


The Usefulness of Magnetic Resonance Imaging (MRI) for the Detection of Local Recurrence after Mastectomy with Reconstructive Surgery in Breast Cancer Patients

Abstract
:1. Introduction
2. Materials and Methods
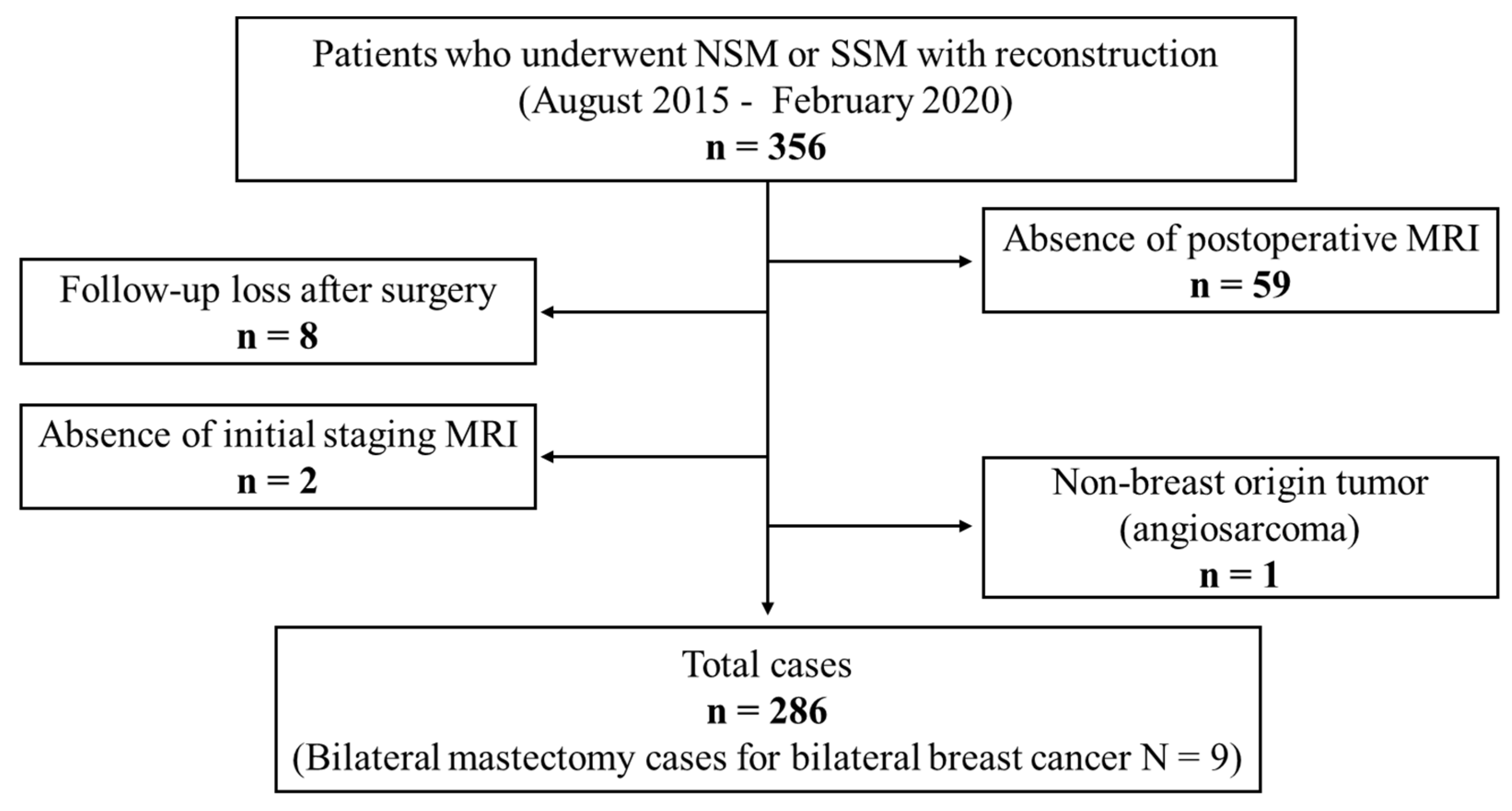
2.1. Subjective
2.2. Clinicopathologic Information
2.3. MRI Protocols
2.4. Imaging Surveillance after Surgery
2.5. Imaging Analysis of Primary Cancer and Recurrent Lesions
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Patients
3.2. Imaging Characteristics of Primary Breast Cancer
3.3. Characteristics of the Recurrent Lesions
3.3.1. Lesion Detectability Rates of the Imaging Modalities for Symptomatic Recurrence
3.3.2. Lesion Detectability Rates of the Imaging Modalities for Asymptomatic Recurrence
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | Surgery | Surveillance | Characteristics of Primary Cancer | Adjuvant Therapy | Imaging Characteristics | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case Number | Lesion Number | Age | Mastectomy | Reconstruction | Detection Modality | Follow-Up Period (Months) | Histology | Grade | ER 8 | PR 9 | HER2 10 | Stage | Chemotherapy | Endocrine | Target Agent | Early Kinetics | Delay Kinetics | Size (cm) |
| No. 1 | No. 1 † | 29 | NSM 1 | implant | Targeted US 3 | 51 | IDC, NST | 2 | + 11 | + | − 12 | IA | no | yes | no | fast | washout | 0.6 |
| No. 2 | No. 2 | 53 | NSM | flap | MRI | 29 | Metaplastic | 3 | + | − | − | IA | yes | yes | no | fast | plateau | 1.1 |
| No. 3 | No. 3 | 47 | NSM | flap | MRI | 48 | IDC 5, NST 6 | 2 | + | + | + | IIIA | yes | yes | yes | fast | washout | 0.5 |
| No. 4 | NSM | flap | MRI | 48 | IDC, NST | 2 | + | + | + | yes | yes | yes | medium | persistent | 0.3 | |||
| No. 4 | No. 5 | 47 | NSM | flap | US | 35 | IDC, NST | 2 | − | − | + | IA | no | no | no | fast | washout | 1.1 |
| No. 5 | No. 6 | 42 | NSM | implant | MRI 4 | 39 | IDC, NST | 3 | + | + | − | IA | no | yes | no | fast | washout | 0.9 |
| No. 6 | No. 7 | 46 | SSM 2 | flap | MRI | 49 | IDC, NST | 2 | + | + | − | IIA | no | yes | no | fast | plateau | 0.6 |
| No. 7 | No. 8 | 38 | NSM | flap | MRI | 48 | IDC, NST | 2 | + | + | − | IIB | yes | yes | no | fast | plateau | 0.9 |
| No. 8 | No. 9 | 26 | SSM | implant | US | 36 | Mucinous | 2 | + | + | − | IA | no | yes | no | fast | washout | 0.8 |
| No. 10 | SSM | implant | MRI | 36 | Mucinous | 2 | + | + | − | IA | no | yes | no | fast | washout | 0.5 | ||
| No. 9 | No. 11 | 36 | NSM | implant | US | 25 | DCIS 7 | 2 | + | + | + | 0 | yes | yes | no | fast | washout | 0.7 |
| No. 12 | NSM | implant | MRI | 25 | DCIS | 2 | + | + | + | 0 | yes | yes | no | fast | plateau | 0.4 | ||
