
A Meta-Analysis of Observational Studies on Prolactin Levels in Women with Polycystic Ovary Syndrome
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Result
3.1. Characteristics of Included Studies
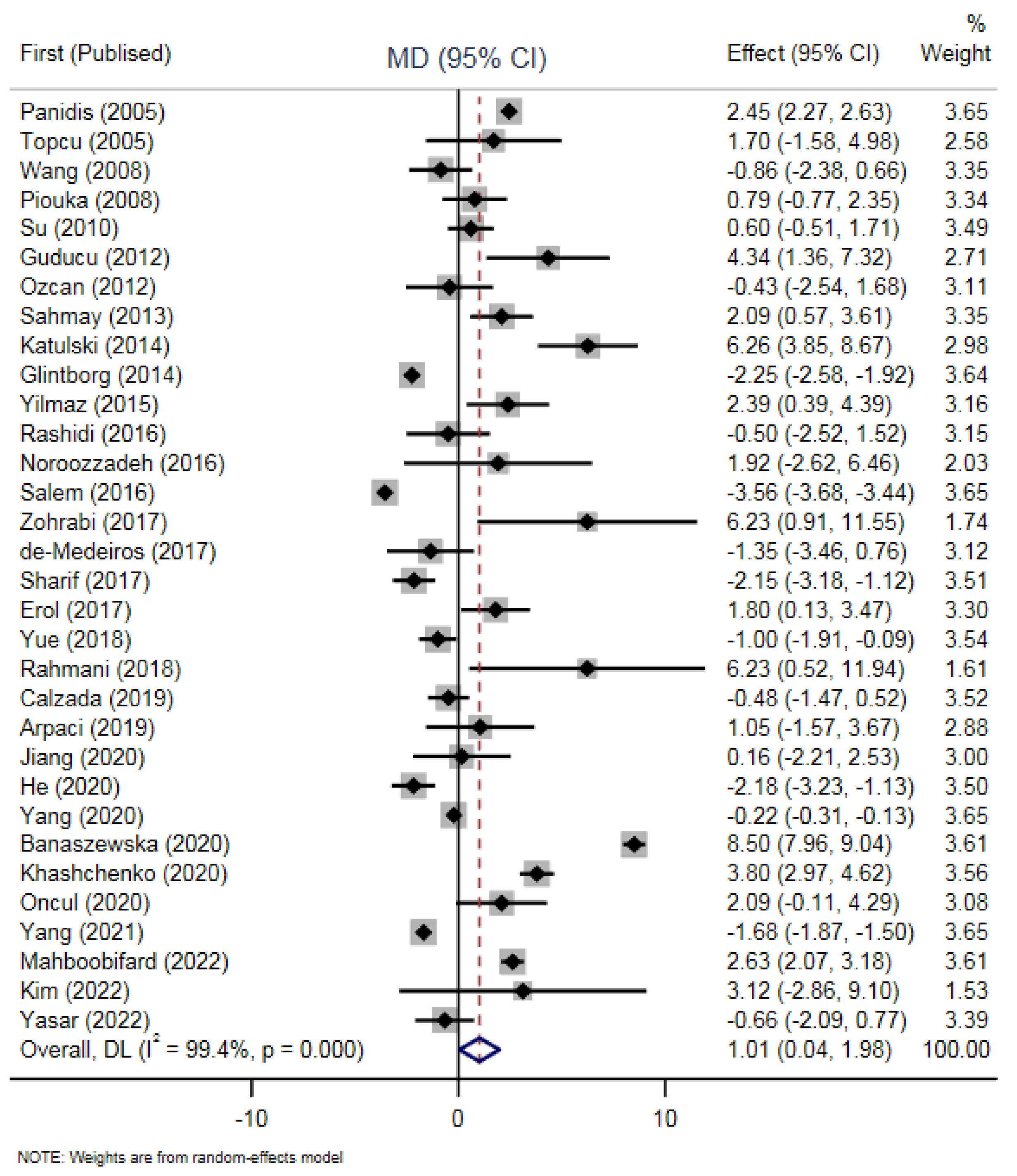
3.2. Differences in PRL Levels between PCOS Patients and Non-PCOS
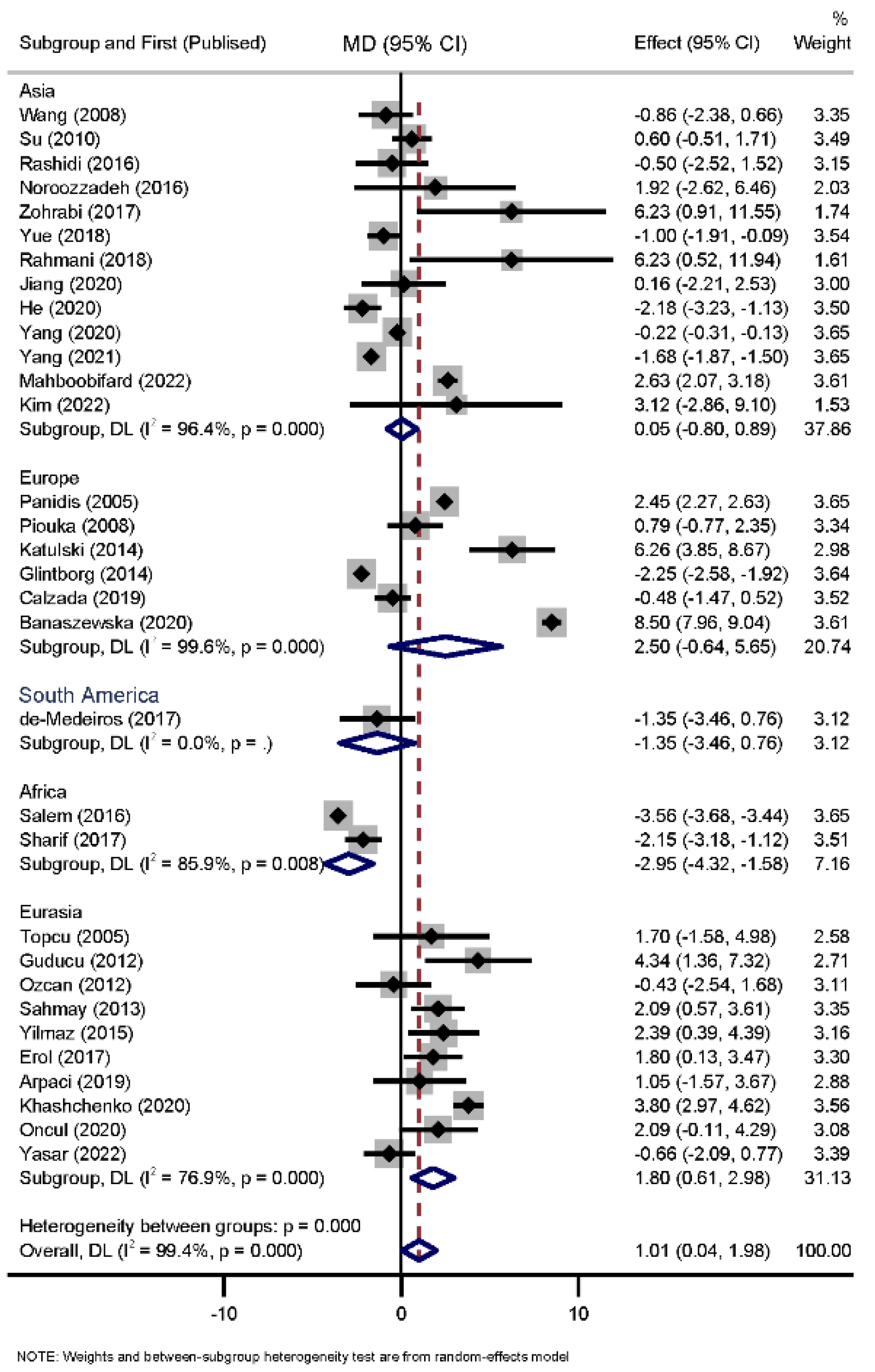
3.3. Sub-Grouped Meta-Analysis
3.4. Heterogeneity
3.5. Meta-Regression Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Barthelmess, E.K.; Naz, R.K. Polycystic ovary syndrome: Current status and future perspective. Front. Biosci. (Elite Ed.) 2014, 6, 104–119. [Google Scholar] [PubMed] [Green Version]
- Azziz, R. Polycystic Ovary Syndrome. Obstet. Gynecol. 2018, 132, 321–336. [Google Scholar] [CrossRef] [PubMed]
- Naz, M.S.G.; Tehrani, F.R.; Majd, H.A.; Ahmadi, F.; Ozgoli, G.; Fakari, F.R.; Ghasemi, V. The prevalence of polycystic ovary syndrome in adolescents: A systematic review and meta-analysis. Int. J. Reprod. Biomed. 2019, 17, 533–542. [Google Scholar]
- Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [CrossRef] [Green Version]
- Melmed, S.; Casanueva, F.F.; Hoffman, A.R.; Kleinberg, D.L.; Montori, V.M.; Schlechte, J.A.; Wass, J.A. Diagnosis and treatment of hyperprolactinemia: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 273–288. [Google Scholar] [CrossRef] [PubMed]
- Delcour, C.; Robin, G.; Young, J.; Dewailly, D. PCOS and Hyperprolactinemia: What do we know in 2019? Clin. Med. Insights Reprod. Health 2019, 13, 1179558119871921. [Google Scholar] [CrossRef] [Green Version]
- Coffler, M.S.; Patel, K.; Dahan, M.H.; Malcom, P.J.; Kawashima, T.; Deutsch, R.; Chang, R.J. Evidence for Abnormal Granulosa Cell Responsiveness to Follicle-Stimulating Hormone in Women with Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2003, 88, 1742–1747. [Google Scholar] [CrossRef]
- Hernández, I.; Parra, A.; Méndez, I.; Cabrera, V.; del Carmen Cravioto, M.; Mercado, M.; Larrea, F. Hypothalamic dopaminergic tone and prolactin bioactivity in women with polycystic ovary syndrome. Arch. Med. Res. 2000, 31, 216–222. [Google Scholar] [CrossRef]
- Glintborg, D.; Altinok, M.; Mumm, H.; Buch, K.; Ravn, P.; Andersen, M. Prolactin is associated with metabolic risk and cortisol in 1007 women with polycystic ovary syndrome. Hum. Reprod. 2014, 29, 1773–1779. [Google Scholar] [CrossRef] [Green Version]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar] [CrossRef]
- Singla, R.; Gupta, Y.; Khemani, M.; Aggarwal, S. Thyroid disorders and polycystic ovary syndrome: An emerging relationship. Indian J. Endocrinol. Metab. 2015, 19, 25. [Google Scholar] [CrossRef] [PubMed]
- Paulson, M.; Norstedt, G.; Sahlin, L.; Hirschberg, A.L. Association between prolactin receptor expression and proliferation in the endometrium of obese women with polycystic ovary syndrome. Gynecol. Endocrinol. 2020, 36, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Di, J.; Pan, J.; Yu, R.; Teng, Y.; Cai, Z.; Deng, X. The association between prolactin and metabolic parameters in pcos women: A retrospective analysis. Front. Endocrinol. 2020, 11, 263. [Google Scholar] [CrossRef] [PubMed]
