
Lung Dual-Energy CT Perfusion Blood Volume as a Marker of Severity in Chronic Thromboembolic Pulmonary Hypertension
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
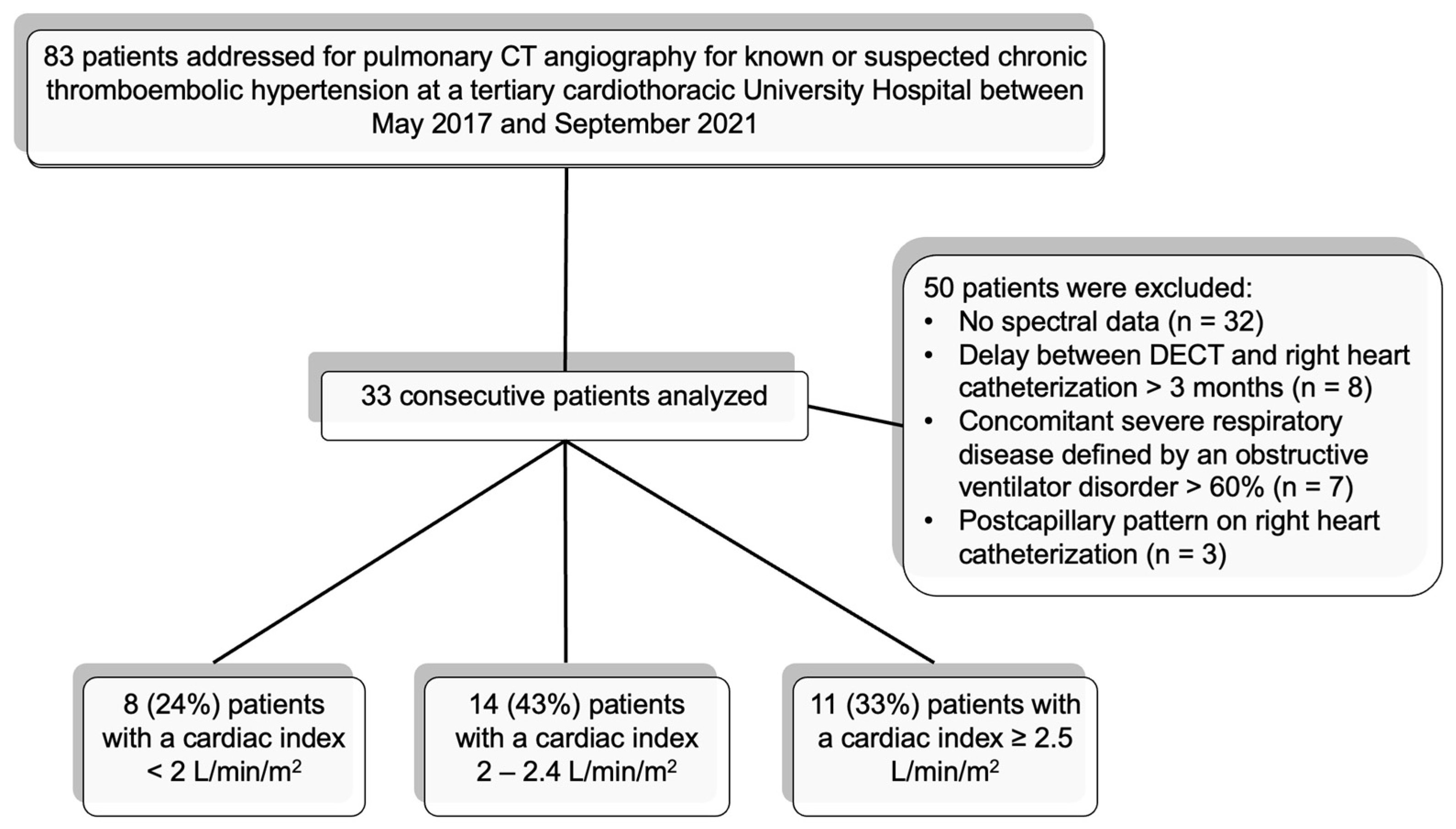
2.1. Population
2.2. Image Acquisition
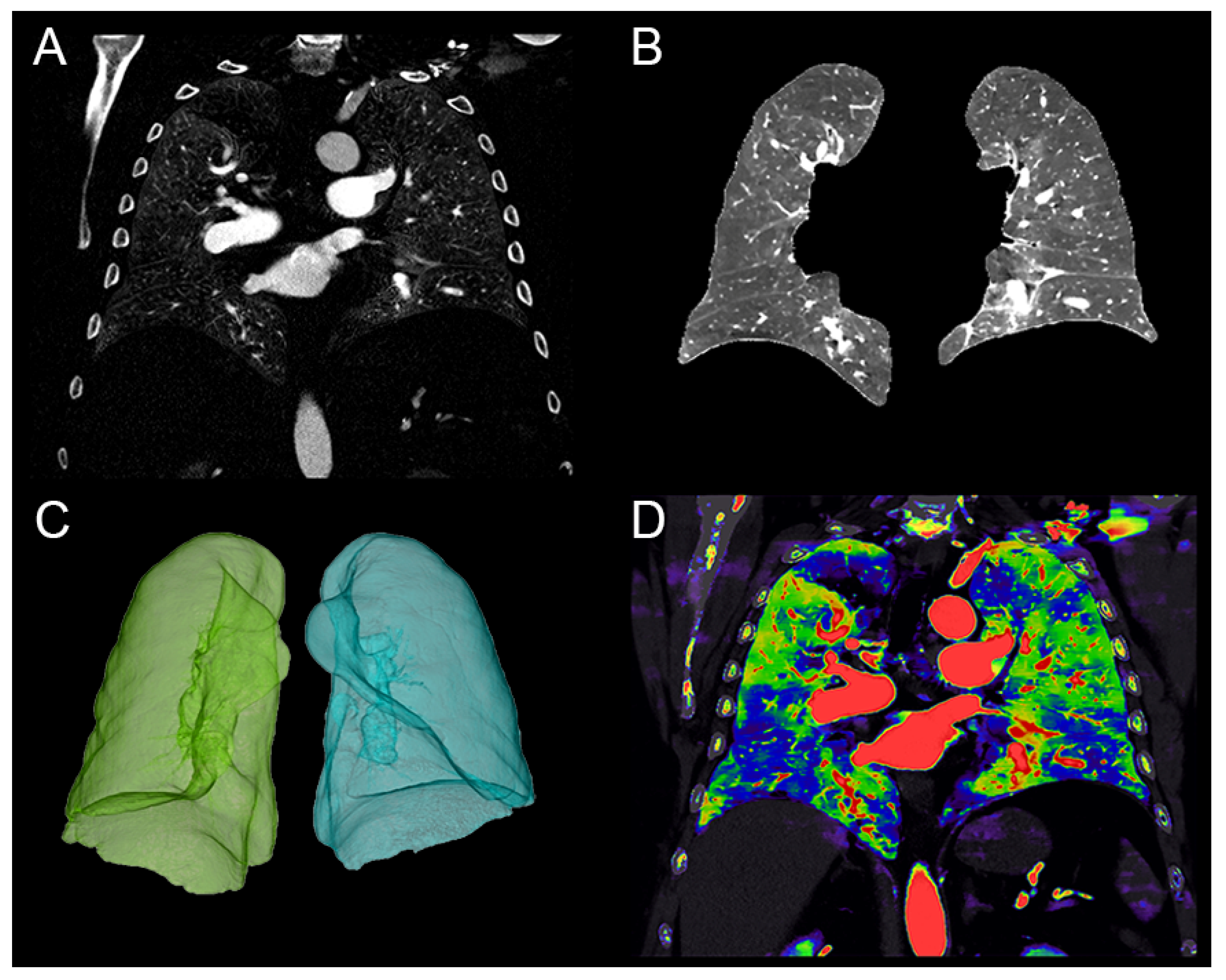
2.3. Quantitative Perfusion Blood Volume (PBV)
2.4. Per-Segment Qualitative Analysis of the PBV
2.5. Assessment of Clinical Severity
2.6. Statistical Analyses
3. Results
3.1. Patients’ Characteristics
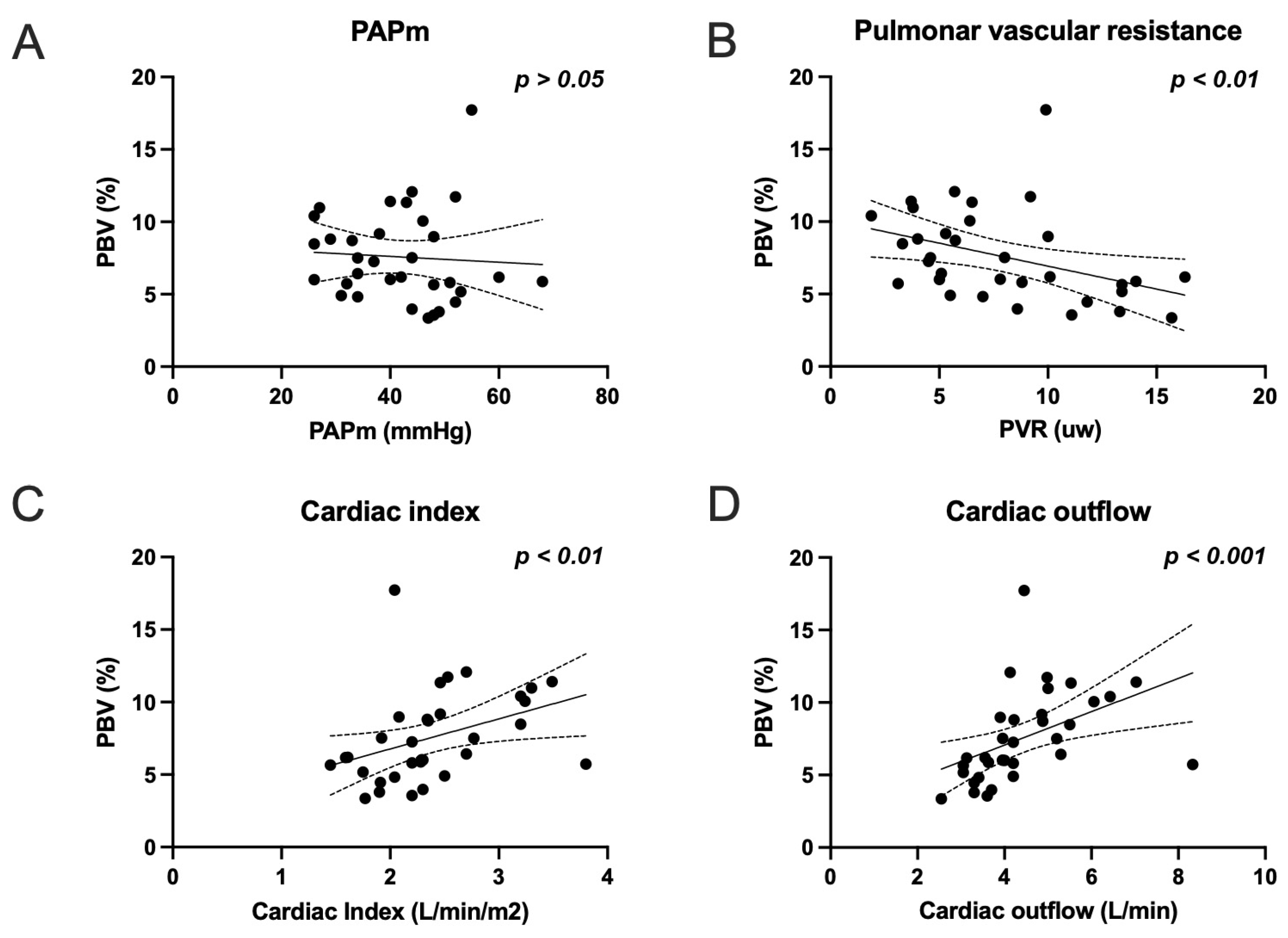
3.2. Correlation Analysis
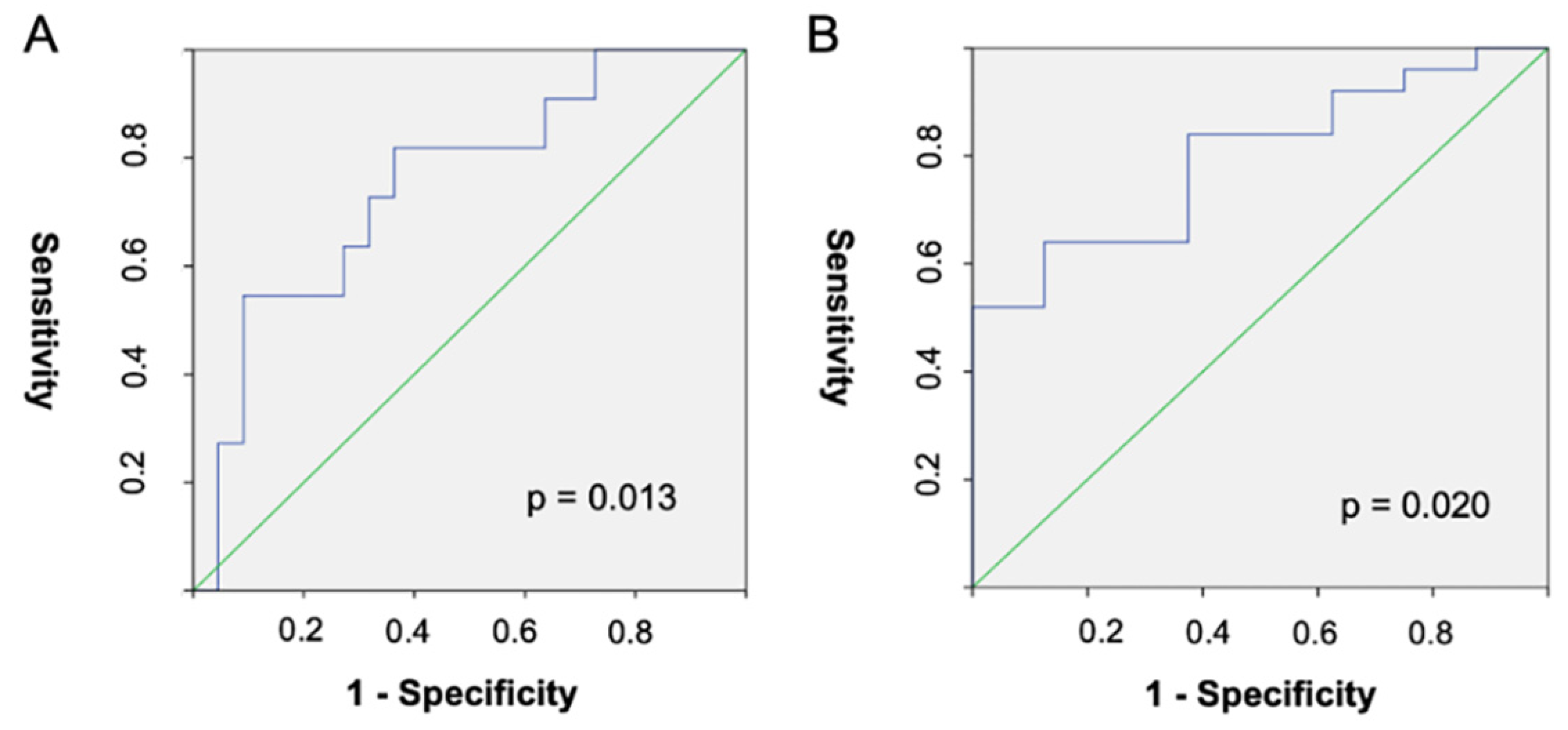
3.3. Diagnostic Performances of Quantitative PBV for Cardiac Index Groups
3.4. Radiation Dose Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pepke-Zaba, J.; Delcroix, M.; Lang, I.; Mayer, E.; Jansa, P.; Ambroz, D.; Treacy, C.; D’Armini, A.M.; Morsolini, M.; Snijder, R.; et al. Chronic Thromboembolic Pulmonary Hypertension (CTEPH): Results from an International Prospective Registry. Circulation 2011, 124, 1973–1981. [Google Scholar] [CrossRef] [Green Version]
- Becattini, C.; Agnelli, G.; Pesavento, R.; Silingardi, M.; Poggio, R.; Taliani, M.R.; Ageno, W. Incidence of Chronic Thromboembolic Pulmonary Hypertension After a First Episode of Pulmonary Embolism. Chest 2006, 130, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Pengo, V.; Lensing, A.W.; Prins, M.H.; Marchiori, A.; Davidson, B.L.; Tiozzo, F.; Albanese, P.; Biasiolo, A.; Pegoraro, C.; Iliceto, S.; et al. Incidence of Chronic Thromboembolic Pulmonary Hypertension after Pulmonary Embolism. N. Engl. J. Med. 2004, 8, 2257–2264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonneau, G.; Montani, D.; Celermajer, D.; Denton, C.P.; Gatzoulis, M.A.; Krowka, M.; Williams, P.G.; Souza, R. