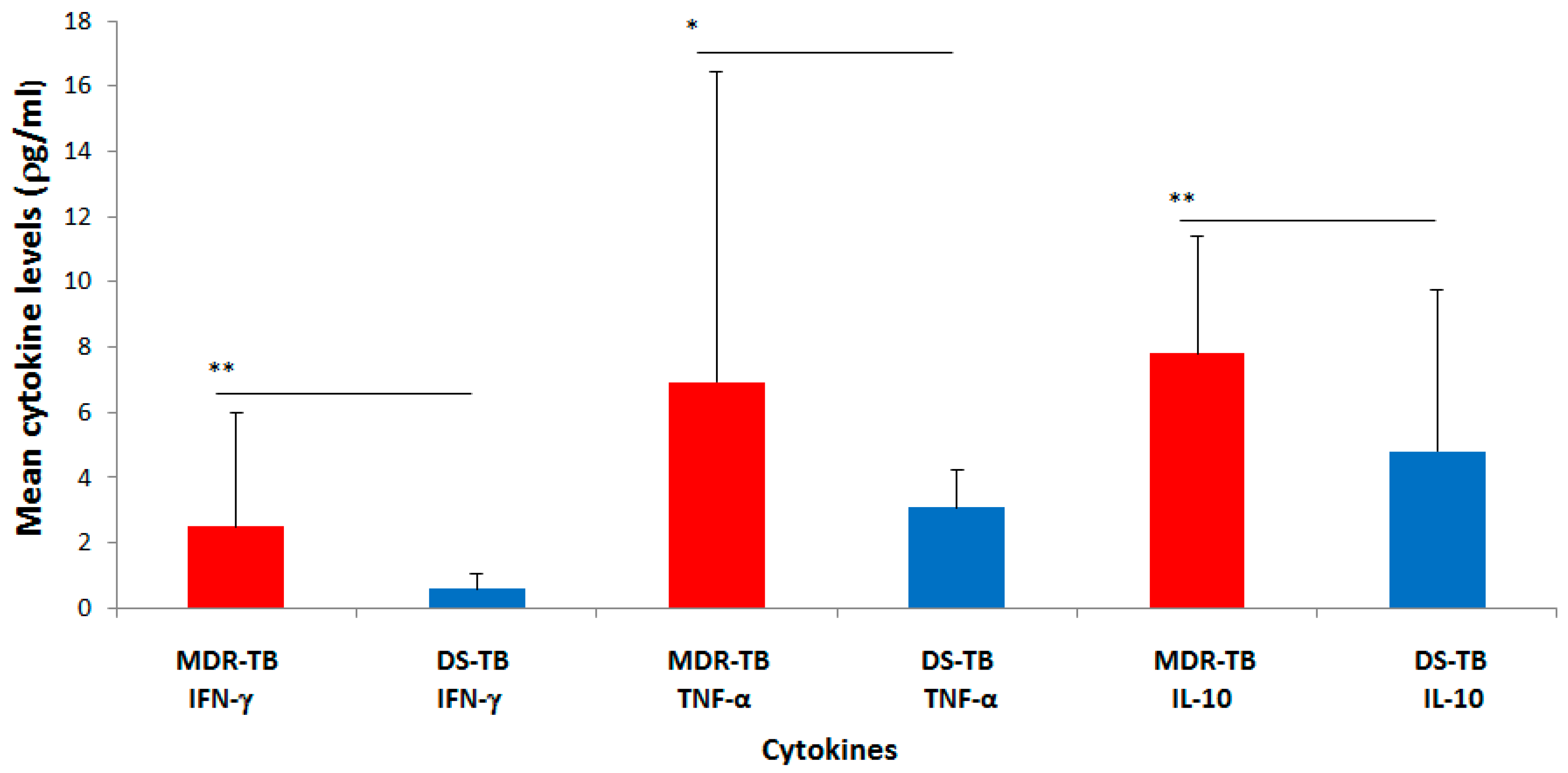
3. Results
Plasma Levels of Pro- (IFN-γ and TNF-α) and Anti-Inflammatory Cytokines (IL-10) in MDR-TB and DS-TB Cases
4. Discussion
4.1. Relationship between MDR-TB and Socio-Demographic Information
4.2. Plasma Concentration of the Cytokines (IL-10, IFN-γ and TNF-α)
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lönnroth, K.; Migliori, G.B.; Abubakar, I.; D’Ambrosio, L.; de Vries, G.; Diel, R.; Douglas, P.; Falzon, D.; Gaudreau, M.A.; Goletti, D.; et al. Towards tuberculosis elimination: An action framework for low-incidence countries. Eur. Respir. J. 2015, 45, 928–952. [Google Scholar] [CrossRef] [PubMed]
- Jassal, M.S.; Bishai, W.R. Epidemiology and challenges to the elimination of global tuberculosis. Clin. Infect. Dis. 2010, 50 (Suppl. 3), S156–S164. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Global Tuberculosis Report 2017. (WHO/HTM/TB/2017.04); WHO: Geneva, Switzerland, 2017; Available online: https://www.who.int/tb/publications/global_report/gtbr2017_main_text.pdf (accessed on 13 December 2018).
