
Primary Tumor Resection Provides Survival Benefits for Patients with Synchronous Brain Metastases from Colorectal Cancer


Abstract
:1. Introduction
2. Material and Methods
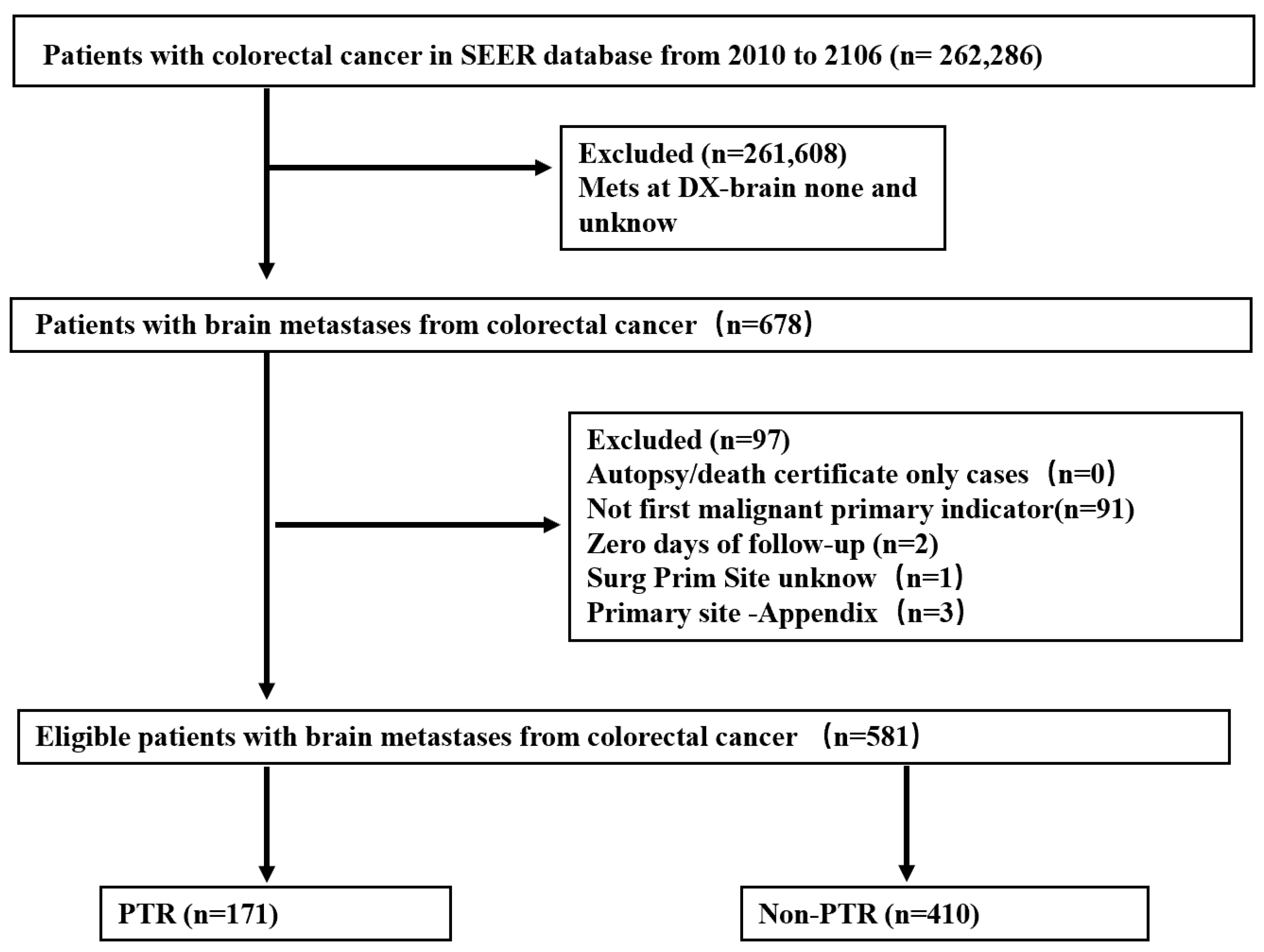
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
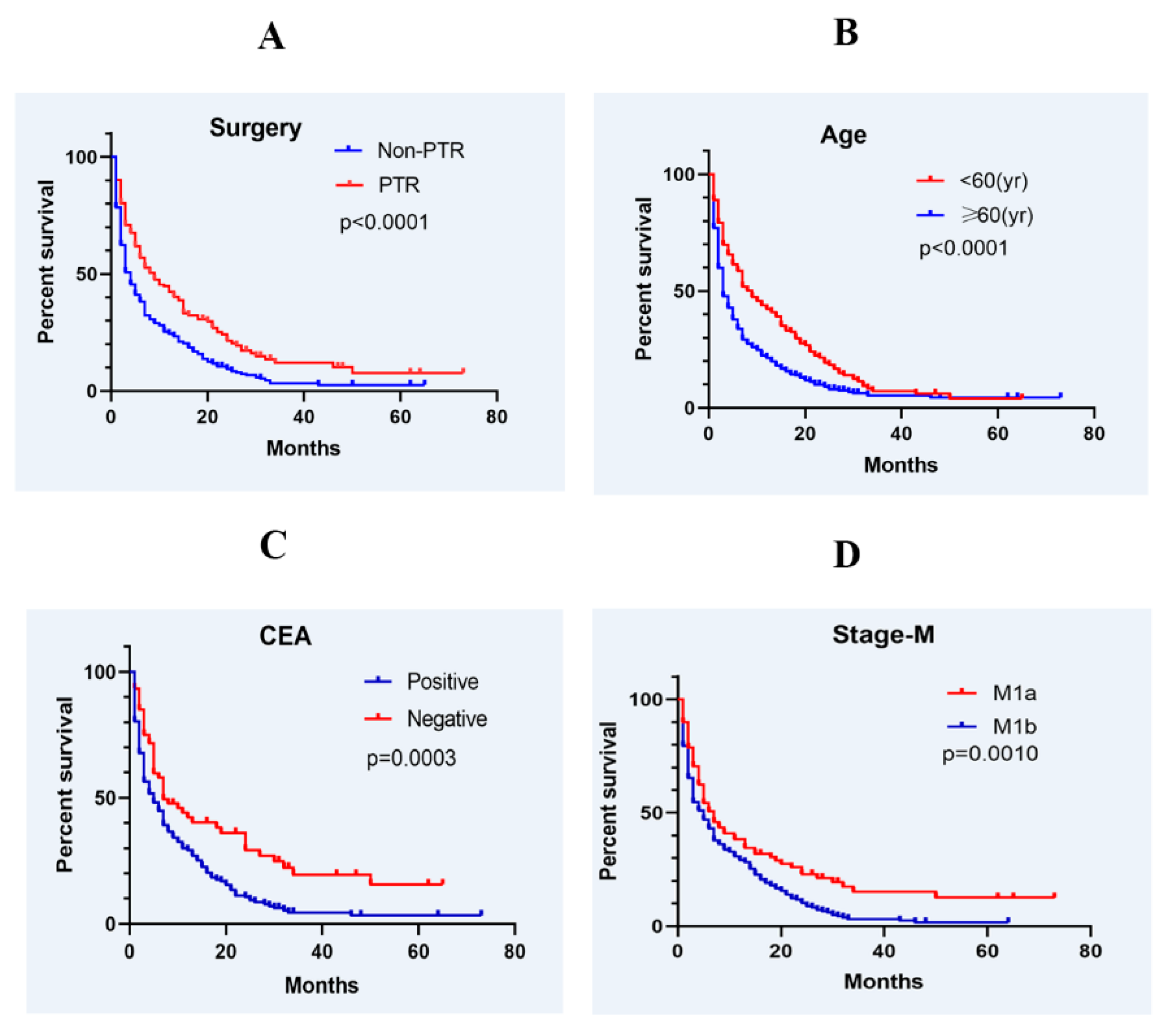
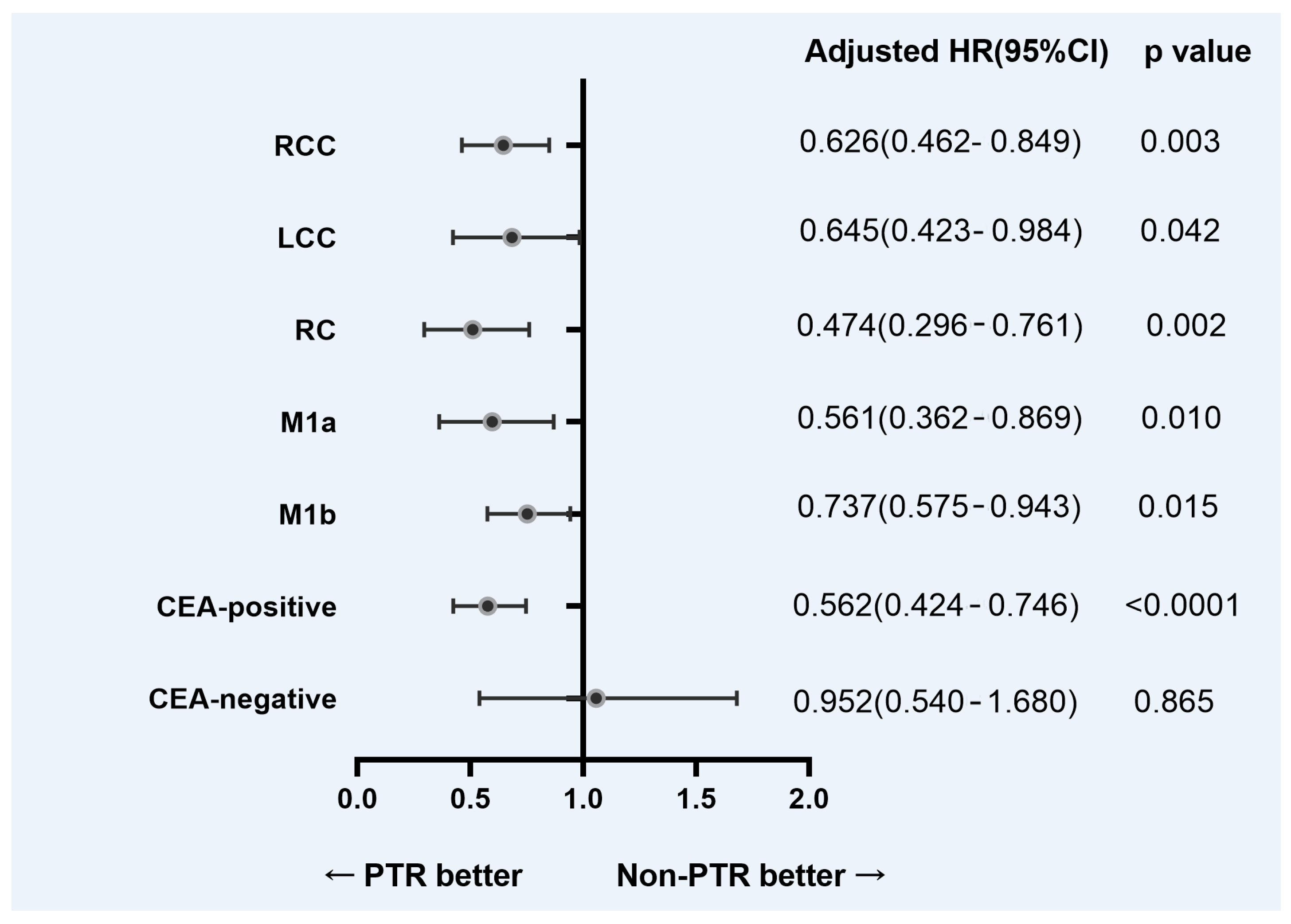
3.2. Survival and Prognostic Factors
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CRC | colorectal cancer |
| BMs | brain metastases |
| SEER | Surveillance, Epidemiology, and End Results |
| CEA | carcinoembryonic antigen |
| RCC | right colon cancer |
| LCC | left colon cancer |
| RC | rectal cancer |
| CI | confidence interval |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Van Cutsem, E.; Nordlinger, B.; Cervantes, A.; Group, E.G.W. Advanced colorectal cancer: ESMO Clinical Practice Guidelines for treatment. Ann. Oncol. 2010, 21 (Suppl. 5), v93–v97. [Google Scholar] [CrossRef]
- Muller, S.; Kohler, F.; Hendricks, A.; Kastner, C.; Borner, K.; Diers, J.; Lock, J.F.; Petritsch, B.; Germer, C.T.; Wiegering, A. Brain Metastases from Colorectal Cancer: A Systematic Review of the Literature and Meta-Analysis to Establish a Guideline for Daily Treatment. Cancers 2021, 13, 900. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Berghoff, A.S.; Schur, S.; Fureder, L.M.; Gatterbauer, B.; Dieckmann, K.; Widhalm, G.; Hainfellner, J.; Zielinski, C.C.; Birner, P.; Bartsch, R.; et al. Descriptive statistical analysis of a real life cohort of 2419 patients with brain metastases of solid cancers. ESMO Open 2016, 1, e000024. [Google Scholar] [CrossRef] [Green Version]
- Noura, S.; Ohue, M.; Shingai, T.; Fujiwara, A.; Imada, S.; Sueda, T.; Yamada, T.; Fujiwara, Y.; Ohigashi, H.; Yano, M.; et al. Brain metastasis from colorectal cancer: Prognostic factors and survival. J. Surg. Oncol. 2012, 106, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Tapia Rico, G.; Price, T.J.; Karapetis, C.; Piantadosi, C.; Padbury, R.; Roy, A.; Maddern, G.; Moore, J.; Carruthers, S.; Roder, D.; et al. Brain metastasis in advanced colorectal cancer: Results from the South Australian metastatic colorectal cancer (SAmCRC) registry. Cancer Biol. Med. 2017, 14, 371–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, X.D.; Cai, Y.T.; Zhou, Y.M.; Li, Z.Y.; Xiang, J.B.; Chen, Z.Y. Prognostic factors and multidisciplinary