
HCV RNA Quantification by a Domestic Commercial Assay: A Case Study among People Who Inject Drugs in Vietnam
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population and Study Conduct
2.3. Sample Collection and Processing
2.4. HIV and Hepatitis Biological Assessments
2.5. HCV RNA Quantification by Light Power iVA HCV qPCR Assay
2.6. HCV RNA Quantification by Xpert® HCV VL
2.7. HCV Genotyping
2.8. Data Collection and Data Analyses
3. Results
3.1. Study Population and Characteristics
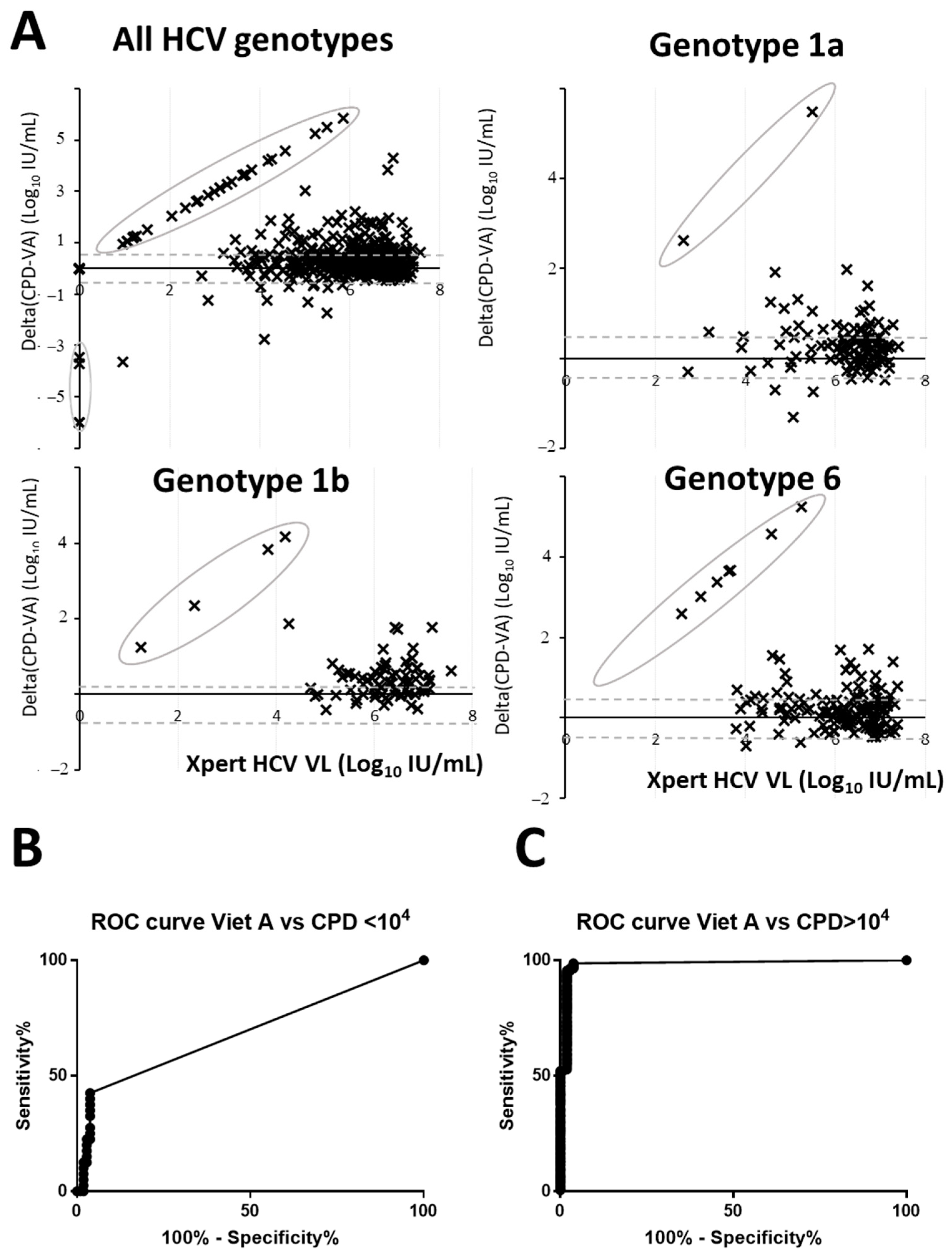
3.2. Diagnostic Accuracy Analysis
3.3. Factor Influencing the Discordant Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global Hepatitis Report. 2017. Available online: http://www.who.int/hepatitis/publications/global-hepatitis-report2017/en/ (accessed on 13 October 2023).