- Mahboobifard, F.; Rahmati, M.; Amiri, M.; Azizi, F.; Tehrani, F.R. To what extent does polycystic ovary syndrome influence the cut-off value of prolactin? Findings of a community-based study. Adv. Med. Sci. 2022, 67, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Sahmay, S.; Atakul, N.; Aydogan, B.; Aydın, Y.; Imamoglu, M.; Seyisoglu, H. Elevated serum levels of anti-Müllerian hormone can be introduced as a new diagnostic marker for polycystic ovary syndrome. Acta Obstet. Gynecol. Scand. 2013, 92, 1369–1374. [Google Scholar] [CrossRef]
- Khashchenko, E.; Uvarova, E.; Vysokikh, M.; Ivanets, T.; Krechetova, L.; Tarasova, N.; Sukhikh, G. The relevant hormonal levels and diagnostic features of polycystic ovary syndrome in adolescents. J. Clin. Med. 2020, 9, 1831. [Google Scholar] [CrossRef]
- Calzada, M.; López, N.; Noguera, J.A.; Mendiola, J.; Hernández, A.I.; Corbalán, S.; Torres, A.M. AMH in combination with SHBG for the diagnosis of polycystic ovary syndrome. J. Obstet. Gynaecol. 2019, 39, 1130–1136. [Google Scholar] [CrossRef]
- Kim, G.-M.; Lee, J.A.; Park, S.W.; Lee, J.G.; Jeon, G.-H. Are plasma Brain-Derived Neurotrophic Factor or reproductive hormones related to depression in PCOS patients?: A prospective cohort study. Clin. Exp. Obstet. Gynecol. 2021, 48, 1146–1153. [Google Scholar]
- Jiang, Y.; Liu, Y.; Yu, Z.; Yang, P.; Zhao, S. Serum asprosin level in different subtypes of polycystic ovary syndrome: A cross-sectional study. Rev. Assoc. Med. Bras. 2021, 67, 590–596. [Google Scholar] [CrossRef]
- Erol, O.; Özel, M.K.; Ellidağ, H.Y.; Toptaş, T.; Derbent, A.U.; Yılmaz, N. Assessment of circulating betatrophin concentrations in lean glucose-tolerant women with polycystic ovary syndrome. J. Obstet. Gynaecol. 2017, 37, 633–638. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Research methods & reporting-Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement-David Moher and colleagues introduce PRISMA, an update of the QUOROM guidelines for reporting systematic reviews and meta-analyses. Ann. Intern. Med. 2009, 338, 332. [Google Scholar]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luchini, C.; Stubbs, B.; Solmi, M.; Veronese, N. Assessing the quality of studies in meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale. World J. Meta-Anal. 2017, 5, 80–84. [Google Scholar] [CrossRef]
- Ben Salem, A.; Megdich, F.; Kacem, O.; Souayeh, M.; Hachani Ben Ali, F.; Hizem, S.; Mahjoub, T. Vascular endothelial growth factor (VEGFA) gene variation in polycystic ovary syndrome in a Tunisian women population. BMC Genom. 2016, 17, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katulski, K.; Slawek, S.; Czyzyk, A.; Podfigurna-Stopa, A.; Paczkowska, K.; Ignaszak, N.; Meczekalski, B. Bone mineral density in women with polycystic ovary syndrome. J. Endocrinol. Investig. 2014, 37, 1219–1224. [Google Scholar] [CrossRef] [Green Version]
- Yasar, H.Y.; Demirpence, M.; Colak, A.; Zeytinli, M.; Yasar, E.; Taylan, A. Serum neudesin levels in patients with polycystic ovary syndrome. Ginekol. Pol. 2022, 93, 525–530. [Google Scholar]
- He, S.; Mao, X.; Lei, H.; Dong, B.; Guo, D.; Zheng, B.; Sun, P. Peripheral blood inflammatory-immune cells as a predictor of infertility in women with polycystic ovary syndrome. J. Inflamm. Res. 2020, 13, 441. [Google Scholar] [CrossRef]
- Yue, C.-Y.; Lu, L.; Li, M.; Zhang, Q.-L.; Ying, C.-M. Threshold value of anti-Mullerian hormone for the diagnosis of polycystic ovary syndrome in Chinese women. PLoS ONE 2018, 13, e0203129. [Google Scholar] [CrossRef]
