

The Role of TAR DNA Binding Protein 43 (TDP-43) as a CandiDate Biomarker of Amyotrophic Lateral Sclerosis: A Systematic Review and Meta-Analysis
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Study Selection
- the manuscript describes a retrospective and prospective study design;
- it was written in the English language;
- the study must provide a full description of the method used to measure TDP-43 levels;
- the study must use TDP-43 as a biomarker in the blood or CSF to differentiate ALS patients from a control group;
- the study must use a quantitative method for TDP-43 detection;
- the study must provide sufficient data to calculate the outcome.
- evaluation of only the prognostic role of TDP-43;
- studies without healthy controls or without disease control;
- letters, case reports, animal studies, reviews, and meta-analyses;
- languages other than English;
- qualitative method for TDP-43 detection;
- full text not found.
2.3. Data Collection
2.4. Statistical Analysis
3. Results
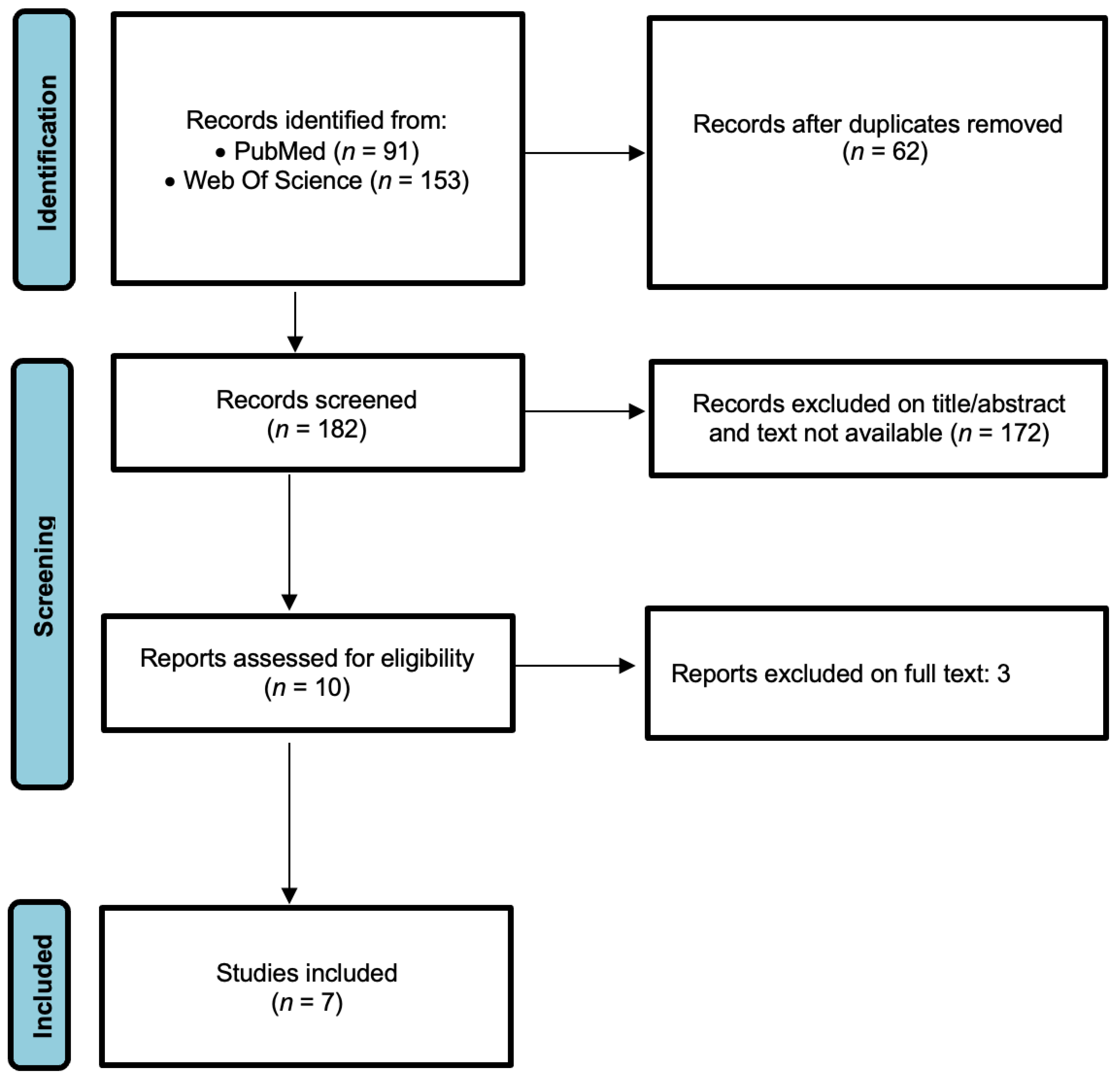
3.1. Study Selection
3.2. Study Characteristics and Quality Assessment
3.3. Diagnostic Accuracy of TDP-43 for ALS
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Strong, M.J.; Abrahams, S.; Goldstein, L.H.; Woolley, S.; Mclaughlin, P.; Snowden, J.; Mioshi, E.; Roberts-South, A.; Benatar, M.; HortobáGyi, T.; et al. Amyotrophic lateral sclerosis—Frontotemporal spectrum disorder (ALS-FTSD): Revised diagnostic criteria. Amyotroph Lateral Scler Front. Degener 2017, 18, 153–174. [Google Scholar] [CrossRef] [PubMed]
- Hardiman, O.; Al-Chalabi, A.; Chio, A.; Corr, E.M.; Logroscino, G.; Robberecht, W.; Shaw, P.J.; Simmons, Z.; van den Berg, L.H. Amyotrophic lateral sclerosis. Nat. Rev. Dis. Primers 2017, 3, 17085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phukan, J.; Elamin, M.; Bede, P.; Jordan, N.; Gallagher, L.; Byrne, S.; Lynch, C.; Pender, N.; Hardiman, O. The syndrome of cognitive impairment in amyotrophic lateral sclerosis: A population-based study. J. Neurol. Neurosurg. Psychiatry 2012, 83, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Elamin, M.; Bede, P.; Byrne, S.; Jordan, N.; Gallagher, L.; Wynne, B.; O’Brien, C.; Phukan, J.; Lynch, C.; Pender, N.; et al. Cognitive changes predict functional decline in ALS: A population-based longitudinal study. Neurology 2013, 80, 1590–1597. [Google Scholar] [CrossRef] [PubMed]
- Verma, A. Tale of two diseases: Amyotrophic lateral sclerosis and frontotemporal dementia. Neurol. India 2014, 62, 347–351. [Google Scholar] [CrossRef]
- Brown, R.H.; Al-Chalabi, A. Amyotrophic Lateral Sclerosis. N. Engl. J. Med. 2017, 377, 162–172. [Google Scholar] [CrossRef] [Green Version]
- van Es, M.A.; Hardiman, O.; Chio, A.; Al-Chalabi, A.; Pasterkamp, R.J.; Veldink, J.H.; van den Berg, L.H. Amyotrophic lateral sclerosis. Lancet 2017, 390, 2084–2098. [Google Scholar] [CrossRef]
