
Superb Microvascular Imaging (SMI) Compared with Color Doppler Ultrasound for the Assessment of Hepatic Artery in Pediatric Liver Transplants: A Feasibility Study

 , , ,
, , ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Duffy, J.P.; Hong, J.C.; Farmer, D.G.; Ghobrial, R.M.; Yersiz, H.; Hiatt, J.R.; Busuttil, R.W. Vascular complications of orthotopic liver transplantation: Experience in more than 4200 patients. J. Am. Coll. Surg. 2009, 208, 896–905. [Google Scholar] [CrossRef] [PubMed]
- Kutluturk, K.; Sahin, T.T.; Karakas, S.; Unal, B.; Gozukara Bag, H.G.; Akbulut, S.; Aydin, C.; Yilmaz, S. Early Hepatic Artery Thrombosis after Pediatric Living Donor Liver Transplantation. In Transplantation Proceedings; Elsevier: Amsterdam, The Netherlands, 2019; Volume 51, pp. 1162–1168. [Google Scholar] [CrossRef]
- Rela, M.; Muiesan, P.; Bhatnagar, V.; Baker, A.; Mowat, A.P.; Mieli-Vergani, G.; Karani, J.; Williams, R.; Heaton, N.D. Hepatic artery thrombosis after liver transplantation in children under 5 years of age. Transplantation 1996, 61, 1355–1357. [Google Scholar] [CrossRef] [PubMed]
- Vincenzo, M.; Carlos, E.; Leonard, M.; Steven, B.; Delawir, K.; Baburao, K.; Velma, P.S.; Andrei, C.S.; Satoru, T.; Andres, G.T.; et al. Hepatic artery thrombosis after pediatric liver transplantation—A medical or surgical event? Transplantation 1989, 47, 971–977. [Google Scholar]
- Piardi, T.; Lhuaire, M.; Bruno, O.; Memeo, R.; Pessaux, P.; Kianmanesh, R.; Sommacale, D. Vascular complications following liver transplantation: A literature review of advances in 2015. World J. Hepatol. 2016, 8, 36–57. [Google Scholar] [CrossRef] [PubMed]
- Teegen, E.M.; Denecke, T.; Eisele, R.; Lojewski, C.; Neuhaus, P.; Chopra, S.S. Clinical application of modern ultrasound techniques after liver transplantation. Acta Radiol. 2016, 57, 1161–1170. [Google Scholar] [CrossRef] [PubMed]
- Itri, J.N.; Heller, M.T.; Tublin, M.E. Hepatic transplantation: Postoperative complications. Abdom Imaging 2013, 38, 1300–1333. [Google Scholar] [CrossRef]
- Frongillo, F.; Lirosi, M.C.; Nure, E.; Inchingolo, R.; Bianco, G.; Silvestrini, N.; Avolio, A.W.; De Gaetano, A.M.; Cina, A.; Di Stasi, C.; et al. Diagnosis and Management of Hepatic Artery Complications After Liver Transplantation. In Transplantation Proceedings; Elsevier: Amsterdam, The Netherlands, 2015; Volume 47, pp. 2150–2155. [Google Scholar] [CrossRef]