- Oncul, M.; Albayrak, M.; Sozer, V.; Karakus, B.; Gelisgen, R.; Karatas, S.; Uzun, H. Polycystic ovary syndrome and endothelial dysfunction: A potential role for soluble lectin-like oxidized low density lipoprotein receptor-1. Reprod. Biol. 2020, 20, 396–401. [Google Scholar] [CrossRef]
- Su, H.-W.; Chen, C.-M.; Chou, S.-Y.; Liang, S.-J.; Hsu, C.-S.; Hsu, M.-I. Polycystic ovary syndrome or hyperprolactinaemia: A study of mild hyperprolactinaemia. Gynecol. Endocrinol. 2011, 27, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Sharif, M.E.; Adam, I.; Ahmed, M.A.; Rayis, D.A.; Hamdan, H.Z. Serum level of zinc and copper in Sudanese women with polycystic ovarian syndrome. Biol. Trace Elem. Res. 2017, 180, 23–27. [Google Scholar] [CrossRef]
- Panidis, D.; Balaris, C.; Farmakiotis, D.; Rousso, D.; Kourtis, A.; Balaris, V.; Diamanti-Kandarakis, E. Serum parathyroid hormone concentrations are increased in women with polycystic ovary syndrome. Clin. Chem. 2005, 51, 1691–1697. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, B.H.; Gorginzadeh, M.; Aalipour, S.; Sills, E.S. Age related endocrine patterns observed in polycystic ovary syndrome patients vs. ovulatory controls: Descriptive data from a university based infertility center. Arch. Endocrinol. Metab. 2016, 60, 486–491. [Google Scholar] [CrossRef] [Green Version]
- Noroozzadeh, M.; Tehrani, F.R.; Mobarakabadi, S.S.; Farahmand, M.; Dovom, M.R. Sexual function and hormonal profiles in women with and without polycystic ovary syndrome: A population-based study. Int. J. Impot. Res. 2017, 29, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Lin, J.; Li, H.; Liu, Z.; Chen, X.; Chen, Q. Prolactin Is Associated With Insulin Resistance and Beta-Cell Dysfunction in Infertile Women With Polycystic Ovary Syndrome. Front. Endocrinol. 2021, 12, 571229. [Google Scholar] [CrossRef]
- Piouka, A.; Farmakiotis, D.; Katsikis, I.; Macut, D.; Gerou, S.; Panidis, D. Anti-Mullerian hormone levels reflect severity of PCOS but are negatively influenced by obesity: Relationship with increased luteinizing hormone levels. Am. J. Physiol. Endocrinol. Metab. 2009, 296, E238–E243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yılmaz, S.A.; Altınkaya S, Ö.; Kebabçılar, A.; Kerimoğlu, Ö.S.; Pekin, A.T.; Abuşoğlu, S.; Ünlü, A. The relationship between polycystic ovary syndrome and vitamin D levels. Turk. J. Obstet. Gynecol. 2015, 12, 18. [Google Scholar] [CrossRef]
- Güdücü, N.; Işçi, H.; Yiğiter, A.B.; Dünder, I. C-reactive protein and lipoprotein-a as markers of coronary heart disease in polycystic ovary syndrome. J. Turk. Ger. Gynecol. Assoc. 2012, 13, 227–232. [Google Scholar] [CrossRef]
- Arpaci, H. Major determinants of circulating myostatin in polycystic ovary syndrome. Exp. Ther. Med. 2019, 17, 1383–1389. [Google Scholar] [CrossRef]
- Banaszewska, B.; Siakowska, M.; Chudzicka-Strugala, I.; Chang, R.J.; Pawelczyk, L.; Zwozdziak, B.; Duleba, A.J. Elevation of markers of endotoxemia in women with polycystic ovary syndrome. Hum. Reprod. 2020, 35, 2303–2311. [Google Scholar] [CrossRef]
- Zohrabi, M.; Rahmani, E.; Motamed, N.; Akbarzadeh, S. CXC Ligand 5 cytokine serum level in women with polycystic ovary syndrome and normal body mass index: A case-control study. Int. J. Reprod. BioMed. 2017, 15, 619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De-Medeiros, S.F.; Yamamoto, M.M.W.; de-Medeiros, M.A.S.; Barbosa, J.S.; Norman, R.J. Should Subclinical Hypothyroidism Be an Exclusion Criterion for the Diagnosis of Polycystic Ovary Syndrome? J. Reprod. Infertil. 2017, 18, 242–250. [Google Scholar] [PubMed]
