
Clinical Assessment of Chronic Musculoskeletal Pain—A Framework Proposal Based on a Narrative Review of the Literature

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
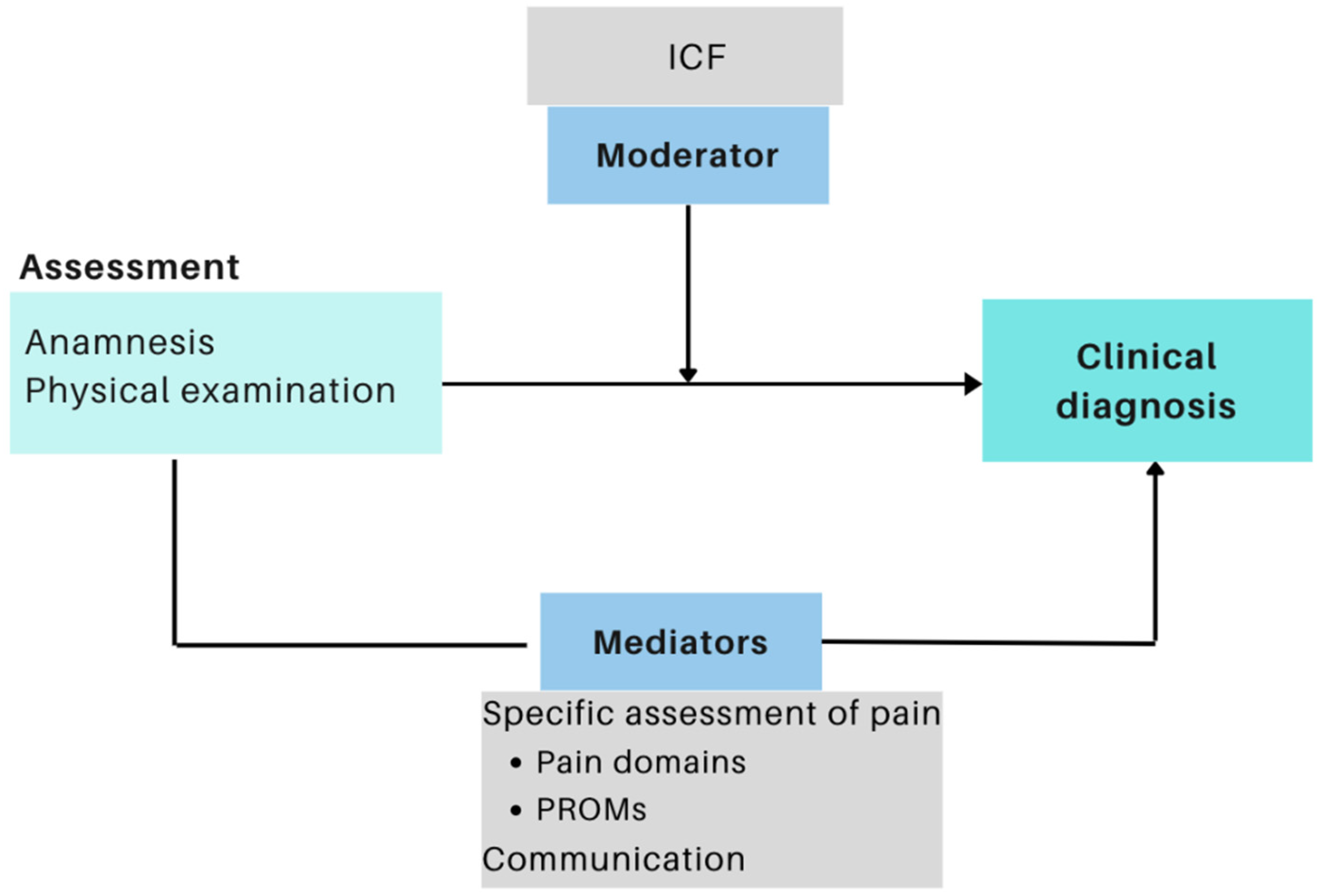
3. The Framework Proposal
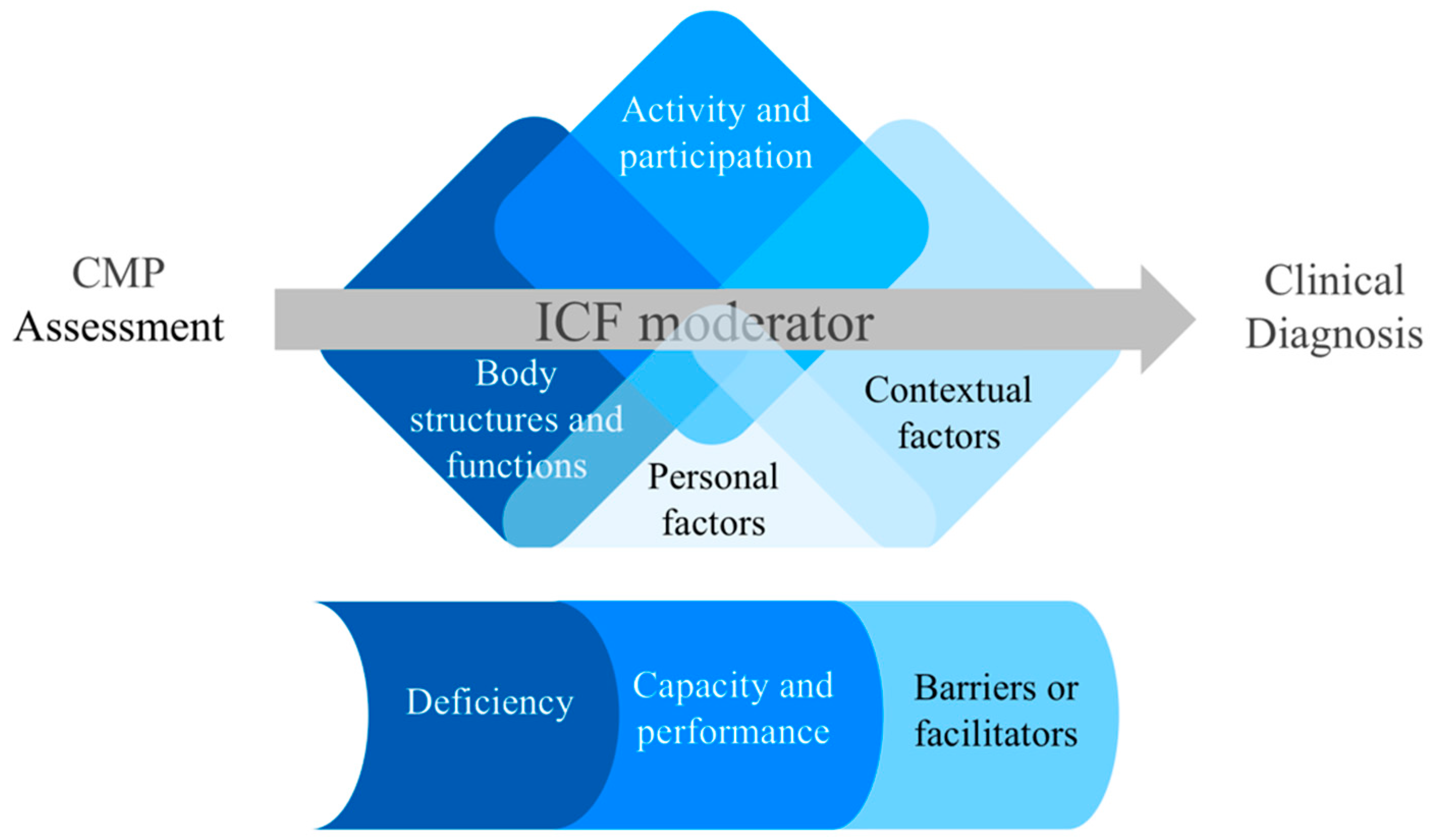
3.1. The ICF as a Moderator of CMP Assessment
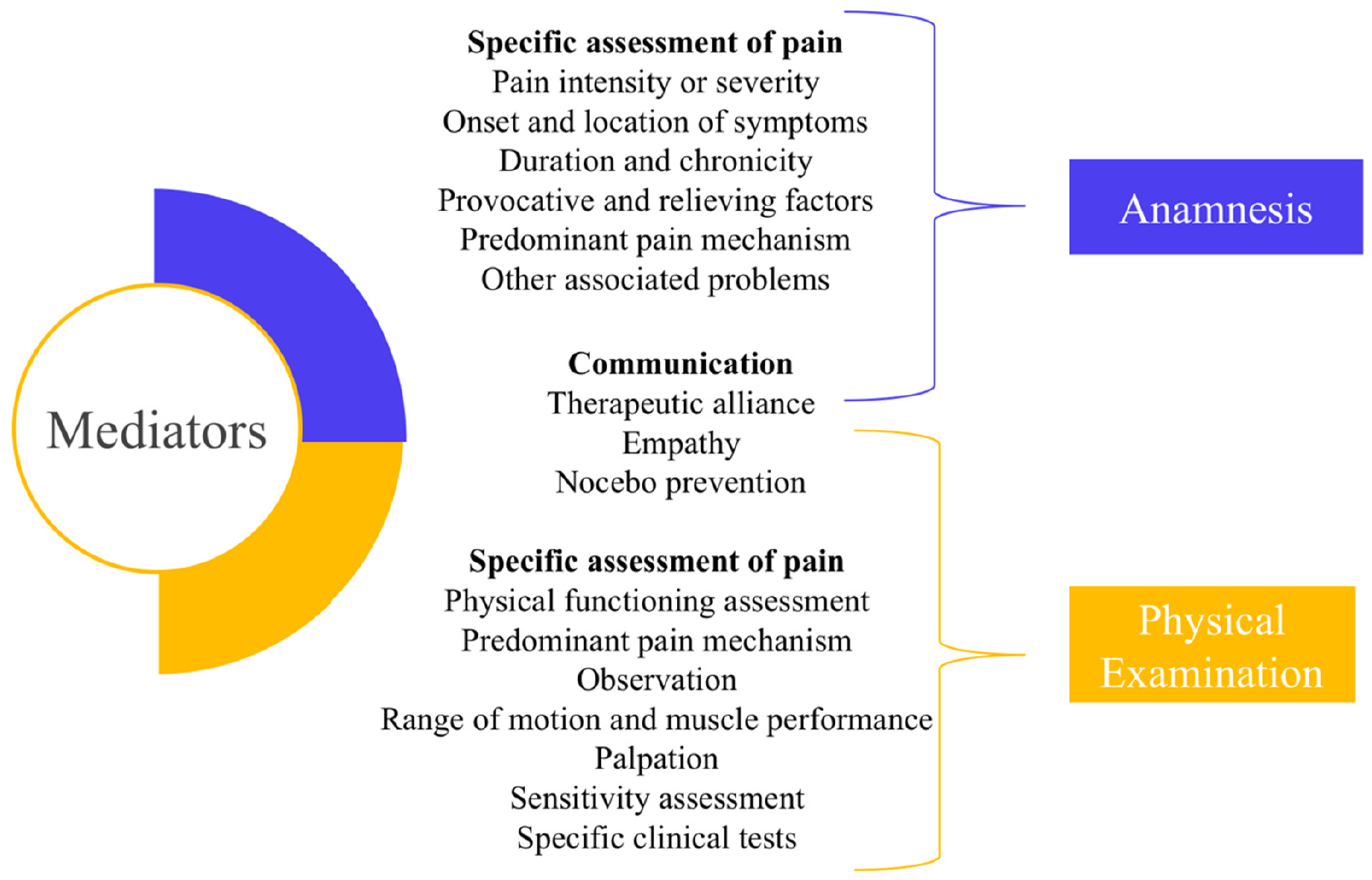
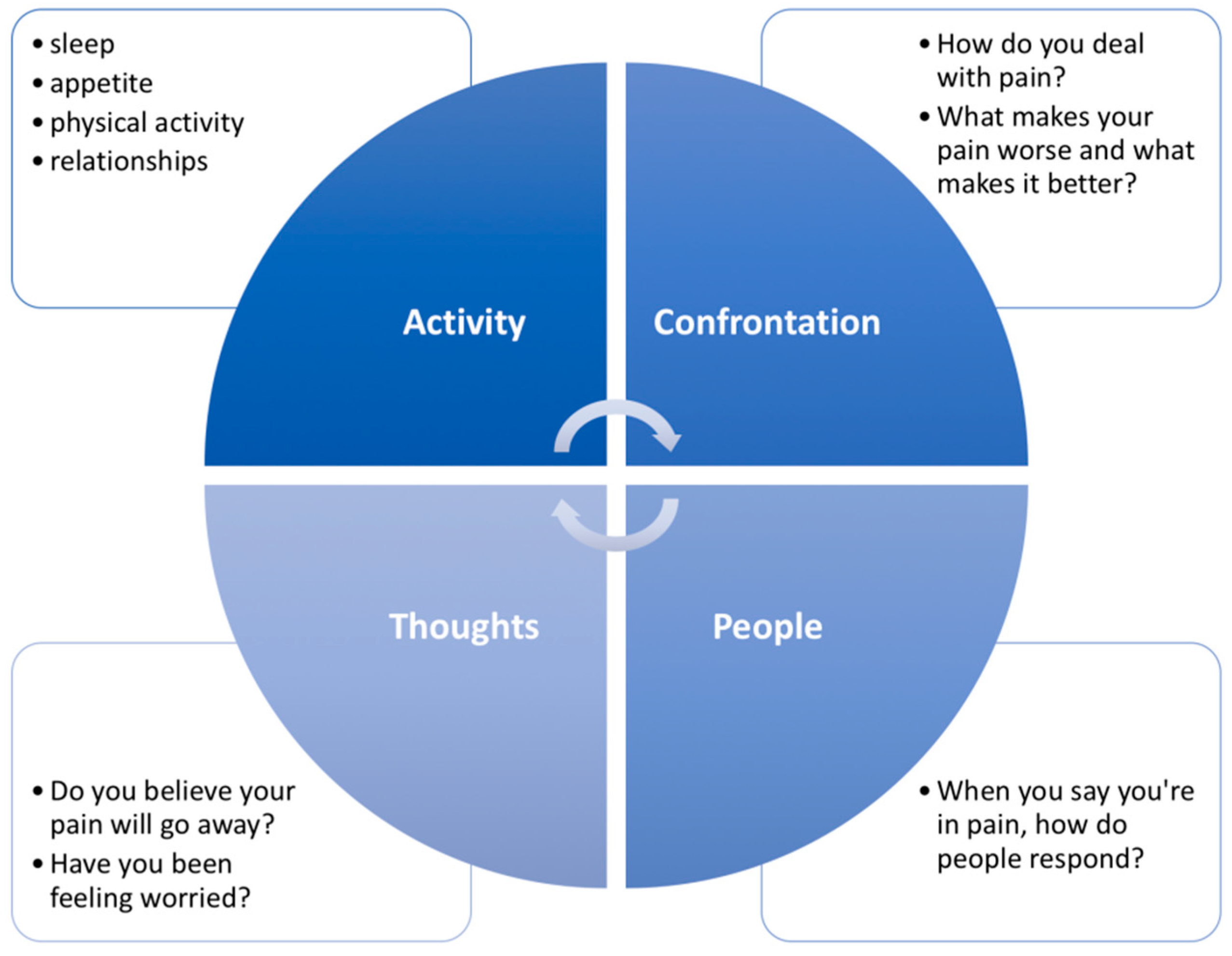
3.2. Mediators of CMP Assessment: Specific Assessment of Pain and Effective Communication
4. Current Concepts on Anamnesis for CMP Assessment
4.1. Pain Intensity or Severity
4.2. Onset and Location of Symptoms
4.3. Duration and Chronicity
4.4. Provocative and Relieving Factors
4.5. Predominant Pain Mechanism
4.6. Other Associated Problems
5. Current Concepts on Physical Examination of CMP
5.1. Assessing Physical Functioning
5.2. Pain Mechanism
5.3. Observation
5.4. Palpation
5.5. Range of Motion (ROM) and Muscle Performance
5.6. Sensitivity Assessment
5.7. Specific Clinical Tests
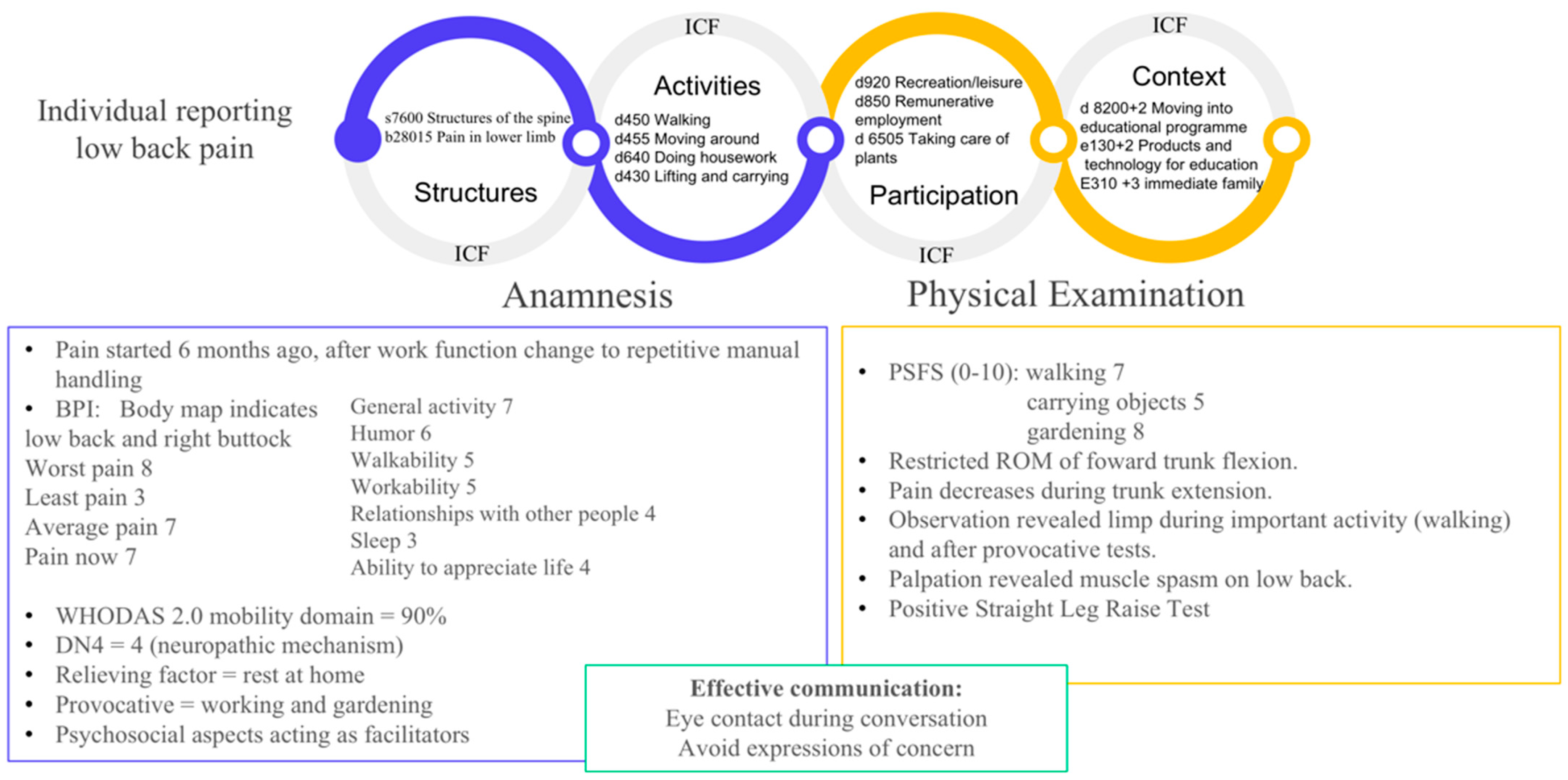
6. An Example of Clinical Application of the Framework Proposal
7. Final Considerations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vos, T.; Lim, S.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahi, M.; Abdollahpour, I.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Fillingim, R.B. Individual differences in pain: Understanding the mosaic that makes pain personal. Pain 2017, 158, S11–S18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paap, D.; Krops, L.A.; SchiphorstPreuper, H.R.; Geertzen, J.H.B.; Dijkstra, P.U.; Pool, G. Participants’ unspoken thoughts and feelings negatively influence the therapeutic alliance; a qualitative study in a multidisciplinary pain rehabilitation setting. Disabil. Rehabil. 2022, 44, 5090–5100. [Google Scholar] [CrossRef] [PubMed]
- Clauw, D.J.; Essex, M.N.; Pitman, V.; Jones, K.D. Reframing chronic pain as a disease, not a symptom: Rationale and implications for pain management. Postgrad Med. 2019, 131, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Chiarotto, A.; Boers, M.; Deyo, R.A.; Buchbinder, R.; Corbin, T.P.; Costa, L.O.P.; Foster, N.E.; Grotle, M.; Koes, B.W.; Kovacs, F.M.; et al. Core outcome measurement instruments for clinical trials in nonspecific low back pain. Pain 2018, 159, 481–495. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M.L.; Machado, G.; Latimer, J.; Maher, C.; Ferreira, P.H.; Smeets, R.J. Factors defining care-seeking in low back pain--a meta-analysis of population based surveys. Eur. J. Pain 2010, 14, 747. [Google Scholar] [CrossRef]
