
A Novel Modality Enables New Evidence-Based Individual Risk Stratification That Can Potentially Lead to Decisive Management and Treatment Decisions in Prostate Cancer
Abstract
:1. Introduction
1.1. Prostate Cancer Background
1.2. Zinc Depletion as a PCa Marker
1.3. X-ray Fluorescence (XRF)
2. Materials and Methods
2.1. X-ray Fluorescence (XRF) for ScoRisk
2.2. The Souraski Clinical Study
2.2.1. Equipment
2.2.2. Study Routine
2.2.3. Pathology Report
2.3. Data Analysis and Results
2.3.1. Background
2.3.2. Analysis Observations
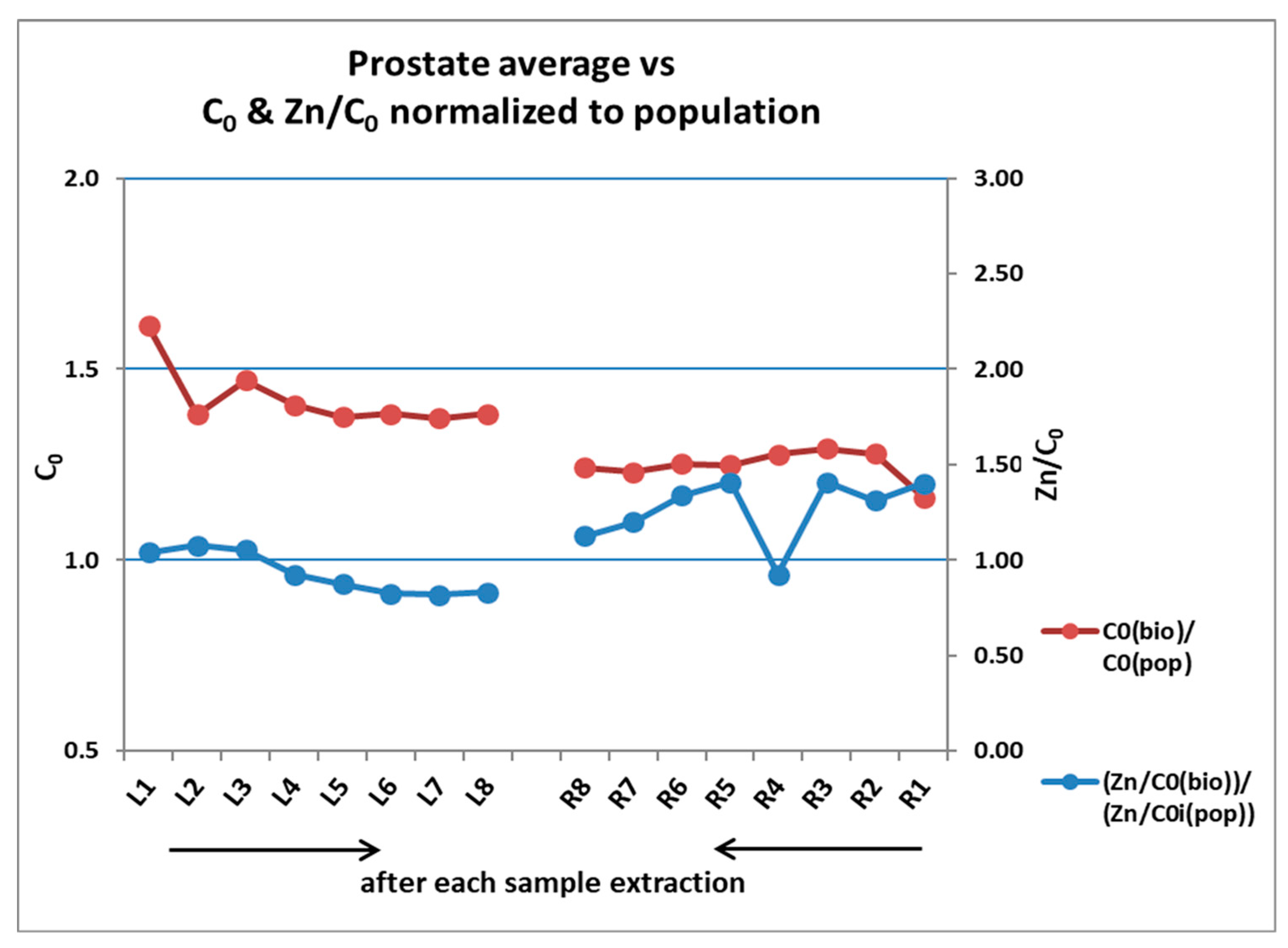
- Zn levels vary substantially among prostates and, therefore, a population (all prostates, all cores, and all pixels) normalization scheme was introduced.