- Wang, K.; Wang, L.; Zhao, Y.; Shi, Y.; Wang, L.; Chen, Z.J. No association of the Arg51Gln and Leu72Met polymorphisms of the ghrelin gene and polycystic ovary syndrome. Hum. Reprod. 2009, 24, 485–490. [Google Scholar] [CrossRef] [Green Version]
- Ozcan, A.; Yücel, A.; Noyan, V.; Sağsöz, N.; Cağlayan, O. Total and lipid bound sialic acid levels in patients with polycystic ovary syndrome. J. Turk. Ger. Gynecol. Assoc. 2012, 13, 79–84. [Google Scholar] [CrossRef]
- Rahmani, E.; Akbarzadeh, S.; Broomand, A.; Torabi, F.; Motamed, N.; Zohrabi, M. Serum levels of angiopoietin-like protein 2 and obestatin in iranian women with polycystic ovary syndrome and normal body mass index. J. Clin. Med. 2018, 7, 159. [Google Scholar] [CrossRef] [Green Version]
- Topcu, S.; Caliskan, M.; Ozcimen, E.E.; Tok, D.; Uckuyu, A.; Erdogan, D.; Muderrisoglu, H. Do young women with polycystic ovary syndrome show early evidence of preclinical coronary artery disease? Hum. Reprod. 2006, 21, 930–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernard, V.; Young, J.; Binart, N. Prolactin—A pleiotropic factor in health and disease. Nat. Rev. Endocrinol. 2019, 15, 356–365. [Google Scholar] [CrossRef]
- Serri, O.; Chik, C.L.; Ur, E.; Ezzat, S. Diagnosis and management of hyperprolactinemia. CMAJ 2003, 169, 575–581. [Google Scholar]
- Vilar, L.; Fleseriu, M.; Bronstein, M.D. Challenges and pitfalls in the diagnosis of hyperprolactinemia. Arq. Bras. Endocrinol. Metabol. 2014, 58, 9–22. [Google Scholar] [CrossRef] [Green Version]
- Wong, A.; Eloy, J.A.; Couldwell, W.T.; Liu, J.K. Update on prolactinomas. Part 1: Clinical manifestations and diagnostic challenges. J. Clin. Neurosci. 2015, 22, 1562–1567. [Google Scholar] [CrossRef]
- Shimatsu, A.; Hattori, N. Macroprolactinemia: Diagnostic, clinical, and pathogenic significance. Clin. Dev. Immunol. 2012, 2012, 167132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hattori, N.; Inagaki, C. Anti-prolactin (PRL) autoantibodies cause asymptomatic hyperprolactinemia: Bioassay and clearance studies of PRL-immunoglobulin G complex. J. Clin. Endocrinol. Metab. 1997, 82, 3107–3110. [Google Scholar] [CrossRef] [PubMed]
- Corenblum, B.; Taylor, P.J. The hyperprolactinemic polycystic ovary syndrome may not be a distinct entity. Fertil. Steril. 1982, 38, 549–552. [Google Scholar] [CrossRef]
- Işik, A.Z.; Gülekli, B.; Zorlu, G.; Ergin, T.; Gö kmen, O. Endocrinological and clinical analysis of hyperprolactinemic patients with and without ultrasonically diagnosed polycystic ovarian changes. Gynecol. Obstet. Investig. 1997, 43, 183–185. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Ganie, M.A. Idiopathic Hyperprolactinemia Presenting as Polycystic Ovary Syndrome in Identical Twin Sisters: A Case Report and Literature Review. Cureus 2018, 10, e3004. [Google Scholar] [CrossRef] [PubMed]
- Levine, S.; Muneyyirci-Delale, O. Stress-Induced Hyperprolactinemia: Pathophysiology and Clinical Approach. Obstet. Gynecol. Int. 2018, 2018, 9253083. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.J.; Jennes, L. Neural signals that regulate GnRH neurones directly during the oestrous cycle. Reproduction 2001, 122, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chaudhari, N.; Dawalbhakta, M.; Nampoothiri, L. GnRH dysregulation in polycystic ovarian syndrome (PCOS) is a manifestation of an altered neurotransmitter profile. Reprod. Biol. Endocrinol. 2018, 16, 37. [Google Scholar] [CrossRef]