- La Touche, R.; Grande-Alonso, M.; Arnes-Prieto, P.; Paris-Alemany, A. How Does Self-Efficacy Influence Pain Perception, Postural Stability and Range of Motion in Individuals with Chronic Low Back Pain? Pain Physician 2019, 22, E1–E13. [Google Scholar] [CrossRef]
- Luque-Suarez, A.; Martinez-Calderon, J.; Falla, D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: A systematic review. Br. J. Sport. Med. 2019, 53, 554–559. [Google Scholar] [CrossRef] [Green Version]
- Solé, E.; Racine, M.; Tomé-Pires, C.; Galán, S.; Jensen, M.P.; Miró, J. Social Factors, Disability, and Depressive Symptoms in Adults With Chronic Pain. Clin. J. Pain 2020, 36, 371–378. [Google Scholar] [CrossRef]
- Orhan, C.; Van Looveren, E.; Cagnie, B.; Mukhtar, N.B.; Lenoir, D.; Meeus, M. Are Pain Beliefs, Cognitions, and Behaviors Influenced by Race, Ethnicity, and Culture in Patients with Chronic Musculoskeletal Pain: A Systematic Review. Pain Physician 2018, 21, 541–558. [Google Scholar] [PubMed]
- Maart, S.; Sykes, C. Expanding on the use of The International Classification of Functioning, Disability and Health: Examples and resources. South Afr. J. Physiother. 2022, 78, 1614. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, M.; Lee, H.; Kostanjsek, N.; Fornari, A.; Raggi, A.; Martinuzzi, A.; Yáñez, M.; Almborg, A.H.; Fresk, M.; Besstrashnova, Y.; et al. 20 Years of ICF-International Classification of Functioning, Disability and Health: Uses and Applications around the World. Int. J. Env. Res. Public Health 2022, 19, 11321. [Google Scholar] [CrossRef] [PubMed]
- Waterschoot, F.P.; Bennen, E.; van der Woude, L.H.; Schiphorst Preuper, H.R.; Reneman, M.F. Case complexity in patients with chronic nonspecific musculoskeletal pain: A Delphi and feasibility study. Int. J. Rehabil. Res. 2016, 39, 48–56. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. How to Use the ICF: A Practical Manual for Using the International Classification of Functioning, Disability and Health (ICF); Exposure Draft for Comment; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Kisner, C.; Colby, L.A. Exercícios Terapêuticos: Fundamentos E Técnicas, 6th ed.; Manole: Barueri, Brazil, 2016. [Google Scholar]
- Dworkin, R.H.; Bruehl, S.; Fillingim, R.B.; Loeser, J.D.; Terman, G.W.; Turk, D.C. Multidimensional diagnostic criteria for chronic pain: Introduction to the acttion–american pain society pain taxonomy(Aapt). J. Pain 2016, 17, T1–T9. [Google Scholar] [CrossRef] [Green Version]
- Fillingim, R.B.; Bruehl, S.; Dworkin, R.H.; Dworkin, S.F.; Loeser, J.D.; Turk, D.C.; Widerstrom-Noga, E.; Arnold, L.; Bennett, R.; Edwards, R.R.; et al. The acttion-american pain society pain taxonomy (Aapt): An evidence-based and multidimensional approach to classifying chronic pain conditions. J. Pain 2014, 15, 241–249. [Google Scholar] [CrossRef] [Green Version]
