
Artificial Intelligence and Machine Learning in the Diagnosis and Management of Gastroenteropancreatic Neuroendocrine Neoplasms—A Scoping Review


Abstract
:1. Introduction
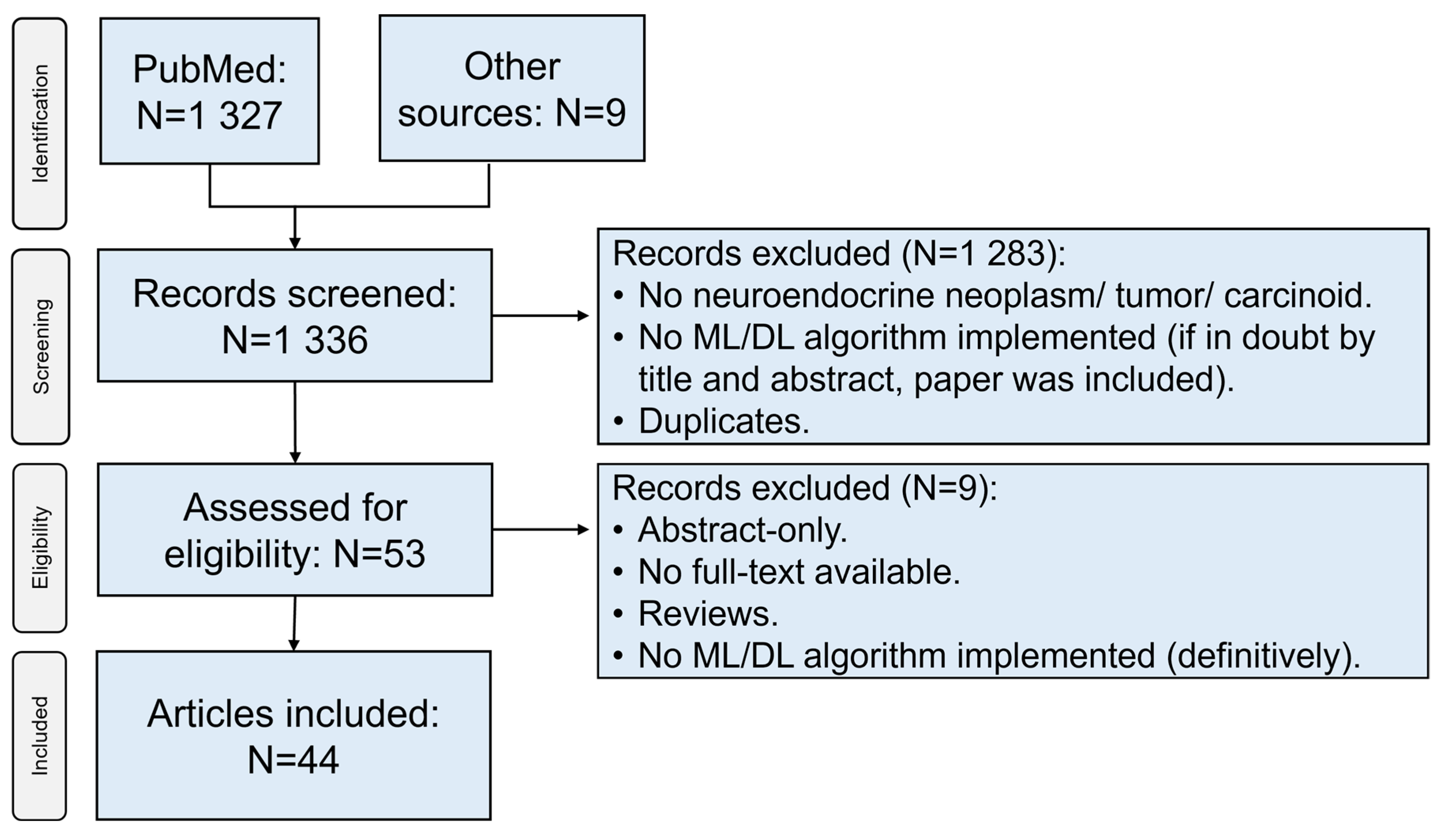
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bonds, M.; Rocha, F.G. Neuroendocrine Tumors of the Pancreatobiliary and Gastrointestinal Tracts. Surg. Clin. 2020, 100, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Clift, A.K.; Kidd, M.; Bodei, L.; Toumpanakis, C.; Baum, R.P.; Oberg, K.; Modlin, I.M.; Frilling, A. Neuroendocrine Neoplasms of the Small Bowel and Pancreas. Neuroendocrinology 2020, 110, 444–476. [Google Scholar] [CrossRef] [PubMed]
- Pavel, M.; Öberg, K.; Falconi, M.; Krenning, E.P.; Sundin, A.; Perren, A.; Berruti, A. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 844–860. [Google Scholar] [CrossRef]
- Modlin, I.M.; Kidd, M.; Latich, I.; Zikusoka, M.N.; Shapiro, M.D. Current Status of Gastrointestinal Carcinoids. Gastroenterology 2005, 128, 1717–1751. [Google Scholar] [CrossRef] [PubMed]
- IARC Publications Website—Digestive System Tumours. Available online: https://publications.iarc.fr/579 (accessed on 26 February 2022).
- Loftus, T.J.; Tighe, P.J.; Filiberto, A.C.; Efron, P.A.; Brakenridge, S.C.; Mohr, A.M.; Rashidi, P.; Upchurch, G.R., Jr.; Bihorac, A. Artificial Intelligence and Surgical Decision-Making. JAMA Surg. 2020, 155, 148–158. Available online: https://jamanetwork.com/journals/jamasurgery/fullarticle/2756311 (accessed on 18 December 2019). [CrossRef] [PubMed]
- Yu, K.H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Luo, W.; Phung, Q.-D.; Tran, T.; Gupta, S.; Rana, S.; Karmakar, C.; Shilton, A.; Yearwood, J.L.; Dimitrova, N.; Ho, T.B.; et al. Guidelines for Developing and Reporting Machine Learning Predictive Models in Biomedical Research: A Multidisciplinary View. J. Med. Internet Res. 2016, 18, e323. [Google Scholar] [CrossRef] [Green Version]
- Bevilacqua, A.; Calabrò, D.; Malavasi, S.; Ricci, C.; Casadei, R.; Campana, D.; Baiocco, S.; Fanti, S.; Ambrosini, V. A [68Ga] Ga-DOTANOC PET/CT Radiomic Model for Non-Invasive Prediction of Tumour Grade in Pancreatic Neuroendocrine Tumours. Diagnostics 2021, 11, 870. [Google Scholar] [CrossRef]
- Chen, K.; Zhang, W.; Zhang, Z.; He, Y.; Liu, Y.; Yang, X. Simple Vascular Architecture Classification in Predicting Pancreatic Neuroendocrine Tumor Grade and Prognosis. Am. J. Dig. Dis. 2018, 63, 3147–3152. [Google Scholar] [CrossRef]