treatment modalities for brain metastases from colorectal cancer: Analysis of 93 patients. BMC Cancer 2015, 15, 902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartelt, S.; Momm, F.; Weissenberger, C.; Lutterbach, J. Patients with brain metastases from gastrointestinal tract cancer treated with whole brain radiation therapy: Prognostic factors and survival. World J. Gastroenterol. 2004, 10, 3345–3348. [Google Scholar] [CrossRef] [PubMed]
- Cagney, D.N.; Martin, A.M.; Catalano, P.J.; Redig, A.J.; Lin, N.U.; Lee, E.Q.; Wen, P.Y.; Dunn, I.F.; Bi, W.L.; Weiss, S.E.; et al. Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: A population-based study. Neuro. Oncol. 2017, 19, 1511–1521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokoro, T.; Okuno, K.; Hida, J.C.; Ueda, K.; Yoshifuji, T.; Daito, K.; Sugiura, F. Prognostic factors for patients with advanced colorectal cancer and symptomatic brain metastases. Clin. Colorectal Cancer 2014, 13, 226–231. [Google Scholar] [CrossRef]
- Chang, Y.; Wong, C.E.; Lee, P.H.; Huang, C.C.; Lee, J.S. Survival Outcome of Surgical Resection vs. Radiotherapy in Brain Metastasis From Colorectal Cancer: A Meta-Analysis. Front. Med. 2022, 9, 768896. [Google Scholar] [CrossRef]
- Quan, J.C.; Guan, X.; Ma, C.X.; Liu, Z.; Yang, M.; Zhao, Z.X.; Sun, P.; Zhuang, M.; Wang, S.; Jiang, Z.; et al. Prognostic scoring system for synchronous brain metastasis at diagnosis of colorectal cancer: A population-based study. World J. Gastrointest. Oncol. 2020, 12, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Bergen, E.S.; Scherleitner, P.; Ferreira, P.; Kiesel, B.; Muller, C.; Widhalm, G.; Dieckmann, K.; Prager, G.; Preusser, M.; Berghoff, A.S. Primary tumor side is associated with prognosis of colorectal cancer patients with brain metastases. ESMO Open 2021, 6, 100168. [Google Scholar] [CrossRef] [PubMed]
- Vogelbaum, M.A.; Suh, J.H. Resectable brain metastases. J. Clin. Oncol. 2006, 24, 1289–1294. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.D.; Trifiletti, D.M.; Gondi, V.; Chan, M.; Minniti, G.; Rusthoven, C.G.; Schild, S.E.; Mishra, M.V.; Bovi, J.; Williams, N.; et al. Multidisciplinary patient-centered management of brain metastases and future directions. Neurooncol. Adv. 2020, 2, vdaa034. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, K.J.; Chua, W.; Ng, W.; Roohullah, A. Management of asymptomatic primary tumours in stage IV colorectal cancer: Review of outcomes. World J. Gastrointest. Oncol. 2015, 7, 513–523. [Google Scholar] [CrossRef]