- Fillingim, R.B.; Loeser, J.D.; Baron, R.; Edwards, R.R. Assessment of chronic pain: Domains, methods, and mechanisms. J. Pain 2016, 17, T10–T20. [Google Scholar] [CrossRef] [Green Version]
- Green, B.N.; Johnson, C.D.; Adams, A. Writing narrative literature reviews for peer-reviewed journals: Secrets of the trade. J. Chiropr. Med. 2006, 5, 101–117. [Google Scholar] [CrossRef] [Green Version]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA-a scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Edwards, J.R.; Lambert, L.S. Métodos para integrar lamoderación y lamediación: Un marco analítico general utilizando unanálisis de trayectoria moderada. Métodos Psychol 2007, 12, 1–22. [Google Scholar]
- Wong, J.J.; DeSouza, A.; Hogg-Johnson, S.; De Groote, W.; Varmazyar, H.; Mior, S.A.; Stern, P.J.; Southerst, D.; Alexopulos, S.; Belchos, M.; et al. Pre-rehabilitation scores of functioning measured using the World Health Organization Disability Assessment Schedule in persons with nonspecific low back pain: A scoping review. Int. J. Rehabil. Res. 2022, 45, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Aartun, E.; Axén, I.; Mior, S.; Røe, Y.; Hondras, M.; Kretz, L.; Côté, P. Contextualizing the lived experiences of patients with low back pain from different countries according to the ICF framework. J. Rehabil. Med. 2021, 53, jrm00189. [Google Scholar] [CrossRef] [PubMed]
- Røe, Y.; Rysstad, T.; Tveter, A.T.; Sandbakk, T.B.; Jæger, M.; Grotle, M. What are the most important problems in functioning among patients with shoulder pain? An analysis of the patient-specific functional scale. Phys. Therapy 2021, 101, pzab141. [Google Scholar] [CrossRef] [PubMed]
- Cerniauskaitė, M.; Quintas, R.; Boldt, C.; Raggi, A.; Cieza, A.; Bickenbach, J.; Leonardi, M. Systematic literature review on ICF from 2001 to 2009: Its use, implementation and operationalisation. Disabil. Rehabil. 2001, 33, 281–309. [Google Scholar] [CrossRef] [PubMed]
- Jelsma, J. Use of the International Classification of Functioning, Disability and Health: A literature survey. J. Rehabil. Med. 2009, 41, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Paton, M.; Lane, R.; Paul, E.; Linke, N.; Shehabi, Y.; Hodgson, C.L. Correlation of patient-reported outcome measures to performance-based function in critical care survivors: PREDICTABLE. Aust. Crit. Care 2022. S1036-7314(22)00070-4. [Google Scholar] [CrossRef]
- Saltychev, M.; Katajapuu, N.; Bärlund, E.; Laimi, K. Psychometric properties of 12-item self-administered World Health Organization disability assessment schedule 2.0 (WHODAS 2.0) among general population and people with non-acute physical causes of disability—Systematic review. Disabil. Rehabil. 2021, 43, 789–794. [Google Scholar] [CrossRef]