- Brooks, B.R. El Escorial World Federation of Neurology criteria for the diagnosis of amyotrophic lateral sclerosis. Subcommittee on Motor Neuron Diseases/Amyotrophic Lateral Sclerosis of the World Federation of Neurology Research Group on Neuromuscular Diseases and the El Escorial “Clinical limits of amyotrophic lateral sclerosis” workshop contributors. J. Neurol. Sci. 1994, 124, 96–107. [Google Scholar]
- Arthur, K.C.; Calvo, A.; Price, T.R.; Geiger, J.T.; Chiò, A.; Traynor, B.J. Projected increase in amyotrophic lateral sclerosis from 2015 to 2040. Nat. Commun. 2016, 7, 12408. [Google Scholar] [CrossRef] [Green Version]
- Colletti, T.; Agnello, L.; Spataro, R.; Guccione, L.; Notaro, A.; Lo Sasso, B.; Blandino, V.; Graziano, F.; Gambino, C.M.; Giglio, R.V.; et al. Prognostic Role of CSF β-amyloid 1-42/1-40 Ratio in Patients Affected by Amyotrophic Lateral Sclerosis. Brain Sci. 2021, 11, 302. [Google Scholar] [CrossRef]
- Agnello, L.; Colletti, T.; Lo Sasso, B.; Vidali, M.; Spataro, R.; Gambino, C.M.; Giglio, R.V.; Piccoli, T.; Bivona, G.; La Bella, V.; et al. Tau protein as a diagnostic and prognostic biomarker in amyotrophic lateral sclerosis. Eur. J. Neurol. 2021, 28, 1868–1875. [Google Scholar] [CrossRef] [PubMed]
- Chen-Plotkin, A.S.; Lee, V.M.; Trojanowski, J.Q. TAR DNA-binding protein 43 in neurodegenerative disease. Nat. Rev. Neurol. 2010, 6, 211–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, M.; Sampathu, D.M.; Kwong, L.K.; Truax, A.C.; Micsenyi, M.C.; Chou, T.T.; Bruce, J.; Schuck, T.; Grossman, M.; Clark, C.M.; et al. Ubiquitinated TDP-43 in frontotemporal lobar degeneration and amyotrophic lateral sclerosis. Science 2006, 314, 130–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benajiba, L.; Le Ber, I.; Camuzat, A.; Lacoste, M.; Thomas-Anterion, C.; Couratier, P.; Legallic, S.; Salachas, F.; Hannequin, D.; Decousus, M.; et al. TARDBP mutations in motoneuron disease with frontotemporal lobar degeneration. Ann. Neurol. 2009, 65, 470–473. [Google Scholar] [CrossRef]
- Sephton, C.F.; Good, S.K.; Atkin, S.; Dewey, C.M.; Mayer, P., 3rd; Herz, J.; Yu, G. TDP-43 is a developmentally regulated protein essential for early embryonic development. J. Biol. Chem. 2010, 285, 6826–6834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, A.; Bharathi, V.; Sivalingam, V.; Girdhar, A.; Patel, B.K. Molecular Mechanisms of TDP-43 Misfolding and Pathology in Amyotrophic Lateral Sclerosis. Front. Mol. Neurosci. 2019, 12, 25. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.S.; Cheng, W.C.; Chen, C.Y.; Wu, M.C.; Wang, Y.C.; Tseng, Y.H.; Chuang, T.J.; Shen, C.J. Transcriptomopathies of pre- and post-symptomatic frontotemporal dementia-like mice with TDP-43 depletion in forebrain neurons. Acta Neuropathol. Commun. 2019, 7, 50. [Google Scholar] [CrossRef]