- Kurz, S.G.; Furin, J.J.; Bark, C.M. Drug-Resistant Tuberculosis: Challenges and Progress. Infect. Dis. Clin. N. Am. 2016, 30, 509–522. [Google Scholar] [CrossRef] [PubMed]
- Diel, R.; Vandeputte, J.; de Vries, G.; Stillo, J.; Wanlin, M.; Nienhaus, A. Costs of tuberculosis disease in the European Union: A systematic analysis and cost calculation. Eur. Respir. J. 2014, 43, 554–565. [Google Scholar] [CrossRef] [PubMed]
- Skrahina, A.; Hurevich, H.; Zalutskaya, A.; Sahalchyk, E.; Astrauko, A.; Hoffner, S.; Rusovich, V.; Dadu, A.; de Colombani, P.; Dara, M.; et al. Multidrug-resistant tuberculosis in Belarus: The size of the problem and associated risk factors. Bull. World Health Organ. 2013, 91, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Ulmasova, D.J.; Uzakova, G.; Tillyashayhov, M.N.; Turaev, L.; van Gemert, W.; Hoffmann, H.; Zignol, M.; Kremer, K.; Gombogaram, T.; Gadoev, J.; et al. Multidrug-resistant tuberculosis in Uzbekistan: Results of a nationwide survey, 2010 to 2011. Eur. Surveill. 2013, 17, 20609. [Google Scholar] [CrossRef]
- Berhan, A.; Berhan, Y.; Yizengaw, D. A Meta-Analysis of Drug Resistant Tuberculosis in Sub-Saharan Africa: How Strongly Associated with Previous Treatment and HIV Co-Infection? Ethiop. J. Health Sci. 2013, 23, 271–282. [Google Scholar] [CrossRef]
- Zignol, M.; van Gemert, W.; Falzon, D.; Sismanidis, C.; Glaziou, P.; Floyd, K.; Raviglione, M. Surveillance of anti-tuberculosis drug resistance in the world: An updated analysis, 2007–2010. Bull. World Health Organ. 2012, 90, 111D–119D. [Google Scholar] [CrossRef]
- Abubakar, I.; Zignol, M.; Falzon, D.; Raviglione, M.; Ditiu, L.; Masham, S.; Adetifa, I.; Ford, N.; Cox, H.; Lawn, S.D.; et al. Drug-resistant tuberculosis: Time for visionary political leadership. Lancet Infect. Dis. 2013, 13, 529–539. [Google Scholar] [CrossRef]
- Owusu-Dabo, E.; Adjei, O.; Meyer, C.G.; Horstmann, R.D.; Enimil, A.; Kruppa, T.F.; Bonsu, F.; Browne, E.N.L.; Chinbuah, M.A.; Osei, I.; et al. Mycobacterium tuberculosis drug resistance, Ghana. Emerg. Infect. Dis. 2006, 12, 1170–1172. [Google Scholar] [CrossRef]
- Domingo-Gonzalez, R.; Prince, O.; Cooper, A.; Khader, S.A. Cytokines and Chemokines in Mycobacterium tuberculosis Infection. Microbiol. Spectr. 2016, 4, 1–58. [Google Scholar]
- Adrian, T.B.R.; Montiel, J.L.; Fernandez, G.; Valecillo, A. Role of Cytokines and other Factors Involved in the Mycobacterium Tuberculosis Infection. World J. Immunol. 2015, 5, 16–50. [Google Scholar] [CrossRef]
- Olsen, A.; Chen, Y.; Ji, Q.; Zhu, G.; De Silva, A.D.; Vilcheze, C.; Weisbrod, T.; Li, W.; Xu, J.; Larsen, M.; et al. Targeting Mycobacterium tuberculosis Tumor Necrosis Factor Alpha-Downregulating Genes for the Development of Antituberculous Vaccines. MBio 2016, 7, e01023-15. [Google Scholar] [CrossRef]
