
Associations of the Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio with Osteoporosis: A Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
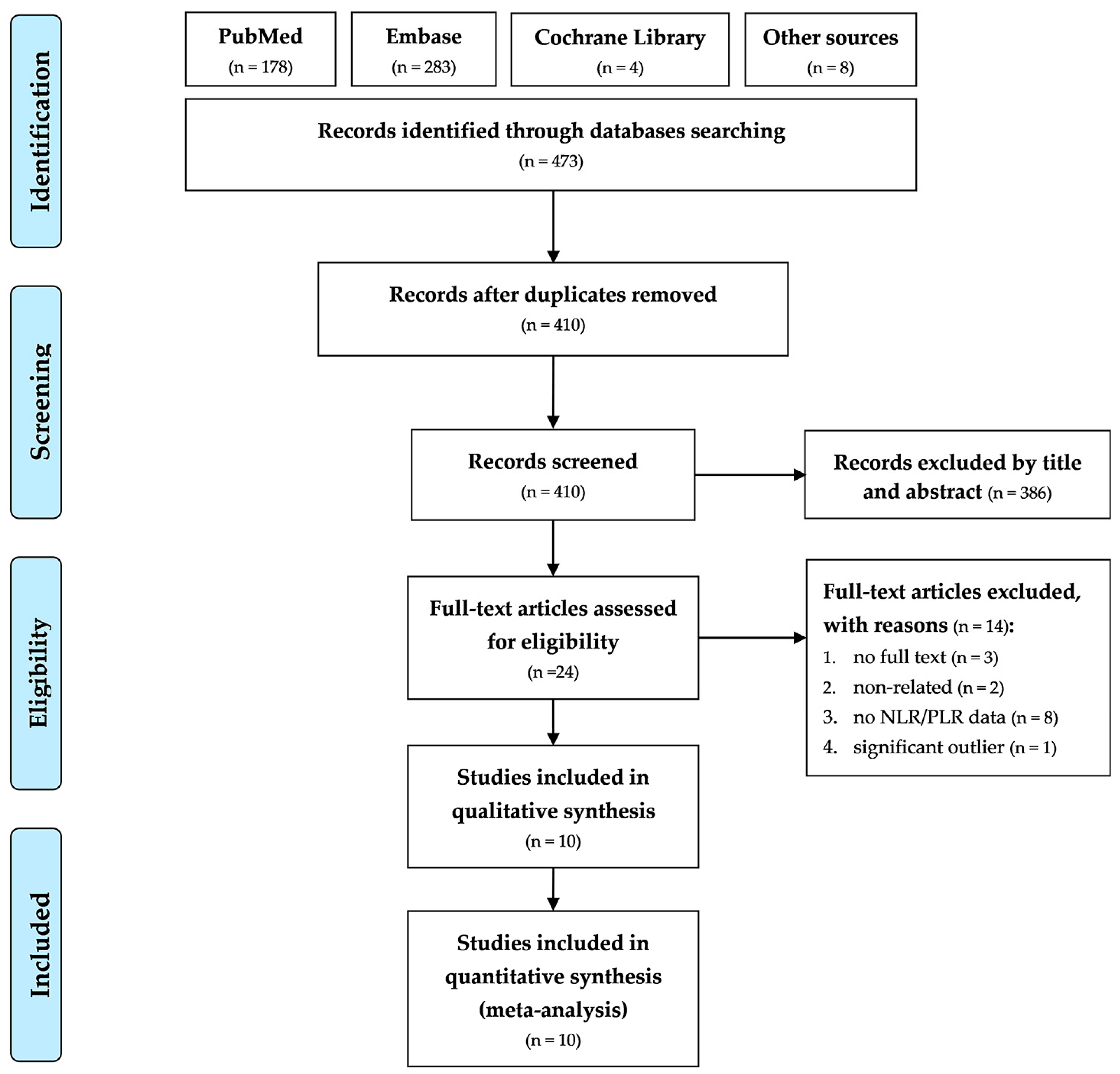
2.1. Search Strategy and Identification of Eligible Studies
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Appraisal of Methodological Quality
2.4. Outcomes
2.5. Statistical Analysis and Data Synthesis
3. Results
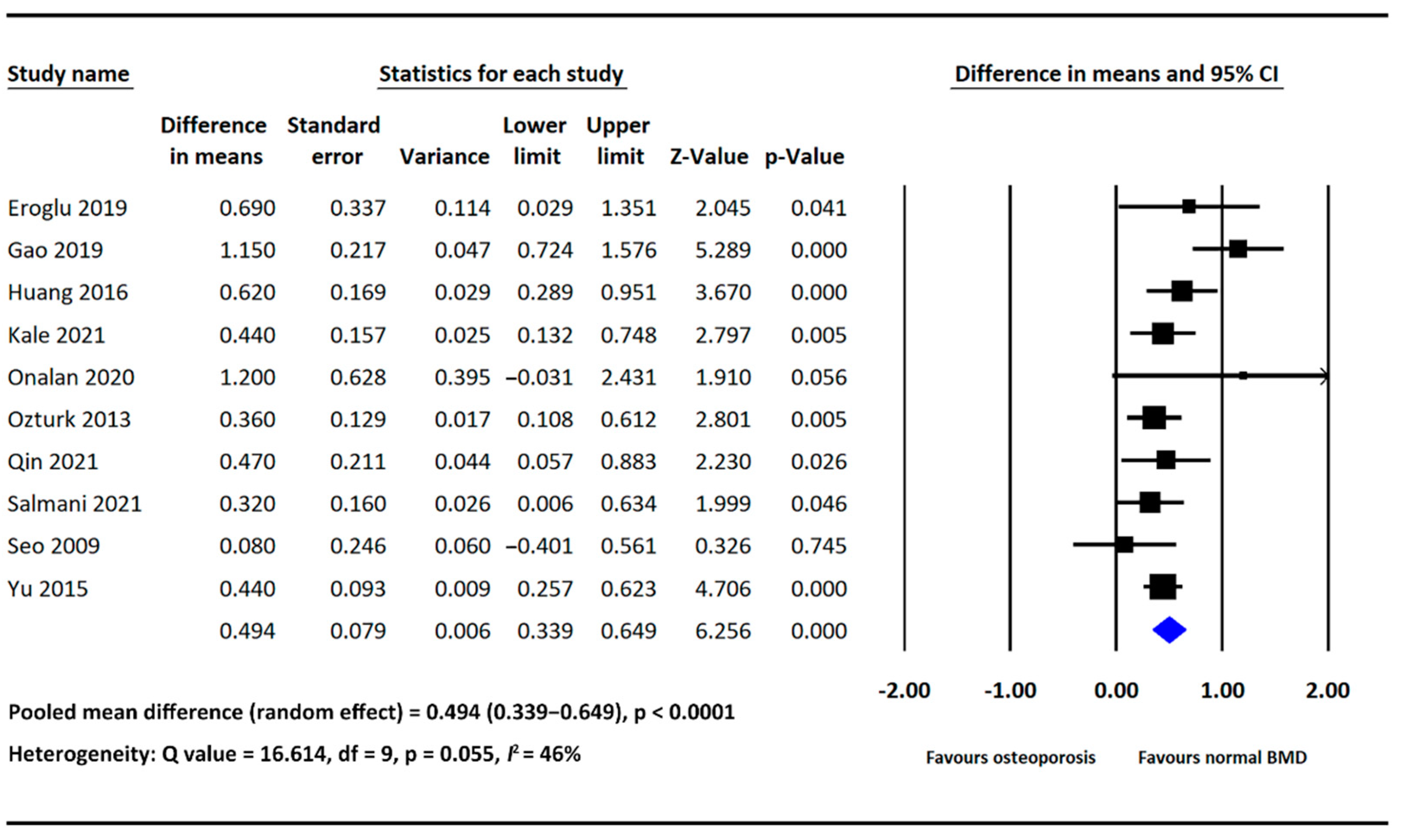
3.1. Association of NLR with Osteoporosis
3.1.1. Mean Difference in NLR between the Osteoporosis and Normal BMD Groups
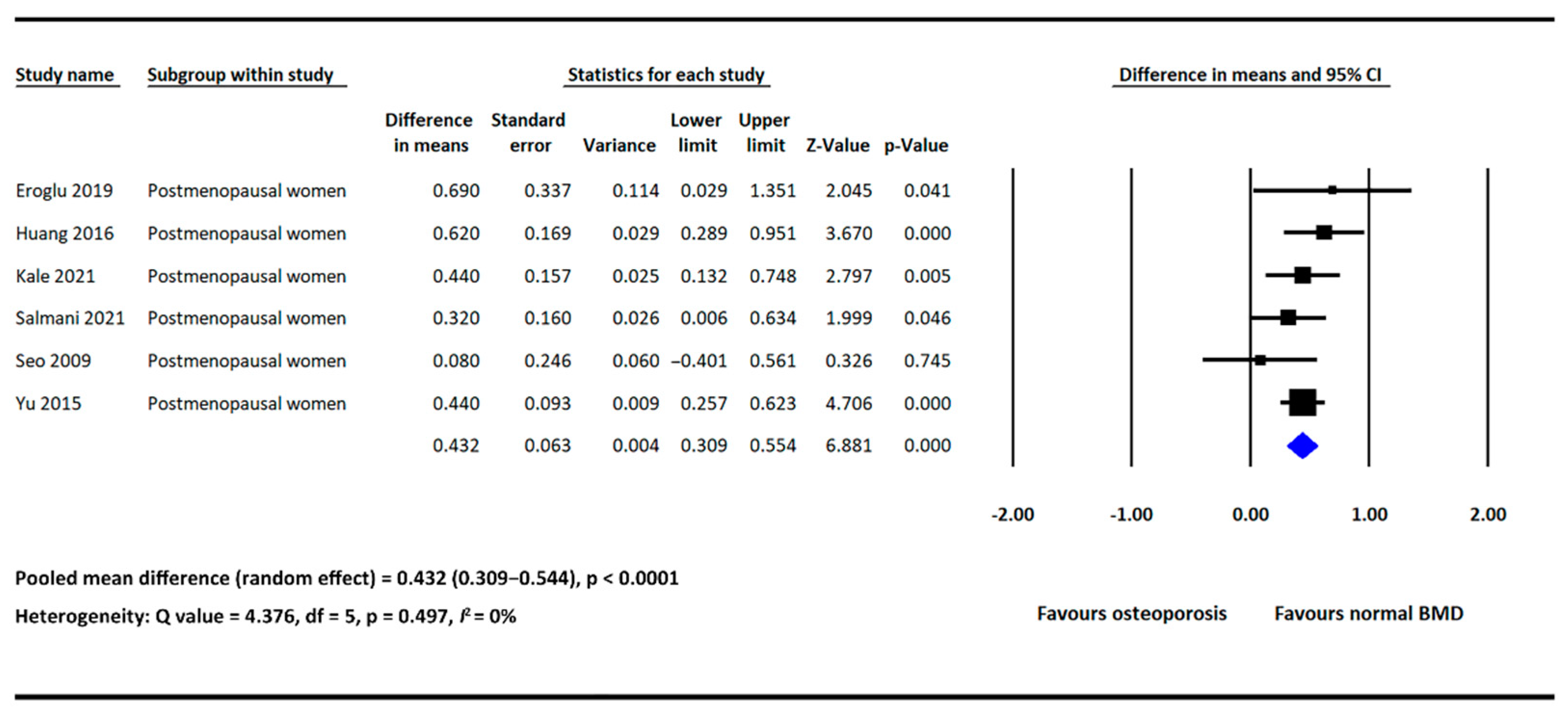
3.1.2. Subgroup Analysis
3.1.3. Meta Regression
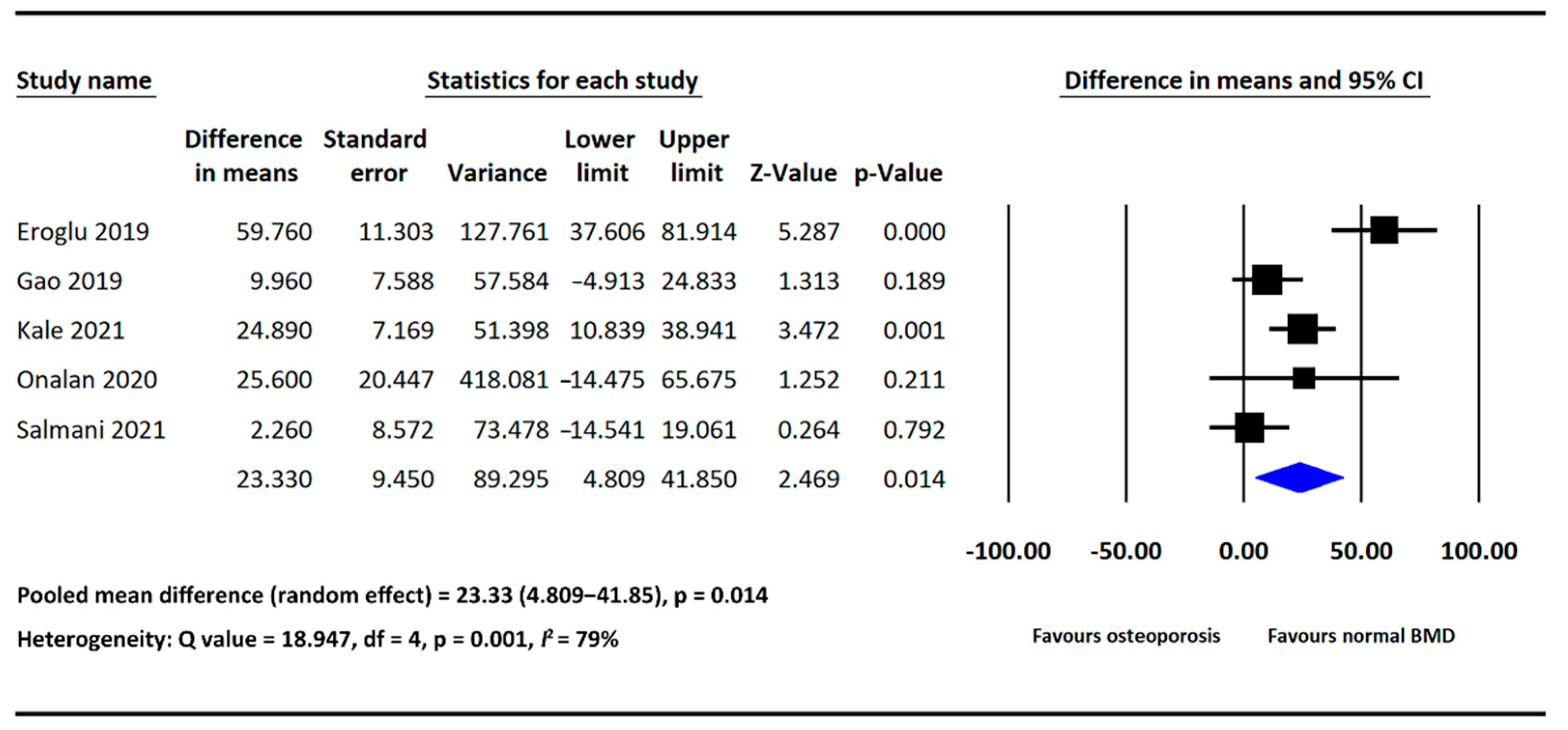
3.2. Association of PLR with Osteoporosis
Mean Difference in PLR between the Osteoporosis and Normal BMD Groups
3.3. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schultz, K.; Wolf, J.M. Emerging Technologies in Osteoporosis Diagnosis. J. Hand Surg. 2018, 44, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Sozen, T.; Ozisik, L.; Basaran, N.C. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef]
- Hernlund, E.; Svedbom, A.; Ivergård, M.; Compston, J.; Cooper, C.; Stenmark, J.; McCloskey, E.V.; Jönsson, B.; Kanis, J.A. Osteoporosis in the European Union: Medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch. Osteoporos. 2013, 8, 136. [Google Scholar] [CrossRef] [PubMed]
- Akkawi, I.; Zmerly, H. Osteoporosis: Current Concepts. Joints 2018, 6, 122–127. [Google Scholar] [CrossRef] [PubMed]