- Taylor, A.M.; Phillips, K.; Patel, K.V.; Turk, D.C.; Dworkin, R.H.; Beaton, D.; Clauw, D.J.; Gignac, M.A.M.; Markman, J.D.; Williams, D.A.; et al. Assessment of physical function and participation in chronic pain clinical trials: IMMPACT/OMERACT recommendations. Pain 2016, 157, 1836–1850. [Google Scholar] [CrossRef] [Green Version]
- MacKinnon, D.P.; Luecken, L.J. How and for whom? Mediation and moderation in health psychology. Health Psychol. 2008, 27, S99–S100. [Google Scholar] [CrossRef] [Green Version]
- Holmes, M.M.; Lewith, G.; Newell, D.; Field, J.; Bishop, F.L. The impact of patient-reported outcome measures in clinical practice for pain: A systematic review. Qual. Life Res. 2017, 26, 245–257. [Google Scholar] [CrossRef] [Green Version]
- Longtin, C.; Coutu, M.F.; Tousignant-Laflamme, Y. Deciphering programs for optimal self-management of persistent musculoskeletal-related pain and disability—Clinical implications for PTs. Physiother. Theory Pract. 2021, 37, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Henry, S.G.; Matthias, M.S. Patient-clinician communication about pain: A conceptual model and narrative review. Pain Med. 2018, 19, 2154–2165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haußmann, A. Diagnostik von akuten und chronischen Rückenschmerzen. Radiologe 2020, 60, 109–116. [Google Scholar] [CrossRef]
- Costa, L.O.P.; Maher, C.G.; Latimer, J.; Ferreira, P.H.; Ferreira, M.L.; Pozzi, G.C.; Freitas, L.M.A. Clinimetric testing of three self-report outcome measures for low back pain patients in Brazil: Which one is the best? Spine 2008, 33, 2459–2463. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.G.; Alvarelhão, J.; Queirós, A.; Rocha, N.P. Pain intensity is associated with self-reported disability for several domains of life in a sample of patients with musculoskeletal pain aged 50 or more. Disabil. Health J. 2013, 6, 369–376. [Google Scholar] [CrossRef]
- Cleeland, C.S. Measurement of Pain by Subjective Report. Adv. Pain Res. Ther. 1989, 12, 391–403. [Google Scholar]
- Melzack, R. The mcgill pain questionnaire: Major properties and scoring methods. Pain 1975, 1, 277–299. [Google Scholar] [CrossRef]