- Each prostate has a unique malignancy signature/score (akin to Epstein’s prostate grade [12]), which is dependent not only on the Zn content, but also on tissue characteristics typical of PCa—oncogenic manifestations of neoplasia/hyperplasia in glands and tissue proliferation mechanisms, which are known indicators of the malignancy processes.
2.3.3. Analysis Steps—Scanning and Data Generation
2.3.4. Data Cleaning—Population and Prostate Levels
- The normalized population level data were cleaned to remove invalid pixels: non-uniform, or certain edge pixels, or pixels that were disconnected from the sample, or very small and/or very thin pixels, typically characterized by very small C and very small Zn/C.
- Pixels with very small ΔC, indicative of low or no glandular tissue.
2.3.5. Prostates—Population Data
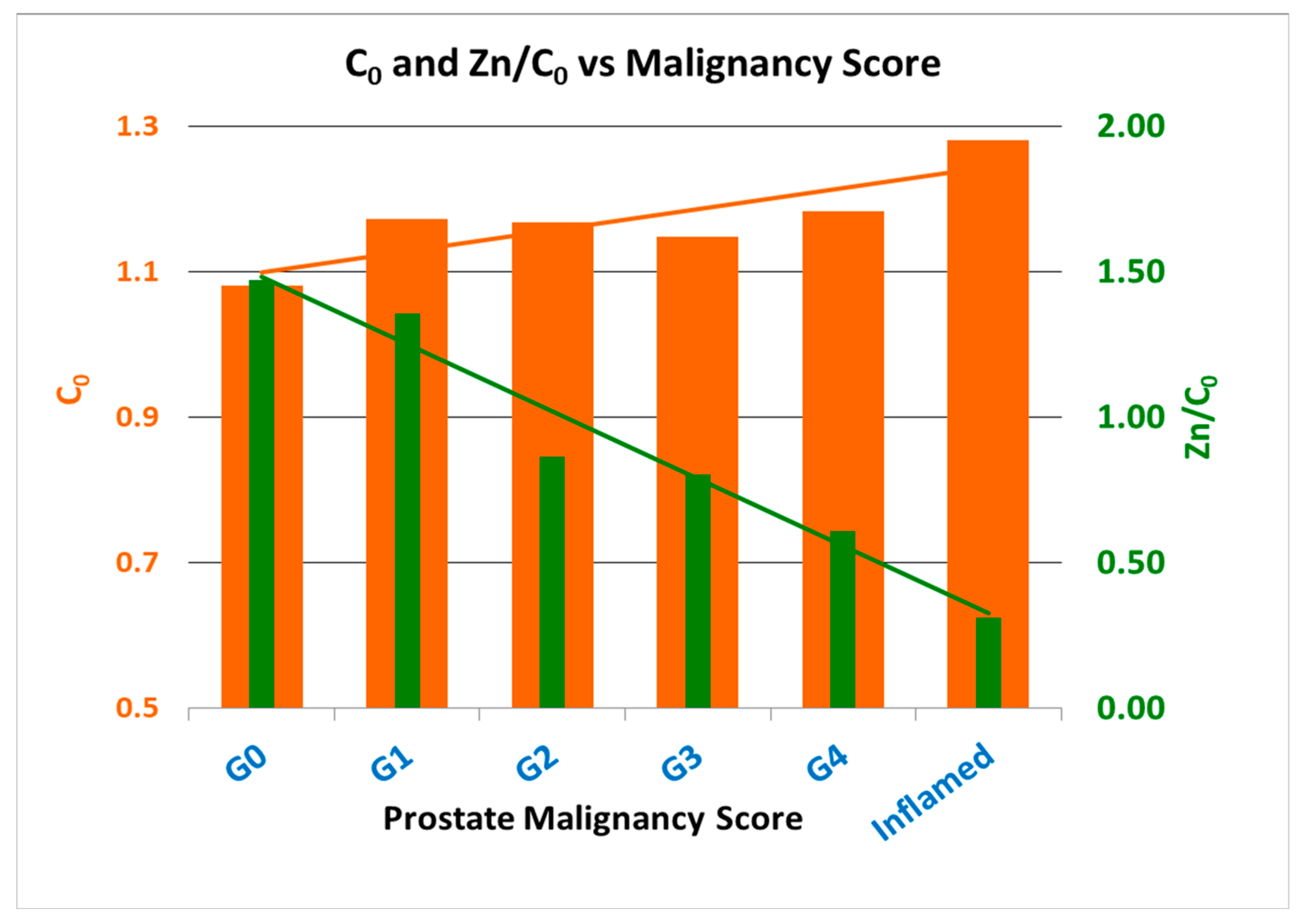
2.4. Prostates Aggressiveness—Malignancy Score
- G0 corresponds to prostates where no positive samples were identified during the biopsy due to either the absence of tissue proliferation or Zn depletion or both at the prostate and core levels; while,
- G1 corresponds to a prostate where tissue proliferation (C0) and Zn depletion for the prostate were around the population average and only a few samples had levels of C0 and Zn depletion (Zn/C0) characteristic of low-malignancy-score PCa.
2.4.1. Prostate Malignancy Score—Diagnosis Results
- For low-/mid-Zn prostates (positive):
- ●
- The mean C0 for PCa samples classes was significantly higher than those for the benign classes.
- ●
- The mean Zn/C0 for PCa samples classes was smaller (and, for the majority of the classes, much smaller) than for the benign sample classes.