- Ito, H.; Uragami, N.; Miyazaki, T.; Yang, W.; Issha, K.; Matsuo, K.; Kimura, S.; Arai, Y.; Tokunaga, H.; Okada, S.; et al. Highly accurate colorectal cancer prediction model based on Raman spectroscopy using patient serum. World J. Gastrointest. Oncol. 2020, 12, 1311–1324. [Google Scholar] [CrossRef] [PubMed]
- Kidd, M.; Kitz, A.; Drozdov, I.A.; Modlin, I.M. Neuroendocrine Tumor Omic Gene Cluster Analysis Amplifies the Prognostic Accuracy of the NETest. Neuroendocrinology 2021, 111, 490–504. [Google Scholar] [CrossRef] [PubMed]
- Kjellman, M.; Knigge, U.; Welin, S.; Thiis-Evensen, E.; Gronbaek, H.; Schalin-Jäntti, C.; Sorbye, H.; Joergensen, M.T.; Johanson, V.; Metso, S.; et al. A Plasma Protein Biomarker Strategy for Detection of Small Intestinal Neuroendocrine Tumors. Neuroendocrinology 2021, 111, 840–849. [Google Scholar] [CrossRef] [PubMed]
- Klimov, S.; Xue, Y.; Gertych, A.; Graham, R.P.; Jiang, Y.; Bhattarai, S.; Pandol, S.J.; Rakha, E.A.; Reid, M.D.; Aneja, R. Predicting Metastasis Risk in Pancreatic Neuroendocrine Tumors Using Deep Learning Image Analysis. Front. Oncol. 2021, 10, 593211. [Google Scholar] [CrossRef]
- Liu, Y.; Sadowski, S.M.; Weisbrod, A.B.; Kebebew, E.; Summers, R.M.; Yao, J. Patient specific tumor growth prediction using multimodal images. Med. Image Anal. 2014, 18, 555–566. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Chen, X.; Chen, J.; Song, C.; Shen, J.; Xiao, H.; Chen, M.; Li, Z.-P.; Huang, B.; Feng, S.-T. Preoperative Prediction of Pancreatic Neuroendocrine Neoplasms Grading Based on Enhanced Computed Tomography Imaging: Validation of Deep Learning with a Convolutional Neural Network. Neuroendocrinology 2020, 110, 338–350. [Google Scholar] [CrossRef]
- Nanayakkara, J.; Tyryshkin, K.; Yang, X.; Wong, J.J.M.; Vanderbeck, K.; Ginter, P.S.; Scognamiglio, T.; Chen, Y.-T.; Panarelli, N.; Cheung, N.-K.; et al. Characterizing and classifying neuroendocrine neoplasms through microRNA sequencing and data mining. NAR Cancer 2020, 2, zcaa009. [Google Scholar] [CrossRef]
- Nguyen, V.X.; Nguyen, C.C.; Li, B.; Das, A. Digital image analysis is a useful adjunct to endoscopic ultrasonographic diagnosis of subepithelial lesions of the gastrointestinal tract. J. Ultrasound Med. 2010, 29, 1345–1351. [Google Scholar] [CrossRef]
- Niazi, M.K.K.; Tavolara, T.E.; Arole, V.; Hartman, U.J.; Pantanowitz, L.; Gurcan, M.N. Identifying tumor in pancreatic neuroendocrine neoplasms from Ki67 images using transfer learning. PLoS ONE 2018, 13, e0195621. [Google Scholar] [CrossRef] [Green Version]
