
Screening for Liver Fibrosis in the General Population: Where Do We Stand in 2022?

1
Service d’Hépato-Gastroentérologie et Oncologie Digestive, Centre Hospitalier Universitaire d’Angers, 49100 Angers, France
2
Laboratoire HIFIH, UPRES EA3859, SFR 4208, Université d’Angers, 49035 Angers, France
*
Author to whom correspondence should be addressed.
Diagnostics 2023, 13(1), 91; https://doi.org/10.3390/diagnostics13010091
Submission received: 17 November 2022
/
Revised: 19 December 2022
/
Accepted: 20 December 2022
/
Published: 28 December 2022
(This article belongs to the Special Issue Recent Advances in Liver Diseases Diagnosis)
Abstract
:Approximately 30% of the worldwide population has at least one risk factor for liver disease. Identifying advanced liver disease before the occurrence of complications remains a difficult challenge in clinical practice, where diagnosis comes too late for many patients, at the time of liver decompensation or palliative hepatocellular carcinoma, with poor short-term prognosis. Noninvasive, blood- or elastography-based tests of liver fibrosis (NITs) have been developed for the early diagnosis of advanced liver fibrosis. Recent population-based studies evaluating the screening of liver fibrosis with these NITs have provided important information on at-risk groups that should be targeted. New measures based on the sequential use of NITs help to better organize the referral of at-risk patients to the liver specialist. However, energizing these measures will require increased awareness of both chronic liver diseases and the use of NITs among non-specialists.
1. Introduction
Chronic liver diseases have become a growing health burden [1,2]. Approximately 25% of the worldwide population is currently living with non-alcoholic fatty liver disease (NAFLD), 1.2% with alcohol use disorders (AUDs), 3.5% with chronic hepatitis B, and 1% with hepatitis C [3,4,5]. Liver fibrosis is the main prognostic factor in chronic liver diseases and longitudinal studies have shown that patient morbidity and mortality were significantly increased in patients with advanced liver fibrosis, i.e., septal fibrosis on liver biopsy [6,7,8]. Patients with chronic liver diseases often have no symptoms, normal physical examinations, and non-specific biological abnormalities. Indeed, only a minority of them will develop advanced liver fibrosis and thus their identification in clinical practice is a challenge for physicians. Consequently, chronic liver diseases are often diagnosed far too belatedly, when the patient’s medium-term prognosis has already become poor. At the time of diagnosis, 75% of cirrhosis cases are already decompensated and 78% of hepatocellular carcinoma cases are at the palliative stage [9,10]. Today, in their quest to identify cases of advanced fibrosis, physicians have at their disposal a range of blood or elastography-based tests able to assess liver fibrosis noninvasively [11]. In this review, we aim to present the current state of screening for advanced liver fibrosis. Thereto, we will attempt to address several questions: Which approach (mass or targeted) should be preferred for the screening of advanced liver fibrosis? Which tests could be relevant for it? What would be the ideal patient pathway? Finally, are non-specialists aware of chronic liver diseases and willing to participate in screening?
2. Mass Versus Targeted Screening
Several studies have evaluated screening for advanced liver fibrosis in the general population (Table 1) [12,13,14,15,16,17]. Almost all of them included large samples of unselected patients and evaluated advanced fibrosis with vibration-controlled transient elastography (VCTE) at a threshold of 8.0 kPa, as it provides 90% sensitivity for the diagnosis of advanced liver fibrosis [18]. The prevalence of advanced fibrosis was, overall, similar between the studies at about 5–7%. Moreover, in multivariate analyses, these studies reported the same main factors associated with advanced liver fibrosis: diabetes, other metabolic risk factors (obesity, low high-density lipoprotein cholesterol, high triglycerides, and the presence of metabolic syndrome), excessive alcohol use, and elevated liver enzymes [12,13,14,15,16,19,20].
2.1. Type 2 Diabetes Mellitus
Demonstrating the importance of this liver risk factor (Table 1), type 2 diabetes mellitus (T2DM) was consistently associated with an increased risk of advanced liver fibrosis in the general population. In the Rotterdam study, the prevalence of T2DM was 9.8% in patients with VCTE <8 kPa but reached 33.7% in those with VCTE ≥8 kPa [15]. Specific studies in T2DM patients from community-based populations and patients not under insulin therapy showed a 7–10% prevalence of advanced fibrosis as evaluated by VCTE (≥9.6 kPa) [21,22]. In tertiary care centers, the prevalence of advanced liver fibrosis, as evaluated by that same VCTE threshold, increased to 17–21% [23,24,25,26,27]. Some studies have suggested that T2DM severity and duration were associated with a higher risk of advanced fibrosis [25,28]. Kwok et al. found that T2DM patients with VCTE ≥9.6 kPa had a longer duration of diabetes as compared to patients with T2DM and VCTE <9.6 kPa [25]. Another study found that every 1% increase in glycated hemoglobin, measured at the time of liver biopsy, was associated with 15% higher odds of increased fibrosis stage [29]. These findings are helpful for refining subpopulations of interest within the larger T2DM population.
Large studies focusing on hard endpoints have confirmed the strong link between T2DM and liver-related complications. The increased risk of death from cancer in diabetics compared to non-diabetics is the highest for liver cancer, while chronic liver diseases account for the third-highest increase in the risk of death from non-cancer and non-vascular disease [30]. For all these reasons, both the American Diabetes Association (ADA) and the European Associations for the Study of Diabetes (EASD), of the Liver (EASL) and of Obesity (EASO) recommend screening for advanced liver fibrosis in all T2DM patients [31,32].
2.2. Factors Related to Metabolic Conditions
In patients with metabolic risk factors, T2DM, obesity and the presence of metabolic syndrome have been shown to be the key features associated with VCTE >7 kPa (Table 1) [33,34,35,36]. An independent association between VCTE ≥8.2 kPa and obesity or diabetes has also been reported in the community-based Framingham Heart Study [34]. In this work, elevated liver stiffness was also independently associated with other cardiovascular risk factors, including metabolic syndrome, hypertension, and low high-density lipoprotein cholesterol. The concurrency of several metabolic risk factors acts synergically on the risk of advanced liver fibrosis. For example, in 3076 patients from the general Spanish population, the prevalence of VCTE >9.2 kPa was only 0.4% in patients without risk factors but it grew to 5.0% in those with ≥1 risk factor (among obesity, T2DM, hyperlipidemia, hypertension, metabolic syndrome or alcohol consumption) [14]. In 890 patients from Sicily, the prevalences of VCTE ≥9.6 kPa in patients without risk factors, with genetic risk factors, with T2DM, and with T2DM + genetic risk factors were 3.7%, 7.7%, 11%, and 36%, respectively [37].
2.3. Alcohol Use Disorders
Caballeria et al. showed that the prevalence of VCTE ≥8 kPa was 10.3% in subjects with alcohol use disorders (AUD) (>14 units/week (U/w) for women and >21 U/w for men) compared to 5% in patients without [14]. In a specific study on patients referred from primary care with alcohol consumption >14 U/w, advanced liver fibrosis was independently associated with increasing units of alcohol consumed. In that study, there was a five-fold increase in the risk of developing advanced fibrosis in patients who drank >100 U/w compared to those who drink <35 U/w [38]. Moreover, a longitudinal study in a Swedish population-based cohort with biopsy-proven alcohol-related liver disease found a two-fold increase in the risk of mortality and a very high risk of liver-related death compared to individuals without liver disease [39]. These results should encourage physicians to systematically assess alcohol consumption during patient consultations.
The combination of AUD and metabolic factors has been shown to synergically increase the risk of advanced liver fibrosis [40,41,42]. In a study on primary care patients with AUD and/or T2DM and/or obesity, the prevalence of elevated VCTE was 8.9% in obese patients, 10.8% in T2DM, 36.7% in patients having both obesity and T2DM, and 44% in patients with obesity, T2DM and AUD [36]. Furthermore, a study on NAFLD patients in a tertiary center showed that alcohol consumption >7 U/w was associated with higher overall morbidity, and furthermore that the presence of metabolic syndrome in AUD patients was associated with 27% and 47% increases in overall and liver mortalities, respectively [43].
2.4. Elevated Liver Enzymes
As expected, elevated liver enzymes (transaminases) are associated with advanced liver fibrosis (Table 1). In Caballeria’s study, aspartate aminotransferase (AST) and/or alanine aminotransferase (ALT) ≥40 IU/L were associated with a two-fold increased risk of VCTE ≥8 kPa independently of T2DM, obesity and dyslipidemia [14]. Furthermore, a 10-point increase in ALT values has been shown to be associated with a 10% increased risk of elevated liver stiffness measurement [16]. In a study on 190 apparently healthy subjects who underwent a medical health check-up, advanced liver fibrosis was observed in 11.5% of the subjects with ALT ≥19 IU/L but only in 2.5% of those with ALT <19 IU/L [17]. However, it is important to underline that liver enzymes offered only low sensitivity, as 43% of the patients with advanced liver fibrosis had normal AST and ALT values, and only 4.2% of subjects with abnormal AST/ALT had liver stiffness measurement <8 kPa [12].
In summary, screening studies performed in the general population have identified the key risk factors of advanced fibrosis. Specific studies have further confirmed the increased prevalence of advanced fibrosis in populations with those key liver risk factors, giving a rationale for a targeted rather than mass screening approach for advanced liver fibrosis.