- For high-Zn prostates:
- ●
- High-Zn PCa prostates had much higher C0 (tissue proliferation) values than those for high-Zn benign prostates.
- ●
- High malignancy score in a prostate was also correlated with a high number of positive cores in the prostate.
- ●
- Decrease in Zn/C0, in tandem with high tissue proliferation (C0), was indicative of a higher malignancy score.
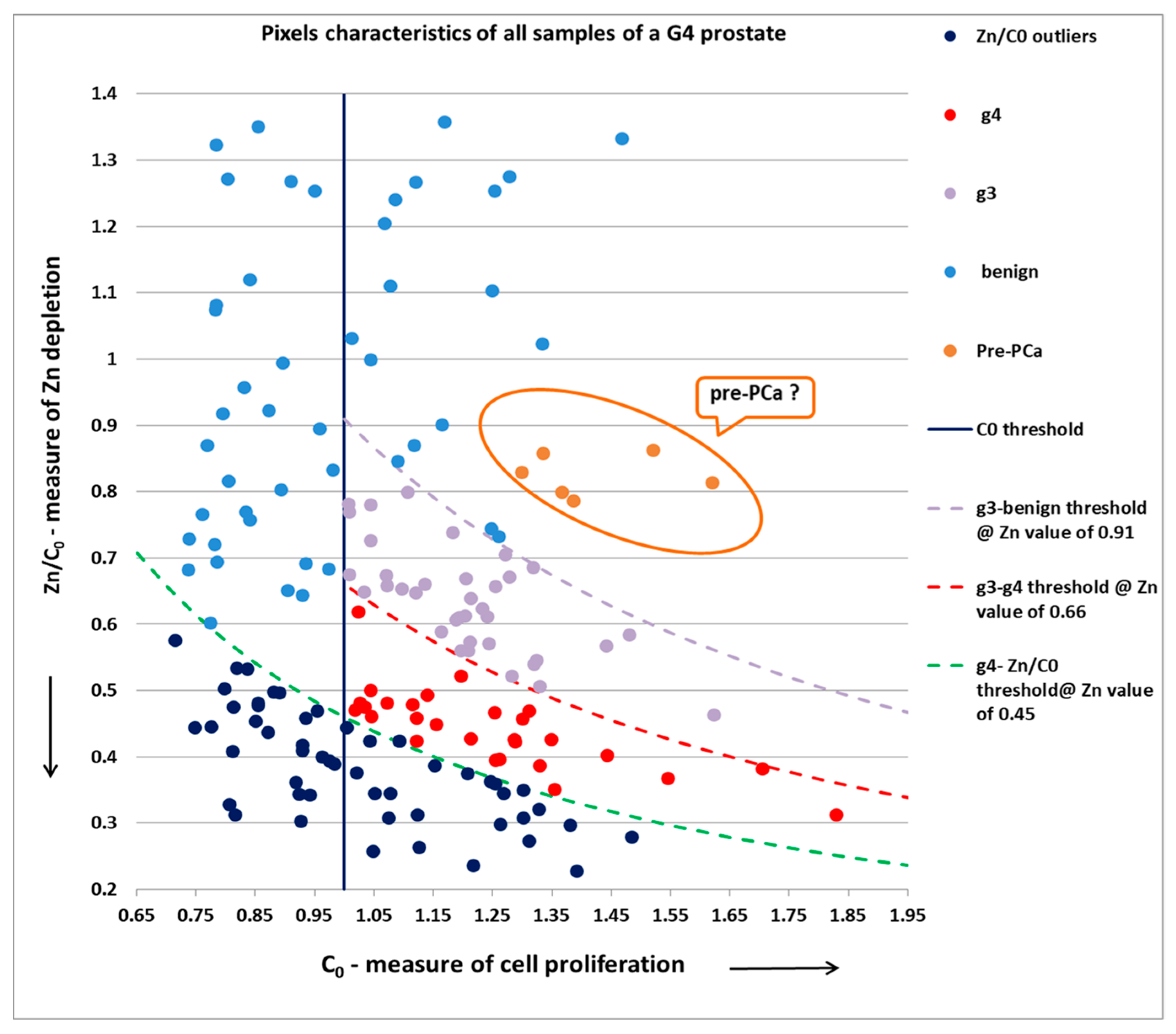
2.4.2. Pixels Grading
- High Zn/C0 → no Zn depletion → non-PCa pixel.
- Very low C0 → no tissue proliferation → non-PCa pixel.
- Mid or low Zn/C0 and mid/high C0 → PCa pixel.
2.4.3. Biopsy Metrics
3. Considerations on the Routine Use of ScoRisk in the Clinic
3.1. Flowchart—as Part of Routine Clinical Flow
3.2. Interactive Biopsy Guidance
3.2.1. Interactive Guidance Examples
- Low prostate malignancy score in tandem with low-grade samples: recommendation to abandon the current region and continue to the next;
- In case of a mid to high malignancy score in tandem with low- to mid-grade samples: continue taking more samples from the same region to increase the positive yield (cancer volume) and sharpen the index lesion;
- In the event inflammation (prostatitis) is detected: consider stopping the biopsy and avoid the extraction of unnecessary additional samples.
3.2.2. Personalized Treatment Recommendations
4. Discussion
- It is a direct measurement of the most reliable prostate cancer malignancy indicator known to science, Zn depletion, accurately measured by XRF.
- The newly discovered ability of XRF to discriminate tissue-related signs of cancer (including tissue proliferation), which is an additional marker of PCa and further improves the accuracy of ScoRisk.