- Polaris Observatory. Available online: https://cdafound.org/dashboard/polaris/dashboard.html (accessed on 13 October 2023).
- WHO. Global Health Sector Strategies 2022–2030. Available online: https://www.who.int/publications/i/item/9789240053779 (accessed on 13 October 2023).
- WHO. Guidelines on Hepatitis B and C Testing. Available online: https://www.who.int/publications/i/item/9789241549981 (accessed on 13 October 2023).
- Buckwalter, S.P.; Sloan, L.M.; Cunningham, S.A.; Espy, M.J.; Uhl, J.R.; Jones, M.F.; Vetter, E.A.; Mandrekar, J.; Cockerill, F.R.; Pritt, B.S.; et al. Inhibition controls for qualitative real-time PCR assays: Are they necessary for all specimen matrices? J. Clin. Microbiol. 2014, 52, 2139–2143. [Google Scholar] [CrossRef] [PubMed]
- Polaris Observatory. Available online: https://cdafound.org/dashboard/polaris/maps_prev.html (accessed on 13 October 2023).
- Le Ngoc, C.; Tran Thi Thanh, T.; Tran Thi Lan, P.; Nguyen Mai, T.; Nguyen Hoa, T.; Nghiem My, N.; Le Van, T.; Le Manh, H.; Le Thanh, P.; Nguyen Van Vinh, C.; et al. Differential prevalence and geographic distribution of hepatitis C virus genotypes in acute and chronic hepatitis C patients in Vietnam. PLoS ONE 2019, 14, e0212734. [Google Scholar] [CrossRef] [PubMed]
- Des Jarlais, D.C.; Khue, P.M.; Feelemyer, J.; Arasteh, K.; Thi Huong, D.; Thi Hai Oanh, K.; Hoang Thi, G.; Nham, T.T.T.; Vu Hai, V.; Heckathorn, D.D.; et al. Using dual capture/recapture studies to estimate the population size of persons who inject drugs (PWID) in the city of Hai Phong, Vietnam. Drug Alcohol Depend. 2018, 185, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Des Jarlais, D.; Duong, H.T.; Pham Minh, K.; Khuat, O.H.; Nham, T.T.; Arasteh, K.; Feelemyer, J.; Heckathorn, D.D.; Peries, M.; Moles, J.P.; et al. and the Drive team. Integrated respondent-driven sampling and peer support for persons who inject drugs in Haiphong, Vietnam: A case study with implications for interventions. AIDS Care 2017, 51, 938–946. [Google Scholar] [CrossRef]
- Molès, J.-P.; Vallo, R.; Khue, P.M.; Huong, D.T.; Oanh, K.T.H.; Thoa, N.T.; Giang, H.T.; Thanh, N.T.T.; Vinh, V.H.; Bui Thi, T.A.; et al. HIV Control Programs Reduce HIV Incidence but Not HCV Incidence among People Who Inject Drugs in HaiPhong, Vietnam. Sci. Rep. 2020, 10, 6999. [Google Scholar] [CrossRef] [PubMed]
- Schrader, C.; Schielke, A.; Ellerbroek, L.; Johne, R. PCR inhibitors—Occurrence, properties and removal. J. Appl. Microbiol. 2012, 113, 1014–1026. [Google Scholar] [CrossRef] [PubMed]
- Pybus, O.G.; Barnes, E.; Taggart, R.; Lemey, P.; Markov, P.V.; Rasachak, B.; Syhavong, B.; Phetsouvanah, R.; Sheridan, I.; Humphreys, I.S.; et al. Genetic history of hepatitis C virus in East Asia. J. Virol. 2009, 83, 1071–1082. [Google Scholar] [CrossRef] [PubMed]