3. What Do the Guidelines Say about Screening for Advanced Liver Fibrosis?
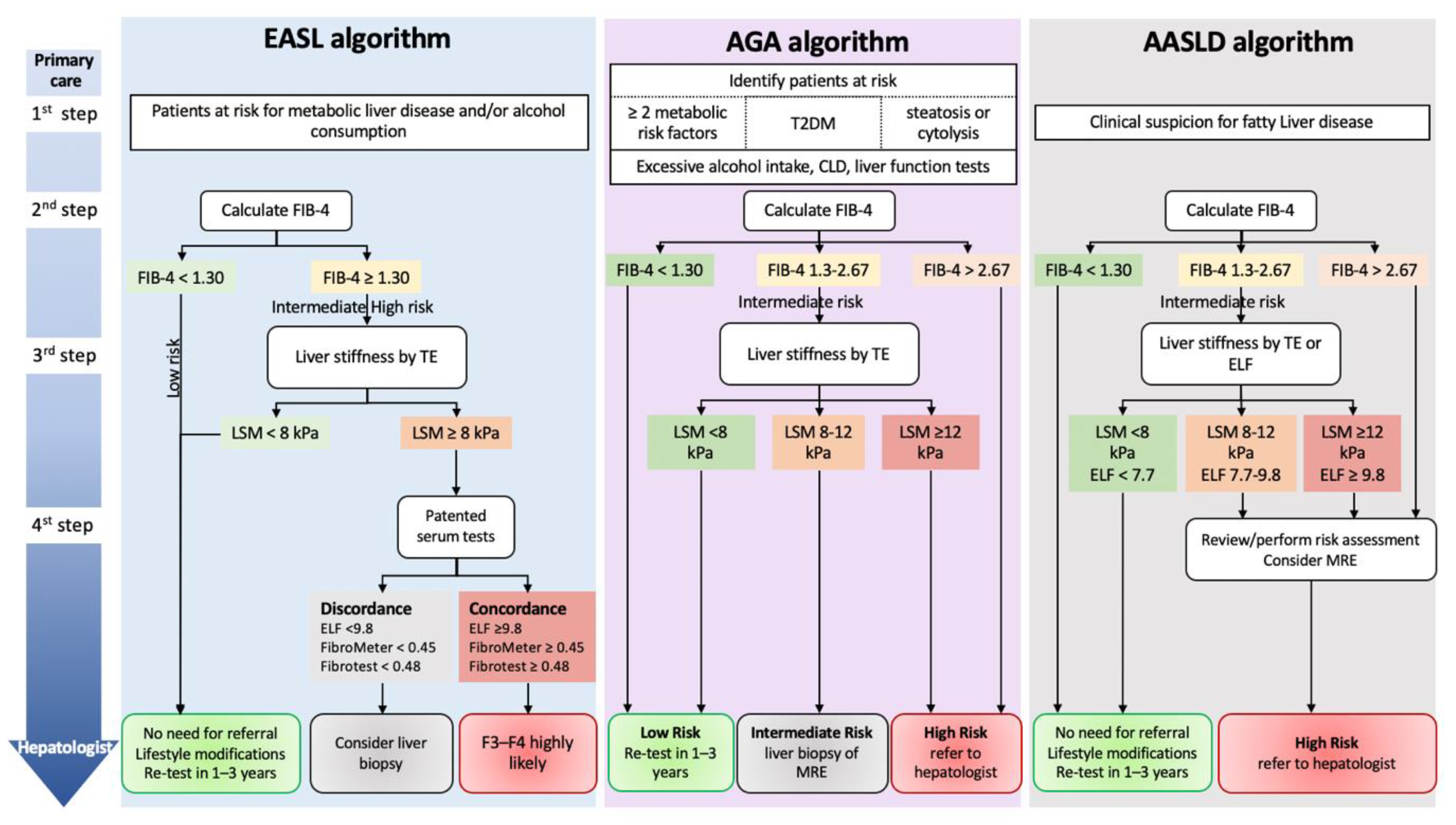
Since 2016, the EASD, EASL, and EASO recommend liver fibrosis screening in patients with T2DM [31]. In its 2021 guidelines, EASL extended the screening to populations with risk factors for liver diseases (Figure 1) [11]. In 2018, the American Association for the Study of Liver Diseases (AASLD) did not recommend the routine screening for NAFLD in high-risk groups because of uncertainties surrounding diagnostic tests and treatment options, along with a lack of knowledge related to long-term benefits and cost-effectiveness of screening [44]. In its last meeting held in November 2022, the AASLD presented its new practice guidelines and now recommends screening for liver fibrosis in case of clinical suspicion of fatty liver disease (Figure 1) [unpublished]. In their collaborative 2021 guidelines, both the American Gastroenterology Association (AGA) and the American Diabetes Association (ADA) recommend the screening of liver fibrosis in at-risk patients because a timely diagnosis of fibrosis can prevent progression to complications (Figure 1) [45].
4. Tools for Screening
A liver biopsy is the gold standard for the assessment of liver fibrosis. However, it is an invasive procedure associated with severe complications in 1–3% of cases and a mortality rate of approximately 1 in 10,000 [46,47]. Because of those aspects, not to mention the high cost of the procedure and the large population to be screened, it becomes clear that noninvasive, repeatable, and ideally cheaper alternatives for the assessment of liver fibrosis are highly desirable—and currently available. These noninvasive alternatives exist mainly in the form of blood-based tests (“functional” methods) or radiology-based techniques using elastography (“physical” methods) [11]. Blood tests include either direct or indirect markers of liver fibrosis, the former reflecting impaired liver function with increasing fibrosis levels, and the latter proteins directly linked to the process of liver fibrogenesis and fibrolysis. Blood tests have the advantages of good reproducibility and potentially extensive availability as they can be prescribed by any physician (Table 2). “Simple” blood tests combine indirect biomarkers of fibrosis, cost nothing (except lab work), and involve only easy calculations via smartphone applications [48]. “Specialized” blood tests combine both direct and indirect biomarkers of fibrosis and do incur usually unreimbursed costs, but they provide better accuracy than simple blood tests [49,50,51,52,53].
There are still controversies about whether non-invasive tests, such as blood-based tests and imaging tests could be complete substitutes for pathology tests by liver biopsy. Even if it remains currently the reference for the evaluation of liver lesions, liver biopsy is impaired by sampling variability and suboptimal inter-observed reproducibility between pathologists, which makes this method not a Gold Standard [54,55]. For this reason, it is not possible to assess the true diagnostic accuracy of NITs in cross-sectional diagnostic studies [56,57]. Nevertheless, diagnostic studies have attracted great interest by demonstrating that NITs are well calibrated on liver fibrosis, the main determinant of the liver-related prognosis in NAFLD. Now, the key challenge is to demonstrate that NITs can accurately stratify the risk of liver-related complications in NAFLD as do the histological stages of liver fibrosis. Such achievement will definitely allow the shift from biopsy to management based on NITs results. Prognostic studies performed in the general population and in patients from tertiary care centers have recently shown the good prognostic accuracy of NITs with results comparable to that of liver biopsy [58,59,60,61,62,63]. In addition, as compared to liver biopsy, NITs can be more easily repeated during follow-up and their evolution allows for a more refined assessment of the prognosis of patients [64].
5. Simple Blood Tests
5.1. FIB-4
Fibrosis-4 (FIB-4) is a simple blood fibrosis test based on AST, ALT, platelets, and age [65]. In tertiary care, values below its low threshold (1.30) exclude advanced fibrosis with a negative predictive value of >90% and good sensitivity [66,67,68,69]. However, values at or exceeding its high threshold (2.67), with a positive predictive value of around 60–70%, are not sufficiently accurate to confirm advanced fibrosis [69,70,71]. Furthermore, about 30% of patients will have FIB-4 scores in the “grey zone” between the low and high thresholds, where no conclusions can be drawn regarding the diagnosis of advanced liver fibrosis [65,69,70]. Therefore, in these two latter situations (≥high threshold and grey zone scores), a second-line confirmation is mandatory.
5.2. NFS
The NAFLD-Fibrosis Score (NFS) is a simple blood test specific to NAFLD. Its calculation requires hyperglycemia, age, body-mass index, AST, ALT, platelet count, and albumin [72]. As with FIB-4, NFS scores ≤1.455 (low threshold) exclude advanced fibrosis with a negative predictive value >90% [69,70] but those ≥0.676 (high threshold), with PPVs at 20–40% in a low prevalence setting, lack sufficient accuracy to rule in advanced fibrosis [70]. NFS too has a grey zone between its low and high thresholds into which 30% of patients fall [72]. Therefore, a second-line confirmatory test for NFS scores ≥0.676 or in the grey zone appears to be the most suitable strategy [11]. Importantly, because the variable “hyperglycemia” weighs heavily in the calculation of the score and when looking to identify advanced fibrosis in the T2DM setting, there is a very low rate of patients under the low threshold: 30% in primary care and 3–13% in diabetes clinics [73,74,75]. Consequently, NFS should not be used for the screening of advanced fibrosis in T2DM patients.
6. Specialized Test
6.1. Elastography-Based Techniques
VCTE with Fibroscan (Echosens, Paris, France) was the first of the various elastography techniques available today and continues to have the most available data [66,76,77]. VCTE quantifies the speed of a mechanically induced shear wave in liver tissue and calculates liver stiffness from it [78]. Several studies have shown that liver stiffness correlates well with the degree of liver fibrosis in chronic liver diseases and especially in NAFLD [52,76]. In direct comparisons, the accuracy of VCTE has been shown to be higher than those of simple and specialized blood tests [52]. In recent studies from over 5,000 biopsy-proven NAFLD patients, VCTE <7–8 kPa had very good, 85%, sensitivity, and VCTE >12 kPa provided 90% specificity for diagnosing advanced fibrosis [18,70]. These results suggest that VCTE is a viable second-line option after simple tests [11,31].
Other elastography-based techniques coupled with ultrasound, such as point shear wave elastography and two-dimensional shear wave elastography, are now available (Table 2). Because these devices are readily available in radiology practices, they represent an interesting option to increase the availability of liver elastography in the context of screening. These techniques are as accurate as VCTE for the diagnosis of advanced fibrosis [76,79,80,81,82,83,84]. However, the consensus remains to be reached on thresholds for disease risk stratification in relation to histology, and reliability criteria await validation [85,86]. Finally, magnetic resonance elastography, based on magnetic resonance imaging, is the most accurate technique for staging liver fibrosis but its use is restricted to clinical research because of its limited availability and high cost [76,87].