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur. Respir. J. 2019, 53, 1801913. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.H.; Delcroix, M.; Jais, X.; Madani, M.M.; Matsubara, H.; Mayer, E.; Ogo, T.; Tapson, V.F.; Ghofrani, H.-A.; Jenkins, D.P. Chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2019, 53, 1801915. [Google Scholar] [CrossRef] [Green Version]
- Humbert, M.; Guignabert, C.; Bonnet, S.; Dorfmüller, P.; Klinger, J.R.; Nicolls, M.R.; Olschewski, A.J.; Pullamsetti, S.S.; Schermuly, R.T.; Stenmark, K.R.; et al. Pathology and pathobiology of pulmonary hypertension: State of the art and research perspectives. Eur. Respir. J. 2019, 53, 1801887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorfmüller, P.; Günther, S.; Ghigna, M.-R.; De Montpréville, V.T.; Boulate, D.; Paul, J.-F.; Jais, X.; Decante, B.; Simonneau, G.; Dartevelle, P.; et al. Microvascular disease in chronic thromboembolic pulmonary hypertension: A role for pulmonary veins and systemic vasculature. Eur. Respir. J. 2014, 44, 1275–1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonneau, G.; Torbicki, A.; Dorfmüller, P.; Kim, N. The pathophysiology of chronic thromboembolic pulmonary hypertension. Eur. Respir. Rev. 2017, 26, 160112. [Google Scholar] [CrossRef] [Green Version]
- Galié, N.; Humbert, M.; Vachiéry, J.-L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Noordegraaf, A.V.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [CrossRef]
- Delcroix, M.; Torbicki, A.; Gopalan, D.; Sitbon, O.; Klok, F.A.; Lang, I.; Jenkins, D.; Kim, N.H.; Humbert, M.; Jais, X.; et al. ERS statement on chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2020, 57, 2002828. [Google Scholar] [CrossRef] [PubMed]