- The ability to remove and scan the most suspected samples, thanks to real-time guidance during the biopsy, in order to extract as many positive, or “closest” to positive, biopsy cores.
- Zn depletion precedes the morphology changes that the current pathology is based on, thereby providing earlier detection.
- The measurements are on the full depth (3D) of the needle biopsy core, providing inherently more representative results than looking at a 25-micron-thin microscopy slide sample (over 1/50 thinner than the original biopsy core, on the surface of it only).
- The ability to determine the prostate-level malignancy score, which is a higher granularity prostate-grading capability, especially effective in doubtful cases, where the urologist/oncologist seeks support in decision making, beyond Epstein’s grading scheme. Concurrently, our modality is designed to generate higher granularity sample grading, both through continuous reference to a large, AI-enhanced, continuously updated population database incorporating the various pathologies and the corresponding XRF parameters
4.1. Limitations of the Study
4.2. Short-Term Plans
- In addition to the clinical trials for the regulatory steps, conduct on-going systematic retrospective follow-up on treatment recommendations, to ensure the fidelity of the prostate malignancy score in providing improved risk stratification for better treatment recommendations.
- Implement a real-time guidance and grading digital code, centered on multivariate statistical analysis and deep-learning tools, including a large-scale accessible population database and real-time diagnosis, grading/scoring and guidance during the biopsy.