| No. 13 | NSM | implant | US | 25 | DCIS | 2 | + | + | + | 0 | yes | yes | no | fast | washout | 0.4 | ||
| No. 10 | No. 14 | 40 | SSM | implant | US | 29 | IDC, NST | 3 | − | − | + | 0 | no | no | no | fast | plateau | 1 |
| No. 11 | No. 15 | 44 | SSM | flap | MRI | 25 | IDC, NST | 2 | + | − | IIA | no | yes | no | fast | plateau | 0.9 | |

References
- Jung, K.W.; Won, Y.J.; Kong, H.J.; Lee, E.S. Prediction of Cancer Incidence and Mortality in Korea, 2019. Cancer Res. Treat. 2019, 51, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.Y.; Lee, S.B.; Kim, Y.S.; Kim, Z.; Kim, H.Y.; Kim, H.J.; Park, S.; Bae, S.Y.; Yoon, K.; Lee, S.K.; et al. Breast Cancer Statistics in Korea, 2018. J. Breast Cancer 2021, 24, 123–137. [Google Scholar] [CrossRef] [PubMed]
- Cemal, Y.; Albornoz, C.R.; Disa, J.J.; McCarthy, C.M.; Mehrara, B.J.; Pusic, A.L.; Cordeiro, P.G.; Matros, E. A paradigm shift in U.S. breast reconstruction: Part 2. The influence of changing mastectomy patterns on reconstructive rate and method. Plast. Reconstr. Surg. 2013, 131, 320e–326e. [Google Scholar] [CrossRef]
- Kummerow, K.L.; Du, L.; Penson, D.F.; Shyr, Y.; Hooks, M.A. Nationwide trends in mastectomy for early-stage breast cancer. JAMA Surg. 2015, 150, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Song, W.J.; Kang, S.G.; Kim, E.K.; Song, S.Y.; Lee, J.S.; Lee, J.H.; Jin, U.S. Current status of and trends in post-mastectomy breast reconstruction in Korea. Arch. Plast. Surg. 2020, 47, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Mariscotti, G.; Durando, M.; Houssami, N.; Berzovini, C.M.; Esposito, F.; Fasciano, M.; Campanino, P.P.; Bosco, D.; Bussone, R.; Ala, A.; et al. Preoperative MRI evaluation of lesion-nipple distance in breast cancer patients: Thresholds for predicting occult nipple-areola complex involvement. Clin. Radiol. 2018, 73, 735–743. [Google Scholar] [CrossRef]
- Hudson, D.A.; Skoll, P.J. Single-stage, autologous breast restoration. Plast. Reconstr. Surg. 2001, 108, 1163–1171; discussion 1172–3. [Google Scholar] [CrossRef]
- Sacchini, V.; Pinotti, J.A.; Barros, A.C.; Luini, A.; Pluchinotta, A.; Pinotti, M.; Boratto, M.G.; Ricci, M.D.; Ruiz, C.A.; Nisida, A.C.; et al. Nipple-sparing mastectomy for breast cancer and risk reduction: Oncologic or technical problem? J. Am. Coll. Surg. 2006, 203, 704–714. [Google Scholar] [CrossRef]
- Garcia-Etienne, C.A.; Cody Iii, H.S., 3rd; Disa, J.J.; Cordeiro, P.; Sacchini, V. Nipple-sparing mastectomy: Initial experience at the Memorial Sloan-Kettering Cancer Center and a comprehensive review of literature. Breast J. 2009, 15, 440–449. [Google Scholar] [CrossRef]
- Chung, A.P.; Sacchini, V. Nipple-sparing mastectomy: Where are we now? Surg. Oncol. 2008, 17, 261–266. [Google Scholar] [CrossRef]