6.2. Specialized Blood Test
The three most-validated specialized blood tests are the Enhanced Liver Fibrosis (ELF) test, FibroMeter, and Fibrotest. ELF is a panel of three direct markers of fibrosis: type III procollagen peptide, hyaluronate, and tissue inhibitor of metalloproteinase-1 [88,89]. FibroMeter is based on age, sex, AST, platelets, prothrombin time, urea, hyaluronate, and α2-macroglobulin [90], and Fibrotest on age, sex, glutamyl gamma transferase, alpha-2 macroglobulin, haptoglobin, apolipoprotein A1 and bilirubin [54]. Diagnostic studies using liver biopsy as a reference have demonstrated good rule-out sensitivity (80–90%) and good rule-in specificity (90–95%) of these NITs for the diagnosis of advanced liver fibrosis in chronic liver diseases [49,51,71,91,92]. Because these specialized blood tests include more expensive blood markers, they are best reserved for second-line evaluations of liver fibrosis, as recently proposed [93].
7. Referral Pathways with Algorithms
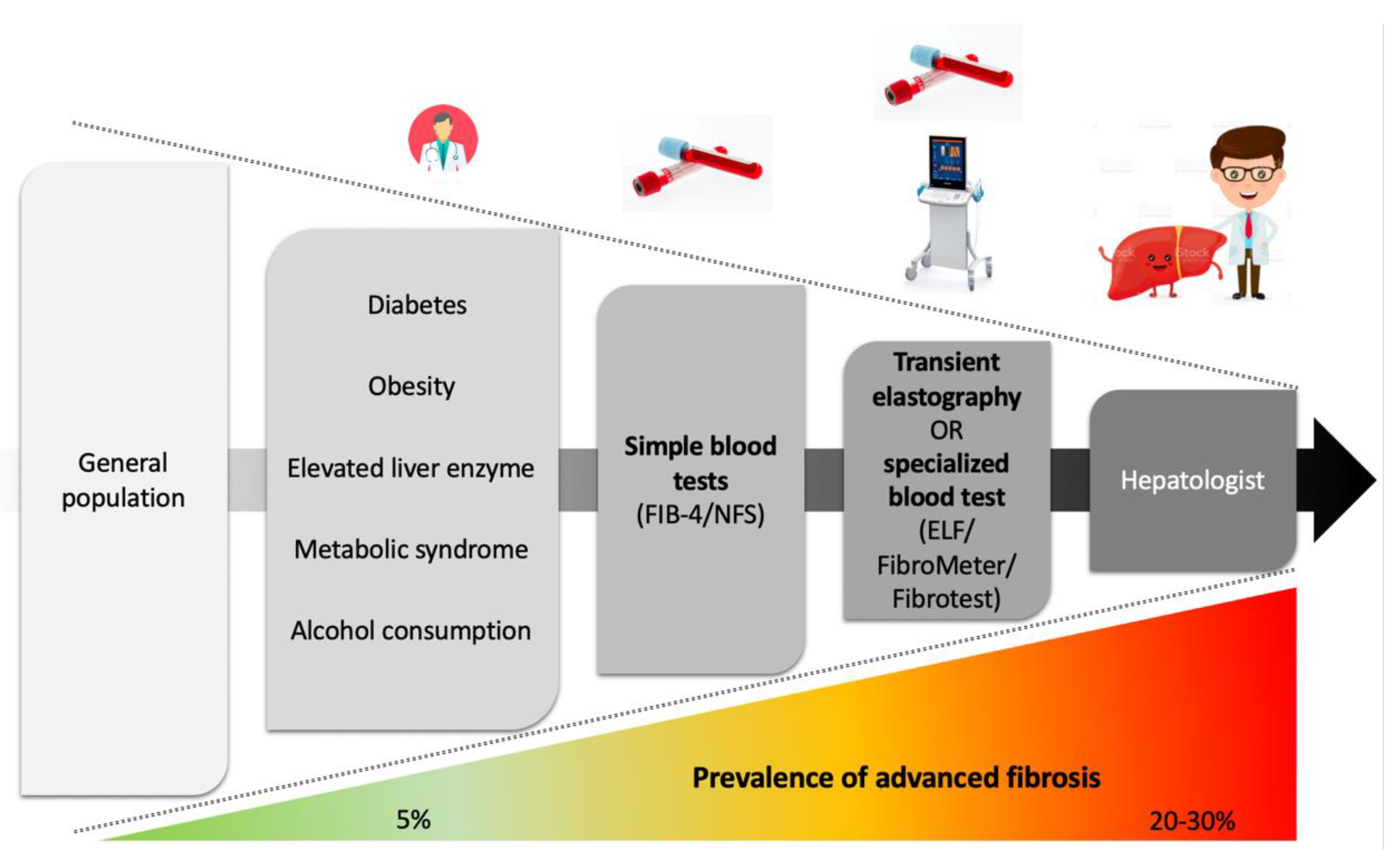
NITs have complementary advantages (Table 2). They offer the potential to identify, among the many patients with liver risk factors, those who have developed advanced liver disease and therefore require specialized management. As combined NITs give better results than single ones [94], the patient pathway must be built upon an initial simple test followed by a specialized test to optimize the identification of patients with advanced liver fibrosis (Figure 2) [11,45,93,95,96,97,98,99].
Patients with risk factors for chronic liver diseases (type 2 diabetes mellitus, obesity, metabolic syndrome, elevated liver enzymes, and alcohol consumption) seen in primary care should undergo testing by a simple blood test (FIB-4 or NFS), followed, if positive, by transient elastography or a specialized blood test (ELF, FibroMeter or Fibrotest) before being referred to a liver specialist.
ELF: enhanced liver fibrosis; FIB-4: Fibrosis-4; NFS: NAFLD fibrosis score
8. Algorithms in Primary Care
Srivastava et al. evaluated a two-step pathway based on FIB-4 and ELF in new NAFLD patients from primary care. Patients with FIB-4 <1.30 were deemed to be at low risk of advanced fibrosis and remained in primary care. Patients with FIB-4 >3.25 were considered to be at high risk of advanced fibrosis and recommended for referral to secondary care. Patients with FIB-4 in the grey zone had an ELF test (used with the 9.8 threshold) to determine the risk of advanced fibrosis. It should be noted that very few studies have used the 3.25 rule-in threshold (coming from HIV-HCV co-infection [65]) and that international guidelines uniformly propose to use FIB-4 with its 1.30 rule-out and 2.67 rule-in thresholds adapted for NAFLD [67]. Compared to standard care, the pathway proposed by Srivastava et al. resulted in an 81% reduction in unnecessary referrals and improved the identification of patients with advanced fibrosis and cirrhosis [93]. In a Canadian study, Davyduke et al. evaluated an algorithm combining FIB-4 with a threshold of 1.30 and VCTE with a threshold of 8.0 kPa. Of the 597 patients included from primary care with steatosis on ultrasound or elevated ALT, only 4% had FIB-4 ≥1.30 and VCTE ≥8 kPa, demonstrating a significant reduction in the number of patients requiring referral to a liver specialist [98]. Mansour et al. evaluated the FIB-4/VCTE algorithm in 467 T2DM patients from primary care. Among the 85/467 patients with raised FIB-4, 38/58 had a VCTE ≥8 kPa, and 20 were found to have advanced fibrosis (4.5%). Alcohol use (particularly drinking >14/21 U/w) and body-mass index were predictors of advanced liver fibrosis in that study [99]. Cost-effectiveness studies have confirmed that these pathways do reduce costs compared to a refer-all strategy [100,101]. Nevertheless, although such pathways have been widely studied in at-risk patients [11,45,95,96,97], their sequential use in primary care has received little attention [93,98,99]. Additionally, cost-effectiveness analyses have been performed only in the United Kingdom and Italy; similar studies should be encouraged in other countries to validate these results [100,101].
9. What Do the Guidelines Say about Referral Pathways Based on Noninvasive Tests?
The EASL and the AGA recommend evaluation of liver fibrosis in patients with AUD or metabolic cofactors (Figure 1) [11,45]. In its last meeting held in November 2022, the AASLD also presented its practice guidelines with an algorithm for liver fibrosis assessment in patients with suspected fatty liver disease [not published] (Figure 1). All three algorithms from EASL, AGA, and AASLD propose as a first step the identification of liver risk factors (alcohol and metabolic disorders). Further steps rely on NITs with first the simple blood test FIB-4 eventually followed by liver stiffness measurement with VCTE and/or a specialized blood test. The thresholds for the different tests used are similar between the three algorithms (Figure 1).
10. Awareness of Chronic Liver Diseases
Due to the large population of patients at risk of chronic liver diseases, general practitioners (GPs) and other non-liver specialists need to play a major role in the early diagnosis of advanced liver disease.
However, several studies have reported that GPs have little awareness of chronic liver diseases [102,103,104,105,106]. In a survey sent to 64 GPs, Van Asten et al. showed that the acronyms NAFLD and NASH were not known by, respectively, 34% and 53% of the respondents and that 96% of them never or rarely screened for the corresponding pathologies [107]. Other studies have shown that GPs were often unaware of the existence of NITs (25%) [105] and unsure whether VCTE (36.3%), NFS/FIB-4 (43.1%), or ELF (56.9%) could help monitor disease progression [102]. In a Dutch survey, NITs were never (73%) or rarely (22%) used by GPs to evaluate disease severity [102,107]. Therefore, most patients diagnosed with a risk factor for chronic liver disease are referred to a liver specialist because of non-specific liver enzyme abnormalities rather than abnormal NITs suggesting advanced liver fibrosis [102,107]. Interestingly, however, after a brief explanation of the simple NITs, almost all physicians expressed a willingness to use them in practice [105].
Low awareness is not limited to GPs. A retrospective analysis of the French hospitalizations database found a very low 0.4% prevalence of the NAFLD/NASH diagnosis code among 50 million adult patients [108]. A questionnaire sent to non-liver specialists in two tertiary hospitals in Brisbane (Australia) showed that the respondents were aware of the association of NAFLD with cardiovascular risk factors (90%) and that of NASH with increased overall mortality, but 71% of them did not refer patients to hepatology if NAFLD was suspected [109]. In a survey sent to 133 British diabetologists, only 5.7% had used or would use a noninvasive algorithm to assess the severity of NAFLD [110]. Another survey of 178 French diabetologists showed that 59% of them underestimated the prevalence of chronic liver diseases. Although 97% of the diabetologists were familiar with NITS, only 29% of them cited FIB-4 [105].