- Panarelli, N.; Tyryshkin, K.; Wong, J.; Majewski, A.; Yang, X.; Scognamiglio, T.; Kim, M.K.; Bogardus, K.; Tuschl, T.; Chen, Y.-T.; et al. Evaluating gastroenteropancreatic neuroendocrine tumors through microRNA sequencing. Endocr. Relat. Cancer 2019, 26, 47–57. [Google Scholar] [CrossRef]
- Cheng, X.; Li, J.; Xu, T.; Li, K.; Li, J. Predicting Survival of Patients With Rectal Neuroendocrine Tumors Using Machine Learning: A SEER-Based Population Study. Front. Surg. 2021, 8, 745220. [Google Scholar] [CrossRef] [PubMed]
- Hanson, J.A.; Redemann, J.; Schultz, F.A.; Martinez, C.; Harrell, M.; Clark, D.P.; Martin, D.R. Comparing deep learning and immunohistochemistry in determining the site of origin for well-differentiated neuroendocrine tumors. J. Pathol. Inform. 2020, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Saccomandi, P.; Larocca, E.S.; Rendina, V.; Schena, E.; D’Ambrosio, R.; Crescenzi, A.; Di Matteo, F.M.; Silvestri, S. Estimation of optical properties of neuroendocrine pancreas tumor with double-integrating-sphere system and inverse Monte Carlo model. Lasers Med. Sci. 2016, 31, 1041–1050. [Google Scholar] [CrossRef] [PubMed]
- Săftoiu, A.; Vilmann, P.; Gorunescu, F.; Gheonea, D.I.; Gorunescu, M.; Ciurea, T.; Popescu, G.L.; Iordache, A.; Hassan, H.; Iordache, S. Neural network analysis of dynamic sequences of EUS elastography used for the differential diagnosis of chronic pancreatitis and pancreatic cancer. Gastrointest. Endosc. 2008, 68, 1086–1094. [Google Scholar] [CrossRef] [PubMed]
- Soldevilla, B.; López-López, A.; Lens-Pardo, A.; Carretero-Puche, C.; Lopez-Gonzalvez, A.; La Salvia, A.; Gil-Calderon, B.; Riesco-Martinez, M.; Espinosa-Olarte, P.; Sarmentero, J.; et al. Comprehensive Plasma Metabolomic Profile of Patients with Advanced Neuroendocrine Tumors (NETs). Diagnostic and Biological Relevance. Cancers 2021, 13, 2634. [Google Scholar] [CrossRef]
- Song, Y.; Gao, S.; Tan, W.; Qiu, Z.; Zhou, H.; Zhao, Y. Multiple Machine Learnings Revealed Similar Predictive Accuracy for Prognosis of PNETs from the Surveillance, Epidemiology, and End Result Database. J. Cancer 2018, 9, 3971–3978. [Google Scholar] [CrossRef]
- Song, C.; Wang, M.; Luo, Y.; Chen, J.; Peng, Z.; Wang, Y.; Zhang, H.; Li, Z.-P.; Shen, J.; Huang, B.; et al. Predicting the recurrence risk of pancreatic neuroendocrine neoplasms after radical resection using deep learning radiomics with preoperative computed tomography images. Ann. Transl. Med. 2021, 9, 833. [Google Scholar] [CrossRef]
