
Platelet-to-White Blood Cell Ratio: A Feasible Biomarker for Pyogenic Liver Abscess

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Treatment Protocol
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Analysis of Factors Related to a Low PWR in Patients with PLA
3.3. Analysis of Risk Factors for Complications of PLA
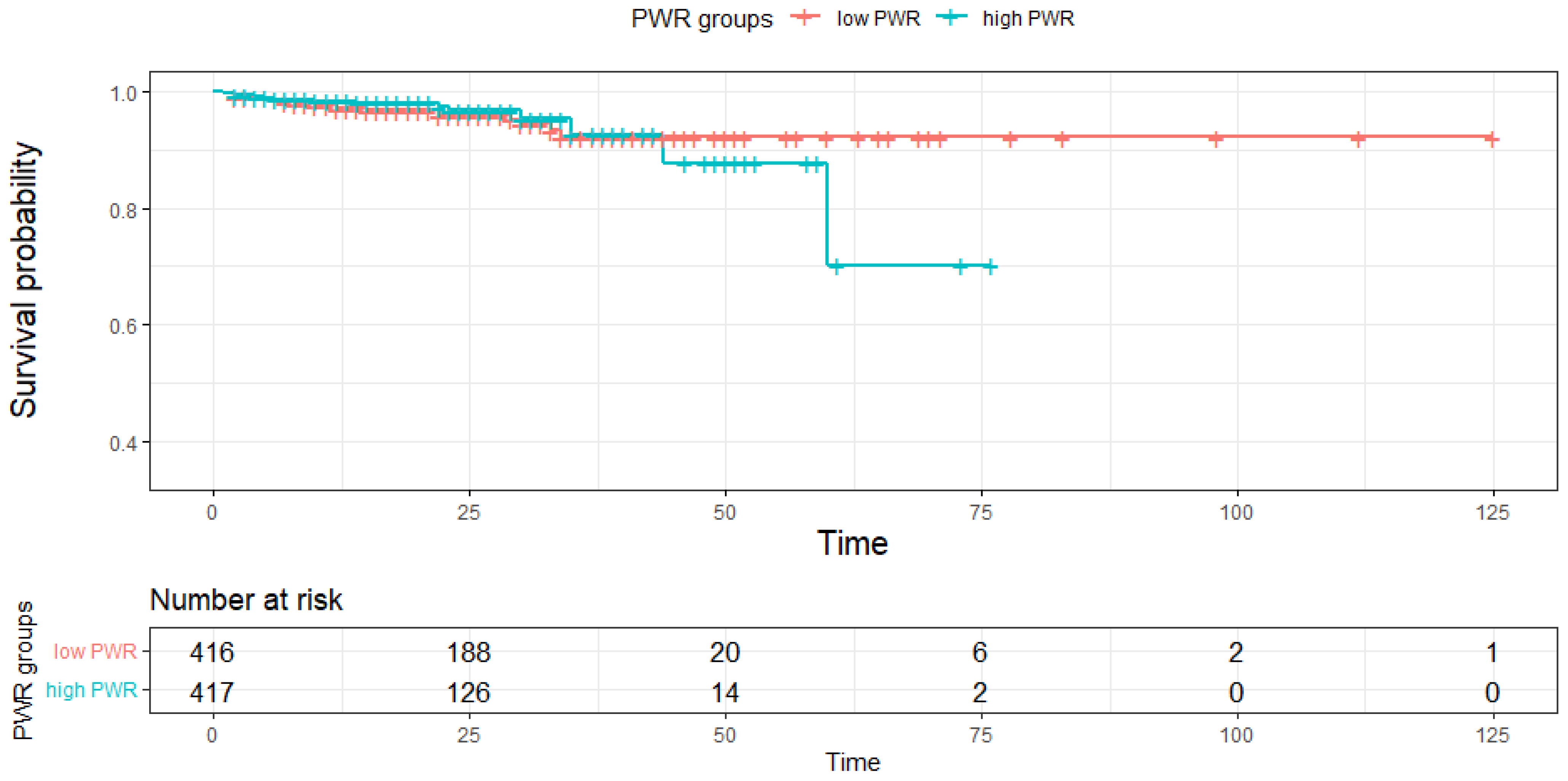
3.4. Comparison of the Mortality Rate and Hospital Stay between PWR Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meddings, L.; Myers, R.P.; Hubbard, J.; Shaheen, A.A.; Laupland, K.B.; Dixon, E.; Coffin, C.; Kaplan, G.G. A population-based study of pyogenic liver abscesses in the United States: Incidence, mortality, and temporal trends. Am. J. Gastroenterol. 2010, 105, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Mohsen, A.H.; Green, S.T.; Read, R.C.; McKendrick, M.W. Liver abscess in adults: Ten years experience in a UK centre. Qjm 2002, 95, 797–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, G.G.; Gregson, D.B.; Laupland, K.B. Population-based study of the epidemiology of and the risk factors for pyogenic liver abscess. Clin. Gastroenterol. Hepatol. 2004, 2, 1032–1038. [Google Scholar] [CrossRef]
- Jepsen, P.; Vilstrup, H.; Schønheyder, H.C.; Sørensen, H.T. A nationwide study of the incidence and 30-day mortality rate of pyogenic liver abscess in Denmark, 1977–2002. Aliment. Pharmacol. Ther. 2005, 21, 1185–1188. [Google Scholar] [CrossRef] [PubMed]
- Tian, L.T.; Yao, K.; Zhang, X.Y.; Zhang, Z.D.; Liang, Y.J.; Yin, D.L.; Lee, L.; Jiang, H.C.; Liu, L.X. Liver abscesses in adult patients with and without diabetes mellitus: An analysis of the clinical characteristics, features of the causative pathogens, outcomes and predictors of fatality: A report based on a large population, retrospective study in China. Clin. Microbiol. Infect. 2012, 18, E314–E330. [Google Scholar] [CrossRef] [Green Version]
- Tsai, F.C.; Huang, Y.T.; Chang, L.Y.; Wang, J.T. Pyogenic liver abscess as endemic disease, Taiwan. Emerg. Infect. Dis. 2008, 14, 1592–1600. [Google Scholar] [CrossRef]
- Yoo, J.J.; Lee, T.K.; Kyoung, D.S.; Park, M.A.; Kim, S.G.; Kim, Y.S. A population-based study of pyogenic liver abscess in Korea: Incidence, mortality and temporal trends during 2007–2017. Liver Int. 2021, 41, 2747–2758. [Google Scholar] [CrossRef]
- Pearce, N.W.; Knight, R.; Irving, H.; Menon, K.; Prasad, K.R.; Pollard, S.G.; Lodge, J.P.; Toogood, G.J. Non-operative management of pyogenic liver abscess. HPB 2003, 5, 91–95. [Google Scholar] [CrossRef] [Green Version]