- Kalro, B.N.; Loucks, T.L.; Berga, S.L. Neuromodulation in polycystic ovary syndrome. Obstet. Gynecol. Clin. N. Am. 2001, 28, 35–62. [Google Scholar] [CrossRef]
- Gómez, R.; Ferrero, H.; Delgado-Rosas, F.; Gaytan, M.; Morales, C.; Zimmermann, R.C.; Pellicer, A. Evidences for the existence of a low dopaminergic tone in polycystic ovarian syndrome: Implications for OHSS development and treatment. J. Clin. Endocrinol. Metab. 2011, 96, 2484–2492. [Google Scholar] [CrossRef] [Green Version]
- Onaka, T.; Takayanagi, Y.; Leng, G. Metabolic and stress-related roles of prolactin-releasing peptide. Trends Endocrinol. Metab. 2010, 21, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Damone, A.L.; Joham, A.E.; Loxton, D.; Earnest, A.; Teede, H.J.; Moran, L.J. Depression, anxiety and perceived stress in women with and without PCOS: A community-based study. Psychol. Med. 2019, 49, 1510–1520. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Garrido, M.A.; Tena-Sempere, M. Metabolic dysfunction in polycystic ovary syndrome: Pathogenic role of androgen excess and potential therapeutic strategies. Mol. Metab. 2020, 35, 100937. [Google Scholar] [CrossRef] [PubMed]
- Sobrinho, L.G.; Horseman, N.D. Prolactin and human weight disturbances: A puzzling and neglected association. Rev. Endocr. Metab. Disord. 2019, 20, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, J.J.; Kuppusamy, M.; Koshy, T.; Narayana, M.K.; Ramaswamy, P. Cortisol and polycystic ovarian syndrome–a systematic search and meta-analysis of case–control studies. Gynecol. Endocrinol. 2021, 37, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Curlewis, J.D. Seasonal prolactin secretion and its role in seasonal reproduction: A review. Reprod. Fertil. Dev. 1992, 4, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Steger, R.; Bartke, A.; Goldman, B.; Soares, M.; Talamantes, F. Effects of Short Photoperiod on the Ability of Golden Hamster Ptuitaries to Secrete Prolactin and Gonadotropins in Vitro. Biol. Reprod. 1983, 29, 872–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekinci, E.I.; Torkamani, N.; Ramchand, S.K.; Churilov, L.; Sikaris, K.A.; Lu, Z.X.; Houlihan, C.A. Higher maternal serum prolactin levels are associated with reduced glucose tolerance during pregnancy. J. Diabetes Investig. 2017, 8, 697–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Castro, L.F.; Dos Santos, Á.A.; Casulari, L.A.; Naves, L.A.; Amato, A.A. Association between variations of physiological prolactin serum levels and the risk of type 2 diabetes: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2020, 166, 108247. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Lu, J.; Xu, Y.; Li, M.; Sun, J.; Zhang, J.; Ning, G. Circulating prolactin associates with diabetes and impaired glucose regulation: A population-based study. Diabetes Care 2013, 36, 1974–1980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okoroh, E.M.; Hooper, W.C.; Atrash, H.K.; Yusuf, H.R.; Boulet, S.L. Prevalence of polycystic ovary syndrome among the privately insured, United States, 2003–2008. Am. J. Obstet. Gynecol. 2012, 207, 299.e1–299.e7. [Google Scholar] [CrossRef] [PubMed]
