
Periodontal Disease Monitoring by Raman Spectroscopy of Phosphates: New Insights into Pyrophosphate Activity

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
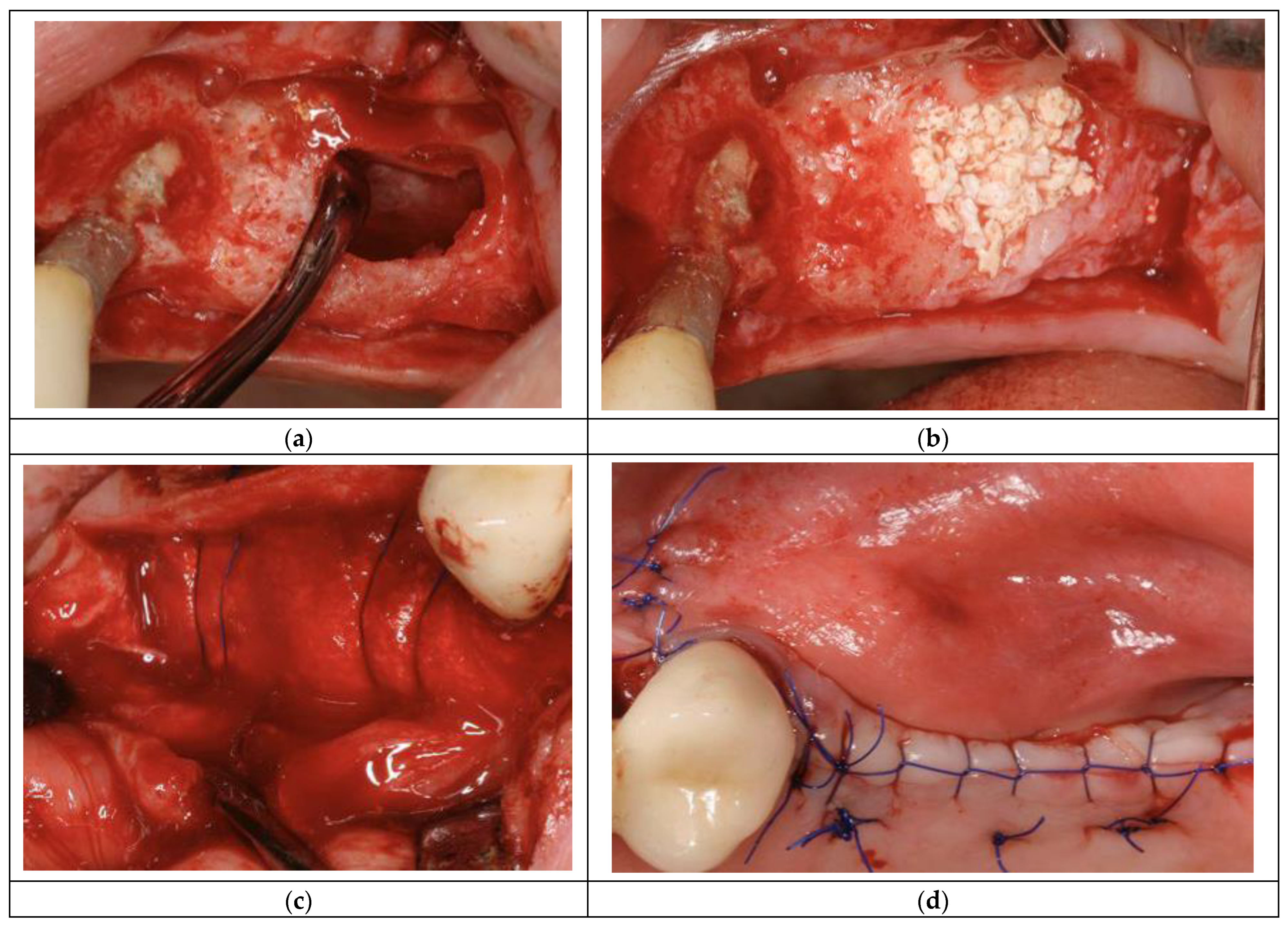
2.1. In Vivo Measurements
2.2. Characterization Methods
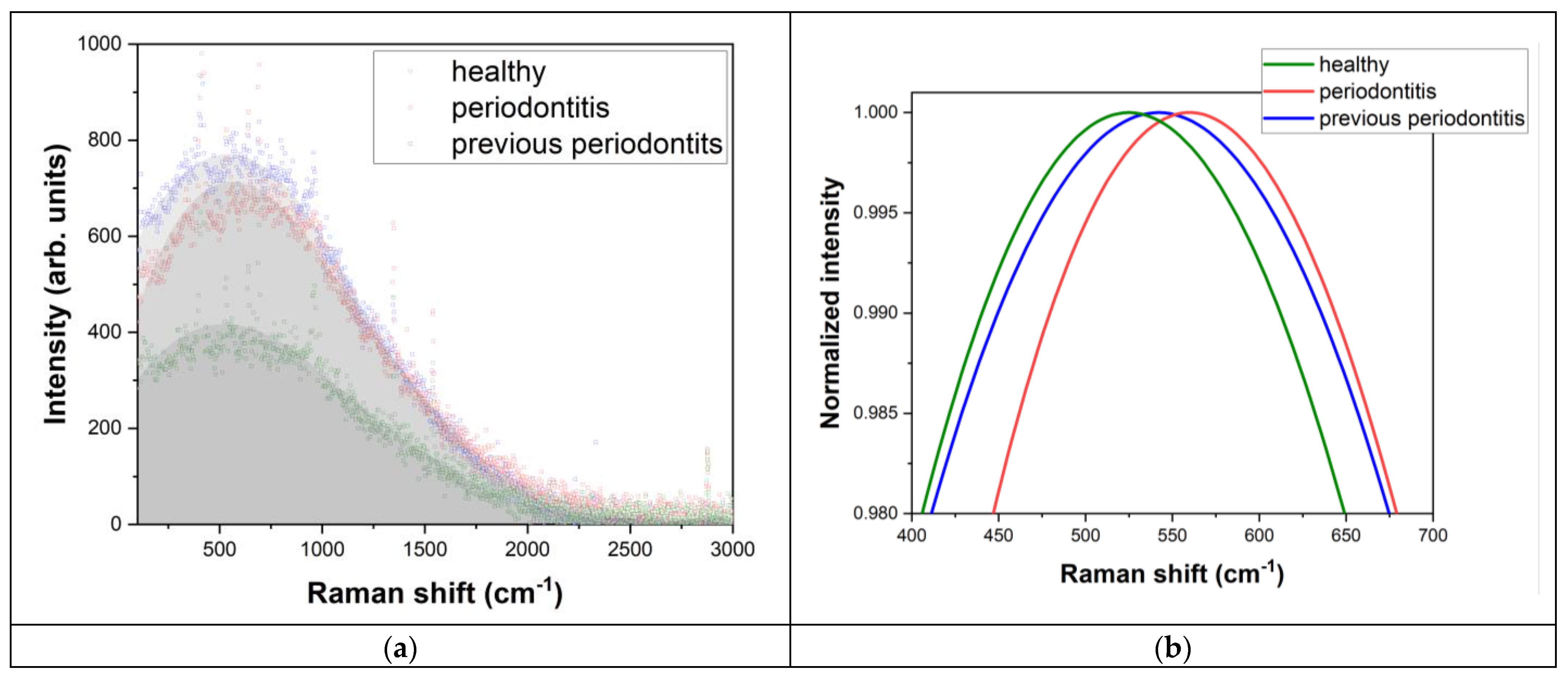
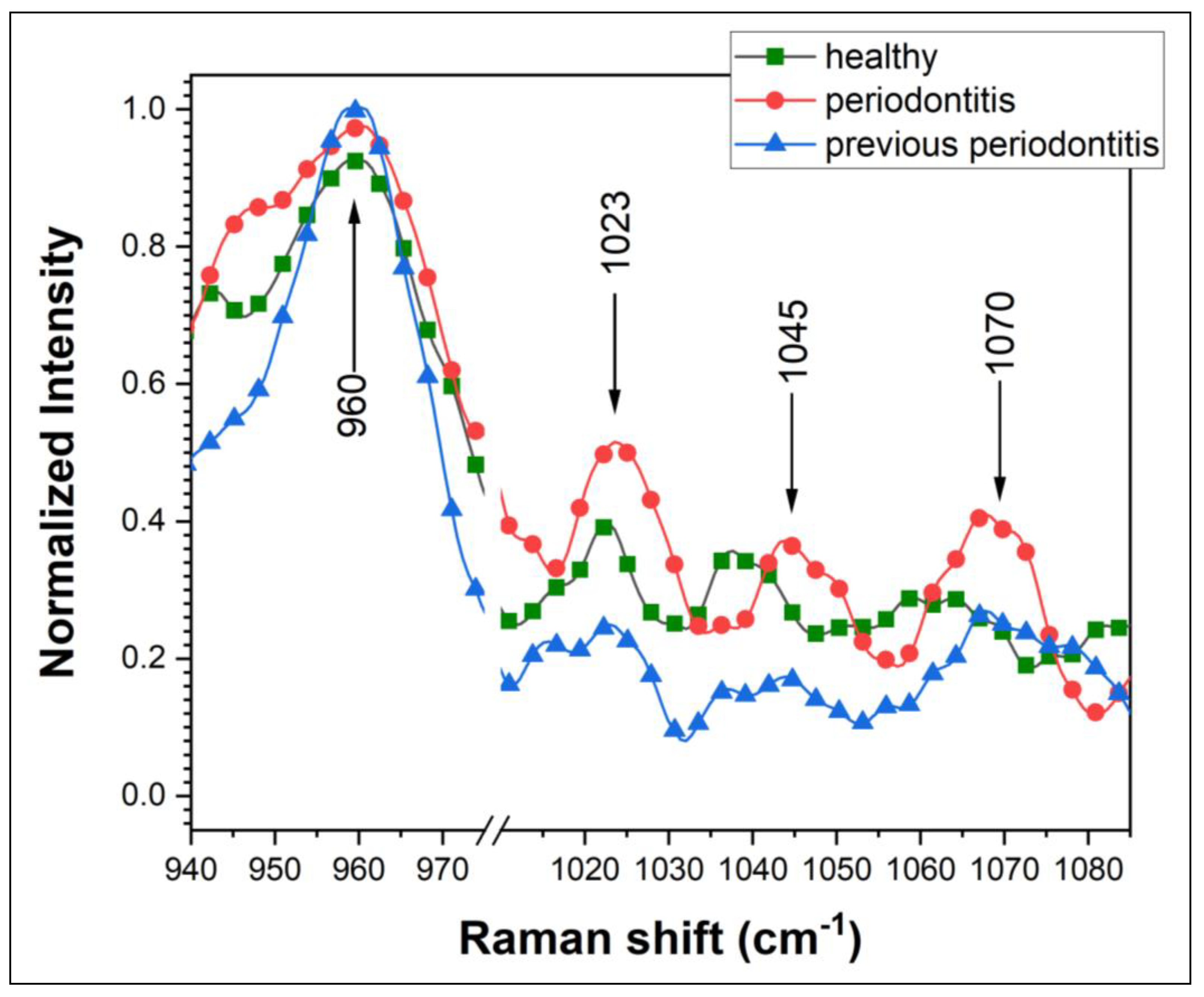
3. Results and Discussion
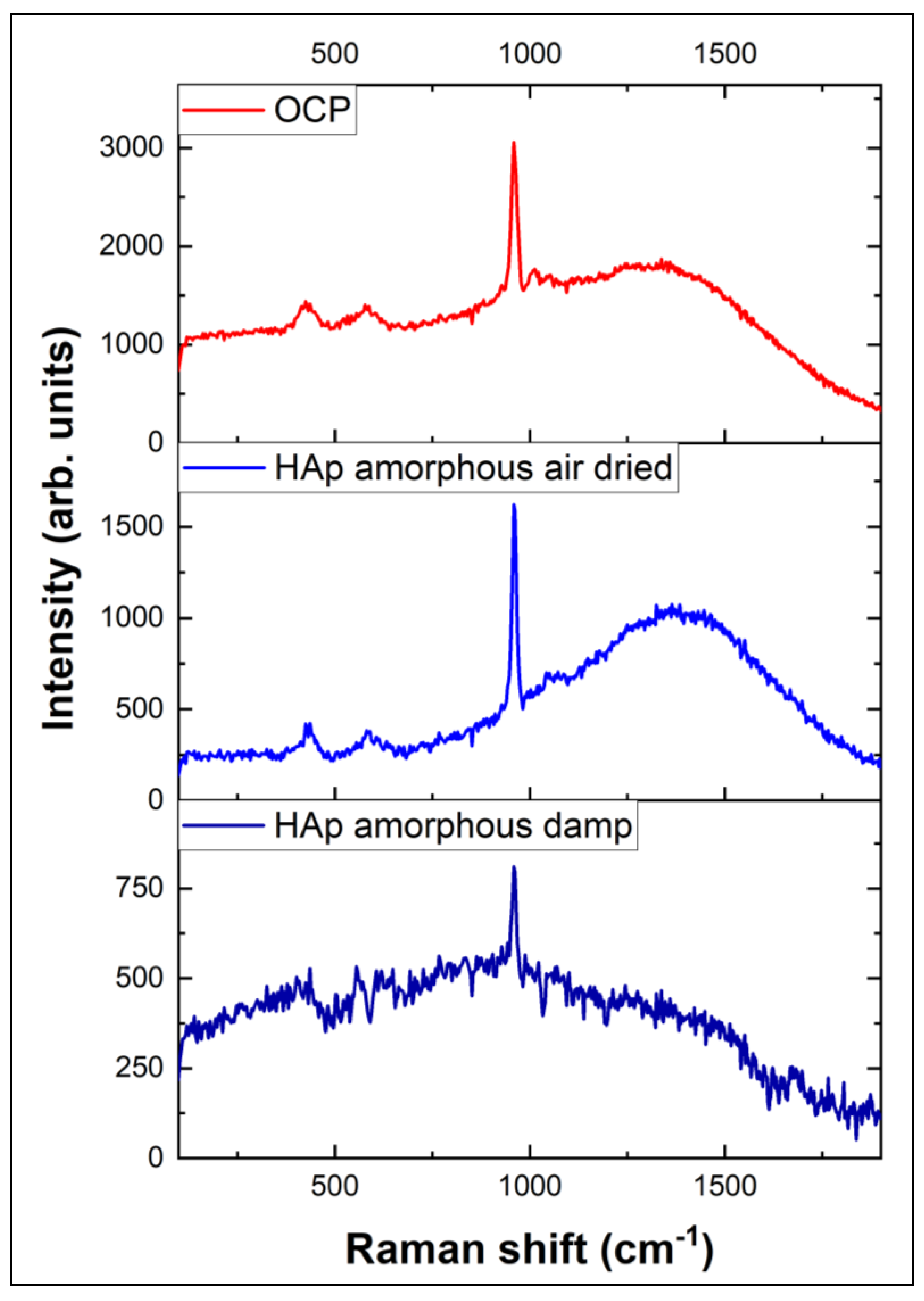
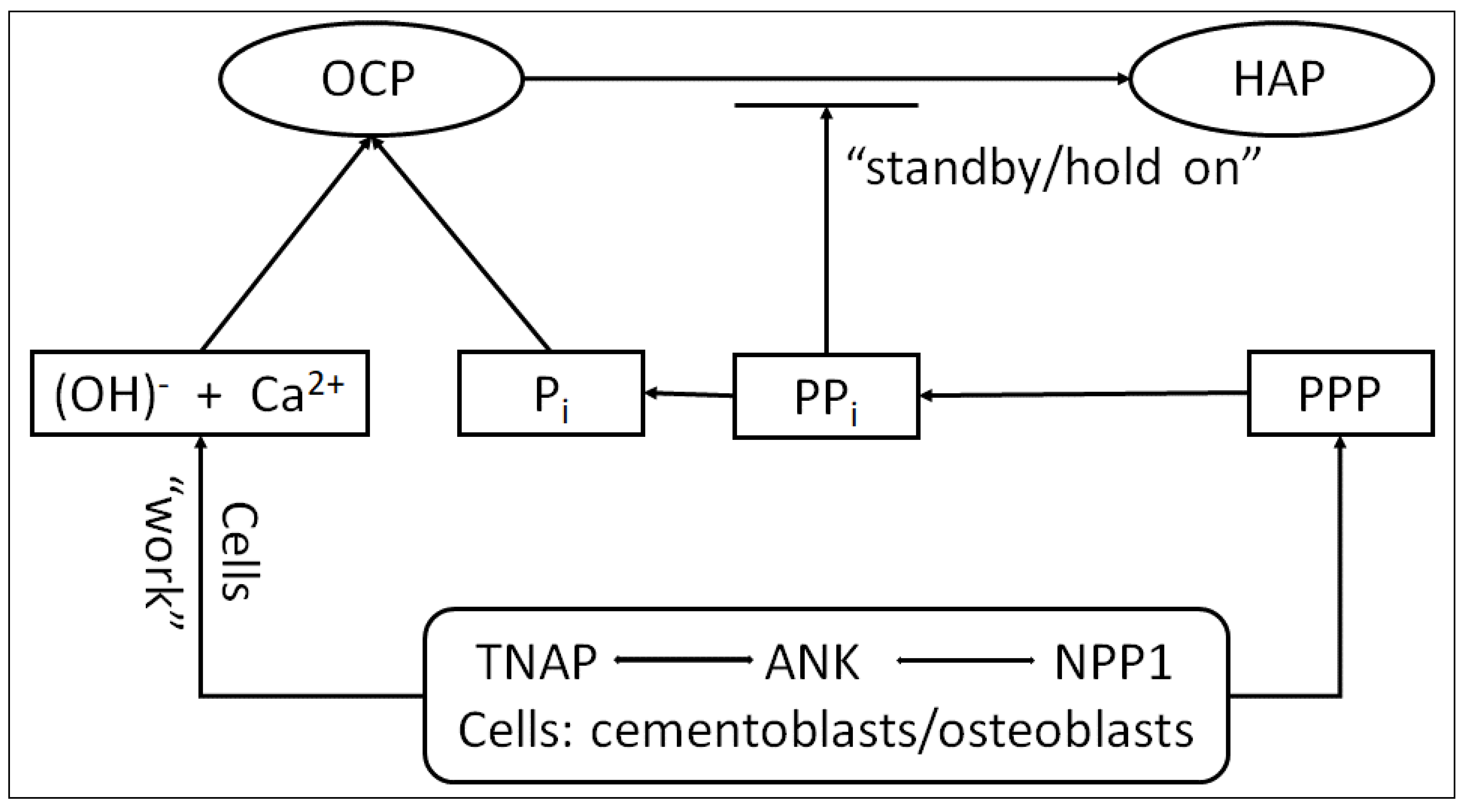
Proposed Phase Transition Mechanism Starting with OCP Considered Precursor for HAP
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fuji, S.; Sato, S.; Fukuda, K.; Okinaga, T.; Ariyoshi, W.; Usui, M.; Nakashima, K.; Nishihara, T.; Takenaka, S. Diagnosis of periodontal disease from saliva samples using Fourier Transform Infrared Microscopy coupled with partial least squares discriminant analysis. Anal. Sci. 2016, 32, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Chapple, I.L.C.; Giannobile, W.V. Wound models for periodontal and bone regeneration: The role of biologic research. Periodontol. 