- Addo, K.K.; Yeboah-manu, D.; Dan-Dzide, M.; Owusu-Darko, K.; Caulley, P.; Mensah, G.I.; Minamikawa, M.; Lienhardt, C.; Bonsu, F.A.; Ofori-Adjei, D. Diagnosis of Tuberculosis in Ghana: The role of laboratory training. Ghana Med. J. 2010, 44. [Google Scholar] [CrossRef]
- Siddiqi, S.; Ahmed, A.; Asif, S.; Behera, D.; Javaid, M.; Jani, J.; Jyoti, A.; Mahatre, R.; Mahto, D.; Richter, E.; et al. Direct drug susceptibility testing of Mycobacterium tuberculosis for rapid detection of multidrug resistance using the Bactec MGIT 960 system: A multicenter study. J. Clin. Microbiol. 2012, 50, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.Y.; Enarson, D.A.; Yu, M.C.; Bai, K.J.; Huang, R.M.; Hsu, C.J.; Suo, J.; Lin, T.P. Outcome of pulmonary multidrug-resistant tuberculosis: A 6-yrs follow-up study. Eur. Respir. J. 2006, 5, 980–985. [Google Scholar] [CrossRef]
- Ollé-Goig, J.E.; Sandy, R. Outcomes of individualised treatment for multidrug-Resistant Tuberculosis before DOTs-plus. Int. J. Tuberculosis Lung Dis. 2005, 9, 765–770. [Google Scholar]
- Kpessa, M.W. The politics of retirement income security policy in Ghana: Historical trajectories and transformative capabilities. Afri. J. Pol. Sci. Int. Relat. 2011, 5, 92–102. [Google Scholar]
- Nhamoyebonde, S.; Alasdair, L. Biological differences between the sexes and susceptibility to Tuberculosis. J. Infect. Dis. 2014, 209 (Suppl. 3), S100–S106. [Google Scholar] [CrossRef]
- Eftekhar, M.; Pourmasumi, S.; Sabeti, P.; Aflatoonian, A.; Sheikhha, M.H. Mycobacterium tuberculosis infection in women with unexplained infertility. Int. J. Reprod. Biomed. 2015, 13, 749–754. [Google Scholar] [CrossRef]
- Atre, S.R.; Kudale, A.M.; Morankar, S.N.; Rangan, S.G.; Weiss, M.G. Cultural concepts of tuberculosis and gender among the general population without tuberculosis in rural Maharashtra, India. Trop. Med. Int. Health 2004, 9, 1228–1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, S. Tuberculosis and patient gender: An analysis and its implications in tuberculosis control. Lung India 2009, 26, 46–47. [Google Scholar] [CrossRef] [PubMed]
- Horton, K.C.; MacPherson, P.; Houben, R.M.; White, R.G.; Corbett, E.L. Sex Differences in Tuberculosis Burden and Notifications in Low- and Middle-Income Countries: A Systematic Review and Meta-analysis. PLoS Med. 2016, 13, e1002119. [Google Scholar] [CrossRef] [PubMed]
- World Health Organiation. Global Tuberculosis Control: Surveillance, Planning and Financing; WHO: Geneva, Switzerland, 2004; Available online: http//www.who.int/g.tb (accessed on 8 December 2017).