- Kuo, S.H.; Lee, Y.T.; Li, C.R.; Tseng, C.J.; Chao, W.N.; Wang, P.H.; Wong, R.H.; Chen, C.C.; Chen, S.C.; Lee, M.C. Mortality in Emergency Department Sepsis score as a prognostic indicator in patients with pyogenic liver abscess. Am. J. Emerg. Med. 2013, 31, 916–921. [Google Scholar] [CrossRef]
- Webb, G.J.; Chapman, T.P.; Cadman, P.J.; Gorard, D.A. Pyogenic liver abscess. Frontline Gastroenterol. 2014, 5, 60–67. [Google Scholar] [CrossRef]
- Chen, Y.C.; Lin, C.H.; Chang, S.N.; Shi, Z.Y. Epidemiology and clinical outcome of pyogenic liver abscess: An analysis from the National Health Insurance Research Database of Taiwan, 2000–2011. J. Microbiol. Immunol. Infect. 2016, 49, 646–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, J.H.; Kim, Y.J.; Jun, Y.H.; Kim, S.I.; Kang, J.Y.; Suk, K.T.; Kim, D.J. Liver abscess due to Klebsiella pneumoniae: Risk factors for metastatic infection. Scand. J. Infect. Dis. 2014, 46, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Kim, J.H.; Jung, J.H.; Kim, S.E.; Kim, H.S.; Jeong, H.; Suk, K.T.; Jang, M.K.; Kim, D.J.; Lee, M.S.; et al. A Multicenter Retrospective Study on Clinical Characteristics and Outcome of Pyogenic Liver Abscess Focusing Multidrug-Resistant Organisms. J. Clin. Med. 2022, 11, 1114. [Google Scholar] [CrossRef] [PubMed]
- Roediger, R.; Lisker-Melman, M. Pyogenic and Amebic Infections of the Liver. Gastroenterol Clin. North. Am. 2020, 49, 361–377. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Graubard, B.I.; Rabkin, C.S.; Engels, E.A. Neutrophil-to-lymphocyte ratio and mortality in the United States general population. Sci. Rep. 2021, 11, 464. [Google Scholar] [CrossRef]
- Yousefi, B.; Sanaie, S.; Ghamari, A.A.; Soleimanpour, H.; Karimian, A.; Mahmoodpoor, A. Red Cell Distribution Width as a Novel Prognostic Marker in Multiple Clinical Studies. Indian J. Crit. Care Med. Peer-Rev. Off. Publ. Indian Soc. Crit. Care Med. 2020, 24, 49–54. [Google Scholar] [CrossRef]
- Sakin, A.; Secmeler, S.; Arici, S.; Geredeli, C.; Yasar, N.; Demir, C.; Aksaray, F.; Cihan, S. Prognostic Significance of Mean Platelet Volume on Local Advanced Non-Small Cell Lung Cancer Managed with Chemoradiotherapy. Sci. Rep. 2019, 9, 3959. [Google Scholar] [CrossRef] [Green Version]
- Korniluk, A.; Koper-Lenkiewicz, O.M.; Kamińska, J.; Kemona, H.; Dymicka-Piekarska, V. Mean Platelet Volume (MPV): New Perspectives for an Old Marker in the Course and Prognosis of Inflammatory Conditions. Mediat. Inflamm. 2019, 2019, 9213074. [Google Scholar] [CrossRef] [Green Version]