2000 2015, 68, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Gatin, E.; Nagy, P.; Paun, I.; Dubok, O.; Bucur, V.; Windisch, P. Raman spectroscopy: Application in periodontal and oral regenerative surgery for bone evaluation. IRBM 2019, 40, 279–285. [Google Scholar] [CrossRef]
- Stevens, O.; Petterson, I.E.I.; Day, J.C.C.; Stone, N. Developing fiber optic Raman probes for applications in clinical spectroscopy. Chem. Soc. Rev. 2016, 45, 1919–1934. [Google Scholar] [CrossRef] [PubMed]
- Gatin, E.; Nagy, P.; Iordache, S.M.; Iordache, A.M.; Luculescu, C. Raman Spectroscopy: In vivo Application for Bone Evaluation in Oral Reconstructive (Regenerative) Surgery. Diagnostics 2022, 12, 723. [Google Scholar] [CrossRef] [PubMed]
- Birtoiu, I.A.; Rizea, C.; Togoe, D.; Munteanu, R.M.; Micsa, C.; Rusu, M.I.; Tautan, M.; Braic, L.; Scoicaru, L.O.; Parau, A.; et al. Diagnosing clean margins through Raman spectroscopy in human and animal mammary tumour surgery: A short review. Interface Focus 2016, 6, 20160067. [Google Scholar] [CrossRef] [PubMed]