- Riku, Y.; Seilhean, D.; Duyckaerts, C.; Boluda, S.; Iguchi, Y.; Ishigaki, S.; Iwasaki, Y.; Yoshida, M.; Sobue, G.; Katsuno, M. Pathway from TDP-43-Related pathology to neuronal dysfunction in amyotrophic lateral sclerosis and frontotemporal lobar degeneration. Int. J. Mol. Sci 2021, 22, 3843. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Erlbaum Press: Mahwah, NJ, USA, 1988. [Google Scholar]
- Hedges, L.V. Distribution theory for glass’s estimator of effect size and related estimators. J. Educ. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- Viechtbauer, W. Bias and efficiency of meta-analytic variance estimators in the random-effects model. J. Educ. Behav. Stat. 2005, 30, 261–293. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Knapp, G.; Hartung, J. Improved tests for a random effects meta-regression with a single covariate. Stat. Med. 2003, 22, 2693–2710. [Google Scholar] [CrossRef]
- Ren, Y.; Li, S.; Chen, S.; Sun, X.; Yang, F.; Wang, H.; Li, M.; Cui, F.; Huang, X. TDP-43 and phosphorylated TDP-43 levels in paired plasma and CSF samples in amyotrophic lateral sclerosis. Front. Neurol. 2021, 12, 663637. [Google Scholar] [CrossRef] [PubMed]
- Khosla, R.; Rain, M.; Chawathey, S.; Modgil, S.; Tyagi, R.; Thakur, K.; Pannu, V.; Sharma, S.K.; Anand, A. Identifying putative cerebrospinal fluid biomarkers of amyotrophic lateral sclerosis in a north Indian population. Muscle Nerve 2020, 62, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Kasai, T.; Kojima, Y.; Ohmichi, T.; Tatebe, H.; Tsuji, Y.; Noto, Y.I.; Kitani-Morii, F.; Shinomoto, M.; Allsop, D.; Mizuno, T.; et al. Combined use of CSF NfL and CSF TDP-43 improves diagnostic performance in ALS. Ann. Clin. Transl. Neurol. 2019, 6, 2489–2502. [Google Scholar] [CrossRef]
- Bourbouli, M.; Rentzos, M.; Bougea, A.; Zouvelou, V.; Constantinides, V.C.; Zaganas, I.; Evdokimidis, I.; Kapaki, E.; Paraskevas, G.P. Cerebrospinal Fluid TAR DNA-Binding Protein 43 combined with tau proteins as a candidate biomarker for amyotrophic lateral sclerosis and frontotemporal dementia spectrum disorders. Dement. Geriatr. Cogn. Disord. 2017, 44, 144–152. [Google Scholar] [CrossRef]
- Hosokawa, M.; Arai, T.; Yamashita, M.; Tsuji, H.; Nonaka, T.; Masuda-Suzukake, M.; Tamaoka, A.; Hasegawa, M.; Akiyama, H. Differential diagnosis of amyotrophic lateral sclerosis from Guillain-Barré syndrome by quantitative determination of TDP-43 in cerebrospinal fluid. Int. J. Neurosci. 2014, 124, 344–349. [Google Scholar] [CrossRef]
- Noto, Y.; Shibuya, K.; Sato, Y.; Kanai, K.; Misawa, S.; Sawai, S.; Mori, M.; Uchiyama, T.; Isose, S.; Nasu, S.; et al. Elevated CSF TDP-43 levels in amyotrophic lateral sclerosis: Specificity, sensitivity, and a possible prognostic value. Amyotroph. Lateral Scler. 2011, 12, 140–143. [Google Scholar] [CrossRef]