- Broekmans, F.; Knauff, E.; Valkenburg, O.; Laven, J.; Eijkemans, M.; Fauser, B. PCOS according to the Rotterdam consensus criteria: Change in prevalence among WHO-II anovulation and association with metabolic factors. BJOG 2006, 113, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Carmina, E. Diagnosis of polycystic ovary syndrome: From NIH criteria to ESHRE-ASRM guidelines. Minerva Ginecol. 2004, 56, 1–6. [Google Scholar] [PubMed]
- Kok, P.; Roelfsema, F.; Frolich, M.; Meinders, A.E.; Pijl, H. Prolactin Release is Enhanced in Proportion to Excess Visceral Fat in Obese Women. J. Clin. Endocrinol. Metab. 2004, 89, 4445–4449. [Google Scholar] [CrossRef]
- Sawin, C.T.; Carlson, H.E.; Geller, A.; Castelli, W.P.; Bacharach, P. Serum prolactin and aging: Basal values and changes with estrogen use and hypothyroidism. J. Gerontol. 1989, 44, M131–M135. [Google Scholar] [CrossRef]
- Roelfsema, F.; Pijl, H.; Keenan, D.M.; Veldhuis, J.D. Prolactin secretion in healthy adults is determined by gender, age and body mass index. PLoS ONE 2012, 7, e31305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharif, E.; Rahman, S.; Zia, Y.; Rizk, N.M. The frequency of polycystic ovary syndrome in young reproductive females in Qatar. Int. J. Womens Health 2017, 9, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakrabarti, J. Serum leptin level in women with polycystic ovary syndrome: Correlation with adiposity, insulin, and circulating testosterone. Ann. Med. Health Sci. Res. 2013, 3, 191. [Google Scholar] [CrossRef] [PubMed]
- Pedroso, D.C.C.; Miranda-Furtado, C.L.; Kogure, G.S.; Meola, J.; Okuka, M.; Silva, C.; dos Reis, R.M. Inflammatory biomarkers and telomere length in women with polycystic ovary syndrome. Fertil Steril. 2015, 103, 542–547.e2. [Google Scholar] [CrossRef]
- Higuchi, K.; Nawata, H.; Maki, T.; Higashizima, M.; Kato, K.-I.; Ibayashi, H. Prolactin has a direct effect on adrenal androgen secretion. J. Clin. Endocrinol. Metab. 1984, 59, 714–718. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| First Author, Year (Ref.) | Type of Study | Location | Sample Size | Participants Characteristics PCOS/Non-PCOS | PRL Levels | Assay Methods | Quality | ||
|---|---|---|---|---|---|---|---|---|---|
| PCOS | Control | PCOS | Control | ||||||
| Mahboobifard, 2022 [14] | cross-sectional | Iran | 216 | 702 | Age: 31.2 ± 7.9/34.9 ± 7.6 BMI: 26.7 ± 5.4/26.8 ± 5.1 | 16.1 (10.5–23.6) (ng/mL) | 13.4 (9.3–19.7) (ng/mL) | IRMA 1 | High |
| Calzada, 2019 [17] | case-control | Spain | 77 | 106 | Age: 27 (24–32)/29 (22–33) BMI: 25.3 (20.6–30.7)/21.6 (19.8–23.0) | 396.6 (290.5–515.0) (mIU/mL) | 371.0 (307.6–589.7) (mIU/mL) | chemiluminescent enzymatically two-site immunoassays | Moderate |
| Kim, 2021 [18] | cohort | Korea | 43 | 28 | Age: 24.91 ± 6.80/27.89 ± 9.57 BMI: 23.19 ± 4.67/21.94 ± 4.57 | 18.84 ± 15.86 (ng/mL) | 15.72 ± 9.84 (ng/mL) | Not clear | High |
| Salem, 2015 [24] | cross-sectional | Tunisia | 118 | 150 | Age: 29.8 ± 0.4/33.5 ± 0.5 BMI: 28.4 ± 0.7/23.1 ± 0.2 | 73.1 ± 11.7 (mU/L) | 148.8 ± 9.4 (mU/L) | Not clear | Moderate |
| Katulski, 2016 [25] | case-control | Poland | 69 | 30 | Age: 23.13 ± 4.43/24.53 ± 2.67 BMI: 23.07 ± 5.9/21.93 ± 1.23 | 14.98 ± 9.09 (ng/mL) | 8.72 ±3.07 (ng/mL) | electrochemiluminescence immunoassay | Moderate |