- Yi, M.; Kronowitz, S.J.; Meric-Bernstam, F.; Feig, B.W.; Symmans, W.F.; Lucci, A.; Ross, M.I.; Babiera, G.V.; Kuerer, H.M.; Hunt, K.K. Local, regional, and systemic recurrence rates in patients undergoing skin-sparing mastectomy compared with conventional mastectomy. Cancer 2011, 117, 916–924. [Google Scholar] [CrossRef] [PubMed]
- Romics, L., Jr.; Chew, B.K.; Weiler-Mithoff, E.; Doughty, J.C.; Brown, I.M.; Stallard, S.; Wilson, C.R.; Mallon, E.A.; George, W.D. Ten-year follow-up of skin-sparing mastectomy followed by immediate breast reconstruction. Br. J. Surg. 2012, 99, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Tokin, C.; Weiss, A.; Wang-Rodriguez, J.; Blair, S.L. Oncologic safety of skin-sparing and nipple-sparing mastectomy: A discussion and review of the literature. Int. J. Surg. Oncol. 2012, 2012, 921821. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.T.; Webster, D.J.; Mansel, R.E.; Hughes, L.E. Is immediate postmastectomy reconstruction safe in the long-term? Eur. J. Surg. Oncol. 1993, 19, 372–375. [Google Scholar]
- Fisher, B.; Jeong, J.H.; Anderson, S.; Bryant, J.; Fisher, E.R.; Wolmark, N. Twenty-five-year follow-up of a randomized trial comparing radical mastectomy, total mastectomy, and total mastectomy followed by irradiation. N. Engl. J. Med. 2002, 347, 567–575. [Google Scholar] [CrossRef]
- Veronesi, U.; Cascinelli, N.; Mariani, L.; Greco, M.; Saccozzi, R.; Luini, A.; Aguilar, M.; Marubini, E. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N. Engl. J. Med. 2002, 347, 1227–1232. [Google Scholar] [CrossRef]
- Fisher, B.; Anderson, S.; Bryant, J.; Margolese, R.G.; Deutsch, M.; Fisher, E.R.; Jeong, J.H.; Wolmark, N. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N. Engl. J. Med. 2002, 347, 1233–1241. [Google Scholar] [CrossRef]
- Zakhireh, J.; Fowble, B.; Esserman, L.J. Application of screening principles to the reconstructed breast. J. Clin. Oncol. 2010, 28, 173–180. [Google Scholar] [CrossRef]
- Patterson, S.G.; Teller, P.; Iyengar, R.; Carlson, G.W.; Gabram-Mendola, S.G.; Losken, A.; Styblo, T.; Torres, M.; Wood, W.C.; Perez, S.D.; et al. Locoregional recurrence after mastectomy with immediate transverse rectus abdominis myocutaneous (TRAM) flap reconstruction. Ann. Surg. Oncol. 2012, 19, 2679–2684. [Google Scholar] [CrossRef]
- Freyvogel, M.; Padia, S.; Larson, K.; Dietz, J.; Grobmyer, S.; O’Rourke, C.; Valente, S. Screening mammography following autologous breast reconstruction: An unnecessary effort. Ann. Surg. Oncol. 2014, 21, 3256–3260. [Google Scholar] [CrossRef]