- Remy-Jardin, M.; Ryerson, C.J.; Schiebler, M.L.; Leung, A.N.C.; Wild, J.M.; Hoeper, M.M.; Alderson, P.O.; Goodman, L.R.; Mayo, J.; Haramati, L.B.; et al. Imaging of Pulmonary Hypertension in Adults: A Position Paper from the Fleischner Society. Radiology 2021, 298, 531–549. [Google Scholar] [CrossRef]
- Greffier, J.; Villani, N.; Defez, D.; Dabli, D.; Si-Mohamed, S. Spectral CT imaging: Technical principles of dual-energy CT and multi-energy photon-counting CT. Diagn. Interv. Imaging 2022, S2211-5684(22)00221-2. [Google Scholar] [CrossRef] [PubMed]
- Fuld, M.K.; Halaweish, A.F.; Haynes, S.E.; Divekar, A.A.; Guo, J.; Hoffman, E.A. Pulmonary Perfused Blood Volume with Dual-Energy CT as Surrogate for Pulmonary Perfusion Assessed with Dynamic Multidetector CT. Radiology 2013, 267, 747–756. [Google Scholar] [CrossRef] [Green Version]
- Tang, C.X.; Yang, G.F.; Schoepf, U.J.; Han, Z.H.; Qi, L.; Zhao, Y.E.; Wu, J.; Zhou, C.S.; Zhu, H.; Stubenrauch, A.C.; et al. Chronic thromboembolic pulmonary hypertension: Comparison of dual-energy computed tomography and single photon emission computed tomography in canines. Eur. J. Radiol. 2015, 85, 498–506. [Google Scholar] [CrossRef]
- Dournes, G.; Verdier, D.; Montaudon, M.; Bullier, E.; Rivière, A.; Dromer, C.; Picard, F.; Billes, M.-A.; Corneloup, O.; Laurent, F.; et al. Dual-energy CT perfusion and angiography in chronic thromboembolic pulmonary hypertension: Diagnostic accuracy and concordance with radionuclide scintigraphy. Eur. Radiol. 2013, 24, 42–51. [Google Scholar] [CrossRef]