| Yasar, 2022 [26] | cross-sectional | Turkey | 180 | 100 | Age: 25.94 ± 6.18/28.12 ± 7.27 BMI: 29.77 ± 6.65/28.04 ± 6.16 | 11.44 ± 5.02 (ng/mL) | 12.10 ± 6.25 (ng/mL) | chemiluminescent method | High |
| Sahmay, 2013 [15] | cross-sectional | Turkey | 419 | 151 | Age: 25.82 ± 5.3/26.62 ±5 BMI: 25.43 ± 4.6/25.4 ± 4.4 | 18.85 ±8.79 (ng/mL) | 16.76 ± 7.96 (ng/mL) | Not clear | Moderate |
| Glintborg, 2014 [9] | cross-sectional | Denmark | 1007 | 116 | Age:30 (23–36)/28 (24–37) BMI:27.4 (23.2–33.0)/25 (22.3–29.2) | 7 (5–10) (μg/L) | 9 (7–13) (μg/L) | two-site commercial kit | Moderate |
| Jiang, 2020 [19] | cross-sectional | China | 93 | 77 | Age: 28.60 ± 3.78/26.62 ± 5 BMI: 24.95 ± 4.05/22.30±3.69 | 16.82 ± 8.88 (ng/mL) | 16.66 ± 6.85 (ng/mL) | electrochemiluminescence | Moderate |
| Erol, 2017 [20] | case-control | Turkey | 60 | 50 | Age: 24.7 ± 3.9/25.8 ± 4.4 BMI: 21.9 ± 1.7/21.8 ± 2.1 | 12.3 ± 5.1 (ng/mL) | 10.5 ± 3.8 (ng/mL) | immunoenzymatic methods | Moderate |
| Khashchenko, 2020 [16] | case-control | Russia | 130 | 30 | Age: 24.7 ± 3.9/25.8 ± 4.4 BMI: 21.9 ± 1.7/21.8 ± 2.1 | 266.0 (175.0–405.0) (mIU/L) | 189.0 (142.0–269.0) (mIU/L) | electro- and immunochemiluminiscent methods | Moderate |
| He, 2020 [27] | case-control | China | 175 | 196 | Age: 30.69 ± 1.7/ 31.00± 1.74 BMI: 21.63 ± 1.23/21.14± 1.14 | 16.79 ± 4.12 ng/mL | 18.79 ± 2.92 ng/mL | radioimmunoassay | High |
| Yue, 2018 [28] | case-control | China | 653 | 118 | Age: 26.9 ± 4.2/27.3 ± 4.1 BMI: 26.2 ± 5.2/25.5 ± 5.6 | 11 ± 4.9 (ng/mL) | 12 ± 4.6 (ng/mL) | Beckman Coulter DxI800 | Moderate |
| Oncul, 2020 [29] | case-control | Turkey | 46 | 46 | Age: 24.2 ± 3.6/25.9 ± 4.9 BMI: 27.4 (15.7–38.9)/24.8 (17.6–33.1) | 16.87 ± 6.26 ng/mL | 14.78 ± 4.31 ng/mL | Electrochemiluminescence method | High |
| Yang, 2020 [13] | cross-sectional | China | 2052 | 9696 | Age: 29.12 ± 0.63/30.95 ± 0.66 BMI: 22.8 ± 1.2/21.18 ± 1.03 | 11.71 ± 1.92 (mIU/L) | 11.93 ± 2.01 (mIU/L) | chemiluminescence assay | Moderate |
| SU, 2010 [30] | case-control | Taiwan | 266 | 107 | Age: 26.2 + 5.4/29.5 + 6.2 BMI: 25.5 + 6.3/22.1 + 5.1 | 13.5 ± 4.8 (ng/mL) | 12.9 ± 5.0 (ng/mL) | EIA 2 | High |
| Sharif, 2017 [31] | case-control | Sudan | 50 | 50 | Age: 26.9 (5.2)/27.1 (4.8) BMI: 28.4 (4.2)/25.6 (5.7) | 12.0 (9.9–17.2) mIU/L | 13.9 (10.7–21.2) mIU/L | immunoassay | High |
| Panidis, 2005 [32] | case-control | Greece | 291 | 109 | Age:23.45 ± 0.54/26.74 ± 0.96 BMI:25.51 ± 0.24/25.84 ± 0.505 | 15.34 ± 0.84 (ng/mL) | 12.89 ± 0.83 (ng/mL) | RIA | Moderate |
| Rashidi, 2016 [33] | cohort | Iran | 595 | 157 | Age: 26.94 (4.57)/29.96 (5.91) BMI: 22.27 (4.91)/25.83 (4.45) | 14.75 ± 11.79 (ng/mL) | 15.25 ±11.4 (ng/mL) | radioimmunoassay | High |
| Noroozzadeh, 2016 [34] | cross-sectional | Iran | 63 | 216 | Age: 33.6 ± 7.2/36.3 ± 6.9 BMI: 27.14 ± 5.74/27.35 ± 4.95 | 16.98 ± 17.66 (pg/mL) | 15.06 ± 9.57 (pg/mL) | IRMA 3 | High |
| Yang, 2021 [35] | cross-sectional | China | 792 | 700 | Age: 29 (27–32.5)/31 (28–35) BMI:23.73 (21.48-26.85)/21.64 (19.53–23.88) | 235.74 (186.85–318.03) (mIU/L) | 275.13 (213.60–355.84) (mIU/L) | chemiluminescence | High |
| Piouka, 2008 [36] | case-control | Greece | 200 | 100 | Age:25.18 ± 5.42/26.8 ± 4.65 BMI:26.475 ± 2.8/26.4 ± 3.05 | 14.54 ± 6.72 ng/mL | 13.75 ± 6.4 ng/mL | RIA | Moderate |
| Yilmaz, 2015 [37] | case-control | Turkey | 84 | 56 | Age:22.55 ± 3.45/ 23.5 ± 4.4 | 15.79 ± 7.34 | 13.40 ± 4.85 | Not clear | Moderate |