- Hom, B.K.; Shrestha, R.; Palmer, S.L.; Katz, M.D.; Selby, R.R.; Asatryan, Z.; Wells, J.K.; Grant, E.G. Prospective evaluation of vascular complications after liver transplantation: Comparison of conventional and microbubble contrast-enhanced US. Radiology 2006, 241, 267–274. [Google Scholar] [CrossRef]
- Crossin, J.D.; Muradali, D.; Wilson, S.R. US of liver transplants: Normal and abnormal. Radiographics 2003, 23, 1093–1114. [Google Scholar] [CrossRef]
- García-Criado, A.; Gilabert, R.; Bargalló, X.; Brú, C. Radiology in liver transplantation. In Semin Ultrasound CT MR; Elsevier: Amsterdam, The Netherlands, 2002; Volume 23, pp. 114–129. [Google Scholar] [CrossRef]
- Ntoulia, A.; Anupindi, S.A.; Back, S.J.; Didier, R.A.; Hwang, M.; Johnson, A.M.; McCarville, M.B.; Papadopoulou, F.; Piskunowicz, M.; Sellars, M.E.; et al. Contrast-enhanced ultrasound: A comprehensive review of safety in children. Pediatr. Radiol. 2021, 51, 2161–2180. [Google Scholar] [CrossRef]
- Chodick, G.; Kim, K.P.; Shwarz, M.; Horev, G.; Shalev, V.; Ron, E. Radiation risks from pediatric computed tomography scanning. Pediatr. Endocrinol. Rev. 2009, 7, 29–36. [Google Scholar]
- Artul, S.; Nseir, W.; Armaly, Z.; Soudack, M. Superb microvascular imaging: Added value and novel applications. J. Clin. Imaging Sci. 2017, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.Z.; Huang, Y.H.; Shen, H.L.; Liu, X.T. Clinical applications of superb microvascular imaging in the liver, breast, thyroid, skeletal muscle, and carotid plaques. J. Ultrasound Med. 2019, 38, 2811–2820. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, T.; Chavhan, G.B.; Avitzur, Y.; Moineddin, R.; Oudjhane, K. Doppler Parameters of the Hepatic Artery as Predictors of Graft Status in Pediatric Liver Transplantation. AJR Am. J. Roentgenol. 2017, 209, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Gu, L.H.; Fang, H.; Liu, X.S.; Xia, Q.; Li, F.H. Additional value of superb microvascular imaging for assessing hepatic arterial blood flow after pediatric liver transplantation. Pediatr. Transplant. 2020, 24, e13785. [Google Scholar] [CrossRef]
- Güven, F.; Karaca, L.; Ogul, H.; Sade, R.; Öztürk, G.; Kantarci, M. The Value of Superb Microvascular Imaging in Detecting Hepatic Artery Occlusion in Liver Transplantation: A Preliminary Study. Ultrasound Q. 2019, 35, 325–329. [Google Scholar] [CrossRef]
- Park, A.Y.; Seo, B.K.; Cha, S.H.; Yeom, S.K.; Lee, S.W.; Chung, H.H. An Innovative Ultrasound Technique for Evaluation of Tumor Vascularity in Breast Cancers: Superb Micro-Vascular Imaging. J. Breast Cancer 2016, 19, 210–213. [Google Scholar] [CrossRef]