- Freynhagen, R.; Baron, R.; Gockel, U.; Tölle, T.R. Pain detect: A new screening questionnaire to identify neuropathic components in patients with back pain. Curr. Med. Res. Opin. 2006, 22, 1911–1920. [Google Scholar] [CrossRef]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: Global use of the Brief Pain Inventory. Ann. Acad. Med. Singap. 1994, 23, 129–138. [Google Scholar]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Bilsborrow, J.B.; Peláez-Ballestas, I.; Pons-Estel, B.; Scott, C.; Tian, X.; Alarcon, G.S.; Bucala, R.; Lewandowski, L.B.; Hsieh, E. Global rheumatology research: Frontiers, challenges, and opportunities. Arthritis Rheumatol. 2022, 74, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Roldán-Jiménez, C.; Pérez-Cruzado, D.; Neblett, R.; Gatchel, R.; Cuesta-Vargas, A. Central sensitization in chronic musculoskeletal pain disorders in different populations: A cross-sectional study. Pain Medicine. 2020, 21, 2958–2963. [Google Scholar] [CrossRef] [PubMed]
- Leadley, R.M.; Armstrong, N.; Reid, K.J.; Allen, A.; Misso, K.V.; Kleijnen, J. Healthy aging in relation to chronic pain and quality of life in europe. Pain Pract. 2014, 14, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Colloca, L.; Enck, P.; DeGrazia, D. Relieving pain using dose-extending placebos: A scoping review. Pain 2016, 157, 1590–1598. [Google Scholar] [CrossRef] [Green Version]
- Street, R.L.; Gordon, H.S.; Ward, M.M.; Krupat, E.; Kravitz, R.L. Patient participation in medical consultations: Why some patients are more involved than others. Med. Care 2005, 43, 960–969. [Google Scholar] [CrossRef] [PubMed]
- Col, N.; Hull, S.; Springmann, V.; Ngo, L.; Merritt, E.; Gold, S.; Sprintz, M.; Genova, N.; Nesin, N.; Tierman, B.; et al. Improving patient-provider communication about chronic pain: Development and feasibility testing of a shared decision-making tool. BMC Med. Inform. Decis. Mak. 2020, 20, 267. [Google Scholar] [CrossRef]
- Bouhassira, D.; Attal, N.; Alchaar, H.; Boureau, F.; Brochet, B.; Bruxelle, J.; Cunin, G.; Fermanian, J.; Ginies, P.; Grun-Overdyking, A.; et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (Dn4). Pain 2005, 114, 29–36. [Google Scholar] [CrossRef]
- Haack, M.; Simpson, N.; Sethna, N.; Kaur, S.; Mullington, J. Sleep deficiency and chronic pain: Potential underlying mechanisms and clinical implications. Neuropsychopharmacol 2020, 45, 205–216. [Google Scholar] [CrossRef]
- Andersen, M.L.; Araujo, P.; Frange, C.; Tufik, S. Sleep disturbance and pain. Chest 2018, 154, 1249–1259. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Kremer, M.; Becker, L.J.; Barrot, M.; Yalcin, I. How to study anxiety and depression in rodent models of chronic pain? Eur. J. Neurosci. 2021, 53, 236–270. [Google Scholar] [CrossRef] [PubMed]
- IsHak, W.W.; Wen, R.Y.; Naghdechi, L.; Vanle, B.; Dang, J.; Knosp, M.; Dascal, J.; Marcia, L.; Gohar, Y.; Eskander, L.; et al. Pain and depression: A systematic review. Harv. Rev. Psychiatry 2018, 26, 352–363. [Google Scholar] [CrossRef] [PubMed]