- Si-Mohamed, S.; Moreau-Triby, C.; Tylski, P.; Tatard-Leitman, V.; Wdowik, Q.; Boccalini, S.; Dessouky, R.; Douek, P.; Boussel, L. Head-to-head comparison of lung perfusion with dual-energy CT and SPECT-CT. Diagn. Interv. Imaging 2020, 101, 299–310. [Google Scholar] [CrossRef]
- Otrakji, A.; Digumarthy, S.R.; Gullo, R.L.; Flores, E.; Shepard, J.-A.O.; Kalra, M.K. Dual-Energy CT: Spectrum of Thoracic Abnormalities. Radiographics 2016, 36, 38–52. [Google Scholar] [CrossRef] [PubMed]
- Apfaltrer, P.; Sudarski, S.; Schneider, D.; Nance, J.W.; Haubenreisser, H.; Fink, C.; Schoenberg, S.O.; Henzler, T. Value of monoenergetic low-kV dual energy CT datasets for improved image quality of CT pulmonary angiography. Eur. J. Radiol. 2014, 83, 322–328. [Google Scholar] [CrossRef]
- Weidman, E.K.; Plodkowski, A.J.; Halpenny, D.F.; Hayes, S.A.; Perez-Johnston, R.; Zheng, J.; Moskowitz, C.; Ginsberg, M.S. Dual-Energy CT Angiography for Detection of Pulmonary Emboli: Incremental Benefit of Iodine Maps. Radiology 2018, 289, 546–553. [Google Scholar] [CrossRef] [Green Version]
- Masy, M.; Giordano, J.; Petyt, G.; Hossein-Foucher, C.; Duhamel, A.; Kyheng, M.; De Groote, P.; Fertin, M.; Lamblin, N.; Bervar, J.-F.; et al. Dual-energy CT (DECT) lung perfusion in pulmonary hypertension: Concordance rate with V/Q scintigraphy in diagnosing chronic thromboembolic pulmonary hypertension (CTEPH). Eur. Radiol. 2018, 28, 5100–5110. [Google Scholar] [CrossRef] [PubMed]
- Kosmala, A.; Gruschwitz, P.; Veldhoen, S.; Weng, A.M.; Krauss, B.; Bley, T.A.; Petritsch, B. Dual-energy CT angiography in suspected pulmonary embolism: Influence of injection protocols on image quality and perfused blood volume. Int. J. Cardiovasc. Imaging 2020, 36, 2051–2059. [Google Scholar] [CrossRef]