- McLean, R.R. Proinflammatory cytokines and osteoporosis. Curr. Osteoporos. Rep. 2009, 7, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Ginaldi, L.; Di Benedetto, M.C.; De Martinis, M. Osteoporosis, inflammation and ageing. Immun. Ageing 2005, 2, 14. [Google Scholar] [CrossRef]
- Mun, H.; Liu, B.; Pham, T.H.A.; Wu, Q. C-reactive protein and fracture risk: An updated systematic review and meta-analysis of cohort studies through the use of both frequentist and Bayesian approaches. Osteoporos. Int. 2020, 32, 425–435. [Google Scholar] [CrossRef]
- Lacativa, P.G.; Farias, M.L. Osteoporosis and inflammation. Arq. Bras. Endocrinol. Metabol. 2010, 54, 123–132. [Google Scholar] [CrossRef]
- Uslu, A.U.; Küçük, A.; Şahin, A.; Ugan, Y.; Yılmaz, R.; Güngör, T.; Bağcacı, S.; Küçükşen, S. Two new inflammatory markers associated with Disease Activity Score-28 in patients with rheumatoid arthritis: Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio. Int. J. Rheum. Dis. 2015, 18, 731–735. [Google Scholar] [CrossRef]
- Adami, G.; Fassio, A.; Rossini, M.; Caimmi, C.; Giollo, A.; Orsolini, G.; Viapiana, O.; Gatti, D. Osteoporosis in Rheumatic Diseases. Int. J. Mol. Sci. 2019, 20, 5867. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Luis Del Barrio, J.; Manuel Estrada, J.; Gil, Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef]
- Li, J.; Chen, Q.; Luo, X.; Hong, J.; Pan, K.; Lin, X.; Liu, X.; Zhou, L.; Wang, H.; Xu, Y.; et al. Neutrophil-to-Lymphocyte Ratio Positively Correlates to Age in Healthy Population. J. Clin. Lab. Anal. 2014, 29, 437–443. [Google Scholar] [CrossRef]