- Telalovic, J.H.; Pillozzi, S.; Fabbri, R.; Laffi, A.; Lavacchi, D.; Rossi, V.; Dreoni, L.; Spada, F.; Fazio, N.; Amedei, A.; et al. A Machine Learning Decision Support System (DSS) for Neuroendocrine Tumor Patients Treated with Somatostatin Analog (SSA) Therapy. Diagnostics 2021, 11, 804. [Google Scholar] [CrossRef]
- Tirosh, A.; Mukherjee, S.; Lack, J.; Gara, S.K.; Wang, S.; Quezado, M.M.; Keutgen, X.M.; Wu, X.; Cam, M.; Kumar, S.; et al. Distinct genome-wide methylation patterns in sporadic and hereditary nonfunctioning pancreatic neuroendocrine tumors. Cancer 2019, 125, 1247–1257. [Google Scholar] [CrossRef]
- Udriștoiu, A.L.; Cazacu, I.M.; Gruionu, L.G.; Gruionu, G.; Iacob, A.V.; Burtea, D.E.; Ungureanu, B.S.; Costache, M.I.; Constantin, A.; Popescu, C.F.; et al. Real-time computer-aided diagnosis of focal pancreatic masses from endoscopic ultrasound imaging based on a hybrid convolutional and long short-term memory neural network model. PLoS ONE 2021, 16, e0251701. [Google Scholar] [CrossRef]
- van Gerven, M.A.; Jurgelenaite, R.; Taal, B.G.; Heskes, T.; Lucas, P.J. Predicting carcinoid heart disease with the noisy-threshold classifier. Artif. Intell. Med. 2007, 40, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Drozdov, I.; Kidd, M.; Nadler, B.; Camp, R.L.; Mane, S.M.; Hauso, O.; Gustafsson, B.I.; Modlin, I.M. Predicting neuroendocrine tumor (carcinoid) neoplasia using gene expression profiling and supervised machine learning. Cancer 2009, 115, 1638–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, Y.; Yang, P.; Xu, L.; Yang, J.; Luo, C.; Wang, J.; Chen, F.; Wu, Y.; Lu, Y.; Ruan, D.; et al. Radiomics analysis combining unsupervised learning and handcrafted features: A multiple-disease study. Med. Phys. 2021, 48, 7003–7015. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Yu, C. Expression profiling of small intestinal neuroendocrine tumors identified pathways and gene networks linked to tumorigenesis and metastasis. Biosci. Rep. 2020, 40, BSR20193860. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Li, F.; Jiang, Q.; Sun, Y.; Liao, Q.; An, H.; Li, Y.; Li, Z.; Fan, L.; Guo, F.; et al. Gene Expression Profiling for Differential Diagnosis of Liver Metastases: A Multicenter, Retrospective Cohort Study. Front. Oncol. 2021, 11, 725988. [Google Scholar] [CrossRef] [PubMed]
- Wehrend, J.; Silosky, M.; Xing, F.; Chin, B.B. Automated liver lesion detection in 68Ga DOTATATE PET/CT using a deep fully convolutional neural network. EJNMMI Res. 2021, 11, 98. [Google Scholar] [CrossRef]