- Silva, D.R.; Mu-oz-Torrico, M.; Duarte, R.; Galvão, T.; Bonini, E.H.; Arbex, F.F.; Arbex, M.A.; Augusto, V.M.; Rabahi, M.F.; Carvalho de, Q.M.F.; et al. Risk factors for tuberculosis: Diabetes, smoking, alcohol use, and the use of other drugs. J. Bras. Pneumol. 2018, 44, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Lienhardt, C.; Glaziou, P.; Uplekar, M.; Lönnroth, K.; Getahun, H.; Raviglione, M. Global tuberculosis control: Lessons learnt and future prospects. Nat. Rev. Microbiol. 2012, 10, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Bennadi, D. Self-medication: A current challenge. J. Basic Clin. Pharm. 2013, 5, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Bhatias, S.; Dranyi, T.; Ronley, D. Tuberculosis among Tibetan refugees in India. Soc. Med. 2002, 54, 423–432. [Google Scholar] [CrossRef]
- Zetola, N.M.; Modongo, C.; Kip, E.C.; Gross, R.; Bisson, G.P.; Collman, R.G. Alcohol use and abuse among patients with multidrug-resistant tuberculosis in Botswana. Int. J. Tuberc. Lung Dis. 2012, 16, 1529–1534. [Google Scholar] [CrossRef] [Green Version]
- Ferreira-Borges, C.; Parry, C.D.; Babor, T.F. Harmful Use of Alcohol: A Shadow over Sub-Saharan Africa in Need of Workable Solutions. Int. J. Environ. Res. Public Health 2017, 14, 346. [Google Scholar] [CrossRef]
- O’Connell, R.; Chishinga, N.; Kinyanda, E.; Patel, V.; Ayles, H.; Weiss, H.A.; Seedat, S. Prevalence and correlates of alcohol dependence disorder among TB and HIV infected patients in Zambia. PLoS ONE 2013, 8, e74406. [Google Scholar]
- Imtiaz, S.; Shield, K.D.; Roerecke, M.; Samokhvalov, A.V.; Lönnroth, K.; Rehm, J. Alcohol consumption as a risk factor for tuberculosis: Meta-analyses and burden of disease. Eur. Respir. J. 2017, 50, 1700216. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, K.; Bloss, E. Alcohol brewing and the African tuberculosis epidemic. Med Anthropol. 2011, 30, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Walker, N.F.; Meintjes, G.; Wilkinson, R.J. HIV-1 and the immune response to TB. Future Virol. 2013, 8, 57–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roider, J.M.; Muenchhoff, M.; Goulder, P.J. Immune activation and paediatric HIV-1 disease outcome. Curr. Opin. HIV AIDS 2016, 11, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, H.; Assefa, N.; Mengistie, B. Prevalence of extrapulmonary tuberculosis among people living with HIV/AIDS in sub-Saharan Africa: A systemic review and meta-analysis. HIV/AIDS 2018, 10, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Amelio, P.; Portevin, D.; Reither, K.; Mhimbira, F.; Mpina, M.; Tumbo, A.; Nickel, B.; Marti, H.; Knopp, S.; Ding, S.; et al. Mixed Th1 and Th2 Mycobacterium tuberculosis-specific CD4 T cell responses in patients with active pulmonary tuberculosis from Tanzania. PLoS Negl. Trop. Dis. 2017, 11, e0005817. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Kaul, A.; Tsolaki, A.G.; Kishore, U.; Bhakta, S. Mycobacterium tuberculosis: Immune evasion, latency and reactivation. Immunobiology 2012, 217, 363–374. [Google Scholar] [CrossRef]