- Doan, L.; Manders, T.; Wang, J. Neuroplasticity underlying the comorbidity of pain and depression. Neural. Plast. 2015, 2015, 504691. [Google Scholar] [CrossRef]
- Spitzer, R.L. Validation and utility of a self-report version of prime-mdthephq primary care study. JAMA 1999, 282, 1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swinson, R.P. The GAD-7 scale was accurate for diagnosing generalised anxiety disorder. Evid. -Based Med. 2006, 11, 184. [Google Scholar] [CrossRef] [Green Version]
- Varela, A.J.; Van Asselt, K.W. The relationship between psychosocial factors and reported disability: The role of pain self-efficacy. BMC Musculoskelet Disord 2022, 23, 21. [Google Scholar] [CrossRef]
- Hayden, J.A.; Wilson, M.N.; Riley, R.D.; Iles, R.; Pincus, T.; Ogilvie, R.; Cochrane Back and Neck Group. Individual recovery expectations and prognosis of outcomes in non-specific low back pain: Prognostic factor review. Cochrane Database Syst. Rev. 2019, 2019, CD011284. [Google Scholar] [CrossRef] [PubMed]
- Waddell, G.; Newton, M.; Henderson, I.; Somerville, D.; Main, C.J. A Fear-Avoidance Beliefs Questionnaire (Fabq) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain 1993, 52, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.P.; Kori, S.H.; Todd, D.D. The tampa scale: A measure of kinisophobia. Clin. J. Pain 1991, 7, 51. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Dansie, E.J.; Turk, D.C. Assessment of patients with chronic pain. Br. J. Anaesthesia. 2013, 111, 19–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, L.D.; Daniels, K.J.; Ganguli, B.; Louw, Q.A. An update on the prevalence of low back pain in Africa: A systematic review and meta-analyses. BMC Musculoskelet Disord. 2018, 19, 196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lannon, E.; Sanchez-Saez, F.; Bailey, B.; Hellman, N.; Kinney, K.; Williams, A.; Nag, S.; Kutcher, M.E.; Goodin, B.R.; Rao, U.; et al. Predicting pain among female survivors of recent interpersonal violence: A proof-of-concept machine-learning approach. PLoS ONE 2021, 16, e0255277. [Google Scholar] [CrossRef] [PubMed]
- El-Tallawy, S.N.; Nalamasu, R.; Salem, G.I.; LeQuang, J.A.K.; Pergolizzi, J.V.; Christo, P.J. Management of musculoskeletal pain: An update with emphasis on chronic musculoskeletal pain. Pain Ther. 2021, 10, 181–209. [Google Scholar] [CrossRef]
- Muskardin, T.L.W.; Niewold, T.B. Type I interferon in rheumatic diseases. Nat. Rev. Rheumatol. 2018, 14, 214–228. [Google Scholar] [CrossRef] [PubMed]