- Timchenko, P.E.; Timchenko, E.V.; Volova, L.T.; Dolgushkin, D.A.; Boltovskaya, V.V.; Frolov, O.O. Raman spectroscopy method for the evaluation of bone bioimplants made using the “Lyoplast” technology from cadaveric and in vivo resected bone tissue. J. Phys. Conf. Ser. 2018, 1038, 012090. [Google Scholar] [CrossRef]
- Morris, M.D.; Mandair, G.S. Raman assessment of bone quality. Clin. Orthop. Relat. Res. 2011, 469, 2160–2169. [Google Scholar] [CrossRef]
- Unal, M.; Ahmed, R.; Mahadevan-Jansen, A.; Nyman, J.S. Compositional assessment of bone by Raman spectroscopy. Analyst 2021, 146, 7464–7490. [Google Scholar] [CrossRef]
- Gatin, E.; Pal, N.; Iordache, S.M.; Iordache, A.M.; Luculescu, C.R.; Grygorovskyy, V. Preliminary Assessment of In Vivo Raman Spectroscopy Technique for Bone Quality Evaluation of Augmented Maxillary Sinus Floor. Int. J. Environ. Res. Public Health 2023, 20, 4789. [Google Scholar] [CrossRef]
- Sfeatcu, R.; Luculescu, C.; Ciobanu, L.; Balan, A.; Gatin, E.; Patrascu, I. Dental enamel quality and black tooth stain: A new approach and explanation by using Raman and AFM techniques. Part. Sci. Technol. 2015, 33, 429–435. [Google Scholar] [CrossRef]