- Machado, P.; Segal, S.; Lyshchik, A.; Forsberg, F. A Novel Microvascular Flow Technique: Initial Results in Thyroids. Ultrasound Q. 2016, 32, 67–74. [Google Scholar] [CrossRef]
- Ma, Y.; Li, G.; Li, J.; Ren, W.D. The Diagnostic Value of Superb Microvascular Imaging (SMI) in Detecting Blood Flow Signals of Breast Lesions: A Preliminary Study Comparing SMI to Color Doppler Flow Imaging. Medicine 2015, 94, e1502. [Google Scholar] [CrossRef]
- Karaca, L.; Oral, A.; Kantarci, M.; Sade, R.; Ogul, H.; Bayraktutan, U.; Okur, A.; Yüce, I. Comparison of the superb microvascular imaging technique and the color Doppler techniques for evaluating children’s testicular blood flow. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 1947–1953. [Google Scholar]
- Tokodai, K.; Miyagi, S.; Nakanishi, C.; Hara, Y.; Nakanishi, W.; Miyazawa, K.; Shimizu, K.; Goto, M.; Kamei, T.; Unno, M. The utility of superb microvascular imaging for monitoring low-velocity venous flow following pancreas transplantation: Report of a case. J. Med. Ultrason. 2018, 45, 171–174. [Google Scholar] [CrossRef]
- Mao, Y.; Mu, J.; Zhao, J.; Zhao, L.; Xin, X. The value of superb microvascular imaging in differentiating benign renal mass from malignant renal tumor: A retrospective study. Br. J. Radiol. 2018, 91, 20170601. [Google Scholar] [CrossRef] [PubMed]
- Ayaz, E.; Aslan, A.; Inan, I.; Yikilmaz, A. Evaluation of ovarian vascularity in children by using the “superb microvascular imaging” ultrasound technique in comparison with conventional Doppler ultrasound techniques. J. Ultrasound Med. 2019, 38, 2751–2760. [Google Scholar] [CrossRef] [PubMed]
- Mu, J.; Mao, Y.; Li, F.; Xin, X.; Zhang, S. Superb microvascular imaging is a rational choice for accurate bosniak classification of renal cystic masses. Br. J. Radiol. 2019, 92, 20181038. [Google Scholar] [CrossRef]
- Alis, D.; Erol, B.C.; Akbas, S.; Barut, K.; Kasapcopur, O.; Adaletli, I. Superb microvascular imaging compared with power Doppler ultrasound in assessing synovitis of the knee in juvenile idiopathic arthritis: A preliminary study. J. Ultrasound Med. 2019, 39, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Barletta, A.; Balbi, M.; Surace, A.; Caroli, A.; Radaelli, S.; Musto, F.; Saruggia, M.; Mangili, G.; Gerevini, S.; Sironi, S.; et al. Cerebral superb microvascular imaging in preterm neonates: In vivo evaluation of thalamic, striatal, and extrastriatal angioarchitecture. Neuroradiology 2021, 63, 1103–1112. [Google Scholar] [CrossRef]