- Delcroix, M.; Staehler, G.; Gall, H.; Grünig, E.; Held, M.; Halank, M.; Klose, H.; Vonk-Noordegraaf, A.; Rosenkranz, S.; Pepke-Zaba, J.; et al. Risk assessment in medically treated chronic thromboembolic pulmonary hypertension patients. Eur. Respir. J. 2018, 52, 1800248. [Google Scholar] [CrossRef] [PubMed]
- Humbert, M.; Farber, H.W.; Ghofrani, A.; Benza, R.L.; Busse, D.; Meier, C.; Hoeper, M.M. Risk assessment in pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2019, 53, 1802004. [Google Scholar] [CrossRef] [PubMed]
- Hoey, E.T.; Mirsadraee, S.; Pepke-Zaba, J.; Jenkins, D.P.; Gopalan, D.; Screaton, N.J. Dual-energy CT angiography for assessment of regional pulmonary perfusion in patients with chronic thromboembolic pulmonary hypertension: Initial experience. AJR Am. J. Roentgenol. 2011, 196, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Takagi, H.; Ota, H.; Sugimura, K.; Otani, K.; Tominaga, J.; Aoki, T.; Tatebe, S.; Miura, M.; Yamamoto, S.; Sato, H.; et al. Dual-energy CT to estimate clinical severity of chronic thromboembolic pulmonary hypertension: Comparison with invasive right heart catheterization. Eur. J. Radiol. 2016, 85, 1574–1580. [Google Scholar] [CrossRef]
- Meinel, F.G.; Graef, A.; Thierfelder, K.M.; Armbruster, M.; Schild, C.; Neurohr, C.; Reiser, M.F.; Johnson, T.R.C. Automated Quantification of Pulmonary Perfused Blood Volume by Dual-Energy CTPA in Chronic Thromboembolic Pulmonary Hypertension. Rofo 2013, 186, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Tsutsumi, Y.; Iwano, S.; Okumura, N.; Adachi, S.; Abe, S.; Kondo, T.; Kato, K.; Naganawa, S. Assessment of Severity in Chronic Thromboembolic Pulmonary Hypertension by Quantitative Parameters of Dual-Energy Computed Tomography. J. Comput. Assist. Tomogr. 2020, 44, 578–585. [Google Scholar] [CrossRef]