- Handel, N. The effect of silicone implants on the diagnosis, prognosis, and treatment of breast cancer. Plast. Reconstr. Surg. 2007, 120, 81S–93S. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, M.; Kramer, S.; Friedrich, D.; Kraft, C.; Maass, N.; Rogmans, C. Difficulties of Breast Reconstruction—Problems That No One Likes to Face. Anticancer Res. 2021, 41, 5365–5375. [Google Scholar] [CrossRef] [PubMed]
- Khatcheressian, J.L.; Hurley, P.; Bantug, E.; Esserman, L.J.; Grunfeld, E.; Halberg, F.; Hantel, A.; Henry, N.L.; Muss, H.B.; Smith, T.J.; et al. Breast cancer follow-up and management after primary treatment: American Society of Clinical Oncology clinical practice guideline update. J. Clin. Oncol. 2013, 31, 961–965. [Google Scholar] [CrossRef] [PubMed]
- Paszat, L.; Sutradhar, R.; Grunfeld, E.; Gainford, C.; Benk, V.; Bondy, S.; Coyle, D.; Holloway, C.; Sawka, C.; Shumak, R.; et al. Outcomes of surveillance mammography after treatment of primary breast cancer: A population-based case series. Breast Cancer Res. Treat. 2009, 114, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Howard, M.A.; Polo, K.; Pusic, A.L.; Cordeiro, P.G.; Hidalgo, D.A.; Mehrara, B.; Disa, J.J. Breast cancer local recurrence after mastectomy and TRAM flap reconstruction: Incidence and treatment options. Plast. Reconstr. Surg. 2006, 117, 1381–1386. [Google Scholar] [CrossRef] [PubMed]
- Helvie, M.A.; Bailey, J.E.; Roubidoux, M.A.; Pass, H.A.; Chang, A.E.; Pierce, L.J.; Wilkins, E.G. Mammographic screening of TRAM flap breast reconstructions for detection of nonpalpable recurrent cancer. Radiology 2002, 224, 211–216. [Google Scholar] [CrossRef]
- Brennan, S.; Liberman, L.; Dershaw, D.D.; Morris, E. Breast MRI screening of women with a personal history of breast cancer. AJR Am. J. Roentgenol. 2010, 195, 510–516. [Google Scholar] [CrossRef]
- Gweon, H.M.; Cho, N.; Han, W.; Yi, A.; Moon, H.G.; Noh, D.Y.; Moon, W.K. Breast MR imaging screening in women with a history of breast conservation therapy. Radiology 2014, 272, 366–373. [Google Scholar] [CrossRef]
- Schacht, D.V.; Yamaguchi, K.; Lai, J.; Kulkarni, K.; Sennett, C.A.; Abe, H. Importance of a personal history of breast cancer as a risk factor for the development of subsequent breast cancer: Results from screening breast MRI. AJR Am. J. Roentgenol. 2014, 202, 289–292. [Google Scholar] [CrossRef]
- Morris, E.A.; Comstock, C.E.; Lee, C.H. ACR BI-RADS® Magnetic Resonance Imaging. In ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Drew, P.J.; Kerin, M.J.; Turnbull, L.W.; Imrie, M.; Carleton, P.J.; Fox, J.N.; Monson, J.R. Routine screening for local recurrence following breast-conserving therapy for cancer with dynamic contrast-enhanced magnetic resonance imaging of the breast. Ann. Surg. Oncol. 1998, 5, 265–270. [Google Scholar] [CrossRef]