- Ruo, L.; Gougoutas, C.; Paty, P.B.; Guillem, J.G.; Cohen, A.M.; Wong, W.D. Elective bowel resection for incurable stage IV colorectal cancer: Prognostic variables for asymptomatic patients. J. Am. Coll. Surg. 2003, 196, 722–728. [Google Scholar] [CrossRef]
- Poultsides, G.A.; Servais, E.L.; Saltz, L.B.; Patil, S.; Kemeny, N.E.; Guillem, J.G.; Weiser, M.; Temple, L.K.; Wong, W.D.; Paty, P.B. Outcome of primary tumor in patients with synchronous stage IV colorectal cancer receiving combination chemotherapy without surgery as initial treatment. J. Clin. Oncol. 2009, 27, 3379–3384. [Google Scholar] [CrossRef] [Green Version]
- Mege, D.; Ouaissi, M.; Fuks, D.; Metellus, P.; Peltier, J.; Dufour, H.; Regimbeau, J.M.; Dahan, L.; Sielezneff, I.; Sastre, B. Patients with brain metastases from colorectal cancer are not condemned. Anticancer. Res. 2013, 33, 5645–5648. [Google Scholar]
- Prasanna, T.; Karapetis, C.S.; Roder, D.; Tie, J.; Padbury, R.; Price, T.; Wong, R.; Shapiro, J.; Nott, L.; Lee, M.; et al. The survival outcome of patients with metastatic colorectal cancer based on the site of metastases and the impact of molecular markers and site of primary cancer on metastatic pattern. Acta Oncol. 2018, 57, 1438–1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boysen, A.K.; Ording, A.G.; Astradsson, A.; Hoyer, M.; Spindler, K.L. Metastasis directed treatment of brain metastases from colorectal cancer—A Danish population-based cohort study. Acta Oncol. 2020, 59, 1118–1122. [Google Scholar] [CrossRef]
- Kruser, T.J.; Chao, S.T.; Elson, P.; Barnett, G.H.; Vogelbaum, M.A.; Angelov, L.; Weil, R.J.; Pelley, R.; Suh, J.H. Multidisciplinary management of colorectal brain metastases: A retrospective study. Cancer 2008, 113, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Damiens, K.; Ayoub, J.P.; Lemieux, B.; Aubin, F.; Saliba, W.; Campeau, M.P.; Tehfe, M. Clinical features and course of brain metastases in colorectal cancer: An experience from a single institution. Curr. Oncol. 2012, 19, 254–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fountzilas, C.; Chang, K.; Hernandez, B.; Michalek, J.; Crownover, R.; Floyd, J.; Mahalingam, D. Clinical characteristics and treatment outcomes of patients with colorectal cancer who develop brain metastasis: A single institution experience. J Gastrointest. Oncol. 2017, 8, 55–63. [Google Scholar] [CrossRef] [Green Version]