- Renard, B.; Remy-Jardin, M.; Santangelo, T.P.; Faivre, J.-B.; Tacelli, N.; Remy, J.; Duhamel, A. Dual-energy CT angiography of chronic thromboembolic disease: Can it help recognize links between the severity of pulmonary arterial obstruction and perfusion defects? Eur. J. Radiol. 2011, 79, 467–472. [Google Scholar] [CrossRef]
- Endrys, J.; Hayat, N.; Cherian, G. Comparison of bronchopulmonary collaterals and collateral blood flow in patients with chronic thromboembolic and primary pulmonary hypertension. Heart 1997, 78, 171–176. [Google Scholar] [CrossRef] [Green Version]
- Koike, H.; Sueyoshi, E.; Sakamoto, I.; Uetani, M. Clinical Significance of Late Phase of Lung Perfusion Blood Volume (Lung Perfusion Blood Volume) Quantified by Dual-Energy Computed Tomography in Patients with Pulmonary Thromboembolism. J. Thorac. Imag. 2017, 32, 43–49. [Google Scholar] [CrossRef]
- Si-Mohamed, S.; Chebib, N.; Sigovan, M.; Zumbihl, L.; Turquier, S.; Boccalini, S.; Boussel, L.; Mornex, J.-F.; Cottin, V.; Douek, P. In vivo demonstration of pulmonary microvascular involvement in COVID-19 using dual-energy computed tomography. Eur. Respir. J. 2020, 56, 2002608. [Google Scholar] [CrossRef] [PubMed]
- Kroeger, J.R.; Zöllner, J.; Gerhardt, F.; Rosenkranz, S.; Gertz, R.J.; Kerszenblat, S.; Pahn, G.; Maintz, D.; Bunck, A.C. Detection of patients with chronic thromboembolic pulmonary hypertension by volumetric iodine quantification in the lung—a case control study. Quant. Imaging Med. Surg. 2022, 12, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Nie, R.Z.; Homayounieh, F.; Schmidt, B.; Flohr, T.; Kalra, M.K. Quantitative lobar pulmonary perfusion assessment on dual-energy CT pulmonary angiography: Applications in pulmonary embolism. Eur. Radiol. 