- Hashim, M.M.; Edgeworth, D.M.; Saunders, J.A.; Harmon, D.C. Patient’s perceptions of physical examination in the setting of chronic pain. Ir. J. Med. Sci. 2021, 190, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Deutsch, J.E.; Gill-Body, K.M.; Schenkman, M. Updated Integrated Framework for Making Clinical Decisions Across the Lifespan and Health Conditions. Phys. Ther. 2022, 102, pzab281. [Google Scholar] [CrossRef]
- Verghese, A.; Horwitz, R.I. In praise of the physical examination. BMJ 2009, 339, b5448. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, S.; Macnaughton, J.; Saunders, C.; Evans, M. Cool intimacies of care for contemporary clinical practice. Lancet 2010, 376, 1732–1733. [Google Scholar] [CrossRef] [Green Version]
- Wilson, D.; Williams, M.; Butler, D. Language and the pain experience. Physiother. Res. Int. 2009, 14, 56–65. [Google Scholar] [CrossRef]
- Sterling, M.; Brentnall, D. Patient Specific Functional Scale. Aust. J. Physiother. 2007, 53, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, L.M.; Eppler, S.L.; Roe, A.K.; Morris, A.; Kamal, R.N. The patient perspective on patient-reported outcome measures following elective hand surgery: A convergent mixed-methods analysis. J. Hand Surg. 2021, 46, 153.e1–153.e11. [Google Scholar] [CrossRef] [PubMed]
- Fresk, M.; Brodin, N.; Grooten, W.J.; Joseph, C.; Kiessling, A. Mapping a measure of physical ability for persons with long-term musculoskeletal pain to the ICF and ICF Core Sets. Eur. J. Public Health 2019, 29, 286–291. [Google Scholar] [CrossRef]
- Estévez-López, F.; Álvarez-Gallardo, I.C.; Segura-Jiménez, V.; Soriano-Maldonado, A.; Borges-Cosic, M.; Pulido-Martos, M.; Aparicio, V.A.; Carbonell-Baeza, A.; Delgado-Fernández, M.; Geenen, R. The discordance between subjectively and objectively measured physical function in women with fibromyalgia: Association with catastrophizing and self-efficacy cognitions. The al-Ándalus project. Disabil. Rehabil. 2016, 40, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Wijma, A.J.; van Wilgen, C.P.; Meeus, M.; Nijs, J. Clinical biopsychosocial physiotherapy assessment of patients with chronic pain: The first step in pain neuroscience education. Physiother. Theory Pract. 2016, 32, 368–384. [Google Scholar] [CrossRef] [PubMed]
- Shraim, M.A.; Sluka, K.A.; Sterling, M.; Arendt-Nielsen, L.; Argoff, C.; Bagraith, K.S.; Baron, R.; Brisby, H.; Carr, D.B.; Chimenti, R.L.; et al. Features and methods to discriminate between mechanism-based categories of pain experienced in the musculoskeletal system: A Delphi expert consensus study. Pain 2022, 163, 1812–1828. [Google Scholar] [CrossRef]
- Nijs, J.; Lahousse, A.; Kapreli, E.; Bilika, P.; Saraçoğlu, İ.; Malfliet, A.; Coppieters, I.; De Baets, L.; Leysen, L.; Roose, E.; et al. Nociplastic pain criteria or recognition of central sensitization? Pain phenotyping in the past, present and future. JCM 2021, 10, 3203. [Google Scholar] [CrossRef]