- Müller, W.E.; Neufurth, M.; Ushijima, H.; Muñoz-Espí, R.; Müller, L.-K.; Wang, S.; Schröder, H.C.; Wang, X. Molecular and biochemical approach for understanding the transition of amorphous to crystalline calcium phosphate deposits in human teeth. Dent. Mater. 2022, 38, 2014–2029. [Google Scholar] [CrossRef] [PubMed]
- Petrakova, N.V.; Teterina, A.Y.; Mikheeva, P.V.; Akhmedova, S.A.; Kuvshinova, E.A.; Sviridova, I.K.; Sergeeva, N.S.; Smirnov, I.V.; Fedotov, A.Y.; Kargin, Y.F.; et al. In Vitro Study of Octacalcium Phosphate Behavior in Different Model Solutions. ACS Omega 2021, 6, 7487–7498. [Google Scholar] [CrossRef] [PubMed]
- Pompe, W.; Worch, H.; Habraken, W.J.; Simon, P.; Kniep, R.; Ehrlichd, H.; Pauflere, P. Octacalcium phosphate—A metastable mineral phase controls the evolution of scaffold forming proteins. J. Mater. Chem. B 2015, 3, 5318. [Google Scholar] [CrossRef] [PubMed]
- Gatin, E.; Iordache, S.M.; Luculescu, C.R.; Iordache, A.M.; Grigorescu, C.E.A.; Ilici, C.R. Raman spectroscopy as spectral tool for assessing the degree of conversion after curing of two resin-based materials used in restorative dentistry. Diagnostics 2022, 12, 1993. [Google Scholar] [CrossRef] [PubMed]