- Mertoglu, C.; Gunay, M. Neutrophil-Lymphocyte ratio and Platelet-Lymphocyte ratio as useful predictive markers of prediabetes and diabetes mellitus. Diabetes Metab. Syndr. 2017, 11, S127–S131. [Google Scholar] [CrossRef]
- Al Salmani, A.; Al Shidhani, A.; Al-Alawi, N.M.; Al Sulaimi, A.A.; Al-Hashemi, M.A. Inflammatory Markers as a Predictor of Postmenopausal Osteoporosis: A cross-sectional study from the Sultan Qaboos University Hospital. Sultan Qaboos Univ. Med. J. SQUMJ 2021, 22, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Eroglu, S.; Karatas, G. Platelet/lymphocyte ratio is an independent predictor for osteoporosis. Saudi Med. J. 2019, 40, 360–366. [Google Scholar] [CrossRef]
- Gao, K.; Zhu, W.; Liu, W.; Ma, D.; Li, H.; Yu, W.; Li, Q.; Cao, Y. The predictive role of monocyte-to-lymphocyte ratio in osteoporosis patient. Medicine 2019, 98, e16793. [Google Scholar] [CrossRef]
- Huang, C.; Li, S. Association of blood neutrophil lymphocyte ratio in the patients with postmenopausal osteoporosis. Pak. J. Med. Sci. 2016, 32, 762–765. [Google Scholar] [CrossRef]
- Kale, I. The predictive role of monocyte-lymphocyte ratio and platelet-lymphocyte ratio in postmenopausal osteoporosis. J. Clin. Investig. Surg. 2021, 6, 141–147. [Google Scholar] [CrossRef]
- Onalan, E.; Gokalp, Y. The relationship between bone mineral density and hematological parameters in the geriatric age group. Fam. Pract. Palliat. Care 2020, 5, 1–5. [Google Scholar]
