
Usefulness of Imaging and Biological Tools for the Characterization of Portal Vein Thrombosis in Hepatocellular Carcinoma

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Determination of AFP Values
2.3. Diagnostic of PVT
2.4. Diagnostic Reference Method
2.5. Extension of PVT
2.6. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Child–Pugh and Meld Classification
3.3. Portal Hypertension and PVT Extension
3.4. AFP Serum Levels for PVT Characterization
3.5. The Performance of CEUS for the Characterization of PVT
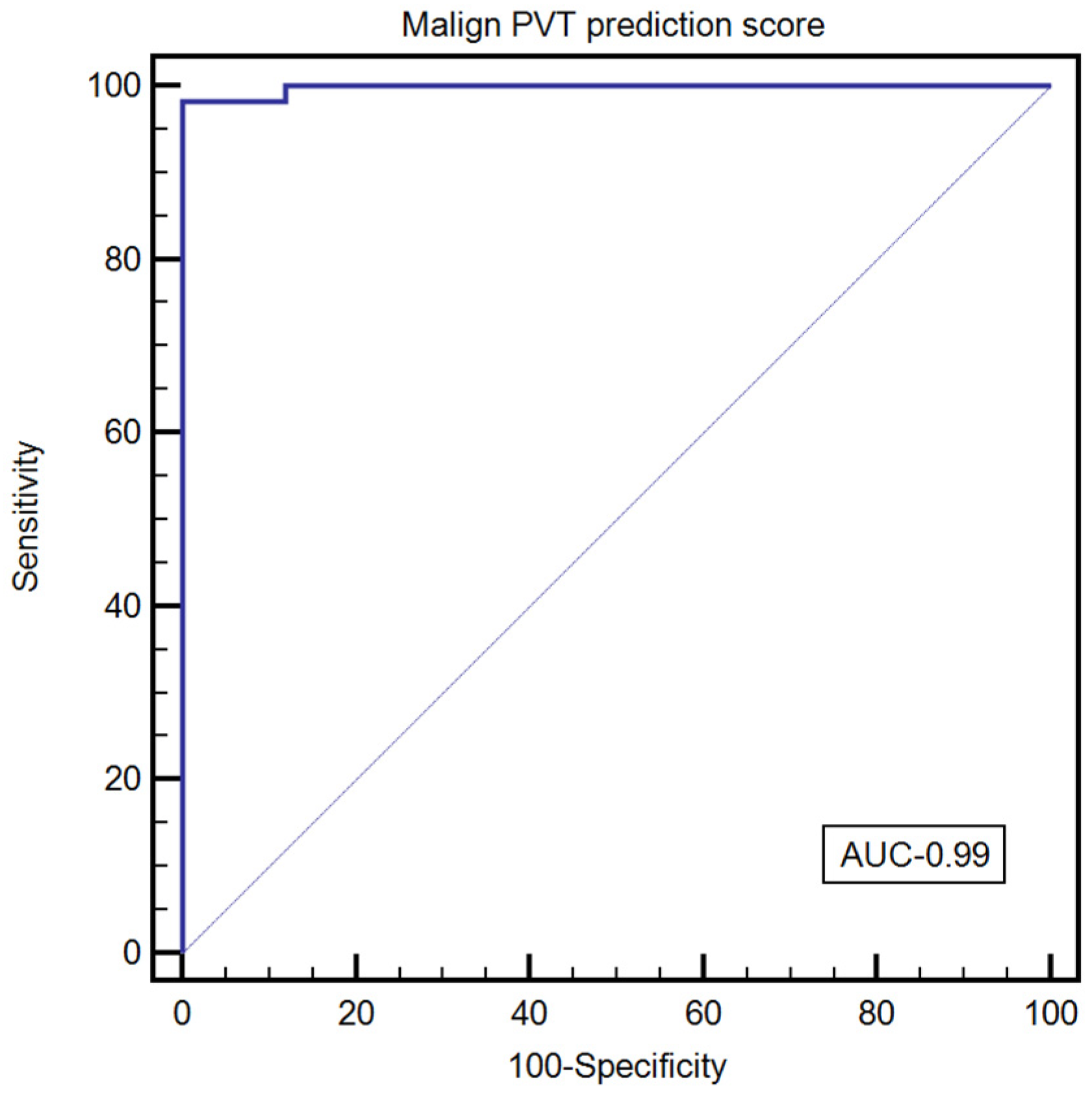
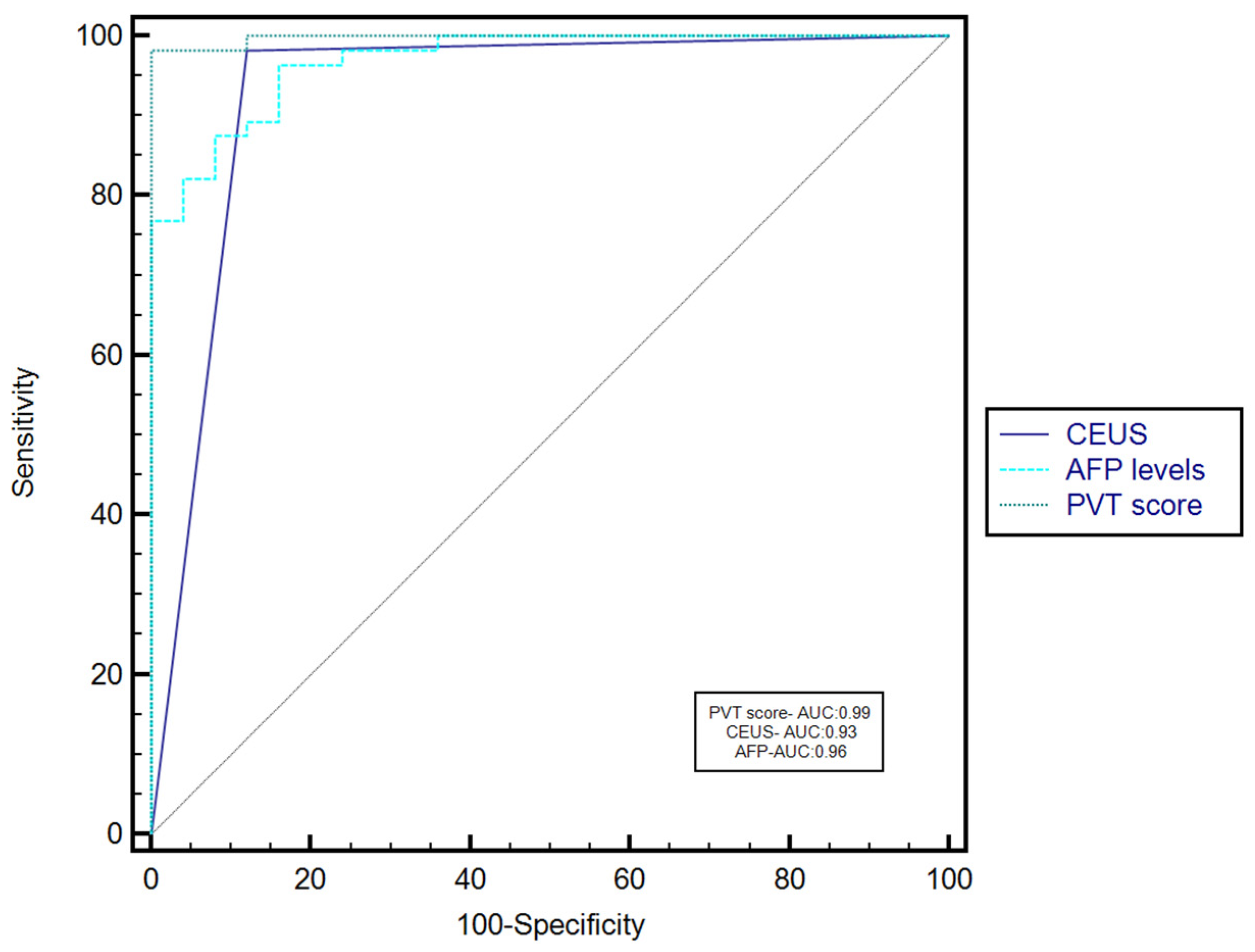
3.6. The Performance of the Combined Use of AFP Serum Levels and CEUS for the Characterization of PVT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- DeLeve, L.D.; Valla, D.C.; Garcia-Tsao, G.; American Association for the Study Liver Diseases. Vascular disorders of the liver. Hepatology 2009, 49, 1729–1764. [Google Scholar] [CrossRef] [PubMed]
- Nery, F.; Chevret, S.; Condat, B.; de Raucourt, E.; Boudaoud, L.; Rautou, P.-E.; Plessier, A.; Roulot, D.; Chaffaut, C.; Bourcier, V.; et al. Causes and consequences of portal vein thrombosis in 1243 patients with cirrhosis: Results of a longitudinal study. Hepatology 2015, 61, 660–667. [Google Scholar] [CrossRef]
- Ogren, M.; Bergqvist, D.; Björck, M.; Acosta, S.; Eriksson, H.; Sternby, N.H. Portal vein thrombosis: Prevalence, patient characteristics and lifetime risk: A population study based on 23,796 consecutive autopsies. World J. Gastroenterol. 2006, 12, 2115–2119. [Google Scholar] [CrossRef]
- Okuda, K.; Ohnishi, K.; Kimura, K.; Matsutani, S.; Sumida, M.; Goto, N.; Musha, H.; Takashi, M.; Suzuki, N.; Shinagawa, T.; et al. Incidence of portal vein thrombosis in liver cirrhosis. An angiographic study in 708 patients. Gastroenterology 1985, 89, 279–286. [Google Scholar] [CrossRef]
- Francoz, C.; Belghiti, J.; Vilgrain, V.; Sommacale, D.; Paradis, V.; Condat, B.; Denninger, M.H.; Sauvanet, A.; Valla, D.; Durand, F. Splanchnic vein thrombosis in candidates for liver transplantation: Usefulness of screening and anticoagulation. Gut 2005, 54, 691–697. [Google Scholar] [CrossRef]
- Condat, B.; Pessione, F.; Helene Denninger, M.; Hillaire, S.; Valla, D. Recent portal or mesenteric venous thrombosis: Increased recognition and frequent recanalization on anticoagulant therapy. Hepatology 2000, 32, 466–470. [Google Scholar] [CrossRef]