- Ellison, M.A.; Gearheart, C.M.; Porter, C.C.; Ambruso, D.R. IFN-γ alters the expression of diverse immunity related genes in a cell culture model designed to represent maturing neutrophils. PLoS ONE 2017, 12, e0185956. [Google Scholar] [CrossRef] [PubMed]
- Amanda, M.; Elena, S.; Mauricio, A.; Rajko, R. TNF-α in Tuberculosis: A Cytokine with a Split Personality. Inflamm Allergy Drug Targets 2009, 8, 53–62. [Google Scholar]
- Redford, P.S.; Murray, P.J.; O’Garra, A. The role of IL-10 in immune regulation during M. tuberculosis infection. Mucosal. Immunol. 2011, 4, 261–270. [Google Scholar] [CrossRef]
- Flynn, J.L.; Chan, J. Immunology of tuberculosis. Annu. Rev. Immunol. 2001, 19, 93–129. [Google Scholar] [CrossRef] [PubMed]
- Mattos, A.M.; Almeida Cde, S.; Franken, K.L. Increased IgG1, IFN-gamma, TNF-alpha and IL-6 responses to Mycobacterium tuberculosis antigens in patients with tuberculosis are lower after chemotherapy. Int. Immunol. 2010, 22, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, J.; Winkler, H.-M.; Zwick, R.H.; Müller, C.; Rumetshofer, R.; Boeck, L.; Burghuber, O.C.; Winkler, S. Specific cytokine patterns of pulmonary tuberculosis in Central Africa. Clin. Immunol. 2012, 138, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Xiao, H.; Fan, Y.; Wu, F.; Zhang, Z.; Li, H.; Yang, Y. Changes of pro-inflammatory cytokines and their receptors in serum from patients with pulmonary tuberculosis. Zhonghua Jie He He Hu Xi Za Zhi 2002, 25, 325–329. [Google Scholar] [PubMed]
- Kart, L.; Buyukoglan, H.; Tekin, I.O.; Altin, R.; Senturk, Z.; Gulmez, I.; Demir, R.; Ozesmi, M. Correlation of serum tumornecrosisfactor-alpha, interleukin-4 and soluble interleukin-2 receptor levels with radiologic and clinical manifestationsin active pulmonary tuberculosis. Mediators Inflamm. 2003, 12, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Joshi, L.; Ponnana, M.; Sivangala, R.; Chelluri, L.K.; Nallari, P.; Penmetsa, S.; Valluri, V.; Gaddam, S. Evaluation of TNF-α, IL-10 and IL-6 Cytokine Production and Their Correlation with Genotype Variants amongst Tuberculosis Patients and Their Household Contacts. PLoS ONE 2015, 10, e0137727. [Google Scholar] [CrossRef]
- Ameglio, F.; Casarini, M.; Capoluongo, E.; Mattia, P.; Puglisi, G.; Giosue, S. Post-treatment changes of six cytokines in active pulmonary tuberculosis: Differences between patients with stable or increased fibrosis. Int. J. Tuberc. Lung Dis. 2005, 9, 98–104. [Google Scholar]
- Gallegos, A.M.; van Heijst, J.W.; Samstein, M.; Su, X.; Pamer, E.G.; Glickman, M.S. A gamma interferon independent mechanism of CD4 T cell mediated control of M. tuberculosis infection in vivo. PLoS Pathog. 2011, 7, e1002052. [Google Scholar] [CrossRef]
- Tötemeyer, S.; Sheppard, M.; Lloyd, A.; Roper, D.; Dowson, C.; Underhill, D.; Murray, P.; Maskell, D.; Bryant, C. IFN-γ enhances production of nitric oxide from macrophages via a mechanism that depends on Nucleotide Oligomerization Domain-2. J. Immunol. 2006, 176, 4804–4810. [Google Scholar] [CrossRef]