- Gatin, E.; Ciucu, C.; Ciobanu, G.; Berlic, C. Investigation and comparative survey of some dental restorative materials. Optoelectron. Adv. Mater. Rapid. Commun. 2008, 2, 284–290. [Google Scholar]
- Gatin, E.; Luculescu, C.; Iordache, S.M.; Patrascu, I. Morphological investigation by AFM of dental ceramics under thermal processing. J. Optoelectron. Adv. Mater. 2013, 15, 1136–1141. [Google Scholar]
- Deng, H.; Callender, R.; Schramm, V.L.; Grubmeyer, C. Pyrophosphate activation in hypoxanthine-guanine phosphoribosyltransferase with transition state analogue. Biochemistry 2010, 49, 2705–2714. [Google Scholar] [CrossRef]
- Mandair, G.S.; Morris, M.D. Contributions of Raman spectroscopy to the understanding of bone strength. Bonekey Rep. 2015, 4, 620. [Google Scholar] [CrossRef]
- Nathanael, A.J.; Hong, S.I.; Mangalaraj, D.; Chen, P.C. Large scale synthesis of hydroxyapatite nanospheres by high gravity method. Chem. Eng. J. 2011, 173, 846–854. [Google Scholar] [CrossRef]
- Daizy, P.; Bini, L.G.; Aruldhas, G. IR and polarized Raman spectra of Na4P2O7 10H20. J. Raman Spectrosc. 1990, 21, 523–524. [Google Scholar]