2020, 30, 2535–2542. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population (n = 33) | Value * | ±SD | [Min–Max] |
|---|---|---|---|
| Age (years) | 68 | ±15 | [63–78] |
| Sex (male) | 11 (33.3%) | ||
| Height (cm) | 165.2 | ±8.5 | [150–183] |
| Weight (kg) | 77.3 | ±16.7 | [44–114] |
| Body mass index (kg/m2) | 28.1 | ±5.1 | [17–38] |
| Delay between pulmonary CT angiography and right heart catheterization | 5 | [1–7] | |
| DECT parameters | |||
| Ratio of the iodine concentrations in the pulmonary trunk and the left auricle | 2.4 | [1.7–3.2] | |
| Quantitative perfused blood volume | 6.5 | [5.4–9.6] | |
| Qualitative perfused blood volume | 41.1 | ±13.4 | [16–67] |
| Iodine concentration in the pulmonary trunk (mg/mL) | 11.12 | [9.16–13.72] | |
| Right heart catheterization parameter | |||
| Mean pulmonary artery pressure (mmHg) | 41.8 | ±10.4 | [26–68] |
| Systolic pulmonary artery pressure (mmHg) | 70.9 | ±17.5 | [39–106] |
| Diastolic pulmonary artery pressure (mmHg) | 25.88 | ±8.2 | [14–48] |
| Right atrial pressure (mmHg) | 7.1 | ±3.4 | [1–16] |
| Pulmonary capillary wedge pressure (mmHg) | 9.7 | ±3.4 | [5–18] |
| Pulmonary vascular resistance (WU) | 7.7 | ±3.9 | [1.9–16.3] |
| Cardiac output (L/min) | 4.2 | [3.6–5.1] | |
| Cardiac index (L/min/m2) | 2.4 | ±0.6 | [1.4–3.8] |
| Other parameters | |||
| 6 min walk distance (min) (n = 28) | 365 | ±164 | [85–645] |
| Brain natriuretic peptide (ng/L) | 171 | [23.5–713] | |