- Öztürk, Z.A.; Yesil, Y.; Kuyumcu, M.E.; Bilici, M.; Öztürk, N.; Yeşil, N.K.; Özkaya, M.; Kısacık, B.; Kepekçi, Y.; Arıoğul, S. Inverse relationship between neutrophil lymphocyte ratio (NLR) and bone mineral density (BMD) in elderly people. Arch. Gerontol. Geriatr. 2013, 57, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Qin, Q.; Yan, S.; Yang, Y.; Chen, J.; Yan, H.; Li, T.; Gao, X.; Wang, Y.; Li, A.; Wang, S.; et al. The Relationship Between Osteoporosis and Intestinal Microbes in the Henan Province of China. Front. Cell Dev. Biol. 2021, 9, 752990. [Google Scholar] [CrossRef]
- Seo, S.K.; Cho, S.; Kim, H.Y.; Choi, Y.S.; Park, K.H.; Cho, D.J.; Lee, B.S. Bone mineral density, arterial stiffness, and coronary atherosclerosis in healthy postmenopausal women. Menopause 2009, 16, 937–943. [Google Scholar] [CrossRef]
- Yu, X.-Y.; Li, X.-S.; Li, Y.; Liu, T.; Wang, R.-T. Neutrophil–lymphocyte ratio is associated with arterial stiffness in postmenopausal women with osteoporosis. Arch. Gerontol. Geriatr. 2015, 61, 76–80. [Google Scholar] [CrossRef]
- Fischer, V.; Haffner-Luntzer, M. Interaction between bone and immune cells: Implications for postmenopausal osteoporosis. Semin. Cell Dev. Biol. 2021, 123, 14–21. [Google Scholar] [CrossRef]
- Ginaldi, L.; De Martinis, M. Osteoimmunology and Beyond. Curr. Med. Chem. 2016, 23, 3754–3774. [Google Scholar] [CrossRef]
- Tsukasaki, M.; Takayanagi, H. Osteoimmunology: Evolving concepts in bone–immune interactions in health and disease. Nat. Rev. Immunol. 2019, 19, 626–642. [Google Scholar] [CrossRef]