- van der Burg, M.E.; van Lent, M.; Buyse, M.; Kobierska, A.; Colombo, N.; Favalli, G.; Lacave, A.J.; Nardi, M.; Renard, J.; Pecorelli, S. The effect of debulking surgery after induction chemotherapy on the prognosis in advanced epithelial ovarian cancer. Gynecological Cancer Cooperative Group of the European Organization for Research and Treatment of Cancer. N. Engl. J. Med. 1995, 332, 629–634. [Google Scholar] [CrossRef]
- Flanigan, R.C.; Salmon, S.E.; Blumenstein, B.A.; Bearman, S.I.; Roy, V.; McGrath, P.C.; Caton, J.R., Jr.; Munshi, N.; Crawford, E.D. Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for metastatic renal-cell cancer. N. Engl. J. Med. 2001, 345, 1655–1659. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L.; et al. Colon Cancer, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2021, 19, 329–359. [Google Scholar] [CrossRef]
- Sarela, A.I.; Guthrie, J.A.; Seymour, M.T.; Ride, E.; Guillou, P.J.; O’Riordain, D.S. Non-operative management of the primary tumour in patients with incurable stage IV colorectal cancer. Br. J. Surg. 2001, 88, 1352–1356. [Google Scholar] [CrossRef]
- Ahmed, S.; Leis, A.; Fields, A.; Chandra-Kanthan, S.; Haider, K.; Alvi, R.; Reeder, B.; Pahwa, P. Survival impact of surgical resection of primary tumor in patients with stage IV colorectal cancer: Results from a large population-based cohort study. Cancer 2014, 120, 683–691. [Google Scholar] [CrossRef]
- Stillwell, A.P.; Buettner, P.G.; Ho, Y.H. Meta-analysis of survival of patients with stage IV colorectal cancer managed with surgical resection versus chemotherapy alone. World J. Surg. 2010, 34, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Xia, Z.; Jia, X.; Chen, K.; Li, D.; Dai, Y.; Tao, M.; Mao, Y. Primary Tumor Resection Is Associated with Improved Survival in Stage IV Colorectal Cancer: An Instrumental Variable Analysis. Sci. Rep. 2015, 5, 16516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterpetti, A.V.; Costi, U.; D’Ermo, G. National statistics about resection of the primary tumor in asymptomatic patients with Stage IV colorectal cancer and unresectable metastases. Need for improvement in data collection. A systematic review with meta-analysis. Surg. Oncol. 2020, 33, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; He, W.; Xie, Q.; Liu, S.; Kong, P.; Jiang, C.; Zhang, B.; Xia, L. Brain metastases in newly diagnosed colorectal cancer: A population-based study. Cancer Manag. Res 2018, 10, 5649–5658. [Google Scholar] [CrossRef] [Green Version]