- Piscaglia, F.; Gianstefani, A.; Ravaioli, M.; Golfieri, R.; Cappelli, A.; Giampalma, E.; Sagrini, E.; Imbriaco, G.; Pinna, A.D.; Bolondi, L. Criteria for diagnosing benign portal vein thrombosis in the assessment of patients with cirrhosis and hepatocellular carcinoma for liver transplantation. Liver Transpl. 2010, 16, 658–667. [Google Scholar] [CrossRef]
- Trebicka, J.; Strassburg, C.P. Etiology and Complications of Portal Vein Thrombosis. Viszeralmedizin 2014, 30, 375–380. [Google Scholar] [CrossRef] [Green Version]
- Claudon, M.; Dietrich, C.F.; Choi, B.I.; Cosgrove, D.O.; Kudo, M.; Nolsøe, C.P.; Piscaglia, F.; Wilson, S.R.; Barr, R.G.; Chammas, M.C.; et al. Guidelines and good clinical practice recommendations for Contrast Enhanced Ultrasound (CEUS) in the liver—update 2012: A WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultrasound Med. Biol. 2013, 39, 187–210. [Google Scholar] [CrossRef]
- Sporea, I.; Badea, R.; Brisc, C.; Ioanițescu, S.; Moga, T.; Popescu, A.; Saftoiu, A.; Săndulescu, L.; Spârchez, Z.; Șirli, R. Romanian National Guidelines on Contrast Enhanced Ultrasound in clinical practice. Med. Ultrason. 2017, 19, 401–415. [Google Scholar] [CrossRef] [Green Version]
- Dietrich, C.F.; Nolsøe, C.P.; Barr, R.G.; Berzigotti, A.; Burns, P.N.; Cantisani, V.; Chammas, M.C.; Chaubal, N.; Choi, B.I.; Clevert, D.A.; et al. Guidelines and Good Clinical Practice Recommendations for Contrast-Enhanced Ultrasound (CEUS) in the Liver-Update 2020 WFUMB in Cooperation with EFSUMB, AFSUMB, AIUM, and FLAUS. Ultrasound Med. Biol. 2020, 46, 2579–2604. [Google Scholar] [CrossRef]
- Ghiuchici, A.M.; Dănilă, M.; Popescu, A.; Șirli, R.; Moga, T.; Topan, M.; Bende, F.; Sporea, I. Contrast-enhanced ultrasound algorithm (ACR CEUS LI-RADSv 2017)- a valuable tool for the noninvasive diagnosis of hepatocellular carcinoma in patients with chronic liver disease. Med. Ultrason. 2021, 23, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, P.; Cantisani, V.; Dietrich, C.F.; Gilja, O.H.; Saftoiu, A.; Bartels, E.; Bertolotto, M.; Calliada, F.; Clevert, D.A.; Cosgrove, D.; et al. The EFSUMB Guidelines and Recommendations for the Clinical Practice of Contrast-Enhanced Ultrasound (CEUS) in Non-Hepatic Applications: Update 2017 (Long Version). Die EFSUMB-Leitlinien und Empfehlungen für den klinischen Einsatz des kontrastverstärkten Ultraschalls (CEUS) bei nicht-hepatischen Anwendungen: Update 2017 (Langversion). Ultraschall Med. 2018, 39, e2–e44. [Google Scholar] [CrossRef] [Green Version]