- Implement a built-in camera to simultaneously measure the volume for each pixel during the XRF scan to further improve normalization.
- Take advantage of digital pathology during the next studies/trials, as it is not practical for pathologists to perform pixel-by-pixel analysis.
4.3. Long-Term Plans
- As Zn depletion precedes the morphological changes, conduct on-going follow-up studies to reinforce ScoRisk’s sample grading as an independent standard by gathering statistical information rather than solely comparing to pathology findings.
- Introduce a dedicated tool for analyzing a prostate following prostatectomy for completely automatic analysis of whole-mount samples that will be much thicker than today’s microtomes and able to create a much more accurate 3D malignancy map reconstruction of the whole prostate.
4.4. One-Stop-Shop
5. Patents
- Granted, US 9,052,319—METHOD OF GUIDING PROSTATE BIOPSY LOCATION—SIMON Avi et al.
- Pending, WO2021/009762—METHOD AND SYSTEM FOR ANALYZING PROSTATE BIOPSY—WEKSLER Meir et al.
- Pending, 2022—WEKSLER Meir et al.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grummet, J.; Gorin, M.A.; Popert, R.; O’Brien, T.; Lamb, A.D.; Hadaschik, B.; Radtke, J.P.; Wagenlehner, F.; Baco, E.; Moore, C.M.; et al. “TREXIT 2020”: Why the time to abandon transrectal prostate biopsy starts now. Prostate Cancer Prostatic Dis. 2020, 23, 62–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinheiro, P.C.; Patel, R.H.; Rui, H.; Jerónimo, C. Biomarkers and personalized risk stratification for patients with clinically localized prostate cancer. Expert Rev. Anticancer Ther. 2014, 14, 1349–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costello, L.C.; Franklin, R.B. A comprehensive review of the role of zinc in normal prostate function and metabolism; and its implications in prostate cancer. Arch. Biochem. Biophys. 2016, 611, 100–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costello, L.C.; Franklin, R.B. The clinical relevance of the metabolism of prostate cancer; zinc and tumor suppression: Connecting the dots. Mol. Cancer 2006, 5, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costello, L.C.; Franklin, R.B.; Feng, P.; Tan, M.; Bagasra, O. Zinc and Prostate Cancer: A Critical Scientific, Medical, and Public Interest Issue (United States). Cancer Causes Control 2005, 16, 901–915. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Ho, E. Zinc and prostatic cancer. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 640–645. [Google Scholar] [CrossRef] [Green Version]
- Zaichick, V. A Systematic Review of the Zinc content of the normal human prostate gland. Biol. Trace Elem. Res. 2021, 199, 3593–3607. [Google Scholar] [CrossRef] [PubMed]
- Cortesi, M.; Rachel, C.; Breskin, A.; Vartsky, D.; Ramon, J.; Raviv, G.; Volkov, A.; Fridman, E. Evaluating the cancer detection and grading potential of prostatic-zinc imaging: A simulation study. Phys. Med. Biol. 2009, 54, 781–796. [Google Scholar] [CrossRef] [PubMed]
- Cortesi, M.; Fridman, E.; Volkov, A.; Shilstein, S.; Chechik, R.; Breskin, A.; Vartsky, D.; Kleinman, N.; Kogan, G.; Moriel, E.; et al. Clinical Assessment of the Cancer Diagnostic Value of Prostatic Zinc: A Comprehensive Needle-Biopsy Study. Prostate 2008, 68, 994–1006. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Yang, D.-R.; Xue, B.-X.; Wang, C.; Chen, H.-B.; Dong, Y.; Wang, C.-S.; Shan, Y.-X. Elastography Targeted Prostate Biopsy. Oncol. Lett. 2017, 14, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, J.M.; Ferguson, J.R. XRF Technical Overview. 2012. University of Missouri Research Reactor (missouri.edu). Available online: https://archaeometry.missouri.edu/xrf_technical.html (accessed on 20 December 2022).