Patients themselves have little awareness of chronic liver diseases. In a study performed in the United States that included more than 10,000 adults from the National Health and Nutrition Examination Survey, 96%, 66%, and 44% of adults with, respectively, NAFLD, hepatitis B or C were unaware they had liver disease [111,112]. A survey among the Turkish community in the Netherlands, wherein hepatitis B is an important health problem, revealed nonetheless a low level of awareness of that pathology [113]. Interestingly, an international cross-sectional survey of 1,411 NAFLD patients recently showed that patients who knew their fibrosis stage were more compliant with lifestyle management [114].
Finally, a survey of European experts to gather information on policies, clinical guidelines, awareness, and monitoring, coupled with data extracted from official documents, revealed a general lack of national policies and awareness campaigns on NAFLD [115]. All these results demonstrate the urgent need for hepatology associations to actively raise awareness of chronic liver diseases and alert authorities as to the weight these pathologies have on current and future public health.
11. Conclusions
Despite the extensive prevalence of chronic liver diseases in the general population, only a small proportion of patients are diagnosed with advanced fibrosis. Patient pathways based on the sequential use of NITs have been proposed in recent years to optimize healthcare systems and improve the identification of patients with advanced fibrosis. These new approaches require the active participation of GPs and other non-liver specialists and the involvement of public authorities to further energize their use.
Author Contributions
Conceptualization, C.M.C. and J.B.; writing—original draft preparation, C.M.C. and J.B.; writing—review and editing, C.M.C. and J.B.; supervision, J.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
J.B. reports consulting activities with Echosens. C.M.C reports no conflict of interest.
Abbreviations
ALT: alanine aminotransferase; AST: aspartate aminotransferase; AUD: alcohol-use disorder; ELF: Enhanced Liver Fibrosis; FIB-4: Fibrosis-4; GP: general practitioner; NAFLD: non-alcoholic fatty liver disease; NFS: NAFLD-Fibrosis Score; NIT: noninvasive test; VCTE: vibration controlled transient elastography; T2DM: type 2 diabetes mellitus; U/w: units/week.
References
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, Regional, and National Age-Sex-Specific Mortality for 282 Causes of Death in 195 Countries and Territories, 1980–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2017 Cirrhosis Collaborators The Global, Regional, and National Burden of Cirrhosis by Cause in 195 Countries and Territories, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol 2020, 5, 245–266. [CrossRef] [PubMed] [Green Version]
- Younossi, Z.; Tacke, F.; Arrese, M.; Chander Sharma, B.; Mostafa, I.; Bugianesi, E.; Wai-Sun Wong, V.; Yilmaz, Y.; George, J.; Fan, J.; et al. Global Perspectives on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis: Hepatology. Hepatology 2019, 69, 2672–2682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, A.M.; Singal, A.G.; Tapper, E.B. Contemporary Epidemiology of Chronic Liver Disease and Cirrhosis. Clin. Gastroenterol. Hepatol. 2020, 18, 2650–2666. [Google Scholar] [CrossRef] [PubMed]
- Asrani, S.K.; Devarbhavi, H.; Eaton, J.; Kamath, P.S. Burden of Liver Diseases in the World. J. Hepatol. 2019, 70, 151–171. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Taylor, R.J.; Bayliss, S.; Hagström, H.; Nasr, P.; Schattenberg, J.M.; Ishigami, M.; Toyoda, H.; Wai-Sun Wong, V.; Peleg, N.; et al. Association Between Fibrosis Stage and Outcomes of Patients With Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Gastroenterology 2020, 158, 1611–1625.e12. [Google Scholar] [CrossRef] [Green Version]
- Sanyal, A.J.; Van Natta, M.L.; Clark, J.; Neuschwander-Tetri, B.A.; Diehl, A.; Dasarathy, S.; Loomba, R.; Chalasani, N.; Kowdley, K.; Hameed, B.; et al. Prospective Study of Outcomes in Adults with Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2021, 385, 1559–1569. [Google Scholar] [CrossRef]
- Lackner, C.; Stauber, R.E.; Davies, S.; Denk, H.; Dienes, H.P.; Gnemmi, V.; Guido, M.; Miquel, R.; Paradis, V.; Schirmacher, P.; et al. Development and Prognostic Relevance of a Histologic Grading and Staging System for Alcohol-Related Liver Disease. J. Hepatol. 2021, 75, 810–819. [Google Scholar] [CrossRef]
- Fialla, A.D.; de Muckadell, O.B.S.; Touborg Lassen, A. Incidence, Etiology and Mortality of Cirrhosis: A Population-Based Cohort Study. Scand. J. Gastroenterol. 2012, 47, 702–709. [Google Scholar] [CrossRef]
- Goutté, N.; Sogni, P.; Bendersky, N.; Barbare, J.C.; Falissard, B.; Farges, O. Geographical Variations in Incidence, Management and Survival of Hepatocellular Carcinoma in a Western Country. J. Hepatol. 2017, 66, 537–544. [Google Scholar] [CrossRef]
- Berzigotti, A.; Tsochatzis, E.; Boursier, J.; Castera, L.; Cazzagon, N.; Friedrich-Rust, M.; Petta, S.; Thiele, M. EASL Clinical Practice Guidelines on Non-Invasive Tests for Evaluation of Liver Disease Severity and Prognosis—2021 Update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef] [PubMed]
- Roulot, D.; Costes, J.-L.; Buyck, J.-F.; Warzocha, U.; Gambier, N.; Czernichow, S.; Le Clesiau, H.; Beaugrand, M. Transient Elastography as a Screening Tool for Liver Fibrosis and Cirrhosis in a Community-Based Population Aged over 45 Years. Gut 2011, 60, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Fabrellas, N.; Alemany, M.; Urquizu, M.; Bartres, C.; Pera, G.; Juvé, E.; Rodríguez, L.; Torán, P.; Caballería, L. Using Transient Elastography to Detect Chronic Liver Diseases in a Primary Care Nurse Consultancy. Nurs. Res. 2013, 62, 450–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caballería, L.; Pera, G.; Arteaga, I.; Rodríguez, L.; Alumà, A.; Morillas, R.M.; de la Ossa, N.; Díaz, A.; Expósito, C.; Miranda, D.; et al. High Prevalence of Liver Fibrosis Among European Adults With Unknown Liver Disease: A Population-Based Study. Clin. Gastroenterol. Hepatol. 2018, 16, 1138–1145.e5. [Google Scholar] [CrossRef] [Green Version]
- Koehler, E.M.; Plompen, E.P.C.; Schouten, J.N.L.; Hansen, B.E.; Murad, S.D.; Taimr, P.; Leebeek, F.W.G.; Hofman, A.; Stricker, B.H.; Castera, L.; et al. Presence of Diabetes Mellitus and Steatosis Is Associated with Liver Stiffness in a General Population: The Rotterdam Study. Hepatology 2016, 63, 138–147. [Google Scholar] [CrossRef] [Green Version]
- Llop, E.; Iruzubieta, P.; Perelló, C.; Fernández Carrillo, C.; Cabezas, J.; Escudero, M.D.; González, M.; Hernández Conde, M.; Puchades, L.; Arias-Loste, M.T.; et al. High Liver Stiffness Values by Transient Elastography Related to Metabolic Syndrome and Harmful Alcohol Use in a Large Spanish Cohort. United Eur. Gastroenterol. J. 2021, 9, 892–902. [Google Scholar] [CrossRef]
- You, S.C.; Kim, K.J.; Kim, S.U.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Lee, W.J.; Han, K.-H. Factors Associated with Significant Liver Fibrosis Assessed Using Transient Elastography in General Population. World J. Gastroenterol. 2015, 21, 1158–1166. [Google Scholar] [CrossRef]
- Papatheodoridi, M.; Hiriart, J.B.; Lupsor-Platon, M.; Bronte, F.; Boursier, J.; Elshaarawy, O.; Marra, F.; Thiele, M.; Markakis, G.; Payance, A.; et al. Refining the Baveno VI Elastography Criteria for the Definition of Compensated Advanced Chronic Liver Disease. J. Hepatol. 2021, 74, 1109–1116. [Google Scholar] [CrossRef]
- Wong, V.W.-S.; Chu, W.C.-W.; Wong, G.L.-H.; Chan, R.S.-M.; Chim, A.M.-L.; Ong, A.; Yeung, D.K.-W.; Yiu, K.K.-L.; Chu, S.H.-T.; Woo, J.; et al. Prevalence of Non-Alcoholic Fatty Liver Disease and Advanced Fibrosis in Hong Kong Chinese: A Population Study Using Proton-Magnetic Resonance Spectroscopy and Transient Elastography. Gut 2012, 61, 409–415. [Google Scholar] [CrossRef]
- Nah, E.-H.; Cho, S.; Kim, S.; Chu, J.; Kwon, E.; Cho, H.-I. Prevalence of Liver Fibrosis and Associated Risk Factors in the Korean General Population: A Retrospective Cross-Sectional Study. BMJ Open 2021, 11, e046529. [Google Scholar] [CrossRef]