- Lisotti, A.; Napoleon, B.; Facciorusso, A.; Cominardi, A.; Crinò, S.F.; Brighi, N.; Gincul, R.; Kitano, M.; Yamashita, Y.; Marchegiani, G.; et al. Contrast-enhanced EUS for the characterization of mural nodules within pancreatic cystic neoplasms: Systematic review and meta-analysis. Gastrointest. Endosc. 2021, 94, 881–889.e5. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- Omata, M.; Cheng, A.-L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.-H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef] [Green Version]
- Stekhin, A.; Yakovleva, G.; Pronko, K.; Zemskov, K.P.V. HCC with low- and normal-serum alpha-fetoprotein levels. Clin. Pract. 2018, 15, 453–464. [Google Scholar] [CrossRef] [Green Version]
- Kuwano, A.; Yada, M.; Nagasawa, S.; Tanaka, K.; Morita, Y.; Masumoto, A.; Motomura, K. Serum α-fetoprotein level at treatment completion is a useful predictor of hepatocellular carcinoma occurrence more than one year after hepatitis C virus eradication by direct-acting antiviral treatment. J. Viral. Hepat. 2022, 29, 35–42. [Google Scholar] [CrossRef]
- Pan, Y.-X.; Sun, X.-Q.; Hu, Z.-L.; Xie, W.; Nie, K.-X.; Fang, A.-P.; Zhang, Y.-Y.; Fu, Y.-Z.; Chen, J.-B.; Wang, J.-C.; et al. Prognostic Values of Alpha-Fetoprotein and Des-Gamma-Carboxyprothrombin in Hepatocellular Carcinoma in China: An Analysis of 4792 Patients. J. Hepatocell. Carcinoma 2021, 8, 657–670. [Google Scholar] [CrossRef] [PubMed]
- Biselli, M.; Conti, F.; Gramenzi, A.; Frigerio, M.; Cucchetti, A.; Fatti, G.; D’Angelo, M.; Dall’Agata, M.; Giannini, E.G.; Farinati, F.; et al. A new approach to the use of α-fetoprotein as surveillance test for hepatocellular carcinoma in patients with cirrhosis. Br. J. Cancer 2015, 112, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Akkız, H.; Carr, B.I.; Kuran, S.; Karaoğullarından, Ü.; Üsküdar, O.; Tokmak, S.; Arslan, B.; Doran, F.; Balli, H.T.; Ülkü, A.; et al. Macroscopic Portal Vein Thrombosis in HCC Patients. Can. J. Gastroenterol. Hepatol. 2018, 2018, 3120185. [Google Scholar] [CrossRef] [Green Version]