- Epstein, J.I.; Zelefsky, M.J.; Sjoberg, D.D.; Nelson, J.B.; Egevad, L.; Magi-Galluzzi, C.; Vickers, J.A.; Parwani, A.V.; Reuter, V.E.; Fine, S.W.; et al. A Contemporary Prostate Cancer Grading System: A Validated Alternative to the Gleason Score. Eur. Urol. 2016, 69, 428–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.; Ong, S.; Lawrentschuk, N. Biomarkers Accurately Inform Treatment Decisions in Localized Prostate Cancer. Eur. Assoc. Urol. 2022, 8, 643–645. [Google Scholar] [CrossRef]
- Cooperberg, M.R. Biomarkers in Urologic Oncology: So Much Progress, So Much Yet to Do. Eur. Urol. Focus 2022, 8, 891–892. [Google Scholar] [CrossRef] [PubMed]
- Moul, J.W. Biomarkers Accurately Inform Treatment Decisions in Localized Prostate Cancer. Eur. Urol. Focus 2022, 8, 641–642. [Google Scholar] [CrossRef] [PubMed]
- Okoth, L.A.; Harris, A.C.; Singhal, U.; Cher, M.L.; Spratt, D.E.; Morgan, T.M. Trials in the Key of G: Building Level 1 Evidence on the Real-world Effectiveness of Prostate Biomarkers. Eur. Urol. Focus 2022, 8, 897–900. [Google Scholar] [CrossRef] [PubMed]
- Vince, R.A., Jr.; Jiang, R.; Qi, J.; Tosoian, J.J.; Takele, R.; Feng, F.Y.; Linsell, S.; Johnson, A.; Shetty, S.; Hurley, P.; et al. Impact of Decipher Biopsy testing on clinical outcomes in localized prostate cancer in a prospective statewide collaborative. Prostate Cancer Prostatic Dis. 2022, 25, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Roehrborn, C. Urology; 30 April 2018—Blog; Prostate Cancer Genomic Testing is Flawed: Three Reasons Why. Available online: https://utswmed.org/medblog/prostate-cancer-genomic-testing/ (accessed on 20 December 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Statistics | C0 (Tissue) | C | ΔC= | Zn | Zn/C | Zn/C0 |
|---|---|---|---|---|---|---|
| (C0 − C) | ||||||
| Mean | 1.14 | 1 | 0.14 | 1 | 1.41 | 1.23 |
| STD | 0.24 | 0.23 | 0.05 | 0.76 | 1.01 | 0.88 |
| Q1 | 0.96 | 0.83 | 0.1 | 0.47 | 0.6 | 0.6 |
| Median | 1.13 | 0.99 | 0.13 | 0.78 | 1.1 | 0.97 |
| Q3 | 1.29 | 1.15 | 0.17 | 1.24 | 1.76 | 1.54 |
| Metrics | Prostate Level | Sample Level |
|---|---|---|
| After data cleaning * P TP (true positive) | 20 10 10 | 308 64 57 |
| N (including Inflamed) TN (true negative) | 10 10 | 244 240 |
| Inflamed prostates (out of TN) | 2 | 32 |
| False N False P Sensitivity | 0 0 100% | 7 4 89% |
| Specificity Accuracy | 100% 100% | 98% 96% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weksler, M.; Simon, A.; Lenkinski, R.E.; Landsman, H.; Matzkin, H.; Mabjeesh, N.; Leibovitch, I. A Novel Modality Enables New Evidence-Based Individual Risk Stratification That Can Potentially Lead to Decisive Management and Treatment Decisions in Prostate Cancer. Diagnostics 2023, 13, 424. https://doi.org/10.3390/diagnostics13030424
Weksler M, Simon A, Lenkinski RE, Landsman H, Matzkin H, Mabjeesh N, Leibovitch I. A Novel Modality Enables New Evidence-Based Individual Risk Stratification That Can Potentially Lead to Decisive Management and Treatment Decisions in Prostate Cancer. Diagnostics. 2023; 13(3):424. https://doi.org/10.3390/diagnostics13030424
Chicago/Turabian StyleWeksler, Meir, Avi Simon, Robert E. Lenkinski, Hagar Landsman, Haim Matzkin, Nicola Mabjeesh, and Ilan Leibovitch. 2023. "A Novel Modality Enables New Evidence-Based Individual Risk Stratification That Can Potentially Lead to Decisive Management and Treatment Decisions in Prostate Cancer" Diagnostics 13, no. 3: 424. https://doi.org/10.3390/diagnostics13030424