- Amalia, L.; Dalimonthe, N.Z. Clinical significance of Platelet-to-White Blood Cell Ratio (PWR) and National Institute of Health Stroke Scale (NIHSS) in acute ischemic stroke. Heliyon 2020, 6, e05033. [Google Scholar] [CrossRef]
- Lathouras, K.; Panagakis, G.; Bowden, S.J.; Saliaris, K.; Saso, S.; Haidopoulos, D.; Fotopoulou, C. Diagnostic value of post-operative platelet-to-white blood cell ratio after splenectomy in patients with advanced ovarian cancer. Int. J. Gynecol. Cancer 2019, 29, 1292–1297. [Google Scholar] [CrossRef]
- Jie, Y.; Gong, J.; Xiao, C.; Zhu, S.; Zhou, W.; Luo, J.; Chong, Y.; Hu, B. Low Platelet to White Blood Cell Ratio Indicates Poor Prognosis for Acute-On-Chronic Liver Failure. BioMed Res. Int. 2018, 2018, 7394904. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Qiu, Y.; He, X.; Mao, W.; Han, Z. Platelet-to-white blood cell ratio: A novel and promising prognostic marker for HBV-associated decompensated cirrhosis. J. Clin. Lab. Anal. 2020, 34, e23556. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, S.E.; Song, D.S.; Kim, H.Y.; Yoon, E.L.; Kim, T.H.; Jung, Y.K.; Suk, K.T.; Jun, B.G.; Yim, H.J.; et al. Platelet-to-White Blood Cell Ratio Is Associated with Adverse Outcomes in Cirrhotic Patients with Acute Deterioration. J. Clin. Med. 2022, 11, 2463. [Google Scholar] [CrossRef] [PubMed]
- Gong, Z.J.; Cheng, J.W.; Gao, P.T.; Huang, A.; Sun, Y.F.; Zhou, K.Q.; Hu, B.; Qiu, S.J.; Zhou, J.; Fan, J.; et al. Clinical Characteristics and Prognostic Factors of Patients with Intrahepatic Cholangiocarcinoma with Fever: A Propensity Score Matching Analysis. Oncol. 2019, 24, 997–1007. [Google Scholar] [CrossRef] [Green Version]
- Weng, J.; Brown, C.V.; Rhee, P.; Salim, A.; Chan, L.; Demetriades, D.; Velmahos, G.C. White blood cell and platelet counts can be used to differentiate between infection and the normal response after splenectomy for trauma: Prospective validation. J. Trauma 2005, 59, 1076–1080. [Google Scholar] [CrossRef]
- Jesri, A.; Okonofua, E.C.; Egan, B.M. Platelet and White Blood Cell Counts Are Elevated in Patients With the Metabolic Syndrome. J. Clin. Hypertens. 2005, 7, 705–711. [Google Scholar] [CrossRef]
- Shelat, V.G.; Chia, C.L.; Yeo, C.S.; Qiao, W.; Woon, W.; Junnarkar, S.P. Pyogenic Liver Abscess: Does Escherichia Coli Cause more Adverse Outcomes than Klebsiella Pneumoniae? World J. Surg. 2015, 39, 2535–2542. [Google Scholar] [CrossRef]
- Chen, S.C.; Huang, C.C.; Tsai, S.J.; Yen, C.H.; Lin, D.B.; Wang, P.H.; Chen, C.C.; Lee, M.C. Severity of disease as main predictor for mortality in patients with pyogenic liver abscess. Am. J. Surg. 2009, 198, 164–172. [Google Scholar] [CrossRef]