- Xing, F.; Su, H.; Yang, L. An Integrated Framework for Automatic Ki-67 Scoring in Pancreatic Neuroendocrine Tumor. Med. Image Comput. Comput. Assist. Interv. 2013, 16, 436–443. [Google Scholar] [CrossRef]
- Xing, F.; Su, H.; Neltner, J.; Yang, L. Automatic Ki-67 Counting Using Robust Cell Detection and Online Dictionary Learning. IEEE Trans. Biomed. Eng. 2014, 61, 859–870. [Google Scholar] [CrossRef]
- Xing, F.; Yang, L. Fast Cell Segmentation Using Scalable Sparse Manifold Learning and Affine Transform-Approximated Active Contour. Med. Image Comput. Comput. Assist. Interv. 2015, 9351, 332–339. [Google Scholar] [CrossRef] [Green Version]
- Xing, F.; Shi, X.; Zhang, Z.; Cai, J.; Xie, Y.; Yang, L. Transfer Shape Modeling Towards High-Throughput Microscopy Image Segmentation. Med. Image Comput. Comput. Assist. Interv. 2016, 9902, 183–190. [Google Scholar] [CrossRef] [Green Version]
- Xing, F.; Xie, Y.; Yang, L. An Automatic Learning-Based Framework for Robust Nucleus Segmentation. IEEE Trans. Med. Imaging 2016, 35, 550–566. [Google Scholar] [CrossRef] [PubMed]
- Xing, F.; Cornish, T.C.; Bennett, T.; Ghosh, D.; Yang, L. Pixel-to-Pixel Learning With Weak Supervision for Single-Stage Nucleus Recognition in Ki67 Images. IEEE Trans. Biomed. Eng. 2019, 66, 3088–3097. [Google Scholar] [CrossRef] [PubMed]
- Fehrenbach, U.; Xin, S.; Hartenstein, A.; Auer, T.; Dräger, F.; Froböse, K.; Jann, H.; Mogl, M.; Amthauer, H.; Geisel, D.; et al. Automatized Hepatic Tumor Volume Analysis of Neuroendocrine Liver Metastases by Gd-EOB MRI—A Deep-Learning Model to Support Multidisciplinary Cancer Conference Decision-Making. Cancers 2021, 13, 2726. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Cornish, T.C.; Yang, L.; Bennett, T.D.; Ghosh, D.; Xing, F. Generative Adversarial Domain Adaptation for Nucleus Quantification in Images of Tissue Immunohistochemically Stained for Ki-67. JCO Clin. Cancer Inform. 2020, 4, 666–679. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Zhang, Y.; Liu, X.; Xu, H.; Chen, C.; Zhou, X.; Liu, Y.; Ma, X. Application of Radiomics Analysis Based on CT Combined With Machine Learning in Diagnostic of Pancreatic Neuroendocrine Tumors Patient’s Pathological Grades. Front. Oncol. 2021, 10, 521831. [Google Scholar] [CrossRef]
- Zhou, R.-Q.; Ji, H.-C.; Liu, Q.; Zhu, C.-Y.; Liu, R. Leveraging machine learning techniques for predicting pancreatic neuroendocrine tumor grades using biochemical and tumor markers. World J. Clin. Cases 2019, 7, 1611–1622. [Google Scholar] [CrossRef]