- Roulot, D.; Roudot-Thoraval, F.; NKontchou, G.; Kouacou, N.; Costes, J.-L.; Elourimi, G.; Le Clesiau, H.; Ziol, M.; Beaugrand, M. Concomitant Screening for Liver Fibrosis and Steatosis in French Type 2 Diabetic Patients Using Fibroscan. Liver Int. 2017, 37, 1897–1906. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Turino, T.; Lando, M.G.; Gjini, K.; Byrne, C.D.; Zusi, C.; Ravaioli, F.; Colecchia, A.; Maffeis, C.; Salvagno, G.; et al. Screening for Non-Alcoholic Fatty Liver Disease Using Liver Stiffness Measurement and Its Association with Chronic Kidney Disease and Cardiovascular Complications in Patients with Type 2 Diabetes. Diabetes Metab. 2020, 46, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Ciardullo, S.; Monti, T.; Perseghin, G. High Prevalence of Advanced Liver Fibrosis Assessed by Transient Elastography Among U.S. Adults With Type 2 Diabetes. Diabetes Care 2021, 44, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Lai, L.-L.; Wan Yusoff, W.N.I.; Vethakkan, S.R.; Nik Mustapha, N.R.; Mahadeva, S.; Chan, W.-K. Screening for Non-Alcoholic Fatty Liver Disease in Patients with Type 2 Diabetes Mellitus Using Transient Elastography. J. Gastroenterol. Hepatol. 2019, 34, 1396–1403. [Google Scholar] [CrossRef] [PubMed]
- Kwok, R.; Choi, K.C.; Wong, G.L.-H.; Zhang, Y.; Chan, H.L.-Y.; Luk, A.O.-Y.; Shu, S.S.-T.; Chan, A.W.-H.; Yeung, M.-W.; Chan, J.C.-N.; et al. Screening Diabetic Patients for Non-Alcoholic Fatty Liver Disease with Controlled Attenuation Parameter and Liver Stiffness Measurements: A Prospective Cohort Study. Gut 2016, 65, 1359–1368. [Google Scholar] [CrossRef] [PubMed]
- Sporea, I.; Mare, R.; Popescu, A.; Nistorescu, S.; Baldea, V.; Sirli, R.; Braha, A.; Sima, A.; Timar, R.; Lupusoru, R. Screening for Liver Fibrosis and Steatosis in a Large Cohort of Patients with Type 2 Diabetes Using Vibration Controlled Transient Elastography and Controlled Attenuation Parameter in a Single-Center Real-Life Experience. J. Clin. Med. 2020, 9, 1032. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Anoop, S.; Ansari, I.A.; Prakash, S.; Misra, A. High Prevalence of Hepatic Steatosis and Hepatic Fibrosis in Patients with Type 2 Diabetes Mellitus. Clin. Nutr. ESPEN 2021, 46, 519–526. [Google Scholar] [CrossRef]
- de Lédinghen, V.; Vergniol, J.; Gonzalez, C.; Foucher, J.; Maury, E.; Chemineau, L.; Villars, S.; Gin, H.; Rigalleau, V. Screening for Liver Fibrosis by Using FibroScan® and FibroTest in Patients with Diabetes. Dig. Liver Dis. 2012, 44, 413–418. [Google Scholar] [CrossRef]
- Alexopoulos, A.-S.; Crowley, M.J.; Wang, Y.; Moylan, C.A.; Guy, C.D.; Henao, R.; Piercy, D.L.; Seymour, K.A.; Sudan, R.; Portenier, D.D.; et al. Glycemic Control Predicts Severity of Hepatocyte Ballooning and Hepatic Fibrosis in Nonalcoholic Fatty Liver Disease. Hepatology 2021, 74, 1220–1233. [Google Scholar] [CrossRef]
- Diabetes Mellitus, Fasting Glucose, and Risk of Cause-Specific Death. N. Engl. J. Med. 2011, 364, 829–841. [CrossRef]
- EASL–EASD–EASO Clinical Practice Guidelines for the Management of Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2016, 64, 1388–1402. [CrossRef] [PubMed]
- American Diabetes Association. 4. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S37–S47. [Google Scholar]
- Zhang, X.; Heredia, N.I.; Balakrishnan, M.; Thrift, A.P. Prevalence and Factors Associated with NAFLD Detected by Vibration Controlled Transient Elastography among US Adults: Results from NHANES 2017–2018. PLoS ONE 2021, 16, e0252164. [Google Scholar] [CrossRef] [PubMed]
- Long, M.T.; Zhang, X.; Xu, H.; Liu, C.-T.; Corey, K.E.; Chung, R.T.; Loomba, R.; Benjamin, E.J. Hepatic Fibrosis Associates With Multiple Cardiometabolic Disease Risk Factors: The Framingham Heart Study. Hepatology 2021, 73, 548–559. [Google Scholar] [CrossRef] [PubMed]
- Mikolasevic, I.; Milic, S.; Orlic, L.; Stimac, D.; Franjic, N.; Targher, G. Factors Associated with Significant Liver Steatosis and Fibrosis as Assessed by Transient Elastography in Patients with One or More Components of the Metabolic Syndrome. J. Diabetes Its Complicat. 2016, 30, 1347–1353. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.; Card, T.R.; Delahooke, T.; Aithal, G.P.; Guha, I.N. Obesity Is the Most Common Risk Factor for Chronic Liver Disease: Results From a Risk Stratification Pathway Using Transient Elastography. Am. J. Gastroenterol. 2019, 114, 1744–1752. [Google Scholar] [CrossRef]
- Petta, S.; Di Marco, V.; Pipitone, R.M.; Grimaudo, S.; Buscemi, C.; Craxì, A.; Buscemi, S. Prevalence and Severity of Nonalcoholic Fatty Liver Disease by Transient Elastography: Genetic and Metabolic Risk Factors in a General Population. Liver Int. 2018, 38, 2060–2068. [Google Scholar] [CrossRef]
- Estes, C.; Anstee, Q.M.; Arias-Loste, M.T.; Bantel, H.; Bellentani, S.; Caballeria, J.; Colombo, M.; Craxi, A.; Crespo, J.; Day, C.P.; et al. Modeling NAFLD Disease Burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the Period 2016–2030. J. Hepatol. 2018, 69, 896–904. [Google Scholar] [CrossRef]
- Hagström, H.; Thiele, M.; Roelstraete, B.; Söderling, J.; Ludvigsson, J.F. Mortality in Biopsy-Proven Alcohol-Related Liver Disease: A Population-Based Nationwide Cohort Study of 3453 Patients. Gut 2021, 70, 170–179. [Google Scholar] [CrossRef]
- Rhodes, F.A.; Cococcia, S.; Patel, P.; Panovska-Griffiths, J.; Tanwar, S.; Westbrook, R.H.; Rodger, A.; Rosenberg, W. Is There Scope to Improve the Selection of Patients with Alcohol-Related Liver Disease for Referral to Secondary Care? A Retrospective Analysis of Primary Care Referrals to a UK Liver Centre, Incorporating Simple Blood Tests. BMJ Open 2021, 11, e047786. [Google Scholar] [CrossRef]
- Lyu, H.; Tang, H.; Liang, Y.; Huang, S.; Wang, Y.; Huang, W.; Zhou, Y. Alcohol Consumption and Risk of Liver Fibrosis in People Living With HIV: A Systematic Review and Meta-Analysis. Front. Immunol. 2022, 13, 841314. [Google Scholar] [CrossRef] [PubMed]
- Glyn-Owen, K.; Böhning, D.; Parkes, J.; Roderick, P.; Buchanan, R. The Combined Effect of Alcohol and Body Mass Index on Risk of Chronic Liver Disease: A Systematic Review and Meta-Analysis of Cohort Studies. Liver Int. 2021, 41, 1216–1226. [Google Scholar] [CrossRef] [PubMed]
- Decraecker, M.; Dutartre, D.; Hiriart, J.-B.; Irles-Depé, M.; Marraud des Grottes, H.; Chermak, F.; Foucher, J.; Delamarre, A.; de Ledinghen, V. Long-Term Prognosis of Patients with Alcohol-Related Liver Disease or Non-Alcoholic Fatty Liver Disease According to Metabolic Syndrome or Alcohol Use. Liver Int. 2022, 42, 350–362. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The Diagnosis and Management of Nonalcoholic Fatty Liver Disease: Practice Guidance from the American Association for the Study of Liver Diseases: Hepatology, Vol. XX, No. X, 2017. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanwal, F.; Shubrook, J.H.; Adams, L.A.; Pfotenhauer, K.; Wai-Sun Wong, V.; Wright, E.; Abdelmalek, M.F.; Harrison, S.A.; Loomba, R.; Mantzoros, C.S.; et al. Clinical Care Pathway for the Risk Stratification and Management of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2021, 161, 1657–1669. [Google Scholar] [CrossRef]
- Thomaides-Brears, H.B.; Alkhouri, N.; Allende, D.; Harisinghani, M.; Noureddin, M.; Reau, N.S.; French, M.; Pantoja, C.; Mouchti, S.; Cryer, D.R.H. Incidence of Complications from Percutaneous Biopsy in Chronic Liver Disease: A Systematic Review and Meta-Analysis. Dig. Dis. Sci. 2022, 67, 3366–3394. [Google Scholar] [CrossRef]
- Bravo, A.A.; Sheth, S.G.; Chopra, S. Liver Biopsy. N. Engl. J Med. 2001, 344, 495–500. [Google Scholar] [CrossRef]
- Lee, J.; Vali, Y.; Boursier, J.; Spijker, R.; Anstee, Q.M.; Bossuyt, P.M.; Zafarmand, M.H. Prognostic Accuracy of FIB-4, NAFLD Fibrosis Score and APRI for NAFLD-Related Events: A Systematic Review. Liver Int. 2021, 41, 261–270. [Google Scholar] [CrossRef]
- Vali, Y.; Lee, J.; Boursier, J.; Spijker, R.; Löffler, J.; Verheij, J.; Brosnan, M.J.; Böcskei, Z.; Anstee, Q.M.; Bossuyt, P.M.; et al. Enhanced Liver Fibrosis Test for the Non-Invasive Diagnosis of Fibrosis in Patients with NAFLD: A Systematic Review and Meta-Analysis. J. Hepatol. 2020, 73, 252–262. [Google Scholar] [CrossRef]