- de Franchis, R. Revising consensus in portal hypertension: Report of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension. J. Hepatol. 2010, 53, 762–768. [Google Scholar] [CrossRef] [Green Version]
- Wani, Z.A.; Bhat, R.A.; Bhadoria, A.S.; Maiwall, R.; Choudhury, A. Gastric varices: Classification, endoscopic and ultrasonographic management. J. Res. Med. Sci. 2015, 20, 1200–1207. [Google Scholar] [CrossRef]
- Yerdel, M.A.; Gunson, B.; Mirza, D.; Karayalçin, K.; Olliff, S.; Buckels, J.; Mayer, D.; McMaster, P.; Pirenne, J. Portal vein thrombosis in adults undergoing liver transplantation: Risk factors, screening, management, and outcome. Transplantation 2000, 69, 1873–1881. [Google Scholar] [CrossRef]
- Cheng, S.; Chen, M.; Cai, J.; Sun, J.; Guo, R.; Bi, X.; Lau, W.Y.; Wu, M.; on behalf of Chinese Association of Liver Cancer and Chinese Medical Doctor Association. Chinese Expert Consensus on Multidisciplinary Diagnosis and Treatment of Hepatocellular Carcinoma with Portal Vein Tumor Thrombus (2018 Edition). Liver Cancer 2020, 9, 28–40. [Google Scholar] [CrossRef]
- Raza, S.A.; Jang, H.J.; Kim, T.K. Differentiating malignant from benign thrombosis in hepatocellular carcinoma: Contrast-enhanced ultrasound. Abdom. Imaging 2014, 39, 153–161. [Google Scholar] [CrossRef]
- Tarantino, L.; Ambrosino, P.; Di Minno, M.N. Contrast-enhanced ultrasound in differentiating malignant from benign portal vein thrombosis in hepatocellular carcinoma. World J. Gastroenterol. 2015, 21, 9457–9460. [Google Scholar] [CrossRef]
- Rossi, S.; Ghittoni, G.; Ravetta, V.; Viera, F.T.; Rosa, L.; Serassi, M.; Scabini, M.; Vercelli, A.; Tinelli, C.; Bello, B.D.; et al. Contrast-enhanced ultrasonography and spiral computed tomography in the detection and characterization of portal vein thrombosis complicating hepatocellular carcinoma. Eur. Radiol. 2008, 18, 1749–1756. [Google Scholar] [CrossRef]
- Chen, J.; Zhu, J.; Zhang, C.; Song, Y.; Huang, P. Contrast-enhanced ultrasound for the characterization of portal vein thrombosis vs tumor-in-vein in HCC patients: A systematic review and meta-analysis. Eur. Radiol. 2020, 30, 2871–2880. [Google Scholar] [CrossRef] [Green Version]