| Güdücü, 2012 [38] | cross-sectional | Turkey | 62 | 40 | Age: 24.77 ± 4.85/28.13 ± 5.66 BMI: 24.15 ± 5.35/23.35 ± 5.33 | 20.87 ± 9.21 (ng/mL) | 16.53 ± 6.16 (ng/mL) | Not clear | High |
| Arpaci, 2019 [39] | case-control | Turkey | 46 | 42 | Age: 24.89 ± 6.11/29.02 ± 6.85 BMI: 25.34 ± 5.54/25.00 ± 4.79 | 13.20 ± 5.52 (ng/mL) | 12.15 ± 6.87 (ng/mL) | CMIA 4 | Moderate |
| Banaszewska, 2020 [40] | case-control | Poland | 62 | 42 | Age: 27.5 ± 0.6/29.1 ± 0.7 BMI: 25.4 ± 0.8/23.3 ± 0.6 | 22.5 ± 1.6 (ng/mL) | 14.0 ± 1.2 (ng/mL) | electrochemiluminescence assays | High |
| Zohrabi, 2017 [41] | case-control | Iran | 30 | 30 | Age: 25.85 ± 5.90/28.91 ± 8.1 BMI: 24.91 ± 3.63/24.02 ± 5.60 | 21.23 ± 11.94 (ng/mL) | 15.00 ± 8.84 (ng/mL) | enzymatic techniques | Moderate |
| deMedeiros, 2017 [42] | case-control | Brazil | 462 | 232 | Age: 26.72 ± 5.38/30.34 ± 4.74 BMI: 29.11 ± 6.74/24.47 ± 4.03 | 558.02 ± 293.24 (nmol/L) | 627.69 ± 287.7 (nmol/L) | electrochemiluminescence assay no bach | Moderate |
| Wang, 2008 [43] | case-control | China | 271 | 296 | Age: 28.84 ± 3.40/29.28 + 3.70 BMI: 24.98 + 4.06/22.19 + 3.03 | 17.70 ± 9.13 (μg/L) | 18.56 ± 9.38 (μg/L) | chemiluminescence immunization | Moderate |
| Özcan, 2012 [44] | case-control | Turkey | 40 | 35 | Age: 22.80 ± 2.70/23.82 ± 1.79 BMI: 27.94 ± 6.78/21.59 ± 2.68 | 15.5 2± 5.07 (ng/mL) | 15.95 ± 4.25 (ng/mL) | electrochemilluminescence immunoassay | Moderate |
| Rahmani, 2018 [45] | case-control | Iran | 26 | 26 | Age: 25.85 ± 5.90/28.91 ± 8.1 BMI: 24.91± 3.63/24.02 ±5.60 | 21.23 ± 11.94 (ng/mL) | 15.00 ± 8.84 (ng/mL) | ELISA 5 | High |
| Topcu, 2005 [46] | case-control | Turkey | 28 | 26 | Age: 27.1 ± 4.5/28.8 ± 4.4 BMI: 26.6 ± 5.7/24.7 ± 3.7 | 15.5 ± 7.7 | 13.8 ± 4.2 | chemiluminescent enzymeimmunoassay | High |
| Outcome | Group | Variable * | Regression Coefficient (95% CI) | p-Value |
|---|---|---|---|---|
| PRL | PCOS | Age | −0.21 (−0.91, 0.48) | 0.536 |
| BMI | −0.61 (−1.71, 0.48) | 0.264 | ||
| Europe | 1.49 (−4.54, 7.52) | 0.609 | ||
| Africa | −6.51 (−13.08, 0.05) | 0.052 | ||
| South America | 13.40 (−16.71, 0.43) | 0.351 | ||
| Eurasia | 1.31 (−2.90, 5.53) | 0.524 | ||
| Non-PCOS | Age | 0.07 (−0.35, 0.49) | 0.732 | |
| BMI | 0.05 (−0.82, 0.93) | 0.901 | ||
| Europe | −1.36 (−4.44, 1.70) | 0.360 | ||
| Africa | −5.07 (−10.21, 0.06) | 0.053 | ||
| America | 13.71 (−10.75, 38.19) | 0.246 | ||
| Eurasia | −2.16 (−5.60, 1.26) | 0.204 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saei Ghare Naz, M.; Mousavi, M.; Mahboobifard, F.; Niknam, A.; Ramezani Tehrani, F. A Meta-Analysis of Observational Studies on Prolactin Levels in Women with Polycystic Ovary Syndrome. Diagnostics 2022, 12, 2924. https://doi.org/10.3390/diagnostics12122924
Saei Ghare Naz M, Mousavi M, Mahboobifard F, Niknam A, Ramezani Tehrani F. A Meta-Analysis of Observational Studies on Prolactin Levels in Women with Polycystic Ovary Syndrome. Diagnostics. 2022; 12(12):2924. https://doi.org/10.3390/diagnostics12122924
Chicago/Turabian StyleSaei Ghare Naz, Marzieh, Maryam Mousavi, Fatemeh Mahboobifard, Atrin Niknam, and Fahimeh Ramezani Tehrani. 2022. "A Meta-Analysis of Observational Studies on Prolactin Levels in Women with Polycystic Ovary Syndrome" Diagnostics 12, no. 12: 2924. https://doi.org/10.3390/diagnostics12122924