- Frei, K.A.; Kinkel, K.; Bonel, H.M.; Lu, Y.; Esserman, L.J.; Hylton, N.M. MR imaging of the breast in patients with positive margins after lumpectomy: Influence of the time interval between lumpectomy and MR imaging. AJR Am. J. Roentgenol. 2000, 175, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Noroozian, M.; Carlson, L.W.; Savage, J.L.; Jeffries, D.O.; Joe, A.I.; Neal, C.H.; Patterson, S.K.; Hadjiiski, L.M.; Helvie, M.A. Use of Screening Mammography to Detect Occult Malignancy in Autologous Breast Reconstructions: A 15-year Experience. Radiology 2018, 289, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Georgian-Smith, D.; Gazelle, G.S.; Halpern, E.F.; Rafferty, E.A.; Moore, R.H.; Yeh, E.D.; D’Alessandro, H.A.; Hitt, R.A.; Kopans, D.B. Detecting nonpalpable recurrent breast cancer: The role of routine mammographic screening of transverse rectus abdominis myocutaneous flap reconstructions. Radiology 2008, 248, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kwak, J.Y.; Choi, J.W.; Bae, J.H.; Shin, K.M.; Lee, H.J.; Kim, G.C.; Jung, J.H.; Park, J.Y. Impact of US surveillance on detection of clinically occult locoregional recurrence after mastectomy for breast cancer. Ann. Surg. Oncol. 2010, 17, 2670–2676. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.Q.; Dong, J.N.; Meng, Q.X.; Sun, P.; Zhang, J. Ultrasound for postoperative surveillance after mastectomy in patients with breast cancer: A retrospective study. Medicine 2017, 96, e9244. [Google Scholar] [CrossRef] [PubMed]
- Houssami, N.; Ciatto, S.; Martinelli, F.; Bonardi, R.; Duffy, S.W. Early detection of second breast cancers improves prognosis in breast cancer survivors. Ann. Oncol. 2009, 20, 1505–1510. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kang, B.J.; Kim, S.H. Usefulness of postoperative surveillance MR for women after breast-conservation therapy: Focusing on MR features of early and late recurrent breast cancer. PLoS ONE 2021, 16, e0252476. [Google Scholar] [CrossRef] [PubMed]
- Preda, L.; Villa, G.; Rizzo, S.; Bazzi, L.; Origgi, D.; Cassano, E.; Bellomi, M. Magnetic resonance mammography in the evaluation of recurrence at the prior lumpectomy site after conservative surgery and radiotherapy. Breast Cancer Res. 2006, 8, R53. [Google Scholar] [CrossRef]
- Kriege, M.; Brekelmans, C.T.; Boetes, C.; Besnard, P.E.; Zonderland, H.M.; Obdeijn, I.M.; Manoliu, R.A.; Kok, T.; Peterse, H.; Tilanus-Linthorst, M.M.; et al. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N. Engl. J. Med. 2004, 351, 427–437. [Google Scholar] [CrossRef]
- Saslow, D.; Boetes, C.; Burke, W.; Harms, S.; Leach, M.O.; Lehman, C.D.; Morris, E.; Pisano, E.; Schnall, M.; Sener, S.; et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J. Clin. 2007, 57, 75–89. [Google Scholar] [CrossRef]