- Vali, Y.; Lee, J.; Boursier, J.; Spijker, R.; Verheij, J.; Brosnan, M.J.; Anstee, Q.M.; Bossuyt, P.M.; Zafarmand, M.H.; on behalf of the LITMUS Systematic Review Team. FibroTest for Evaluating Fibrosis in Non-Alcoholic Fatty Liver Disease Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2415. [Google Scholar] [CrossRef]
- Van Dijk, A.-M.; Vali, Y.; Mak, A.L.; Lee, J.; Tushuizen, M.E.; Zafarmand, M.H.; Anstee, Q.M.; Brosnan, M.J.; Nieuwdorp, M.; Bossuyt, P.M.; et al. Systematic Review with Meta-Analyses: Diagnostic Accuracy of FibroMeter Tests in Patients with Non-Alcoholic Fatty Liver Disease. J. Clin. Med. 2021, 10, 2910. [Google Scholar] [CrossRef] [PubMed]
- Boursier, J.; Vergniol, J.; Guillet, A.; Hiriart, J.-B.; Lannes, A.; Le Bail, B.; Michalak, S.; Chermak, F.; Bertrais, S.; Foucher, J.; et al. Diagnostic Accuracy and Prognostic Significance of Blood Fibrosis Tests and Liver Stiffness Measurement by FibroScan in Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2016, 65, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Guillaume, M.; Moal, V.; Delabaudiere, C.; Zuberbuhler, F.; Robic, M.-A.; Lannes, A.; Metivier, S.; Oberti, F.; Gourdy, P.; Fouchard-Hubert, I.; et al. Direct Comparison of the Specialised Blood Fibrosis Tests FibroMeterV2G and Enhanced Liver Fibrosis Score in Patients with Non-Alcoholic Fatty Liver Disease from Tertiary Care Centres. Aliment. Pharmacol. Ther. 2019, 50, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- Poynard, T.; Imbert-Bismut, F.; Munteanu, M.; Messous, D.; Myers, R.P.; Thabut, D.; Ratziu, V.; Mercadier, A.; Benhamou, Y.; Hainque, B. Overview of the Diagnostic Value of Biochemical Markers of Liver Fibrosis (FibroTest, HCV FibroSure) and Necrosis (ActiTest) in Patients with Chronic Hepatitis C. Comp. Hepatol. 2004, 3, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davison, B.A.; Harrison, S.A.; Cotter, G.; Alkhouri, N.; Sanyal, A.; Edwards, C.; Colca, J.R.; Iwashita, J.; Koch, G.G.; Dittrich, H.C. Suboptimal Reliability of Liver Biopsy Evaluation Has Implications for Randomized Clinical Trials. J. Hepatol. 2020, 73, 1322–1332. [Google Scholar] [CrossRef]
- Poynard, T.; Munteanu, M.; Imbert-Bismut, F.; Charlotte, F.; Thabut, D.; Le Calvez, S.; Messous, D.; Thibault, V.; Benhamou, Y.; Moussalli, J.; et al. Prospective Analysis of Discordant Results between Biochemical Markers and Biopsy in Patients with Chronic Hepatitis C. Clin. Chem. 2004, 50, 1344–1355. [Google Scholar] [CrossRef] [Green Version]
- Fontanges, T.; Bailly, F.; Trepo, E.; Chevallier, M.; Maynard-Muet, M.; Nalet, B.; Beorchia, S.; Pillon, D.; Moindrot, H.; Froissart, B.; et al. Discordance between Biochemical Markers of Liver Activity and Fibrosis (Actitest®–Fibrotest®) and Liver Biopsy in Patients with Chronic Hepatitis C. Gastroentérologie Clin. Biol. 2008, 32, 858–865. [Google Scholar] [CrossRef]
- Hagström, H.; Talbäck, M.; Andreasson, A.; Walldius, G.; Hammar, N. Ability of Noninvasive Scoring Systems to Identify Individuals in the Population at Risk for Severe Liver Disease. Gastroenterology 2020, 158, 200–214. [Google Scholar] [CrossRef] [Green Version]
- Unalp-Arida, A.; Ruhl, C.E. Liver Fibrosis Scores Predict Liver Disease Mortality in the United States Population. Hepatology 2017, 66, 84–95. [Google Scholar] [CrossRef] [Green Version]
- Angulo, P.; Bugianesi, E.; Bjornsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Barrera, F.; Haflidadottir, S.; Day, C.P.; George, J. Simple Noninvasive Systems Predict Long-Term Outcomes of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2013, 145, 782–789.e4. [Google Scholar] [CrossRef] [Green Version]
- Hagström, H.; Nasr, P.; Ekstedt, M.; Stål, P.; Hultcrantz, R.; Kechagias, S. Accuracy of Noninvasive Scoring Systems in Assessing Risk of Death and Liver-Related Endpoints in Patients With Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2019, 17, 1148–1156.e4. [Google Scholar] [CrossRef]
- Boursier, J.; Hagstrom, H.; Ekstedt, M.; Moreau, C.; Bonacci, M.; Cure, S.; Ampuero, J. Prognostic Risk Stratification Using Non-Invasive Tests with Comparison to Liver Biopsy in Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2022, 76, 1013–1020. [Google Scholar] [CrossRef]
- Braude, M.; Roberts, S.; Majeed, A.; Lubel, J.; Prompen, J.; Dev, A.; Sievert, W.; Bloom, S.; Gow, P.; Kemp, W. Liver Stiffness (Fibroscan®) Is a Predictor of All-Cause Mortality in People with Non-Alcoholic Fatty Liver Disease. Liver Int. 2022. [Google Scholar] [CrossRef]
- Hagström, H.; Talbäck, M.; Andreasson, A.; Walldius, G.; Hammar, N. Repeated FIB-4 Measurements Can Help Identify Individuals at Risk of Severe Liver Disease. J. Hepatol. 2020, 73, 1023–1029. [Google Scholar] [CrossRef]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a Simple Noninvasive Index to Predict Significant Fibrosis in Patients with HIV/HCV Coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Siddiqui, M.S.; Yamada, G.; Vuppalanchi, R.; Van Natta, M.; Loomba, R.; Guy, C.; Brandman, D.; Tonascia, J.; Chalasani, N.; Neuschwander-Tetri, B.; et al. Diagnostic Accuracy of Noninvasive Fibrosis Models to Detect Change in Fibrosis Stage. Clin. Gastroenterol. Hepatol. 2019, 17, 1877–1885.e5. [Google Scholar] [CrossRef]
- Shah, A.G.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J. Comparison of Noninvasive Markers of Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef] [Green Version]
- Thiele, M.; Madsen, B.S.; Hansen, J.F.; Detlefsen, S.; Antonsen, S.; Krag, A. Accuracy of the Enhanced Liver Fibrosis Test vs FibroTest, Elastography, and Indirect Markers in Detection of Advanced Fibrosis in Patients With Alcoholic Liver Disease. Gastroenterology 2018, 154, 1369–1379. [Google Scholar] [CrossRef] [Green Version]
- Graupera, I.; Thiele, M.; Serra-Burriel, M.; Caballeria, L.; Roulot, D.; Wong, G.L.-H.; Fabrellas, N.; Guha, I.N.; Arslanow, A.; Expósito, C.; et al. Low Accuracy of FIB-4 and NAFLD Fibrosis Scores for Screening for Liver Fibrosis in the Population. Clin. Gastroenterol. Hepatol. 2022, 20, 2567–2576. [Google Scholar] [CrossRef]
- Mózes, F.E.; Lee, J.A.; Selvaraj, E.A.; Jayaswal, A.N.A.; Trauner, M.; Boursier, J.; Fournier, C.; Staufer, K.; Stauber, R.E.; Bugianesi, E.; et al. Diagnostic Accuracy of Non-Invasive Tests for Advanced Fibrosis in Patients with NAFLD: An Individual Patient Data Meta-Analysis. Gut 2022, 71, 1006–1019. [Google Scholar] [CrossRef]
- Xiao, G.; Zhu, S.; Xiao, X.; Yan, L.; Yang, J.; Wu, G. Comparison of Laboratory Tests, Ultrasound, or Magnetic Resonance Elastography to Detect Fibrosis in Patients with Nonalcoholic Fatty Liver Disease: A Meta-Analysis. Hepatology 2017, 66, 1486–1501. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD Fibrosis Score: A Noninvasive System That Identifies Liver Fibrosis in Patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Hossain, F.; Horsfall, L.U.; Banh, X.; Hayward, K.L.; Williams, S.; Johnson, T.; Bernard, A.; Brown, N.N.; Lampe, G.; et al. A Pragmatic Approach Identifies a High Rate of Nonalcoholic Fatty Liver Disease With Advanced Fibrosis in Diabetes Clinics and At-Risk Populations in Primary Care. Hepatol. Commun. 2018, 2, 897–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciardullo, S.; Muraca, E.; Perra, S.; Bianconi, E.; Zerbini, F.; Oltolini, A.; Cannistraci, R.; Parmeggiani, P.; Manzoni, G.; Gastaldelli, A.; et al. Screening for Non-Alcoholic Fatty Liver Disease in Type 2 Diabetes Using Non-Invasive Scores and Association with Diabetic Complications. BMJ Open Diabetes Res. Care 2020, 8, e000904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boursier, J.; Canivet, C.M.; Costentin, C.; Lannes, A.; Delamarre, A.; Sturm, N.; Le Bail, B.; Michalak, S.; Oberti, F.; Hilleret, M.-N.; et al. Impact of Type 2 Diabetes on the Accuracy of Noninvasive Tests of Liver Fibrosis With Resulting Clinical Implications. Clin. Gastroenterol. Hepatol. 2022, S1542-3565(22)00248-8. [Google Scholar] [CrossRef] [PubMed]