- Jang, H.Y.; Kim, K.W.; Kim, S.Y.; Kim, J.S.; Choi, S.H.; Kim, S.Y.; Lee, S.G. Visibility of the graft hepatic artery using superb microvascular imaging in liver transplantation recipients: Initial experience. Acta Radiol. 2018, 59, 1326–1335. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Total population n | 73 |
| Age (years) Median (IQR) | 7 (5.8) |
| Sex n (%) | |
| F | 35 (47.9) |
| M | 38 (52.1) |
| Weight (kg) Median (IQR) | 19.95 (19) |
| Underlying liver disease n (%) | |
| Biliary atresia | 44 (60.3) |
| Cryptogenic primary cirrhosis | 8 (11) |
| Alagille syndrome | 6 (8.2) |
| Familial cholestasis | 4 (5.5) |
| Neoplasms | 4 (5.5) |
| Other | 7 (10) |
| Acute postoperative complications n (%) | 50 (68.5) |
| Parameter | CDI | SMI | p | |
|---|---|---|---|---|
| HA visibility score (0 to 2 points) Median (IQR) | 2.0 (1.00) | 2.0 (0.00) | 0.007 ** | |
| SWM (0 to 1 point) n (%), total 73 patients | Score 1 | 66 (90) | 68 (93) | |
| Score 0 | 7 (10) | 5 (7) | 0.765 | |
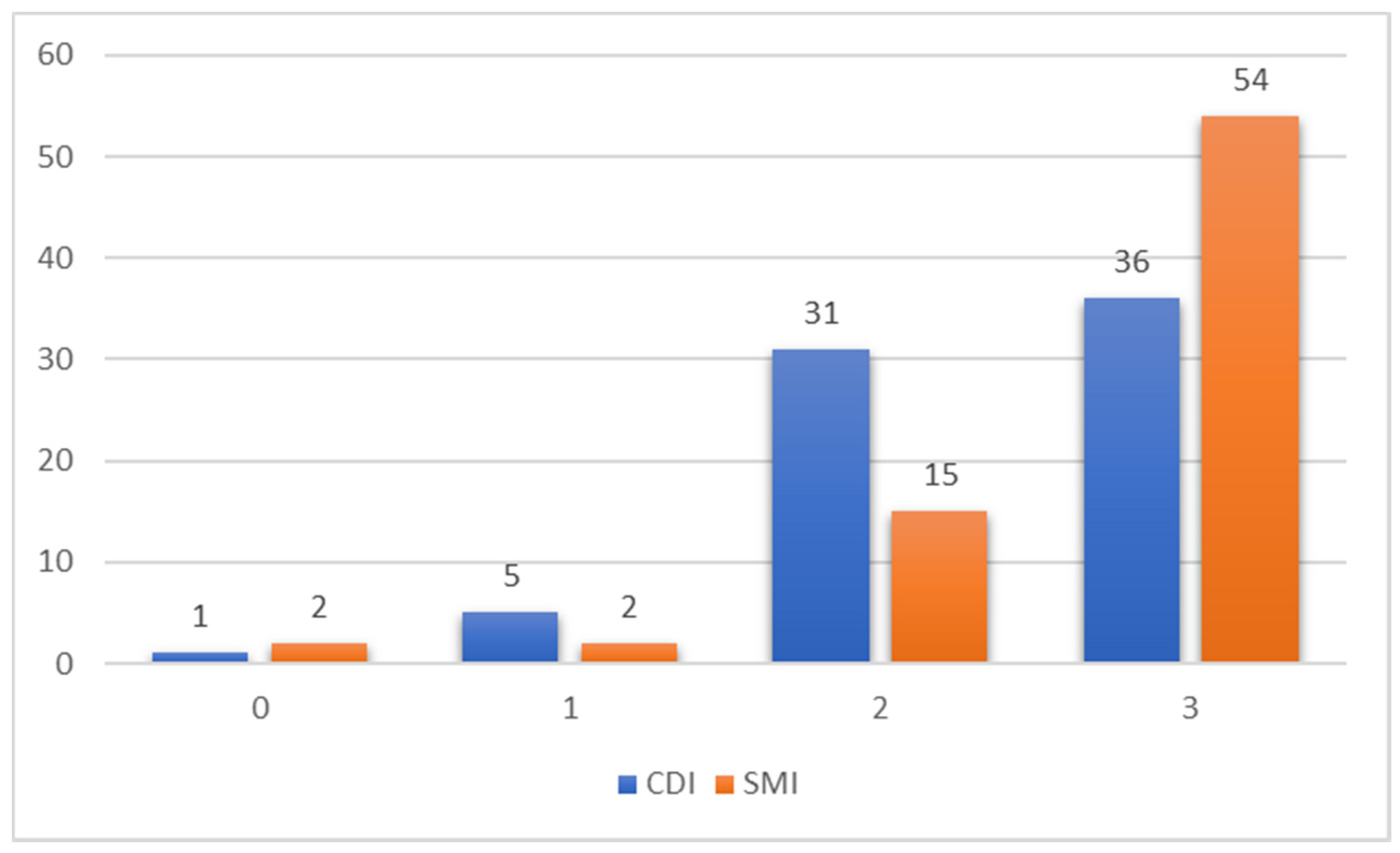
| Total score (0 to 3 points) Median (IQR) | 2.00 (1.00) | 3.00 (1.00) | 0.011 * | |
| Total score < 3 n (%) | 37 (50.7) | 19 (26.0) | 0.002 ** | |
| Total score = 3 n (%) | 36 (49.3) | 54 (74.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Collaku, E.; Simonini, R.; Balbi, M.; Bonaffini, P.A.; Valle, C.; Morzenti, C.; Faseli, R.F.; Ferrari, A.; Ippolito, D.; Marra, P.; et al. Superb Microvascular Imaging (SMI) Compared with Color Doppler Ultrasound for the Assessment of Hepatic Artery in Pediatric Liver Transplants: A Feasibility Study. Diagnostics 2022, 12, 1476. https://doi.org/10.3390/diagnostics12061476
Collaku E, Simonini R, Balbi M, Bonaffini PA, Valle C, Morzenti C, Faseli RF, Ferrari A, Ippolito D, Marra P, et al. Superb Microvascular Imaging (SMI) Compared with Color Doppler Ultrasound for the Assessment of Hepatic Artery in Pediatric Liver Transplants: A Feasibility Study. Diagnostics. 2022; 12(6):1476. https://doi.org/10.3390/diagnostics12061476
Chicago/Turabian StyleCollaku, Elona, Roberto Simonini, Maurizio Balbi, Pietro Andrea Bonaffini, Clarissa Valle, Cesare Morzenti, Romina Fatima Faseli, Alberto Ferrari, Davide Ippolito, Paolo Marra, and et al. 2022. "Superb Microvascular Imaging (SMI) Compared with Color Doppler Ultrasound for the Assessment of Hepatic Artery in Pediatric Liver Transplants: A Feasibility Study" Diagnostics 12, no. 6: 1476. https://doi.org/10.3390/diagnostics12061476