- Swinnen, J.; Keupers, M.; Soens, J.; Lavens, M.; Postema, S.; Van Ongeval, C. Breast imaging surveillance after curative treatment for primary non-metastasised breast cancer in non-high-risk women: A systematic review. Insights Imaging 2018, 9, 961–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, V.Y.; Kim, E.K.; Kim, M.J.; Moon, H.J.; Yoon, J.H. Breast magnetic resonance imaging for surveillance of women with a personal history of breast cancer: Outcomes stratified by interval between definitive surgery and surveillance MR imaging. BMC Cancer 2018, 18, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]







| Total (n = 286) | Non-Recurrence (n = 264) | Recurrence (n = 22) | p Value | |
|---|---|---|---|---|
| Clinical information | ||||
| Age (mean ± SD 1) | 46.0 (± 8.3) | 46.2 (± 8.1) | 43.0 (± 9.7) | 0.352 |
| Operation | 0.716 | |||
| nipple-sparing mastectomy (NSM) | 192 (67.1%) | 178 (67.4%) | 14 (63.6%) | |
| skin-sparing mastectomy (SSM) | 94 (32.9%) | 86 (32.6%) | 8 (36.4%) | |
| Reconstruction | 0.081 | |||
| flap reconstruction | 155 (54.2%) | 147 (55.7%) | 8 (36.4%) | |
| implant bag reconstruction | 131 (45.8%) | 117 (44.3%) | 14 (63.6%) | |
| Follow-up period (months) | 0.766 | |||
| median (range) | 30 (8–63) | 30 (8–63) | 30 (9–51) | |
| Treatment | ||||
| Neoadjuvant chemotherapy | 0.37 | |||
| yes | 40 (14.0%) | 36 (13.6%) | 4 (18.2%) | |
| no | 246 (86%) | 228 (86.4%) | 18 (81.8%) | |
| Adjuvant radiation therapy | 0.523 | |||
| yes | 71 (24.8%) | 66 (25.0%) | 5 (22.7%) | |
| no | 215 (75.2%) | 198 (75.0%) | 17 (77.3%) | |
| Adjuvant chemotherapy | 0.321 | |||
| yes | 133 (46.5%) | 125 (47.3%) | 8 (36.4%) | |
| no | 153 (53.5%) | 139 (52.7%) | 14 (63.6%) | |
| Adjuvant endocrine therapy | 0.834 | |||
| yes | 226 (79.0%) | 209 (79.2%) | 17 (77.3%) | |
| no | 60 (21.0%) | 55 (20.8%) | 5 (22.7%) | |
| Adjuvant target therapy | 0.176 | |||
| yes | 54 (18.9%) | 52 (19.7%) | 2 (9.1%) | |
| no | 232 (81.1%) | 212 (80.3%) | 20 (90.9%) | |
| Pathologic information | ||||
| TNM Staging | ||||
| T | 0.763 | |||
| 0 | 35 (12.2%) | 34 (12.9%) | 1 (4.5%) | |
| 1 | 104 (36.4%) | 94 (35.6%) | 10 (45.5%) | |
| 2 | 111 (38.8%) | 103 (39.0%) | 8 (36.4%) | |
| 3 | 35 (12.2%) | 32 (12.1%) | 3 (13.6%) | |
| 4 | 1 (0.4%) | 1 (0.4%) | 0 (0.0%) | |
| n | 0.831 | |||
| 0 | 169 (59.1%) | 154 (58.3%) | 15 (68.2%) | |
| 1 | 76 (26.6%) | 71 (26.9%) | 5 (22.7%) | |
| 2 | 20 (7.0%) | 19 (7.2%) | 1 (4.5%) | |
| 3 | 21 (7.3%) | 20 (7.6%) | 1 (4.5%) | |
| Stage | 0.298 | |||
| stage 0 | 35 (12.2%) | 34 (12.9%) | 1 (4.5%) | |
| stage I | 83 (29.0%) | 73 (27.6%) | 10 (45.5%) | |