- Trevisani, F.; D’Intino, P.E.; Morselli/labate, A.M.; Mazzella, G.; Accogli, E.; Caraceni, P.; Domenicali, M.; De Notariis, S.; Roda, E.; Bernardi, M. Serum alpha-fetoprotein for diagnosis of hepatocellular carcinoma in patients with chronic liver disease: Influence of HBsAg and anti-HCV status. J. Hepatol. 2001, 34, 570–575. [Google Scholar] [CrossRef]
- Tateishi, R.; Yoshida, H.; Matsuyama, Y.; Mine, N.; Kondo, Y.; Omata, M. Diagnostic accuracy of tumor markers for hepatocellular carcinoma: A systematic review. Hepatol. Int. 2008, 2, 17–30. [Google Scholar] [CrossRef] [Green Version]
- Carr, B.I.; Guerra, V.; Donghia, R. Portal Vein Thrombosis and Markers of Inflammation in Hepatocellular Carcinoma. J. Gastrointest. Cancer 2020, 51, 1141–1147. [Google Scholar] [CrossRef]
- Nonami, T.; Yokoyama, I.; Iwatsuki, S.; Starzl, T.E. The incidence of portal vein thrombosis at liver transplantation. Hepatology 1992, 16, 1195–1198. [Google Scholar] [CrossRef]
- Bagheri Lankarani, K.; Homayon, K.; Motevalli, D.; Heidari, S.T.; Alavian, S.M.; Malek-Hosseini, S.A. Risk Factors for Portal Vein Thrombosis in Patients with Cirrhosis Awaiting Liver Transplantation in Shiraz, Iran. Hepat. Mon. 2015, 15, e26407. [Google Scholar] [CrossRef] [Green Version]
- Pirisi, M.; Avellini, C.; Fabris, C.; Scott, C.; Bardus, P.; Soardo, G.; Beltrami, C.A.; Bartoli, E. Portal vein thrombosis in hepatocellular carcinoma: Age and sex distribution in an autopsy study. J. Cancer Res. Clin. Oncol. 1998, 124, 397–400. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | n = 101 |
|---|---|
| Age (years) | 62.7 ± 9.2 |
| Gender | |
| Men | 73 (72.3%) |
| Women | 28 (27.7%) |
| Etiology of PVT: Liver cirrhosis with HCC | 77(76.2%) |
| Liver cirrhosis without HCC | 24 (23.8%) |
| Etiology of liver cirrhosis in patients with HCC | n = 77 |
| HCV | 27 (35.1%) |
| HBV | 15 (19.5%) |
| HBV + HDV | 2 (2.6%) |
| HBV + HCV | 2 (2.6%) |
| ALD | 16 (20.7%) |
| ALD + HCV | 5 (6.5%) |
| ALD + HBV | 1 (1.3%) |
| NAFLD | 2 (2.6%) |
| Cryptogenic | 7 (9.1%) |
| Etiology of liver cirrhosis in patients without HCC | n = 24 |
| AH | 1 (4.2%) |
| HCV | 6 (25%) |
| PBC | 1 (4.2%) |
| SSC | 1 (4.2%) |
| ALD | 9 (37.5%) |
| HBV | 2 (8.3%) |
| HBV + HDV | 2 (8.3%) |
| HBV + ALD | 1 (4.2%) |
| NAFLD | 1 (4.2%) |
| Subjects without HCC n = 22 | Subjects with HCC n = 62 | p-Value | |
| No or small EV (grade 1) | 7 (31.8%) | 19 (30.6%) | 0.8698 |