| WHO-fc (n = 32), n (%) | |||
| Grade I | 4 (12.5%) | ||
| Grade II | 14 (43.7%) | ||
| Grade III | 12 (37.5%) | ||
| Grade IV | 2 (6.3%) |
| PAPs | PAPd | PAPm | RAP | PAWP | PVR | CO | CI | 6MWD | BNP | WHOfc | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Quantitative PBV | r | −0.302 | −0.194 | −0.181 | 0.103 | 0.118 | −0.466 ** | 0.672 *** | 0.519 ** | 0.071 | −0.307 | −0.189 |
| p | 0.088 | 0.279 | 0.314 | 0.568 | 0.513 | 0.006 | 0.0001 | 0.002 | 0.696 | 0.083 | 0.291 | |
| Qualitative PBV | r | 0.086 | 0.231 | 0.15 | 0.009 | −0.081 | 0.234 | −0.251 | −0.095 | 0.089 | 0.339 | 0.188 |
| p | 0.636 | 0.195 | 0.405 | 0.959 | 0.655 | 0.19 | 0.159 | 0.597 | 0.621 | 0.054 | 0.294 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Si-Mohamed, S.A.; Zumbihl, L.; Turquier, S.; Boccalini, S.; Mornex, J.-F.; Douek, P.; Cottin, V.; Boussel, L. Lung Dual-Energy CT Perfusion Blood Volume as a Marker of Severity in Chronic Thromboembolic Pulmonary Hypertension. Diagnostics 2023, 13, 769. https://doi.org/10.3390/diagnostics13040769
Si-Mohamed SA, Zumbihl L, Turquier S, Boccalini S, Mornex J-F, Douek P, Cottin V, Boussel L. Lung Dual-Energy CT Perfusion Blood Volume as a Marker of Severity in Chronic Thromboembolic Pulmonary Hypertension. Diagnostics. 2023; 13(4):769. https://doi.org/10.3390/diagnostics13040769
Chicago/Turabian StyleSi-Mohamed, Salim A., Léa Zumbihl, Ségolène Turquier, Sara Boccalini, Jean-Francois Mornex, Philippe Douek, Vincent Cottin, and Loic Boussel. 2023. "Lung Dual-Energy CT Perfusion Blood Volume as a Marker of Severity in Chronic Thromboembolic Pulmonary Hypertension" Diagnostics 13, no. 4: 769. https://doi.org/10.3390/diagnostics13040769