- Zimmerman, N.M.; Ray, D.; Princic, N.; Moynihan, M.; Clarke, C.; Phan, A. Exploration of machine learning techniques to examine the journey to neuroendocrine tumor diagnosis with real-world data. Futur. Oncol. 2021, 17, 3217–3230. [Google Scholar] [CrossRef]
- Gao, X.; Wang, X. Deep learning for World Health Organization grades of pancreatic neuroendocrine tumors on contrast-enhanced magnetic resonance images: A preliminary study. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1981–1991. [Google Scholar] [CrossRef]
- Govind, D.; Jen, K.-Y.; Matsukuma, K.; Gao, G.; Olson, K.A.; Gui, D.; Wilding, G.E.; Border, S.P.; Sarder, P. Improving the accuracy of gastrointestinal neuroendocrine tumor grading with deep learning. Sci. Rep. 2020, 10, 11064. [Google Scholar] [CrossRef]
- Han, X.; Yang, J.; Luo, J.; Chen, P.; Zhang, Z.; Alu, A.; Xiao, Y.; Ma, X. Application of CT-Based Radiomics in Discriminating Pancreatic Cystadenomas From Pancreatic Neuroendocrine Tumors Using Machine Learning Methods. Front. Oncol. 2021, 11, 606677. [Google Scholar] [CrossRef]
- Huang, B.; Tian, J.; Zhang, H.; Luo, Z.; Qin, J.; Huang, C.; He, X.; Luo, Y.; Zhou, Y.; Dan, G.; et al. Deep Semantic Segmentation Feature-Based Radiomics for the Classification Tasks in Medical Image Analysis. IEEE J. Biomed. Health Inform. 2021, 25, 2655–2664. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Lin, X.; Shen, J.; Chen, X.; Chen, J.; Li, Z.-P.; Wang, M.; Yuan, C.; Diao, X.-F.; Luo, Y.; et al. Accurate and Feasible Deep Learning Based Semi-Automatic Segmentation in CT for Radiomics Analysis in Pancreatic Neuroendocrine Neoplasms. IEEE J. Biomed. Health Inform. 2021, 25, 3498–3506. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, S.; Seneviratne, N.; Baig, M.S.; Khan, A.H.A. Artificial Intelligence in Medicine: Where Are We Now? Acad. Radiol. 2020, 27, 62–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. Eur. J. Clin. Investig. 2015, 45, 204–214. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, J.; Lehne, M.; Schepers, J.; Prasser, F.; Thun, S. The use of machine learning in rare diseases: A scoping review. Orphanet J. Rare Dis. 2020, 15, 145. [Google Scholar] [CrossRef]
- F1 Score vs ROC AUC vs Accuracy vs PR AUC: Which Evaluation Metric Should You Choose?—Neptune.ai. Available online: https://neptune.ai/blog/f1-score-accuracy-roc-auc-pr-auc (accessed on 27 February 2022).