- Kalaghatgi, P.; Sikorski, A.M.; Knops, E.; Rupp, D.; Sierra, S.; Heger, E.; Neumann-Fraune, M.; Beggel, B.; Walker, A.; Timm, J.; et al. Geno2pheno[HCV]—A Web-based Interpretation System to Support Hepatitis C Treatment Decisions in the Era of Direct-Acting Antiviral Agents. PLoS ONE 2016, 11, e0155869. [Google Scholar] [CrossRef] [PubMed]
- Pawlotsky, J.M.; Bouvier-Alias, M.; Hezode, C.; Darthuy, F.; Remire, J.; Dhumeaux, D. Standardization of Hepatitis C Virus RNA Quantification. Hepatology 2000, 32, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Martinello, M.; Naggie, S.; Rockstroh, J.K.; Matthews, G.V. Direct-Acting Antiviral Therapy for Treatment of Acute and Recent Hepatitis C Virus Infection: A Narrative Review. Clin. Infect. Dis. 2023, 77 (Suppl. S3), S238–S244. [Google Scholar] [CrossRef]
- Martinello, M.; Hajarizadeh, B.; Grebely, J.; Dore, G.J.; Matthews, G.V. Management of Acute HCV Infection in the Era of Direct-Acting Antiviral Therapy. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 412–424. [Google Scholar] [CrossRef]
- Iwamoto, M.; Calzia, A.; Dublineau, A.; Rouet, F.; Nouhin, J.; Yann, S.; Pin, S.; Sun, C.; Sann, K.; Dimanche, C.; et al. Field Evaluation of GeneXpert® (Cepheid) HCV Performance for RNA Quantification in a Genotype 1 and 6 Predominant Patient Population in Cambodia. J. Viral Hepat. 2019, 26, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Larney, S.; Peacock, A.; Leung, J.; Colledge, S.; Hickman, M.; Vickerman, P.; Grebely, J.; Dumchev, K.V.; Griffiths, P.; Hines, L.; et al. Global, Regional, and Country-Level Coverage of Interventions to Prevent and Manage HIV and Hepatitis C among People Who Inject Drugs: A Systematic Review. Lancet Glob. Health 2017, 5, e1208–e1220. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Tao, Y.; Fajardo, E.; Reipold, E.I.; Chou, R.; Tucker, J.D.; Easterbrook, P. Diagnostic Accuracy of Point-of-Care HCV Viral Load Assays for HCV Diagnosis: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 1255. [Google Scholar] [CrossRef] [PubMed]
- Andreoni, M.; Coppola, N.; Craxì, A.; Fagiuoli, S.; Gardini, I.; Mangia, A.; Nava, F.A.; Pasqualetti, P. Meet-Test-Treat for HCV management: Patients’ and clinicians’ preferences in hospital and drug addiction services in Italy. BMC Infect. Dis. 2022, 22, 3. [Google Scholar] [CrossRef] [PubMed]
- Shiha, G.; Metwally, A.M.; Soliman, R.; Elbasiony, M.; Mikhail, N.N.H.; Easterbrook, P. An educate, test, and treat programme towards elimination of hepatitis C infection in Egypt: A community-based demonstration project. Lancet Gastroenterol. Hepatol. 2018, 3, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Smith, M. Validating Real-Time Polymerase Chain Reaction (PCR) Assays. Encycl. Virol. 2021, 5, 35–44. [Google Scholar] [CrossRef]
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE guidelines: Minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patients with Positive HCV Serology (n = 600) | |
|---|---|
| Socio-demographic data | |
| Gender, n (%) Male/Transgender | 575 (95.8) |
| Age, mean [SD] Years | 41.4 [7.9] |
| Co-infection, n (%) | |
| HIV | 220 (36.7) |