- Severgnini, P.; Pelosi, P.; Contino, E.; Serafinelli, E.; Novario, R.; Chiaranda, M. Accuracy of Critical Care Pain Observation Tool and Behavioral Pain Scale to assess pain in critically ill conscious and unconscious patients: Prospective, observational study. J Intensive. Care 2016, 4, 68. [Google Scholar] [CrossRef] [Green Version]
- Gröne, E.; Crispin, A.; Fleckenstein, J.; Irnich, D.; Treede, R.D.; Lang, P.M. Test order of quantitative sensory testing facilitates mechanical hyperalgesia in healthy volunteers. J. Pain 2012, 13, 73–80. [Google Scholar] [CrossRef]
- Kosek, E.; Clauw, D.; Nijs, J.; Baron, R.; Gilron, I.; Harris, R.E.; Mico, J.-A.; Rice, A.S.C.; Sterling, M. Chronic nociplastic pain affecting the musculoskeletal system: Clinical criteria and grading system. Pain 2021, 162, 2629–2634. [Google Scholar] [CrossRef]
- Larkins, L.W.; Baker, R.T.; Baker, J.G. Physical examination of the ankle: A review of the original orthopedic special test description and scientific validity of common tests for ankle examination. Arch. Rehabil. Res. Clin. Transl. 2020, 2, 100072. [Google Scholar] [CrossRef] [PubMed]
- Salamh, P.; Lewis, J. It is time to put special tests for rotator cuff–related shoulder pain out to pasture. J. Orthop. Sport. Phys Ther. 2020, 50, 222–225. [Google Scholar] [CrossRef] [PubMed]
- Rice, A.S.C.; Smith, B.H.; Blyth, F.M. Pain and the global burden of disease. Pain 2016, 157, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Watt-Watson, J.; Siddall, P.J. Improving pain practices through core competencies. Pain Med. 2013, 14, 966–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helme, D. Trust me, I’m a patient: Pain education for professionals from a lay perspective. Br. J. Pain. 2012, 6, 79–80. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nogueira Carrer, H.C.; Zanca, G.G.; Haik, M.N. Clinical Assessment of Chronic Musculoskeletal Pain—A Framework Proposal Based on a Narrative Review of the Literature. Diagnostics 2023, 13, 62. https://doi.org/10.3390/diagnostics13010062
Nogueira Carrer HC, Zanca GG, Haik MN. Clinical Assessment of Chronic Musculoskeletal Pain—A Framework Proposal Based on a Narrative Review of the Literature. Diagnostics. 2023; 13(1):62. https://doi.org/10.3390/diagnostics13010062
Chicago/Turabian StyleNogueira Carrer, Helen Cristina, Gisele Garcia Zanca, and Melina Nevoeiro Haik. 2023. "Clinical Assessment of Chronic Musculoskeletal Pain—A Framework Proposal Based on a Narrative Review of the Literature" Diagnostics 13, no. 1: 62. https://doi.org/10.3390/diagnostics13010062