| stage II | 108 (37.8%) | 101 (38.3%) | 7 (31.8%) | |
| stage III | 60 (21.0%) | 56 (21.2%) | 4 (18.2%) | |
| Cancer histology | 0.553 | |||
| ductal carcinoma in situ | 45 (15.7%) | 42 (15.9%) | 3 (13.6%) | |
| invasive ductal carcinoma, NST 2 | 197 (69.0%) | 180 (68.2%) | 17 (77.3%) | |
| invasive lobular carcinoma | 21 (7.3%) | 21 (8.0%) | 0 (0.0%) | |
| others | 23 (8.0%) | 21 (8.0%) | 2 (9.1%) | |
| Lymphovascular invasion | 0.562 | |||
| positive | 76 (26.6%) | 69 (24.1%) | 7 (31.8%) | |
| negative | 210 (73.4%) | 195 (73.9%) | 15 (68.2%) | |
| Tumor size (cm) | ||||
| Estrogen receptor | 0.766 | |||
| positive | 228 (79.7%) | 211 (79.9%) | 17 (77.3%) | |
| negative | 58 (20.3%) | 53 (20.1%) | 5 (22.7%) | |
| Progesterone receptor | 0.481 | |||
| positive | 213 (74.5%) | 198 (75.0%) | 15 (68.2%) | |
| negative | 73 (25.5%) | 66 (25.0%) | 7 (31.8%) | |
| HER2 3 | 0.912 | |||
| positive | 88 (30.8%) | 81 (30.7%) | 7 (31.8%) | |
| negative | 198 (69.2%) | 183 (69.3%) | 15 (68.2%) | |
| Ki 67 index | 32.7 (± 20.4) | 32.4 (± 20.5) | 36.6 (± 18.9) | 0.963 |
| Subtype | 0.829 | |||
| luminal | 230 (80.4%) | 213 (80.7%) | 17 (77.3%) | |
| HER2 | 40 (14.0%) | 36 (13.6%) | 4 (18.2%) | |
| triple negative | 16 (5.6%) | 15 (5.7%) | 1 (4.5%) | |
| Total (n = 286) | Non-Recurrence (n = 264) | Recurrence (n = 22) | p Value | |
|---|---|---|---|---|
| Tumor location | 0.945 | |||
| right | 128 (44.8%) | 118 (44.7%) | 10 (45.5%) | |
| left | 158 (55.2%) | 146 (55.3%) | 12 (54.5%) | |
| Lesion type | 0.788 | |||
| mass | 73 (25.5%) | 66 (25.0%) | 7 (31.8%) | |
| non-mass enhancement | 103 (36.0%) | 96 (36.4%) | 7 (31.8%) | |
| both | 110 (38.5%) | 102 (38.6%) | 8 (36.4%) | |
| Multifocality/multicentricity | <0.001 | |||
| yes | 206 (72.0%) | 186 (70.5%) | 20 (90.9%) | |
| no | 80 (28.0%) | 78 (29.5%) | 2 (9.1%) | |
| Background parenchymal enhancement | 0.493 | |||
| minimal | 119 (41.6%) | 107 (40.5%) | 12 (54.5%) | |
| mild | 71 (24.8%) | 68 (25.8%) | 3 (13.6%) | |
| moderate | 63 (22.0%) | 59 (22.3%) | 4 (18.2%) | |
| marked | 33 (11.6%) | 30 (11.4%) | 3 (13.6%) | |
| Fibroglandular tissue | 0.037 | |||
| fatty | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| scattered | 12 (4.2%) | 12 (4.6%) | 0 (0.0%) | |
| heterogenous | 194 (67.8%) | 183 (69.3%) | 11 (50.0%) | |
| extreme | 80 (28.0%) | 69 (26.1%) | 11 (50.0%) | |
| Total (n = 27) | Symptomatic (n = 12) | Asymptomatic (n = 15) | p Value | |
|---|---|---|---|---|
| Lesion type | 0.002 | |||
| mass | 21 (77.8%) | 6 (50.0%) | 15 (100.0%) | |
| skin | 6 (22.2%) | 6 (50.0%) | 0 (0.0%) | |
| Recurrence interval (months) | ||||
| median (range) | 12 (3–51) | 8 (3–15) | 12 (5–51) | 0.198 |
| mean (SD 1) | 16.7 (± 14.67) | 10.4 (± 5.82) | 21.7 (± 17.69) | <0.001 |