- Chou, F.F.; Sheen-Chen, S.M.; Chen, Y.S.; Chen, M.C.; Chen, F.C.; Tai, D.I. Prognostic factors for pyogenic abscess of the liver. J. Am. Coll. Surg. 1994, 179, 727–732. [Google Scholar]
- Huang, C.J.; Pitt, H.A.; Lipsett, P.A.; Osterman, F.A., Jr.; Lillemoe, K.D.; Cameron, J.L.; Zuidema, G.D. Pyogenic hepatic abscess. Changing trends over 42 years. Ann. Surg 1996, 223, 600–609. [Google Scholar] [CrossRef]
- Yin, D.; Ji, C.; Zhang, S.; Wang, J.; Lu, Z.; Song, X.; Jiang, H.; Lau, W.Y.; Liu, L. Clinical characteristics and management of 1572 patients with pyogenic liver abscess: A 12-year retrospective study. Liver Int. 2021, 41, 810–818. [Google Scholar] [CrossRef]
- Karki, A.; Riley, L.; Mehta, H.J.; Ataya, A. Abdominal etiologies of pleural effusion. Dis Mon. 2019, 65, 95–103. [Google Scholar] [CrossRef]
- Chen, S.C.; Lee, Y.T.; Yen, C.H.; Lai, K.C.; Jeng, L.B.; Lin, D.B.; Wang, P.H.; Chen, C.C.; Lee, M.C.; Bell, W.R. Pyogenic liver abscess in the elderly: Clinical features, outcomes and prognostic factors. Age Ageing 2009, 38, 271–276. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Wang, T.; Fang, Y.; Wang, M.; Liu, W.; Zhao, J.; Wang, B.; Wu, Z.; Lv, Y.; Wu, R. Clinical Significance of Serum Albumin/Globulin Ratio in Patients With Pyogenic Liver Abscess. Front. Surg. 2021, 8, 677799. [Google Scholar] [CrossRef]
- Lee, C.H.; Jo, H.G.; Cho, E.Y.; Song, J.S.; Jung, G.M.; Cho, Y.K.; Seo, S.Y.; Kim, S.H.; Kim, S.W.; Lee, S.O.; et al. Maximal diameter of liver abscess independently predicts prolonged hospitalization and poor prognosis in patients with pyogenic liver abscess. BMC Infect. Dis. 2021, 21, 171. [Google Scholar] [CrossRef]
- Carter, R.; Brewer, L.A., III. Subphrenic abscess: A thoracoabdominal clinical complex: The changing picture with antibiotics. Am. J. Surg 1964, 108, 165–174. [Google Scholar] [CrossRef]
- McDonald, B.; Dunbar, M. Platelets and Intravascular Immunity: Guardians of the Vascular Space During Bloodstream Infections and Sepsis. Front. Immunol. 2019, 10, 2400. [Google Scholar] [CrossRef]
- Vandijck, D.M.; Blot, S.I.; De Waele, J.J.; Hoste, E.A.; Vandewoude, K.H.; Decruyenaere, J.M. Thrombocytopenia and outcome in critically ill patients with bloodstream infection. Heart Lung 2010, 39, 21–26. [Google Scholar] [CrossRef]
- Wang, Z.; Ren, J.; Liu, Q.; Li, J.; Wu, X.; Wang, W.; Wu, J.; Wang, G.; Li, J. Hypermucoviscous Klebsiella pneumoniae infections induce platelet aggregation and apoptosis and inhibit maturation of megakaryocytes. Thromb. Res. 2018, 171, 45–54. [Google Scholar] [CrossRef]