- de Hond, A.A.H.; Leeuwenberg, A.M.; Hooft, L.; Kant, I.M.J.; Nijman, S.W.J.; van Os, H.J.A.; Aardoom, J.J.; Debray, T.P.A.; Schuit, E.; van Smeden, M.; et al. Guidelines and quality criteria for artificial intelligence-based prediction models in healthcare: A scoping review. Npj Digit. Med. 2022, 5, 2. [Google Scholar] [CrossRef]
- Yang, Y.; Li, Y.-X.; Yao, R.-Q.; Du, X.-H.; Ren, C. Artificial intelligence in small intestinal diseases: Application and prospects. World J. Gastroenterol. 2021, 27, 3734–3747. [Google Scholar] [CrossRef]
- Kim, J.H.; Nam, S.-J.; Park, S.C. Usefulness of artificial intelligence in gastric neoplasms. World J. Gastroenterol. 2021, 27, 3543–3555. [Google Scholar] [CrossRef]
- Bartoli, M.; Barat, M.; Dohan, A.; Gaujoux, S.; Coriat, R.; Hoeffel, C.; Cassinotto, C.; Chassagnon, G.; Soyer, P. INVITED REVIEW CT and MRI of pancreatic tumors: An update in the era of radiomics. Jpn. J. Radiol. 2020, 38, 1111–1124. [Google Scholar] [CrossRef]
- Partouche, E.; Yeh, R.; Eche, T.; Rozenblum, L.; Carrere, N.; Guimbaud, R.; Dierickx, L.O.; Rousseau, H.; Dercle, L.; Mokrane, F.-Z. Updated Trends in Imaging Practices for Pancreatic Neuroendocrine Tumors (PNETs): A Systematic Review and Meta-Analysis to Pave the Way for Standardization in the New Era of Big Data and Artificial Intelligence. Front. Oncol. 2021, 11, 628408. [Google Scholar] [CrossRef]
- Bezzi, C.; Mapelli, P.; Presotto, L.; Neri, I.; Scifo, P.; Savi, A.; Bettinardi, V.; Partelli, S.; Gianolli, L.; Falconi, M.; et al. Radiomics in pancreatic neuroendocrine tumors: Methodological issues and clinical significance. Eur. J. Pediatr. 2021, 48, 4002–4015. [Google Scholar] [CrossRef] [PubMed]
- Kuntz, S.; Krieghoff-Henning, E.; Kather, J.N.; Jutzi, T.; Höhn, J.; Kiehl, L.; Hekler, A.; Alwers, E.; von Kalle, C.; Fröhling, S.; et al. Gastrointestinal cancer classification and prognostication from histology using deep learning: Systematic review. Eur. J. Cancer 2021, 155, 200–215. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Inclusion Criteria |
|---|---|
| Population | Diagnosed cases with NEN (NET/NEC) or NEN included in the differential diagnosis. |
| Intervention | Analysis with a ML/DL algorithm. |
| Comparison | External validation desired but not mandatory. |
| Outcome | Report of accuracy, F1-score, AUROC or AUPRC desired but not mandatory. |
| Study design | Any. Abstract-only studies were excluded |
| Study ID | Prediction Characteristics | Technical Characteristics | Datasets & Benchmarking | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Author | Year of Publication | DOI | Ref. No. | Study Design | Nature of Prediction | Continuity of Output | NET Type | Source of Data | Tested AI Algortihm(s) | Training | AUC-Training | Cross-Validation | Test | AUC-Test | Ext. Validation | AUC |
| Bevilacqua A | 2021 | 10.3390/diagnostics11050870 | [10] | Prospective | Prognostic | Classification | Pancreas | Histology | LDA-model A | Y | 0.870–0.940 | 3-fold x100 | Y | 0.870–0.900 | N | |
| Chen K | 2018 | 10.1016/S1470-2045(20)30323-5 | [11] | Retrospective | Prognostic | Classification | Pancreas | Imaging (EUS) | DT, LR, NN, RF, SVM | N | N | Y | 0.879–0.997 | N | ||
| Cheng X | 2021 | 10.3389/fsurg.2021.745220 | [22] | Retrospective | Prognostic | Classification | Rectum | Database | AdaBoost, NB, Nu-SVC, SVC, RF, XGB | Y | 0.780–0.850 | 10-fold | Y | 0.890 | Y | 0.830–0.890 |