| Detection modality | 0.001 | |||
| physical examination | 6 (22.2%) | 6 (50.0%) | 0 (0.0%) | |
| ultrasound | 9 (33.3%) | 5 (41.7%) | 4 (26.7%) | |
| MRI | 12 (44.4%) | 1 (8.3%) | 11 (73.3%) | |
| Tumor size (MRI) (cm) | ||||
| mean (SD) | 0.8 (± 0.46) | 1.2 (± 0.70) | 0.7 (± 2.67) | 0.004 |
| Primary cancer histology | 0.323 | |||
| ductal carcinoma in situ | 3 (11.1%) | 1 (8.3%) | 3 (20.0%) | |
| invasive ductal carcinoma, NST 2 | 20 (74.1%) | 10 (83.3%) | 9 (60.0%) | |
| invasive lobular carcinoma | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| others | 4 (14.8%) | 1 (8.3%) | 3 (20.0%) | |
| Primary cancer subtype | 0.905 | |||
| luminal | 17 (63.0%) | 8 (66.7%) | 9 (60.0%) | |
| HER2 | 9 (33.3%) | 3 (25.0%) | 6 (40.0%) | |
| triple negative | 1 (3.7%) | 1 (8.3%) | 0 (0.0%) | |
| Stage | 0.152 | |||
| stage 0 | 3 (11.1%) | 1 (8.3%) | 2 (13.3%) | |
| stage I | 13 (48.2%) | 4 (33.3%) | 9 (60.0%) | |
| stage II | 10 (37.0%) | 6 (50.0%) | 4 (26.7%) | |
| stage III | 1 (3.7%) | 1 (8.3%) | 0 (0.0%) | |
| Adjuvant therapy | ||||
| radiation therapy | 0.067 | |||
| yes | 5 (18.5%) | 5 (41.7%) | 0 (0.0%) | |
| no | 22 (81.5%) | 7 (58.3%) | 15 (100.0%) | |
| chemotherapy | 0.792 | |||
| yes | 10 (37.0%) | 4 (33.3%) | 6 (40.0%) | |
| no | 17 (63.0%) | 8 (66.7%) | 9 (60.0%) | |
| endocrine therapy | 0.614 | |||
| yes | 22 (81.5%) | 9 (75.0%) | 13 (86.7%) | |
| no | 5 (18.5%) | 3 (25.0%) | 2 (13.3%) | |
| target therapy | 0.829 | |||
| yes | 3 (11.1%) | 1 (8.3%) | 2 (13.3%) | |
| no | 24 (88.9%) | 11 (91.7%) | 13 (86.7%) |
| Imaging Modality | Total (n = 21) | Symptomatic (n = 6) | Asymptomatic (n = 15) |
|---|---|---|---|
| MRI | 20 (95.2%) | 6 (100.0%) | 14 (93.3%) |
| Ultrasound | 8 (38.1%) | 4 (66.7%) | 4 (26.7%) |
| p value | <0.001 | 0.140 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Kang, B.J.; Park, G.E.; Kim, S.H. The Usefulness of Magnetic Resonance Imaging (MRI) for the Detection of Local Recurrence after Mastectomy with Reconstructive Surgery in Breast Cancer Patients. Diagnostics 2022, 12, 2203. https://doi.org/10.3390/diagnostics12092203
Lee J, Kang BJ, Park GE, Kim SH. The Usefulness of Magnetic Resonance Imaging (MRI) for the Detection of Local Recurrence after Mastectomy with Reconstructive Surgery in Breast Cancer Patients. Diagnostics. 2022; 12(9):2203. https://doi.org/10.3390/diagnostics12092203
Chicago/Turabian StyleLee, Jeongmin, Bong Joo Kang, Ga Eun Park, and Sung Hun Kim. 2022. "The Usefulness of Magnetic Resonance Imaging (MRI) for the Detection of Local Recurrence after Mastectomy with Reconstructive Surgery in Breast Cancer Patients" Diagnostics 12, no. 9: 2203. https://doi.org/10.3390/diagnostics12092203