- Manoun, B.; El Bali, B.; Saxena, S.K.; Gulve, R.P. High-pressure studies of SrNi3(P2O7)2 pyrophosphate by Raman spectroscopy and X-ray diffraction. J. Mol. Struct. 2006, 794, 334–340. [Google Scholar] [CrossRef]
- Crane, N.J.; Popescu, V.; Morris, M.D.; Steenhuis, P.; Ignelzi, M.A., Jr. Raman spectroscopic evidence for octacalcium phosphate and other transient mineral species deposited during intramembranous mineralization. Bone 2006, 39, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Sadowska, J.M.; Wei, F.; Guo, J.; Guillem-Marti, J.; Lin, Z.; Ginebra, M.P.; Xiao, Y. The effect of biomimetic calcium deficient hydroxyapatite and sintered b-tricalcium phosphate on osteoimmune reaction and osteogenesis. Acta Biomater. 2019, 96, 605–618. [Google Scholar] [CrossRef]
- Tsai, T.W.; Chen, W.Y.; Tseng, Y.H.; Chan, J.C. Phase transformation of calcium phosphates in the presence of glutamic acid. Can. J. Chem. 2011, 89, 885–891. [Google Scholar] [CrossRef]
- PubChem Draw Structure. Available online: https://pubchem.ncbi.nlm.nih.gov//edit3/index.html (accessed on 24 September 2023).