- Farnell, G.F.; Buckner, J.C.; Cascino, T.L.; O’Connell, M.J.; Schomberg, P.J.; Suman, V. Brain metastases from colorectal carcinoma. The long term survivors. Cancer 1996, 78, 711–716. [Google Scholar] [CrossRef]
- Duffy, M.J.; Lamerz, R.; Haglund, C.; Nicolini, A.; Kalousova, M.; Holubec, L.; Sturgeon, C. Tumor markers in colorectal cancer, gastric cancer and gastrointestinal stromal cancers: European group on tumor markers 2014 guidelines update. Int. J. Cancer 2014, 134, 2513–2522. [Google Scholar] [CrossRef]
- Tampellini, M.; Ottone, A.; Alabiso, I.; Baratelli, C.; Forti, L.; Berruti, A.; Aroasio, E.; Scagliotti, G.V. The prognostic role of baseline CEA and CA 19-9 values and their time-dependent variations in advanced colorectal cancer patients submitted to first-line therapy. Tumor Biol. 2015, 36, 1519–1527. [Google Scholar] [CrossRef] [Green Version]
- Cascino, T.L.; Leavengood, J.M.; Kemeny, N.; Posner, J.B. Brain metastases from colon cancer. J. Neurooncol. 1983, 1, 203–209. [Google Scholar] [CrossRef]
- Tanriverdi, O.; Kaytan-Saglam, E.; Ulger, S.; Bayoglu, I.V.; Turker, I.; Ozturk-Topcu, T.; Cokmert, S.; Turhal, S.; Oktay, E.; Karabulut, B.; et al. The clinical and pathological features of 133 colorectal cancer patients with brain metastasis: A multicenter retrospective analysis of the Gastrointestinal Tumors Working Committee of the Turkish Oncology Group (TOG). Med. Oncol. 2014, 31, 152. [Google Scholar] [CrossRef]
- Kye, B.H.; Kim, H.J.; Kang, W.K.; Cho, H.M.; Hong, Y.K.; Oh, S.T. Brain metastases from colorectal cancer: The role of surgical resection in selected patients. Colorectal Dis. 2012, 14, e378–e385. [Google Scholar] [CrossRef]
- Christensen, T.D.; Spindler, K.L.; Palshof, J.A.; Nielsen, D.L. Systematic review: Brain metastases from colorectal cancer--Incidence and patient characteristics. BMC Cancer 2016, 16, 260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mo, S.; Cai, X.; Zhou, Z.; Li, Y.; Hu, X.; Ma, X.; Zhang, L.; Cai, S.; Peng, J. Nomograms for predicting specific distant metastatic sites and overall survival of colorectal cancer patients: A large population-based real-world study. Clin. Transl. Med. 2020, 10, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Del Carpio Huerta, L.; Virgili Manrique, A.C.; Szafranska, J.; Martin-Richard, M.; Paez Lopez-Bravo, D.; Sebio Garcia, A.; Espinosa Mariscal, I.; Gomila Pons, P.; Andres Granyo, M.; Barba Joaquin, A.; et al. Brain metastases in colorectal cancer: Prognostic factors and survival analysis. Int. J. Colorectal Dis. 2018, 33, 1517–1523. [Google Scholar] [CrossRef] [PubMed]
- Missiaglia, E.; Jacobs, B.; D’Ario, G.; Di Narzo, A.F.; Soneson, C.; Budinska, E.; Popovici, V.; Vecchione, L.; Gerster, S.; Yan, P.; et al. Distal and proximal colon cancers differ in terms of molecular, pathological, and clinical features. Ann. Oncol. 2014, 25, 1995–2001. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Jiang, F.; Lin, H.; Li, S. Clinical characteristics and prognosis of different primary tumor location in colorectal cancer: A population-based cohort study. Clin. Transl. Oncol. 2019, 21, 1524–1531. [Google Scholar] [CrossRef] [Green Version]
- Renzi, G.D.; Gaballo, G.; Gazzaniga, P.; Nicolazzo, C.J.O. Molecular Biomarkers according to Primary Tumor Location in Colorectal Cancer: Current Standard and New Insights. Oncology 2021, 99, 135–143. [Google Scholar] [CrossRef]
- Roussille, P.; Auvray, M.; Vansteene, D.; Lecomte, T.; Rigault, E.; Maillet, M.; Locher, C.; Dior, M.; Hautefeuille, V.; Artru, P.; et al. Prognostic factors of colorectal cancer patients with brain metastases. Radiother. Oncol. 2021, 158, 67–73. [Google Scholar] [CrossRef]
- Imaizumi, J.; Shida, D.; Narita, Y.; Miyakita, Y.; Tanabe, T.; Takashima, A.; Boku, N.; Igaki, H.; Itami, J.; Kanemitsu, Y. Prognostic factors of brain metastases from colorectal cancer. BMC Cancer 2019, 19, 755. [Google Scholar] [CrossRef] [Green Version]
- Roussille, P.; Tachon, G.; Villalva, C.; Milin, S.; Frouin, E.; Godet, J.; Berger, A.; Emambux, S.; Petropoulos, C.; Wager, M.; et al. Pathological and Molecular Characteristics of Colorectal Cancer with Brain Metastases. Cancers 2018, 10, 504. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.; Cai, Y.; Xia, L.; Ju, H.; Zhao, X. Treatment modalities and relative survival in patients with brain metastasis from colorectal cancer. Biosci. Trends 2019, 13, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Quan, J.; Ma, C.; Sun, P.; Wang, S.; Zhuang, M.; Liu, Z.; Jiang, Z.; Chen, H.; Yang, M.; Zhao, Z.; et al. Brain metastasis from colorectal cancer: Clinical characteristics, timing, survival and prognostic factors. Scand. J. Gastroenterol. 2019, 54, 1370–1375. [Google Scholar] [CrossRef] [PubMed]