| Grade 2 and 3 EV | 11 (50%) | 30 (48.4%) | 0.9051 |
| EV and GV | 4 (18.2%) | 13 (21%) | 0.9777 |
| Subjects with TIV n= 61 | Subjects with Benign PVT n = 23 | p-Value | |
| No or small EV (grade 1) | 20 (32.8%) | 6 (26.1%) | 0.7532 |
| Grade 2 and 3 EV | 31 (50.8%) | 10 (43.5%) | 0.7248 |
| EV and GV | 10 (16.4%) | 7 (30.4%) | 0.2629 |
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | |
|---|---|---|---|---|
| Patients with HCC n = 77 | 31 (40.3%) | 35 (45.4) | 5 (6.5%) | 6 (7.8%) |
| Patients without HCC n = 24 | 9 (37.5%) | 8 (33.3%) | 5 (20.8%) | 2 (8.4%) |
| Subjects | CEUS | CT/MRI | p-Value |
|---|---|---|---|
| Subjects with HCC n = 77 | 72 (93.5%) TIV 5 (6.5%) benign PVT | 72 (93.5%) TIV 5 (6.5%) benign PVT | 0.7438 0.7438 |
| Subjects without HCC n = 24 | 3 (12.5%) TIV 21 (87.5%) benign PVT | 1 (4.2%) TIV 23 (95.8%) benign PVT | 0.6047 0.6047 |
| PVT Grade | CEUS Performance | Correctly Classified Subjects (%) | |||
|---|---|---|---|---|---|
| Sensitivity | Se 95%CI | Specificity | Sp 95%CI | ||
| I | 100% | 87.7–100% | 83.3% | 51.6–97.9% | 95% (38/40) |
| II | 100% | 89.7–100% | 100% | 66.4–100% | 100% (43/43) |
| III | 100% | 47.8–100% | 80% | 28.4–99.5% | 100% (10/10) |
| IV | 83.3% | 35.9–99.6 | 100% | 15.8–100% | 87.5% (7/8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burciu, C.; Șirli, R.; Bende, F.; Fofiu, R.; Popescu, A.; Sporea, I.; Ghiuchici, A.-M.; Miuțescu, B.; Dănilă, M. Usefulness of Imaging and Biological Tools for the Characterization of Portal Vein Thrombosis in Hepatocellular Carcinoma. Diagnostics 2022, 12, 1145. https://doi.org/10.3390/diagnostics12051145
Burciu C, Șirli R, Bende F, Fofiu R, Popescu A, Sporea I, Ghiuchici A-M, Miuțescu B, Dănilă M. Usefulness of Imaging and Biological Tools for the Characterization of Portal Vein Thrombosis in Hepatocellular Carcinoma. Diagnostics. 2022; 12(5):1145. https://doi.org/10.3390/diagnostics12051145
Chicago/Turabian StyleBurciu, Călin, Roxana Șirli, Felix Bende, Renata Fofiu, Alina Popescu, Ioan Sporea, Ana-Maria Ghiuchici, Bogdan Miuțescu, and Mirela Dănilă. 2022. "Usefulness of Imaging and Biological Tools for the Characterization of Portal Vein Thrombosis in Hepatocellular Carcinoma" Diagnostics 12, no. 5: 1145. https://doi.org/10.3390/diagnostics12051145