- Foster, B.L.; Nagatomo, K.J.; Nociti, F.H.; Fong, H.; Dunn, D.; Tran, A.B.; Wang, W.; Narisawa, S.; Millán, J.L.; Somerman, M.J. Central Role of Pyrophosphate in Acellular Cementum Formation. PLoS ONE 2012, 7, e38393. [Google Scholar] [CrossRef] [PubMed]
- Huesa, C.; Houston, D.; Kiffer-Moreira, T.; Yadav, M.C.; Millan, J.L.; Farquharson, C. The functional co-operativity of tissue-nonspecific alkaline phosphatase (TNAP) and PHOSPHO1 during initiation of skeletal mineralization. Biochem. Biophys. 2015, 4, 196–201. [Google Scholar] [CrossRef]
- Saravanan Sekaran, S.; Vimalraj, S.; Thangavelu, L. The Physiological and Pathological Role of Tissue Nonspecific Alkaline Phosphatase beyond Mineralization. Biomolecules 2021, 11, 1564. [Google Scholar] [CrossRef]
- Zhao, M.; Li, S.; Ahn, D.U.; Huang, X. Phosvitin phosphopeptides produced by pressurized hea-trypsin hydrolysis promote the differentiation and mineralization of MC3T3-E1 cells via the OPG/RANKL signaling pathways. Poult. Sci. 2021, 100, 527–536. [Google Scholar] [CrossRef]
- Zhao, J.; Liu, Y.; Sun, W.B.; Zhang, H. Amorphous calcium phosphate and its application in dentistry. Chem. Cent. J. 2011, 5, 40. [Google Scholar] [CrossRef]
- Chen, H.; Fan, W.; He, H.; Huang, F. PGC-1: A key regulator in bone homeostasis. J. Bone Miner. Metab. 2022, 40, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gamsjaeger, S.; Masic, A.; Roschger, P.; Kazanci, M.; Dunlop, J.; Klaushofer, K.; Paschalis, E.; Fratzl, P. Cortical bone composition and orientation as a function of animal and tissue age in mice by Raman spectroscopy. Bone 2010, 47, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Liedtke, D.; Hofmann, C.; Jakob, F.; Klopocki, E.; Graser, S. Tissue-Nonspecific Alkaline Phosphatase-A Gatekeeper of Physiological Conditions in Health and a Modulator of Biological Environments in Disease. Biomolecules 2020, 10, 1648. [Google Scholar] [CrossRef]
- Choi, Y.Y.; Lee, K.H. Periodontitis as a Risk Factor for Rheumatoid Arthritis: A Matched-Cohort Study. Int. Dent. J. 2021, 71, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Iwane, T.; Kikuta, J. Notch Signaling Response to Heavy Compression Force Induces Orthodontic Root Resorption via RANKL and IL-6 from Cementoblasts. Int. J. Oral-Med. Sci. 2020, 18, 287–295. [Google Scholar] [CrossRef]
- Mitsuhashi, M.; Yamaguchi, M.; Kojima, T.; Nakajima, R.; Kasai, K. Effects of HSP70 on the compression force-induced TNF-α and RANKL expression in human periodontal ligament cells. Inflamm. Res. 2011, 60, 187–194. [Google Scholar] [CrossRef]
- Kunii, R.; Yamaguchi, M.; Tanimoto, Y.; Asano, M.; Yamada, K.; Goseki, T.; Kasai, K. Role of interleukin-6 in orthodontically induced inflammatory root resorption in humans. Korean J. Orthod. 2013, 43, 294–301. [Google Scholar] [CrossRef]
- Yao-Umezawa, E.; Yamaguchi, M.; Shimizu, M.; Kikuta, J.; Suzuki, K.; Kasai, K. Relationship between root resorption and individual variation in the calcium/phosphorous ratio of cementum. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 465–470. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Y.; Shao, P.; Wang, L.; Bao, X.; Hu, M. IL1beta inhibits differentiation of cementoblasts via microRNA-325-3p. J. Cell. Biochem. 2020, 121, 2606–2617. [Google Scholar] [CrossRef]
- Ahn, M.Y.; Yoon, H.E.; Park, J.H.; Lee, J.; Min, S.K.; Ahn, S.G.; Yoon, J.H. Characterization of NODs and TLRs in innate immune response of human cementoblast cells. Oral Dis. 2013, 19, 374–380. [Google Scholar] [CrossRef]
- Yong, J.; Groeger, S.; Ruiz-Heiland, G.; Ruf, S. Selection and validation of reference gene for RT-qPCR studies in co-culture system of mouse cementoblasts and periodontal ligament cells. BMC Res. Notes 2022, 15, 57. [Google Scholar] [CrossRef] [PubMed]