- Selvaraj, E.A.; Mózes, F.E.; Jayaswal, A.N.A.; Zafarmand, M.H.; Vali, Y.; Lee, J.A.; Levick, C.K.; Young, L.A.J.; Palaniyappan, N.; Liu, C.-H.; et al. Diagnostic Accuracy of Elastography and Magnetic Resonance Imaging in Patients with NAFLD: A Systematic Review and Meta-Analysis. J. Hepatol. 2021, 75, 770–785. [Google Scholar] [CrossRef]
- Eddowes, P.J.; Sasso, M.; Allison, M.; Tsochatzis, E.; Anstee, Q.M.; Sheridan, D.; Guha, I.N.; Cobbold, J.F.; Deeks, J.J.; Paradis, V.; et al. Accuracy of FibroScan Controlled Attenuation Parameter and Liver Stiffness Measurement in Assessing Steatosis and Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1717–1730. [Google Scholar] [CrossRef] [Green Version]
- Sandrin, L.; Fourquet, B.; Hasquenoph, J.-M.; Yon, S.; Fournier, C.; Mal, F.; Christidis, C.; Ziol, M.; Poulet, B.; Kazemi, F.; et al. Transient Elastography: A New Noninvasive Method for Assessment of Hepatic Fibrosis. Ultrasound Med. Biol. 2003, 29, 1705–1713. [Google Scholar] [CrossRef]
- Cassinotto, C.; Boursier, J.; de Lédinghen, V.; Lebigot, J.; Lapuyade, B.; Cales, P.; Hiriart, J.-B.; Michalak, S.; Bail, B.L.; Cartier, V.; et al. Liver Stiffness in Nonalcoholic Fatty Liver Disease: A Comparison of Supersonic Shear Imaging, FibroScan, and ARFI with Liver Biopsy. Hepatology 2016, 63, 1817–1827. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.S.; Bae, J.M.; Joo, S.K.; Woo, H.; Lee, D.H.; Jung, Y.J.; Kim, B.G.; Lee, K.L.; Kim, W. Prospective Comparison among Transient Elastography, Supersonic Shear Imaging, and ARFI Imaging for Predicting Fibrosis in Nonalcoholic Fatty Liver Disease. PLoS ONE 2017, 12, e0188321. [Google Scholar] [CrossRef]
- Herrmann, E.; de Lédinghen, V.; Cassinotto, C.; Chu, W.C.-W.; Leung, V.Y.-F.; Ferraioli, G.; Filice, C.; Castera, L.; Vilgrain, V.; Ronot, M.; et al. Assessment of Biopsy-proven Liver Fibrosis by Two-dimensional Shear Wave Elastography: An Individual Patient Data-based Meta-analysis. Hepatology 2018, 67, 260–272. [Google Scholar] [CrossRef] [PubMed]
- Dong, B.; Chen, Y.; Lyu, G.; Wang, H.; Lin, G.; Gu, J. Diagnostic Accuracy of Two-dimensional Shear Wave Elastography and Magnetic Resonance Elastography for Staging Liver Fibrosis in Patients with Chronic Hepatitis B: A Systematic Review and Meta-analysis. J. Gastroenterol. Hepatol. 2022, 37, 1646. [Google Scholar] [CrossRef]
- Bauer, D.J.; Matic, V.; Mare, R.; Maiocchi, L.; Chromy, D.; Müllner-Bucsics, T.; Mandorfer, M.; Mustapic, S.; Sporea, I.; Ferraioli, G.; et al. Point Shear Wave Elastography by ElastPQ for Fibrosis Screening in Patients with NAFLD: A Prospective, Multicenter Comparison to Vibration-Controlled Elastography. Ultraschall Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Rao, J.; Wu, X.; Deng, R.; Ma, Y. Comparison of 2-D Shear Wave Elastography and Point Shear Wave Elastography for Assessing Liver Fibrosis. Ultrasound Med. Biol. 2021, 47, 408–427. [Google Scholar] [CrossRef]
- Paisant, A.; Lemoine, S.; Cassinotto, C.; de Lédinghen, V.; Ronot, M.; Irlès-Depé, M.; Vilgrain, V.; Le Bail, B.; Paradis, V.; Canivet, C.M.; et al. Reliability Criteria of Two-Dimensional Shear Wave Elastography: Analysis of 4277 Measurements in 788 Patients. Clinical Gastroenterol. Hepatol. 2022, 20, 400–408.e10. [Google Scholar] [CrossRef]
- Boursier, J.; Cassinotto, C.; Hunault, G.; Shili, S.; Lebigot, J.; Lapuyade, B.; Lannes, A.; Hiriart, J.-B.; Cartier, V.; Le Bail, B.; et al. Criteria to Determine Reliability of Noninvasive Assessment of Liver Fibrosis With Virtual Touch Quantification. Clin. Gastroenterol. Hepatol. 2019, 17, 164–171.e5. [Google Scholar] [CrossRef]
- Singh, S.; Venkatesh, S.K.; Wang, Z.; Miller, F.H.; Motosugi, U.; Low, R.N.; Hassanein, T.; Asbach, P.; Godfrey, E.M.; Yin, M.; et al. Diagnostic Performance of Magnetic Resonance Elastography in Staging Liver Fibrosis: A Systematic Review and Meta-Analysis of Individual Participant Data. Clin. Gastroenterol. Hepatol. 2015, 13, 440–451.e6. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, W.M.C.; Voelker, M.; Thiel, R.; Becka, M.; Burt, A.; Schuppan, D.; Hubscher, S.; Roskams, T.; Pinzani, M.; Arthur, M.J.P. Serum Markers Detect the Presence of Liver Fibrosis: A Cohort Study. Gastroenterology 2004, 127, 1704–1713. [Google Scholar] [CrossRef] [Green Version]
- Guha, I.N.; Parkes, J.; Roderick, P.; Chattopadhyay, D.; Cross, R.; Harris, S.; Kaye, P.; Burt, A.D.; Ryder, S.D.; Aithal, G.P.; et al. Noninvasive Markers of Fibrosis in Nonalcoholic Fatty Liver Disease: Validating the European Liver Fibrosis Panel and Exploring Simple Markers. Hepatology 2008, 47, 455–460. [Google Scholar] [CrossRef]
- Calès, P.; Oberti, F.; Michalak, S.; Hubert-Fouchard, I.; Rousselet, M.-C.; Konaté, A.; Gallois, Y.; Ternisien, C.; Chevailler, A.; Lunel, F. A Novel Panel of Blood Markers to Assess the Degree of Liver Fibrosis. Hepatology 2005, 42, 1373–1381. [Google Scholar] [CrossRef]
- Nguyen-Khac, E.; Thiele, M.; Voican, C.; Nahon, P.; Moreno, C.; Boursier, J.; Mueller, S.; de Ledinghen, V.; Stärkel, P.; Gyune Kim, S.; et al. Non-Invasive Diagnosis of Liver Fibrosis in Patients with Alcohol-Related Liver Disease by Transient Elastography: An Individual Patient Data Meta-Analysis. Lancet Gastroenterol. Hepatol. 2018, 3, 614–625. [Google Scholar] [CrossRef]
- Razavi, H.; Robbins, S.; Zeuzem, S.; Negro, F.; Buti, M.; Duberg, A.-S.; Roudot-Thoraval, F.; Craxi, A.; Manns, M.; Marinho, R.T.; et al. Hepatitis C Virus Prevalence and Level of Intervention Required to Achieve the WHO Targets for Elimination in the European Union by 2030: A Modelling Study. Lancet Gastroenterol. Hepatol. 2017, 2, 325–336. [Google Scholar] [CrossRef]
- Srivastava, A.; Gailer, R.; Tanwar, S.; Trembling, P.; Parkes, J.; Rodger, A.; Suri, D.; Thorburn, D.; Sennett, K.; Morgan, S.; et al. Prospective Evaluation of a Primary Care Referral Pathway for Patients with Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2019, 71, 371–378. [Google Scholar] [CrossRef] [Green Version]
- Majumdar, A.; Campos, S.; Gurusamy, K.; Pinzani, M.; Tsochatzis, E.A. Defining the Minimum Acceptable Diagnostic Accuracy of Noninvasive Fibrosis Testing in Cirrhosis: A Decision Analytic Modeling Study. Hepatology 2020, 71, 627–642. [Google Scholar] [CrossRef]
- Castera, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive Assessment of Liver Disease in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1264–1281.e4. [Google Scholar] [CrossRef] [Green Version]
- Vieira Barbosa, J.; Lai, M. Nonalcoholic Fatty Liver Disease Screening in Type 2 Diabetes Mellitus Patients in the Primary Care Setting. Hepatol. Commun. 2021, 5, 158–167. [Google Scholar] [CrossRef]
- Ginès, P.; Castera, L.; Lammert, F.; Graupera, I.; Serra-Burriel, M.; Allen, A.M.; Wong, V.W.; Hartmann, P.; Thiele, M.; Caballeria, L.; et al. Population Screening for Liver Fibrosis: Toward Early Diagnosis and Intervention for Chronic Liver Diseases. Hepatology 2022, 75, 219–228. [Google Scholar] [CrossRef]
- Davyduke, T.; Tandon, P.; Al-Karaghouli, M.; Abraldes, J.G.; Ma, M.M. Impact of Implementing a “FIB-4 First” Strategy on a Pathway for Patients With NAFLD Referred From Primary Care. Hepatol. Commun. 2019, 3, 1322–1333. [Google Scholar] [CrossRef] [Green Version]
- Mansour, D.; Grapes, A.; Herscovitz, M.; Cassidy, P.; Vernazza, J.; Broad, A.; Anstee, Q.M.; McPherson, S. Embedding Assessment of Liver Fibrosis into Routine Diabetic Review in Primary Care. JHEP Rep. 2021, 3, 100293. [Google Scholar] [CrossRef]
- Crossan, C.; Majumdar, A.; Srivastava, A.; Thorburn, D.; Rosenberg, W.; Pinzani, M.; Longworth, L.; Tsochatzis, E.A. Referral Pathways for Patients with NAFLD Based on Non-Invasive Fibrosis Tests: Diagnostic Accuracy and Cost Analysis. Liver International 2019, 39, 2052–2060. [Google Scholar] [CrossRef]
- Congly, S.E.; Shaheen, A.A.; Swain, M.G. Modelling the Cost Effectiveness of Non-Alcoholic Fatty Liver Disease Risk Stratification Strategies in the Community Setting. PLoS ONE 2021, 16, e0251741. [Google Scholar] [CrossRef]