- Franceschi, C.; Campisi, J. Chronic inflammation (inflammaging) and its potential contribution to age-associated diseases. J. Gerontol. A Ser. Biol. Sci. Med. Sci. 2014, 69 (Suppl. 1), S4–S9. [Google Scholar] [CrossRef]
- Herrero-Cervera, A.; Soehnlein, O.; Kenne, E. Neutrophils in chronic inflammatory diseases. Cell. Mol. Immunol. 2022, 19, 177–191. [Google Scholar] [CrossRef] [PubMed]
- Koupenova, M.; Clancy, L.; Corkrey, H.A.; Freedman, J.E. Circulating Platelets as Mediators of Immunity, Inflammation, and Thrombosis. Circ. Res. 2018, 122, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Redlich, K.; Smolen, J.S. Inflammatory bone loss: Pathogenesis and therapeutic intervention. Nat. Rev. Drug Discov. 2012, 11, 234–250. [Google Scholar] [CrossRef]
- Valderrábano, R.J.; Lui, L.-Y.; Lee, J.; Cummings, S.R.; Orwoll, E.S.; Hoffman, A.R.; Wu, J.Y. Bone Density Loss Is Associated with Blood Cell Counts. J. Bone Miner. Res. 2017, 32, 212–220. [Google Scholar] [CrossRef]
- Zhang, J.; Niu, C.; Ye, L.; Huang, H.; He, X.; Tong, W.-G.; Ross, J.; Haug, J.; Johnson, T.; Feng, J.Q.; et al. Identification of the haematopoietic stem cell niche and control of the niche size. Nature 2003, 425, 836–841. [Google Scholar] [CrossRef] [PubMed]