- Aimetti, M.; Mariani, G.M.; Ferrarotti, F.; Ercoli, E.; Liu, C.C.; Romano, F. Adjunctive efficacy of diode laser in the treatment of peri-implant mucositis with mechanical therapy: A randomized clinical trial. Clin. Oral Implant. Res. 2019, 30, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.H.; Suárez López Del Amo, F.; Wang, H.L. Laser therapy for treatment of peri-implant mucositis and peri-implantitis: An American Academy of Periodontology best evidence review. J. Periodontol. 2018, 89, 766–782. [Google Scholar] [PubMed]
- Rosenberg, N.; Gendelman, R.; Noofi, N. Photobiomodulation of human osteoblast-like cells in vitro by low-intensity-pulsed LED light. FEBS Open Bio 2020, 10, 1276–1287. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, P.A.; Carroll, J.D. How to report low-level laser application (LLLT)/photomedicine dose and beam parameters in clinical and laboratory studies. Photomed. Laser Surg. 2011, 29, 785–787. [Google Scholar] [CrossRef]
- Pawelczyk-Madalinska, M.; Benedicenti, S.; Salagean, T.; Bordea, I.R.; Hanna, R. Impact of adjunctive diode laser application to non-suurgicel periodontal therapy on clinica, microbiological and immunological outcomes in management of chronic periodontitis: A systematic review of human randomized controlled trials. J. Inflamm. Res. 2021, 14, 2515–2545. [Google Scholar] [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S. EFP Workshop Participants and Methodological Consultants. Treatment of stage I-III periodontitis: The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Age (Years) and Gender | Clinical Status | Bone Phenotype/Bone Type |
|---|---|---|---|
| #1 | 58M | Previously periodontal | Thick/more cortical |
| #2 | 70M | Healthy | Thick/more cortical |
| #3 | 64M | Previously periodontal | Thin/more cortical |
| #4 | 50F | Previously periodontal | Thick/more cortical |
| #5 | 70M | Previously periodontal | Thin/more cortical |
| #6 | 35M | Healthy | Thin/more cortical |
| #7 | 62F | Currently periodontal | Thin/more cancellous |
| #8 | 37F | Previously periodontal | Thin/cortical–cancellous |
| #9 | 45F | Healthy on the lower jaw, but previously periodontal on the upper jaw | Thin/more cortical |
| #10 | 43M | Currently periodontal | Thick/more cortical |
| Patient | PL Maximum (cm−1) | Intensity (arb.u.) | Intensity PO4 (@959.6 cm−1) (arb.u.) | ICol/IPO4 |
|---|---|---|---|---|
| #1 | 726.65 | 1550.18 | 1439.33 | 1.07 |
| #2 | 673.55 | 748.43 | 672.66 | 1.11 |
| #3 | 641.91 | 330.80 | 334.75 | 0.98 |
| #4 | 692.39 | 847.90 | 783 | 1.08 |
| #5 | 686.13 | 376.71 | 358.41 | 1.05 |
| #6 | 574.47 | 765.16 | 742.25 | 1.03 |
| #7 | 635.55 | 812.51 | 641.16 | 1.26 |
| #8 | 567.98 | 402.07 | 483.75 | 0.93 |
| #9 | 574.47 | 510.37 | 523.75 | 0.97 |
| #10 | 515.57 | 371.83 | 413.91 | 0.89 |
| Patient | PL Maximum (cm−1) | Intensity (arb.u.) | Intensity Pyro (@1023/1027 cm−1) (arb.u.) | ICol/IPyro |
|---|---|---|---|---|
| #1 | 726.65 | 1550.13 | 1433 | 1.08 |
| #2 | 673.55 | 748.43 | 724 | 1.03 |
| #3 | 641.91 | 330.80 | 293 | 1.12 |
| #4 | 692.39 | 847.90 | 709 | 1.19 |
| #5 | 686.13 | 376.71 | 340 | 1.10 |
| #6 | 574.47 | 765.16 | 752 | 1.01 |
| #7 | 635.55 | 812.51 | 962 | 0.84 |
| #8 | 567.98 | 402.07 | 402 | 1.00 |
| #9 | 574.47 | 510.37 | 502 | 1.01 |
| #10 | 515.57 | 371.83 | 386 | 0.96 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gatin, E.; Iordache, S.M.; Gatin, D.I.; Nagy, P.; Iordache, A.-M.; Luculescu, C. Periodontal Disease Monitoring by Raman Spectroscopy of Phosphates: New Insights into Pyrophosphate Activity. Diagnostics 2024, 14, 66. https://doi.org/10.3390/diagnostics14010066
Gatin E, Iordache SM, Gatin DI, Nagy P, Iordache A-M, Luculescu C. Periodontal Disease Monitoring by Raman Spectroscopy of Phosphates: New Insights into Pyrophosphate Activity. Diagnostics. 2024; 14(1):66. https://doi.org/10.3390/diagnostics14010066
Chicago/Turabian StyleGatin, Eduard, Stefan Marian Iordache, Dina Ilinca Gatin, Pal Nagy, Ana-Maria Iordache, and Catalin Luculescu. 2024. "Periodontal Disease Monitoring by Raman Spectroscopy of Phosphates: New Insights into Pyrophosphate Activity" Diagnostics 14, no. 1: 66. https://doi.org/10.3390/diagnostics14010066