- Wiedermann, C.J. Hypoalbuminemia as Surrogate and Culprit of Infections. Int. J. Mol. Sci. 2021, 22, 4496. [Google Scholar] [CrossRef]
- Aranda-Michel, E.; Bianco, V.; Kilic, A.; Sultan, I. Hypoalbuminemia in patients undergoing transcatheter aortic valve replacement: Culprit or surrogate? J. Thorac. Dis. 2019, 11, S1346–S1348. [Google Scholar] [CrossRef]
- Chan, K.S.; Chia, C.T.W.; Shelat, V.G. Demographics, Radiological Findings, and Clinical Outcomes of Klebsiella pneumonia vs. Non-Klebsiella pneumoniae Pyogenic Liver Abscess: A Systematic Review and Meta-Analysis with Trial Sequential Analysis. Pathogens 2022, 11, 976. [Google Scholar] [CrossRef]
- Quillet, L.; Guilley, H.; Jonard, G.; Richards, K. In vitro synthesis of biologically active beet necrotic yellow vein virus RNA. Virology 1989, 172, 293–301. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical Characteristics | Total (n = 833) | Low PWR (n = 416) | High PWR (n = 417) | p Value |
|---|---|---|---|---|
| Age (years) | 62.2 ± 15.4 | 64.1 ± 14.9 | 60.4 ± 15.6 | <0.001 |
| Male, n (%) | 536 (64.3) | 278 (66.8) | 258 (61.9) | 0.14 |
| BMI, kg/m2 | 23.9 ± 3.4 | 24.0 ± 3.4 | 23.8 ± 3.4 | 0.44 |
| Diabetes mellitus, n (%) | 218 (26.2) | 107 (25.7) | 111 (26.6) | 0.77 |
| Hypertension, n (%) | 306 (36.7) | 168 (40.4) | 138 (33.1) | 0.03 |
| Laboratory finding | ||||
| Anemia, n (%) | 313 (37.6) | 134 (32.2) | 179 (42.9) | 0.001 |
| WBC (×103) | 13.0 ± 6.5 | 15.4 ± 7.0 | 10.5 ± 5.0 | <0.001 |
| Platelet count (×103) | 234.7 ± 14.1 | 157.6 ± 80.7 | 311.6 ± 146.5 | <0.001 |
| AST, IU/L | 105.4 ± 311.6 | 126.5 ± 394.7 | 84.4 ± 194.5 | 0.051 |
| ALT, IU/L | 86.0 ± 121.7 | 96.0 ± 115.9 | 76.0 ± 126.5 | 0.02 |
| ALP, IU/L | 249.0 ± 239.5 | 237.6 ± 229.4 | 260.4 ± 249.0 | 0.17 |
| Albumin, g/dL | 3.4 ± 0.6 | 3.3 ± 0.6 | 3.5 ± 0.6 | <0.001 |
| PT-INR | 1.3 ± 0.1 | 1.4 ± 2.3 | 1.3 ± 0.7 | 0.33 |
| Cr, mg/dL | 1.4 ± 4.1 | 1.5 ± 4.2 | 1.2 ± 3.8 | 0.18 |
| CRP, mg/dL | 184.4 ± 250.1 | 206.8 ± 91.3 | 161.9 ± 340.7 | 0.01 |
| Abscess size, cm | 5.4 ± 2.8 | 5.4 ± 2.6 | 5.3 ± 3.1 | 0.71 |
| Abscess location, n (%) | ||||
| Right | 527 (63.3) | 248 (59.6) | 279 (66.9) | 0.03 |
| Left | 172 (20.6) | 100 (24.0) | 72 (17.3) | 0.02 |
| Both | 134 (16.1) | 68 (16.3) | 66 (15.8) | 0.84 |
| Complications, n (%) | 181 (21.7) | 124 (29.8) | 57 (13.7) | <0.001 |
| Metastatic infection | 88 (48.6) | 63 (50.8) | 25 (43.9) | 0.0014 |
| Septic endophthalmitis | 15 (8.3) | 12 (9.7) | 3 (5.3) | 0.02 |
| Pneumonia | 29 (16.0) | 22 (17.7) | 7 (12.3) | 0.004 |
| Other metastatic infection | 44 (24.3) | 29 (23.4) | 15 (26.3) | 0.0019 |