- Mjahed, R.B.; Astaras, C.; Roth, A.; Koessler, T. Where Are We Now and Where Might We Be Headed in Understanding and Managing Brain Metastases in Colorectal Cancer Patients? Curr. Treat. Options Oncol. 2022, 23, 980–1000. [Google Scholar] [CrossRef] [PubMed]
- Goksu, S.Y.; Beg, M.S.; Sanjeevaiah, A.; Gumusgoz, E.; Hsieh, D.; Ozer, M.; Jones, A.L.; Kainthla, R.; Verma, U.; Al Mutar, S.; et al. The pattern of brain metastasis in colorectal cancer: Efficacy of metastasectomy, chemotherapy. J. Clin. Oncol. 2021, 39, 40. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 581) | Non-PTR (n = 410) | PTR (n = 171) | p Value | |||
|---|---|---|---|---|---|---|---|
| Age (yr) <60 ≥60 | 225 356 | (37.8) (61.3) | 161 249 | (39.3) (60.7) | 64 107 | (37.4) (62.6) | 0.678 |
| Race Black White Other | 67 470 44 | (11.5) (80.9) (7.6) | 49 328 33 | (12.0) (80.0) (8.0) | 18 142 11 | (10.5) (83.0) (6.4) | 0.682 |
| Gender Female Male | 275 306 | (47.3) (52.7) | 196 214 | (47.8) (52.2) | 79 92 | (46.2) (53.8) | 0.724 |
| Primary tumor site RCC LCC RC Unknown | 206 115 170 90 | (35.5) (19.8) (29.3) (15.5) | 115 70 142 83 | (28.0) (17.1) (34.6) (20.2) | 91 45 28 7 | (53.2) (26.3) (16.4) (4.1) | <0.0001 |
| Histology Adenocarcinoma Other | 505 76 | (86.9) (13.1) | 357 53 | (87.1) (12.9) | 148 23 | (86.5) (13.5) | 0.865 |
| Tumor grade Well/moderately Poorly/undifferentiated Unknown | 222 137 222 | (38.2) (23.6) (38.2) | 129 69 212 | (31.5) (16.8) (51.7) | 93 68 10 | (54.4) (39.8) (5.8) | <0.0001 |
| T stage T0/T1 T2 T3 T4 Tx | 64 20 132 100 265 | (11.0) (3.4) (22.7) (17.2) (45.6) | 61 12 44 35 258 | (14.9) (2.9) (10.7) (8.5) (62.9) | 3 8 88 65 7 | (1.8) (4.7) (51.5) (38.0) (4.1) | <0.0001 |
| N stage N0 N1 N2 Nx | 192 162 90 137 | (33.0) (27.9) (15.5) (23.6) | 154 105 17 134 | (37.6) (25.6) (4,1) (32.7) | 38 57 73 3 | (22.2) (33.3) (42.7) (1.8) | <0.0001 |
| M stage M1a M1b M1x | 106 410 65 | (18.2) (70.6) (11.2) | 55 309 46 | (13.4) (75.4) (11.2) | 51 101 19 | (29.8) (59.1) (11.1) | <0.0001 |
| CEA Positive Negative Unknown | 309 64 208 | (53.2) (11.0) (35.8) | 222 32 156 | (54.1) (7.8) (38.0) | 87 32 52 | (50.9) (18.7) (30.4) | <0.0001 |