- Calvi, L.M.; Adams, G.B.; Weibrecht, K.W.; Weber, J.M.; Olson, D.P.; Knight, M.C.; Martin, R.P.; Schipani, E.; Divieti, P.; Bringhurst, F.R.; et al. Osteoblastic cells regulate the haematopoietic stem cell niche. Nature 2003, 425, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Visnjic, D.; Kalajzic, Z.; Rowe, D.W.; Katavic, V.; Lorenzo, J.; Aguila, H.L. Hematopoiesis is severely altered in mice with an induced osteoblast deficiency. Blood 2004, 103, 3258–3264. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Yan, P.; Wan, Q.; Zhang, Z.; Xu, Y.; Miao, Y.; Yang, J. Association of circulating B-type natriuretic peptide with osteoporosis in a Chinese type 2 diabetic population. BMC Musculoskelet. Disord. 2021, 22, 261. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Country | Study Design | Sample (N) | Female (n, %) | Mean Age (Years) | Methodology for BMD Measurement; Site | Model |
|---|---|---|---|---|---|---|---|
| Eroglu et al., (2019) [18] | Turkey | cross-sectional | 140 | 140, 100% | 54.21 | DEXA; lumbar spine, total femur, femoral neck | NLR, PLR |
| Gao et al., (2019) [19] | China | cross-sectional | 210 | 119, 56.7% | 57.16 | DEXA; lumbar spine, femoral neck | NLR, PLR |
| Huang et al., (2016) [20] | China | cross-sectional | 173 | 173, 100% | 62.2 | DEXA; lumbar spine, left total femur | NLR |
| Kale et al., (2021) [21] | Turkey | cross-sectional | 74 | 74, 100% | 59.62 | DEXA; lumbar spine, femoral neck | NLR, PLR |
| Onalan et al., (2020) [22] | Turkey | cross-sectional | 215 | 177, 82.3% | 73.73 | DEXA; not declared | NLR, PLR |
| Ozturk et al., (2013) [23] | Turkey | cross-sectional | 1011 | 608, 60.1% | 72.63 | DEXA; lumbar spine, total femur, femoral neck | NLR |