| Abscess rupture | 8 (4.4) | 5 (4.0) | 3 (5.3) | 0.48 |
| Pleural effusion | 85 (47.0) | 56 (45.2) | 29 (50.9) | 0.0019 |
| Causative organisms, n (%) | ||||
| K. pneumoniae | 400 (48.0) | 234 (56.3) | 166 (39.8) | <0.001 |
| E. coli | 59 (7.1) | 34 (8.2) | 25 (6.0) | 0.22 |
| Others | 163 (19.6) | 27 (6.5) | 31 (7.4) | <0.001 |
| Not identified | 211 (25.3) | 121 (29.1) | 195 (46.8) | <0.001 |
| Variable | Univariate | p Value | Multivariate | p Value |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | |||
| Older age (≥65 years) | 1.567 (1.192–2.061) | 0.0013 | 1.918 (1.330–2.780) | <0.001 |
| Male | 0.805 (0.606–1.070) | 0.136 | ||
| Hypertension | 1.370 (1.033–1.819) | 0.029 | 1.224 (0.857–1.750) | 0.266 |
| DM | 0.955 (0.701–1.300) | 0.768 | ||
| Location of the abscess (Right) | 1.646 (0.975–2.830) | 0.065 | ||
| Abscess size, cm | 1.009 (0.962–1.059) | 0.710 | ||
| Anemia | 0.634 (0.477–0.841) | <0.001 | 0.423 (0.288–0.615) | <0.001 |
| Albumin, g/dL | 0.575 (0.449–0.731) | <0.001 | 0.617 (0.447–0.844) | <0.001 |
| AST, IU/L | 1.001 (1.0001–1.002) | <0.001 | 0.9998(0.998–1.002) | 0.820 |
| ALT, IU/L | 1.0016 (1.0003–1.003) | 0.024 | 1.0007 (0.998–1.004) | 0.657 |
| ALP, IU/L | 0.9995(0.9990–1.0001) | 0.170 | ||
| PT-INR | 1.057 (0.961–1.307) | 0.412 | ||
| Cr, mg/dL | 1.034 (0.991–1.131) | 0.274 | ||
| CRP, mg/dL | 1.003 (1.002–1.004) | <0.001 | 1.0005 (0.999–1.002) | <0.001 |
| Causative organisms | ||||
| K. pneumoniae | 1.944 (1.477–2.564) | <0.001 | 0.829 (0.531–1.291) | 0.410 |
| E. coli | 1.396 (0.820–2.405) | 0.222 | ||
| Others | 1.093 (0.706–1.696) | 0.690 | ||
| Not identified | 0.406 (0.291–0.565) | <0.001 | 0.545 (0.334–0.883) | 0.014 |
| Variable | Univariate | p Value | Multivariate | p Value |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | |||
| Low PWR (<17.05) | 2.591 (1.607–4.293) | <0.001 | 1.953 (1.163–3.364) | 0.013 |
| Older age (≥65 years) | 1.425 (0.907–2.255) | 0.126 | ||
| Hypertension | 1.192 (0.747–1.883) | 0.454 | ||
| Diabetes mellitus | 0.934 (0.544–1.546) | 0.797 | ||
| Abscess location (Right) | 0.839 (0.531–1.338) | 0.454 | ||
| Abscess size, cm | 1.017 (0.939–1.098) | 0.672 | ||
| Anemia | 0.521 (0.304–0.857) | 0.013 | 0.609 (0.339–1.052) | 0.084 |
| Albumin, g/dL | 0.719 (0.489–1.056) | 0.093 | ||
| AST, IU/L | 1.000 (0.999–1.0006) | 0.764 | ||
| ALT, IU/L | 1.000 (0.999–1.002) | 0.467 | ||
| ALP, IU/L | 1.000 (0.999–1.001) | 0.826 | ||
| PT-INR | 0.938 (0.467–1.090) | 0.722 | ||
| Cr, mg/dL | 0.994 (0.868–1.039) | 0.854 | ||