| Clinicopathologic Variable | HR | 95%CI | p Value |
|---|---|---|---|
| Age (yr) <60 ≥60 | Reference 1.708 | 1.418–2.057 | <0.0001 |
| Race Black White Other | Reference 0.903 0.972 | 0.693–1.176 0.648–1.458 | 0.447 0.893 |
| Gender Female Male | Reference 1.087 | 0.911–1.297 | 0.356 |
| Primary tumor site RCC LCC RC Unknown | Reference 0.840 0.838 1.236 | 0.655–1.078 0.671–1.046 0.949–1.611 | 0.171 0.118 0.116 |
| Histology Adenocarcinoma Other | Reference 1.090 | 0.840–1.414 | 0.518 |
| Tumor grade Well/moderately Poorly/undifferentiated Unknown | Reference 1.118 1.432 | 0.884–1.413 1.170–1.751 | 0.352 <0.0001 |
| T stage T0/T1 T2 T3 T4 Tx | Reference 1.219 0.886 1.171 1.336 | 0.721–2.063 0.634–1.237 0.831–1.651 0.988–1.806 | 0.460 0.476 0.366 0.060 |
| N stage N0 N1 N2 Nx | Reference 1.006 0.863 1.242 | 0.801–1.264 0.655–1.137 0.980–1.573 | 0.958 0.295 0.073 |
| M stage M1a M1b M1x | Reference 1.393 1.349 | 1.094–1.772 0.959–1.898 | 0.007 0.086 |
| CEA Positive Negative Unknown | Reference 0.556 1.167 | 0.406–0.759 0.965–1.410 | <0.0001 0.110 |
| Surgery Non-PTR PTR | Reference 0.629 | 0.515–0.768 | <0.0001 |
| Clinicopathologic Variable | HR | 95%CI | p Value |
|---|---|---|---|
| Age (yr) <60 ≥60 | Reference 1.718 | 1.423–2.075 | <0.0001 |
| M stage M1a M1b M1x | Reference 1.167 1.020 | 0.905–1.506 0.716–1.454 | 0.234 0.912 |
| CEA Positive Negative Unknown | Reference 0.652 1.140 | 0.472–0.899 0.935–1.389 | 0.009 0.196 |
| Surgery Non-PTR PTR | Reference 0.654 | 0.531–0.805 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, X.; Li, Y.; Chen, D.; Xu, X.; Liu, F.; Zhao, F. Primary Tumor Resection Provides Survival Benefits for Patients with Synchronous Brain Metastases from Colorectal Cancer. Diagnostics 2022, 12, 1586. https://doi.org/10.3390/diagnostics12071586
Cheng X, Li Y, Chen D, Xu X, Liu F, Zhao F. Primary Tumor Resection Provides Survival Benefits for Patients with Synchronous Brain Metastases from Colorectal Cancer. Diagnostics. 2022; 12(7):1586. https://doi.org/10.3390/diagnostics12071586
Chicago/Turabian StyleCheng, Xiaofei, Yanqing Li, Dong Chen, Xiangming Xu, Fanlong Liu, and Feng Zhao. 2022. "Primary Tumor Resection Provides Survival Benefits for Patients with Synchronous Brain Metastases from Colorectal Cancer" Diagnostics 12, no. 7: 1586. https://doi.org/10.3390/diagnostics12071586