- Kasai, T.; Tokuda, T.; Ishigami, N.; Sasayama, H.; Foulds, P.; Mitchell, D.J.; Mann, D.M.; Allsop, D.; Nakagawa, M. Increased TDP-43 protein in cerebrospinal fluid of patients with amyotrophic lateral sclerosis. Acta Neuropathol. 2009, 117, 55–62. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Chien, H.M.; Lee, C.C.; Huang, J.J. The different faces of the TDP-43 Low-complexity domain: The formation of liquid droplets and amyloid fibrils. Int. J. Mol. Sci. 2021, 22, 8213. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.J.; Mitchell, J.C. Mechanisms of TDP-43 proteinopathy onset and propagation. Int. J. Mol. Sci. 2021, 22, 6004. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Ngo, S.T. Altered TDP-43 structure and function: Key insights into aberrant RNA, mitochondrial, and cellular and systemic metabolism in amyotrophic lateral sclerosis. Metabolites 2022, 12, 709. [Google Scholar] [CrossRef] [PubMed]
- Wobst, H.J.; Delsing, L.; Brandon, N.J.; Moss, S.J. Truncation of the TAR DNA-binding protein 43 is not a prerequisite for cytoplasmic relocalization, and is suppressed by caspase inhibition and by introduction of the A90V sequence variant. PLoS ONE 2017, 12, e0177181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Boer, E.M.J.; Orie, V.K.; Williams, T.; Baker, M.R.; De Oliveira, H.M.; Polvikoski, T.; Silsby, M.; Menon, P.; van den Bos, M.; Halliday, G.M.; et al. TDP-43 proteinopathies: A new wave of neurodegenerative diseases. J. Neurol. Neurosurg. Psychiatry 2020, 92, 86–95. [Google Scholar] [CrossRef]
- Keszycki, R.; Jamshidi, P.; Kawles, A.; Minogue, G.; Flanagan, M.E.; Zaccard, C.R.; Mesulam, M.M.; Gefen, T.; Geula, C. Propagation of TDP-43 proteinopathy in neurodegenerative disorders. Neural. Regen. Res. 2022, 17, 1498–1500. [Google Scholar] [PubMed]
- Agnello, L.; Gambino, C.M.; Lo Sasso, B.; Bivona, G.; Milano, S.; Ciaccio, A.M.; Piccoli, T.; La Bella, V.; Ciaccio, M. Neurogranin as a Novel Biomarker in Alzheimer’s Disease. Lab. Med. 2021, 52, 188–196. [Google Scholar] [CrossRef]
- Piccoli, T.; Blandino, V.; Maniscalco, L.; Matranga, D.; Graziano, F.; Guajana, F.; Agnello, L.; Lo Sasso, B.; Gambino, C.M.; Giglio, R.V.; et al. Biomarkers related to synaptic dysfunction to discriminate alzheimer’s disease from other neurological disorders. Int. J. Mol. Sci. 2022, 23, 10831. [Google Scholar] [CrossRef]
- Agnello, L.; Lo Sasso, B.; Vidali, M.; Scazzone, C.; Gambino, C.M.; Piccoli, T.; Bivona, G.; Ciaccio, A.M.; Giglio, R.V.; La Bella, V.; et al. Evaluation of Alpha-Synuclein Cerebrospinal Fluid Levels in Several Neurological Disorders. J. Clin. Med. 2022, 11, 3139. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year | Study Setting | Study Population | Mean Age (Years) | Male/Female | Disease Duration (Months) | ALSFRS-R | Sample | Analytical Method | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | ALS | ALS | Controls | ALS | Controls | ||||||