| CRP, mg/dL | 1.000 (0.9997–1.001) | 0.21 | ||
| Causative organisms | ||||
| K. pneumoniae | 2.221 (1.396–3.601) | 0.0009 | 1.304 (0.688–2.625) | 0.433 |
| E. coli | 0.296 (0.048–0.974) | 0.095 | ||
| Others | 1.183 (0.572–2.245) | 0.627 | ||
| Not identified | 0.459 (0.231–0.843) | 0.018 | 0.648 (0.279–1.496) | 0.307 |
| Variable | Univariate | p Value | Multivariate | p Value |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | |||
| Low PWR (<17.05) | 2.081 (1.310–3.371) | 0.002 | 2.007 (1.204–3.419) | 0.0087 |
| Older age (≥65 years) | 1.121 (0.715–1.759) | 0.617 | ||
| Hypertension | 0.881 (0.543–1.401) | 0.598 | ||
| Diabetes mellitus | 0.794 (0.454–1.331) | 0.399 | ||
| Abscess location (Right) | 1.641(1.008–2.757) | 0.527 | ||
| Abscess size, cm | 1.141 (1.060–1.227) | <0.001 | 1.077 (0.986–1.173) | 0.095 |
| Anemia | 1.627 (1.034–2.555) | 0.034 | 1.237 (0.733–2.075) | 0.422 |
| Albumin, g/dL | 0.462 (0.312–0.679) | <0.001 | 0.736 (0.461–1.175) | 0.198 |
| AST, IU/L | 1.0001 (0.9993–1.0006) | 0.613 | ||
| ALT, IU/L | 1.0008 (0.9992–1.002) | 0.251 | ||
| ALP, IU/L | 1.001 (1.0005–1.002) | <0.001 | 1.001 (1.000–1.002) | 0.006 |
| PT-INR | 1.017 (0.838–1.113) | 0.751 | ||
| Cr, mg/dL | 0.937 (0.690–1.031) | 0.571 | ||
| CRP, mg/dL | 1.0001 (0.998–1.0008) | 0.679 | ||
| Causative organisms | ||||
| K. pneumoniae | 1.459 (0.931–2.305) | 0.101 | ||
| E. coli | 2.168 (1.031–4.214) | 0.030 | 1.362 (0.592–2.906) | 0.443 |
| Others | 1.538 (0.799–2.787) | 0.174 | ||
| Not identified | 0.345 (0.167–0.640) | 0.002 | 0.458 (0.218–0.883) | 0.027 |
| Variable | Univariate | p Value | Multivariate | p Value |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | |||
| Low PWR (<17.05) | 2.422 (1.774–3.325) | <0.001 | 1.573 (1.053–2.357) | 0.027 |
| Older age (≥65 years) | 1.265 (0.934–1.715) | 0.13 | ||
| Male | 1.226 (0.893–1.694) | 0.211 | ||
| Hypertension | 1.147 (0.838–1.577) | 0.395 | ||
| Diabetes mellitus | 1.309 (0.923–1.877) | 0.137 | ||
| Abscess location (Right) | 0.850 (0.617–1.163) | 0.313 | ||
| Abscess size, cm | 1.253 (1.176–1.339) | <0.001 | 1.094 (1.011–1.186) | 0.028 |
| Anemia | 1.452 (1.057–2.008) | 0.022 | 1.285 (0.826–1.971) | 0.254 |
| Albumin, g/dL | 0.457 (0.343–0.602) | <0.001 | 0.788 (0.547–1.125) | 0.195 |
| AST, IU/L | 0.9997 (0.9991–1.0002) | 0.279 | ||
| ALT, IU/L | 1.0007 (0.9993–1.002) | 0.369 | ||
| ALP, IU/L | 1.002 (1.001–1.003) | <0.001 | 1.002 (1.0007–1.003) | 0.002 |
| PT-INR | 1.020 (0.933–1.245) | 0.724 | ||
| Cr, mg/dL | 1.033 (0.982–1.175) | 0.44 | ||
| CRP, mg/dL | 1.008 (1.007–1.010) | <0.001 | 1.005 (1.003–1.008) | <0.001 |