| HBV | 23 (5.9) * |
| Drug detected by urine test, n (%) | |
| Heroin | 600 (100) |
| Methadone | 383 (63.8) |
| Methamphetamine | 175 (29.2) |
| Cannabis | 8 (1.3) |
| Other drug consumption, self-report, n (%) | |
| Ketamine | 23 (3.8) |
| Ecstasy | 27 (4.5) |
| Amphetamines | 13 (2.2) |
| Cocaine | 2 (0.3) |
| Xpert HCV VL | ||||
|---|---|---|---|---|
| Positive | Negative | Total | ||
| Light Power iVA HCV VL | Positive | 462 | 4 | 465 |
| Negative | 29 | 101 | 131 | |
| Total | 491 | 105 | 596 | |
| HCV RNA Prevalence | 82% | 70% | 10% | 5% | 1% |
|---|---|---|---|---|---|
| Positive predictive value | 99.1% (97.7–99.7) | 98.3% (95.7–99.3) | 73.3% (51.2–87.8) | 56.5% (33.2–77.3) | 20.0% (8.7–39.5) |
| Negative predictive value | 78.1% (71.5–83.6) | 87.5% (83.0–90.9) | 99.3% (99.0–99.5) | 99.7% (99.5–99.8) | 99.9% (99.9–99.9) |
| Accuracy | 94.5% (92.3–96.2) | 94.7% (92.6–96.4) | 96.0% (94.1–97.4) | 96.1% (94.2–97.5) | 96.2% (94.3–97.6) |
| CPD Failure (n = 4) | CPD Failure/Discordant (n = 8) | VA Discordant (n = 29) | |
|---|---|---|---|
| Socio-demographic data | |||
| Gender, n (%) male/transgender | 4 (100) | 8 (100) | 27 (93.1) |
| Age, mean [SD] years | 36 [9.17] | 41.8 [8.55] | 40.8 [8.36] |
| Co-infection, n (%) | |||
| HIV | 0 (0) | 1 (12.5) | 15 (51.7) * |
| HBV | ° | £ | 5 (31.25) §* |
| HCV genotype | n = 0 | n = 0 | n = 14 |
| GT1A | 2 (14.3) | ||
| GT1B | 4 (28.6) | ||
| GT2 | 1 (7.1) | ||
| GT3A/B | 1(7.14) | ||
| GT6 | 6 (42.8) | ||
| Drug detected in urine, n (%) | |||
| Heroin | 4 (100) | 8 (100) | 29 (100) |
| Methadone | 0 (0) | 2 (25.0) * | 19 (65.5) |
| Methamphetamine | 1 (25.0) | 2 (25.0) | 5 (17.2) |
| Cannabis | 1 (25.0) | 1 (12.5) | 0 (0) |
| Drug consumption, self-report, n (%) | |||
| Ketamine | 0 (0) | 0 (0) | 2 (6.8) |
| Ecstasy | 0 (0) | 0 (0) | 2 (6.8) |
| Amphetamines | 0 (0) | 0 (0) | 1 (3.4) |
| Cocaine | 0 (0) | 0 (0) | 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nhu, Q.B.T.; Thuy, L.L.T.; Nguyen, H.T.; Thanh, B.N.; Rapoud, D.; Quillet, C.; Tran, H.T.; Vallo, R.; Tuyet, T.N.T.; Michel, L.; et al. HCV RNA Quantification by a Domestic Commercial Assay: A Case Study among People Who Inject Drugs in Vietnam. Diagnostics 2023, 13, 3456. https://doi.org/10.3390/diagnostics13223456
Nhu QBT, Thuy LLT, Nguyen HT, Thanh BN, Rapoud D, Quillet C, Tran HT, Vallo R, Tuyet TNT, Michel L, et al. HCV RNA Quantification by a Domestic Commercial Assay: A Case Study among People Who Inject Drugs in Vietnam. Diagnostics. 2023; 13(22):3456. https://doi.org/10.3390/diagnostics13223456
Chicago/Turabian StyleNhu, Quynh Bach Thi, Linh Le Thi Thuy, Hong Thi Nguyen, Binh Nguyen Thanh, Delphine Rapoud, Catherine Quillet, Hong Thi Tran, Roselyne Vallo, Thanh Nham Thi Tuyet, Laurent Michel, and et al. 2023. "HCV RNA Quantification by a Domestic Commercial Assay: A Case Study among People Who Inject Drugs in Vietnam" Diagnostics 13, no. 22: 3456. https://doi.org/10.3390/diagnostics13223456