| Ren et al., 2021 [25] | China | 128 | 69 | 51.46 (34–69) | 51.76 (23–76) | 46/23 | 37/22 | 19.59 (3–60) | 37.91 (18.47) | Plasma and CSF | ELISA |
| Khosla et al., 2020 [26] | India | 86 | 54 | 48.01 ± 12.24 | 38.12 ± 16.43 | 43/10 | 28/4 | 19.34 | 34.37 ± 6.17 | CSF | ELISA |
| Kasai et al., 2019 [27] | Japan | 53 | 29 | 65.41 ± 12.34 | 66.40 ± 9.2 | 18/11 | 19/10 | NA | NA | Plasma and CSF | Simoa assay |
| Bourbouli et al., 2017 [28] | Greece | 49 | 32 | 61.4 ± 9.47 | 59.7 ± 10.2 | 17/15 | 30/21 | 15.24 ± 11.4 | 43 (42–46) | CSF | ELISA |
| Hosakawa et al., 2014 [29] | Japan | 20 | 13 | 58.9 ± 15.65 | 48.8 ± 21.58 | 7/6 | 5/2 | 21 ± 26.7 | NA | CSF | ELISA |
| Noto et al., 2011 [30] | Japan | 77 | 27 | NA | NA | NA | NA | NA | NA | CSF | ELISA |
| Kasai et al., 2009 [31] | Japan | 59 | 30 | NA | NA | 19/11 | NA | 14.9 ± 10.6 | NA | CSF | ELISA |
| Author, Year | Representative Spectrum | Acceptable Reference Standard | Acceptable Delay between Tests | Partial Verification Avoided | Differential Verification Avoided | Incorporation Avoided | Reference Standard Results Blinded | Index Test Results Blinded | Uninterpretable Results Reported | Withdrawals Explained | Sponsoring Precluded |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ren et al., 2021 | YES | YES | YES | YES | YES | YES | YES | YES | NO | YES | UNCLEAR |
| Khosla et al., 2020 | YES | YES | YES | YES | YES | YES | NO | UNCLEAR | NO | YES | UNCLEAR |
| Kasai et al., 2019 | YES | UNCLEAR | UNCLEAR | YES | YES | YES | NO | NO | NO | UNCLEAR | YES |
| Bourbouli et al., 2017 | YES | YES | YES | YES | YES | YES | YES | YES | NO | YES | YES |
| Hosakawa et al., 2014 | YES | YES | YES | YES | YES | YES | NO | NO | NO | YES | YES |
| Verstraete et al., 2012 | YES | YES | YES | YES | YES | YES | NO | NO | NO | YES | YES |
| Noto et al., 2011 | YES | YES | YES | YES | YES | YES | NO | NO | NO | YES | YES |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gambino, C.M.; Ciaccio, A.M.; Lo Sasso, B.; Giglio, R.V.; Vidali, M.; Agnello, L.; Ciaccio, M. The Role of TAR DNA Binding Protein 43 (TDP-43) as a CandiDate Biomarker of Amyotrophic Lateral Sclerosis: A Systematic Review and Meta-Analysis. Diagnostics 2023, 13, 416. https://doi.org/10.3390/diagnostics13030416
Gambino CM, Ciaccio AM, Lo Sasso B, Giglio RV, Vidali M, Agnello L, Ciaccio M. The Role of TAR DNA Binding Protein 43 (TDP-43) as a CandiDate Biomarker of Amyotrophic Lateral Sclerosis: A Systematic Review and Meta-Analysis. Diagnostics. 2023; 13(3):416. https://doi.org/10.3390/diagnostics13030416
Chicago/Turabian StyleGambino, Caterina Maria, Anna Maria Ciaccio, Bruna Lo Sasso, Rosaria Vincenza Giglio, Matteo Vidali, Luisa Agnello, and Marcello Ciaccio. 2023. "The Role of TAR DNA Binding Protein 43 (TDP-43) as a CandiDate Biomarker of Amyotrophic Lateral Sclerosis: A Systematic Review and Meta-Analysis" Diagnostics 13, no. 3: 416. https://doi.org/10.3390/diagnostics13030416