- Patel, P.J.; Banh, X.; Horsfall, L.U.; Hayward, K.L.; Hossain, F.; Johnson, T.; Stuart, K.A.; Brown, N.N.; Saad, N.; Clouston, A.; et al. Underappreciation of Non-Alcoholic Fatty Liver Disease by Primary Care Clinicians: Limited Awareness of Surrogate Markers of Fibrosis. Intern. Med. J. 2018, 48, 144–151. [Google Scholar] [CrossRef]
- Said, A.; Gagovic, V.; Malecki, K.; Givens, M.L.; Nieto, F.J. Primary Care Practitioners Survey of Non-Alcoholic Fatty Liver Disease. Ann. Hepatol. 2013, 12, 758–765. [Google Scholar] [CrossRef]
- Grattagliano, I.; Ubaldi, E.; Napoli, L.; Marulli, C.F.; Nebiacolombo, C.; Cottone, C.; Portincasa, P. Utility of Noninvasive Methods for the Characterization of Nonalcoholic Liver Steatosis in the Family Practice. The “VARES” Italian Multicenter Study. Ann. Hepatol. 2013, 12, 70–77. [Google Scholar] [CrossRef]
- Canivet, C.M.; Smati, S.; Lannes, A.; Brisseau, J.; Judon, L.; Roch, M.L.; Cariou, B.; Bellanger, W.; Guerci, B.; Boursier, J. Awareness of Chronic Liver Diseases, a Comparison between Diabetologists and General Practitioners. Clin. Res. Hepatol. Gastroenterol. 2021, 46, 101848. [Google Scholar] [CrossRef]
- Kallman, J.B.; Arsalla, A.; Park, V.; Dhungel, S.; Bhatia, P.; Haddad, D.; Wheeler, A.; Younossi, Z.M. Screening for Hepatitis B, C and Non-Alcoholic Fatty Liver Disease: A Survey of Community-Based Physicians. Aliment. Pharmacol. Ther. 2009, 29, 1019–1024. [Google Scholar] [CrossRef]
- van Asten, M.; Verhaegh, P.; Koek, G.; Verbeek, J. The Increasing Burden of NAFLD Fibrosis in the General Population: Time to Bridge the Gap between Hepatologists and Primary Care. Hepatology 2017, 65, 1078. [Google Scholar] [CrossRef] [Green Version]
- Boursier, J.; Shreay, S.; Fabron, C.; Torreton, E.; Fraysse, J. Hospitalization Costs and Risk of Mortality in Adults with Nonalcoholic Steatohepatitis: Analysis of a French National Hospital Database. EClinicalMedicine 2020, 25, 100445. [Google Scholar] [CrossRef]
- Bergqvist, C.-J.; Skoien, R.; Horsfall, L.; Clouston, A.D.; Jonsson, J.R.; Powell, E.E. Awareness and Opinions of Non-Alcoholic Fatty Liver Disease by Hospital Specialists. Intern. Med. J. 2013, 43, 247–253. [Google Scholar] [CrossRef]
- Marjot, T.; Sbardella, E.; Moolla, A.; Hazlehurst, J.M.; Tan, G.D.; Ainsworth, M.; Cobbold, J.F.L.; Tomlinson, J.W. Prevalence and Severity of Non-Alcoholic Fatty Liver Disease Are Underestimated in Clinical Practice: Impact of a Dedicated Screening Approach at a Large University Teaching Hospital. Diabet. Med. 2018, 35, 89–98. [Google Scholar] [CrossRef]
- Kim, H.; Yang, J.D.; El-Serag, H.B.; Kanwal, F. Awareness of Chronic Viral Hepatitis in the United States: An Update from the National Health and Nutrition Examination Survey. J. Viral Hepat. 2019, 26, 596–602. [Google Scholar] [CrossRef]
- Alqahtani, S.A.; Paik, J.M.; Biswas, R.; Arshad, T.; Henry, L.; Younossi, Z.M. Poor Awareness of Liver Disease Among Adults With NAFLD in the United States. Hepatol. Commun. 2021, 5, 1833–1847. [Google Scholar] [CrossRef]
- van der Veen, Y.J.; Voeten, H.A.; de Zwart, O.; Richardus, J.H. Awareness, Knowledge and Self-Reported Test Rates Regarding Hepatitis B in Turkish-Dutch: A Survey. BMC Public Health 2010, 10, 512. [Google Scholar] [CrossRef] [Green Version]
- Carrieri, P.; Mourad, A.; Marcellin, F.; Trylesinski, A.; Calleja, J.L.; Protopopescu, C.; Lazarus, J.V. Knowledge of Liver Fibrosis Stage among Adults with NAFLD / NASH Improves Adherence to Lifestyle Changes. Liver Int. 2022, 42, 984–994. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ekstedt, M.; Marchesini, G.; Mullen, J.; Novak, K.; Pericàs, J.M.; Roel, E.; Romero-Gómez, M.; Ratziu, V.; Tacke, F.; et al. A Cross-Sectional Study of the Public Health Response to Non-Alcoholic Fatty Liver Disease in Europe. J. Hepatol. 2020, 72, 14–24. [Google Scholar] [CrossRef]
Figure 1.
Referral pathway proposed by the European Association for the Study of the Liver (EASL), the American Gastroenterology Association (AGA), and the American Association for the Study of Liver Disease (AASLD) to noninvasively assess advanced liver fibrosis. Modified from [11,45]. CLD: chronic liver disease; ELF: enhanced liver fibrosis; LSM: liver stiffness measurement; MRE: magnetic resonance elastography; T2DM: type 2 diabetes mellitus, TE: transient elastography.
Figure 1.
Referral pathway proposed by the European Association for the Study of the Liver (EASL), the American Gastroenterology Association (AGA), and the American Association for the Study of Liver Disease (AASLD) to noninvasively assess advanced liver fibrosis. Modified from [11,45]. CLD: chronic liver disease; ELF: enhanced liver fibrosis; LSM: liver stiffness measurement; MRE: magnetic resonance elastography; T2DM: type 2 diabetes mellitus, TE: transient elastography.

Figure 2.
Proposed patient pathway in the general population.


{kind=link}
{kind=link}
Table 1.
Results of the studies reporting liver fibrosis prevalence in unselected participants with the use of transient elastography in a community setting.
Table 1.
Results of the studies reporting liver fibrosis prevalence in unselected participants with the use of transient elastography in a community setting.
| Study Location | Patients (Years) | Sample Size with TE Available (n) | VCTE Thresholds | Prevalence of Outcome (%) | Risk Factors Independently Associated with Liver Fibrosis in Multivariate Analysis | |
|---|---|---|---|---|---|---|
| Roulot 2011 [12] | France | ≥45 | 1190 | 8.0 kPa | 7.5 | Metabolic syndrome; BMI ≥30; Age ≥57 years; Diabetes; GGT ≥45 IU/l; ALT ≥40 IU/l |
| Wong 2012 a [19] | Hong Kong | 18–70 | 759 | 9.6 kPa | 2.0 | ALT level; BMI |
| Fabrellas 2013 [13] | Spain | 18–70 | 495 | 6.8 kPa | 5.7 | - |
| You 2015 [17] | Korea | adults | 159 | 7.0 kPa | 6.9 | BMI >24.2; ALT >19 IU/l; carotid intimal media thickness >0.68 mm; ≥1 calcified carotid plaque |
| Koehler 2016 [15] | The Netherlands | ≥45 | 3041 | 8.0 kPa | 5.6 | Type 2 diabetes; liver steatosis; HBsAg and/or anti-HCV positive; age; spleen size; current or former smoking; ALT level |
| Caballeria 2018 [14] | Spain | 18–75 | 3076 | 8.0 kPa | 5.8 | Male sex; AST and/or ALT >ULN; abdominal obesity; glucose level ≥100 mg/dL; low HDL; triglyceride level ≥150 mg/dL; type 2 diabetes |
| Llop 2021 [16] | Spain | 20–79 | 11,440 | 8.0 kPa | 5.6 | Age; male sex; AST level; ALT level; metabolic syndrome |
| Nah 2021 [20] | Korea | 19–85 | 8183 | 2.90 kPa * | 9.5 | Age; male sex; diabetes; HBsAg positivity; abnormal LFT; obesity; metabolic syndrome |
ALT: alanine aminotransferase; AST: aspartate aminotransferase; BMI: body-mass index in kg/m2; GGT: glutamyl gamma transferase; HBsAg: HBs antigen; HCV: hepatitis C virus; HDL: high-density lipoprotein; LDL: low-density lipoprotein; VCTE: vibration controlled transient elastography. a Exclusion of chronic viral hepatitis. * by MRE.
Table 2.
Advantages and disadvantages of the main noninvasive liver fibrosis tests from [11].
Table 2.
Advantages and disadvantages of the main noninvasive liver fibrosis tests from [11].
| Advantages | Disadvantages | |
|---|---|---|
| Simple blood tests |
|
|
| Specialized blood tests |
|
|
| Transient elastography |
|
|
| pSWE/2D-SWE |
|
|
| MRE |
|
|
VCTE: vibration controlled transient elastography; pSWE: point shear wave elastography; 2D-SWE: bidimensional shear wave elastography; MRE: magnetic resonance elastography; MRI: magnetic resonance imaging; FIB-4: Fibrosis-4; NFS: NAFLD fibrosis score.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Canivet, C.M.; Boursier, J. Screening for Liver Fibrosis in the General Population: Where Do We Stand in 2022? Diagnostics 2023, 13, 91. https://doi.org/10.3390/diagnostics13010091
AMA Style
Canivet CM, Boursier J. Screening for Liver Fibrosis in the General Population: Where Do We Stand in 2022? Diagnostics. 2023; 13(1):91. https://doi.org/10.3390/diagnostics13010091
Chicago/Turabian StyleCanivet, Clémence M., and Jérôme Boursier. 2023. "Screening for Liver Fibrosis in the General Population: Where Do We Stand in 2022?" Diagnostics 13, no. 1: 91. https://doi.org/10.3390/diagnostics13010091
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.