| Qin et al., (2021) [24] | China | cross-sectional | 29 | 20, 69.0% | 59.96 | QCT; not declared | NLR |
| Salmani et al., (2021) [17] | Oman | cross-sectional | 286 | 286, 100% | 64.41 | DEXA; lumbar spine, pelvis, femoral neck | NLR, PLR |
| Seo et al., (2009) [25] | Korea | cross-sectional | 66 | 66, 100% | 56.53 | DEXA; lumbar spine, proximal femur | NLR |
| Yu et al., (2015) [26] | China | cross-sectional | 412 | 412, 100% | 74.95 | DEXA; lumbar spine, femoral neck | NLR |
| Moderators | Regression Coefficient | 95% CI, Lower Limit | 95% CI, Upper Limit | p Value |
|---|---|---|---|---|
| Age | −0.0083 | −0.0312 | 0.0146 | 0.478 |
| DM * | −0.1417 | −0.5044 | 0.2209 | 0.444 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.-C.; Yang, T.-I.; Huang, S.-W.; Kuo, Y.-J.; Chen, Y.-P. Associations of the Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio with Osteoporosis: A Meta-Analysis. Diagnostics 2022, 12, 2968. https://doi.org/10.3390/diagnostics12122968
Liu Y-C, Yang T-I, Huang S-W, Kuo Y-J, Chen Y-P. Associations of the Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio with Osteoporosis: A Meta-Analysis. Diagnostics. 2022; 12(12):2968. https://doi.org/10.3390/diagnostics12122968
Chicago/Turabian StyleLiu, Yu-Cheng, Tzu-I Yang, Shu-Wei Huang, Yi-Jie Kuo, and Yu-Pin Chen. 2022. "Associations of the Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio with Osteoporosis: A Meta-Analysis" Diagnostics 12, no. 12: 2968. https://doi.org/10.3390/diagnostics12122968