- Hoeksema, M.A.; Scicluna, B.P.; Boshuizen, M.C.; vander Velden, S.; Neele, A.E.; Vanden Bossche, J.; Matlung, H.L.; van den Berg, T.K.; Goossens, P.; de Winther, M.P. IFN-γ priming of macrophages represses a part of the inflammatory program and attenuates neutrophil recruitment. J. Immunol. 2015, 194, 3909–3916. [Google Scholar] [CrossRef]
- Sasindran, S.J.; Torrelles, J.B. Mycobacterium Tuberculosis Infection and Inflammation: What is Beneficial for the host and for the bacterium? Front. Microbiol. 2011, 2, 2. [Google Scholar] [CrossRef] [PubMed]
- Figen, D.; Handan, A.H.; Teyfik, T.; HamdiMuz, M. Changes in serum cytokine levels in activetuberculosis with treatment. Med. Inflamm. 2005, 5, 256–262. [Google Scholar]


{kind=link}
| Characteristics | MDR-TB Cases, n (%) | DS-TB Cases, n (%) | p-Value | Chi-Square (X2) |
|---|---|---|---|---|
| Gender | ||||
| Male | 34 (69.4) | 23 (67.7) | 0.866 | 0.028 |
| Female | 15 (30.6) | 11 (32.3) | ||
| Age (years) | ||||
| 18–23 | 8 (16.3) | 10 (29.4) | 0.111 | 2.571 |
| 24–29 | 5 (10.2) | 5 (14.7) | ||
| 30–35 | 9 (18.4) | 6 (17.7) | ||
| 36–41 | 13 (26.5) | 9 (26.5) | ||
| 42–47 | 12 (24.5) | 3 (8.8) | ||
| 48–53 | 2 (4.1) | 1 (2.9) | ||
| Marital status | ||||
| Married | 26 (53.1) | 22 (64.7) | 0.570 | 1.126 |
| Separated | 13 (26.5) | 7 (20.6) | ||
| Divorced | 10 (20.4) | 5 (14.7) | ||
| Residency | ||||
| City | 15 (30.6) | 0 (0.0) | 0.005 | 12.946 |
| Urban | 15 (30.6) | 14 (41.2) | ||
| Suburban | 17 (34.7) | 17 (50.0) | ||
| Rural | 2 (4.1) | 3 (8.8) | ||
| Education Level | ||||
| Tertiary | 1 (2.0) | 6 (17.6) | 0.042 | 9.895 |
| High school | 11 (22.5) | 10 (29.5) | ||
| J.S.S. | 3 (6.1) | 4 (11.7) | ||
| Middle school | 4 (8.2) | 1 (2.9) | ||
| Elementary school | 30 (61.2) | 13 (38.3) | ||
| Employment Status | ||||
| Employed | 5 (10.2) | 11 (32.4) | 0.001 | 19.404 |
| Self-employed | 10 (20.4) | 15 (44.1) | ||
| Farmer | 6 (12.2) | 0 (0.0) | ||
| Student | 4 (8.2) | 5 (14.7) | ||
| Unemployed | 23 (46.9) | 3 (8.8) | ||
| Alcohol Intake | ||||
| Alcohol drinkers | 22 (44.9) | 8 (23.5) | 0.046 | 3.971 |
| Non-Alcohol drinkers | 27 (55.1) | 26 (76.5) | ||
| Smoking Status | ||||
| Smokers | 9 (18.4) | 2 (5.9) | 0.099 | 2.721 |
| Non-smokers | 40 (81.6) | 32 (94.1) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basingnaa, A.; Antwi-Baffour, S.; Nkansah, D.O.; Afutu, E.; Owusu, E. Plasma Levels of Cytokines (IL-10, IFN-γ and TNF-α) in Multidrug Resistant Tuberculosis and Drug Responsive Tuberculosis Patients in Ghana. Diseases 2019, 7, 2. https://doi.org/10.3390/diseases7010002
Basingnaa A, Antwi-Baffour S, Nkansah DO, Afutu E, Owusu E. Plasma Levels of Cytokines (IL-10, IFN-γ and TNF-α) in Multidrug Resistant Tuberculosis and Drug Responsive Tuberculosis Patients in Ghana. Diseases. 2019; 7(1):2. https://doi.org/10.3390/diseases7010002
Chicago/Turabian StyleBasingnaa, Anthony, Samuel Antwi-Baffour, Dinah Obenewaa Nkansah, Emmanuel Afutu, and Enid Owusu. 2019. "Plasma Levels of Cytokines (IL-10, IFN-γ and TNF-α) in Multidrug Resistant Tuberculosis and Drug Responsive Tuberculosis Patients in Ghana" Diseases 7, no. 1: 2. https://doi.org/10.3390/diseases7010002