| Causative organisms | ||||
| K. pneumoniae | 2.678 (1.951-3.702) | <0.001 | 1.519 (0.885–2.578) | 0.124 |
| E. coli | 1.423 (0.776-2.791) | 0.276 | ||
| Others | 1.041 (0.642–1.738) | 0.874 | ||
| Not identified | 0.287 (0.202–0.408) | <0.001 | 0.604 (0.351–1.026) | 0.064 |
| Variable | Univariate | p Value | Multivariate | p Value |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | |||
| Low PWR (<17.05) | 1. 912 (1.396–2.631) | <0.001 | 1.738 (1.211–2.507) | 0.003 |
| Elderly age (≥65 years) | 1.561 (1.144–2.135) | 0.005 | 1.447 (1.007–2.082) | 0.003 |
| Male | 1.400 (1.018–1.922) | 0.038 | 1.477 (1.028–2.082) | 0.035 |
| Hypertension | 1.151 (0.835–1.580) | 0.387 | ||
| Diabetes mellitus | 1.375 (0.974–1.931) | 0.067 | ||
| Abscess location (Right) | 0.992 (0.721–1.371) | 0.963 | ||
| Abscess size, cm | 1.163 (1.101–1.229) | <0.001 | 1.114 (1.045–1.189) | 0.001 |
| Anemia | 1.226 (0.892–1.682) | 0.207 | ||
| Albumin, g/dL | 0.437 (0.328–0.578) | <0.001 | 0.689 (0.490–0.964) | 0.031 |
| AST. IU/L | 1.0001 (0.999–1.0007) | 0.463 | ||
| ALT, IU/L | 1.001 (1.000–1.003) | 0.043 | 1.001 (0.999–1.003) | 0.061 |
| ALP, IU/L | 1.001 (1.0006–1.002) | <0.001 | 1.001 (1.000–1.002) | 0.016 |
| PT-INR | 0.942 (0.661–1.057) | 0.57 | ||
| Cr, mg/dL | 0.997 (0.939–1.033) | 0.877 | ||
| CRP, mg/dL | 1.0009 (0.999–1.002) | 0.235 | ||
| Causative organisms | ||||
| K. pneumoniae | 1.643 (1.203–2.248) | 0.002 | 1.086 (0.698–1.703) | 0.717 |
| E. coli | 1.630 (0.919–2.818) | 0.086 | ||
| Others | 1.263 (0.778–2.007) | 0.333 | ||
| Not identified | 0.403 (0.264–0.601) | <0.001 | 0.569 (0.332–0.971) | 0.039 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ko, D.-G.; Park, J.-W.; Kim, J.-H.; Jung, J.-H.; Kim, H.-S.; Suk, K.-T.; Jang, M.-K.; Park, S.-H.; Lee, M.-S.; Kim, D.-J.; et al. Platelet-to-White Blood Cell Ratio: A Feasible Biomarker for Pyogenic Liver Abscess. Diagnostics 2022, 12, 2556. https://doi.org/10.3390/diagnostics12102556
Ko D-G, Park J-W, Kim J-H, Jung J-H, Kim H-S, Suk K-T, Jang M-K, Park S-H, Lee M-S, Kim D-J, et al. Platelet-to-White Blood Cell Ratio: A Feasible Biomarker for Pyogenic Liver Abscess. Diagnostics. 2022; 12(10):2556. https://doi.org/10.3390/diagnostics12102556
Chicago/Turabian StyleKo, Dong-Gyun, Ji-Won Park, Jung-Hee Kim, Jang-Han Jung, Hyoung-Su Kim, Ki-Tae Suk, Myoung-Kuk Jang, Sang-Hoon Park, Myung-Seok Lee, Dong-Joon Kim, and et al. 2022. "Platelet-to-White Blood Cell Ratio: A Feasible Biomarker for Pyogenic Liver Abscess" Diagnostics 12, no. 10: 2556. https://doi.org/10.3390/diagnostics12102556