| Drozdov I | 2009 | 10.1002/cncr.24180 | [33] | Prospective | Diagnostic | Classification | Primary small intestine; metastatic liver | Histology | DT, SVM | Y | 10-fold | Y | N | |||
| Drozdov I | 2009 | 10.1002/cncr.24180 | [33] | Prospective | Prognostic | Classification | Primary small intestine; metastatic liver | Histology | Perceptron | Y | N | N | N | |||
| Fehrenbach U | 2021 | 10.3390/cancers13112726 | [44] | Prospective | Prognostic | Classification | Liver | Imaging (MRI) | Not specified | Y | 0.908–1.000 | N | Y | N | ||
| Gao X | 2019 | 10.1007/s11548-019-02070-5 | [49] | Prospective | Prognostic | Classification | Pancreas | Imaging (MRI) | CNN | Y | 0.915 * | 5-fold | Y | 0.893 * | N | |
| Govind D | 2020 | 10.1038/s41598-020-67880-z | [50] | Prospective | Prognostic | Classification | GI | Histology | deep-SKIE, SKIE (GAN-based), deep-SKIE (GAN-based) | Y | N | Y | N | |||
| Han X | 2021 | 10.3389/fonc.2021.606677 | [51] | Retrospective | Diagnostic | Classification | Pancreas | Imaging (CT) | AdaBoost, DT, GBDT, GNB, KNN, LDA, LR, SVM, RF | Y | 10-fold x1000 | Y | 0.946–0.997 * | N | ||
| Huang B | 2021 | 10.1109/JBHI.2020.3043236 | [52] | Retrospective | Prognostic | Classification | Pancreas | Imaging (MRI) | DFSR | N | N | Y | 0.919 | Y | 0.688–0.840 | |
| Huang B | 2021 | 10.1109/JBHI.2021.3070708 | [53] | Retrospective | Prognostic | Classification | Pancreas | Imaging (CT) | GBDT, LR, RF, SVM | Y | 0.660–0.760 | N | Y | 0.700–0.870 | Y | 0.710–0.830 |
| Ito H | 2020 | 10.4251/wjgo.v12.i11.1311 | [12] | Retrospective | Diagnostic | Classification | Colon & rectum | Serum | BT | Y | N | N | N | |||
| Kidd M | 2021 | 10.1159/000508573 | [13] | Retrospective | Prognostic | Classification | Multiple | Database | N | N | N | N | ||||
| Kidd M | 2021 | 10.1159/000508573 | [13] | Prospective | Prognostic | Classification | Multiple | Database | DT | N | N | Y | N | |||
| Kjellman | 2021 | 10.1159/000510483: 10.1159/000510483 | [14] | Prospective | Diagnostic | Classification | Small intestine | Serum | RF | Y | 0.970–0.990 | 5-fold | N | N | ||
| Klimov S | 2021 | 10.3389/fonc.2020.593211 | [15] | Retrospective | Diagnostic | Classification | Pancreas | Histology | CNN | Y | 5-fold | Y | N | |||
| Klimov S | 2021 | 10.3389/fonc.2020.593211 | [15] | Retrospective | Prognostic | Classification | Pancreas | Histology | CNN, ML “zoo” (18 different models) | Y | 5-fold, leave-one-out | N | N | |||
| Liu Y | 2014 | 10.1016/j.media.2014.02.005. | [16] | Prospective | Prognostic | Classification | Pancreas | Imaging (PET/CT) | RDM | N | N | N | N | |||
| Luo Y | 2019 | 10.1159/000503291 | [17] | Retrospective | Prognostic | Classification | Pancreas | Imaging (CT) | CNN, LR, RF, SVM | Y | 0.570–0.810 | 8-fold | Y | 0.820 | N | |
| Nanayakkara J | 2020 | 10.1093/narcan/zcaa009 | [18] | Retrospective | Diagnostic | Classification | Pancreas | miRNA | data mining | N | N | Y | N | |||
| Nguyen VX | 2010 | 10.7863/jum.2010.29.9.1345 | [19] | Retrospective | Diagnostic | Classification | Pancreas | Imaging (EUS) | ANN | Y | N | Y | 0.890 | N | ||
| Niazi MKK | 2018 | 10.1371/journal.pone.0195621 | [20] | Retrospective | Diagnostic | Classification | Pancreas | Histology | Inception v3-C1 (type of CNN), Bootstrapped Inception v3-C1 | N | N | Y | 0.922–0.973 | N | ||
| Panarelli N | 2019 | 10.1530/ERC-18-0244 | [21] | Retrospective | Diagnostic | Classification | Appendix, GEP, ileum, pancreas, rectum | miRNA | SVM | Y | 10-fold | Y | N | |||
| Redemann J | 2020 | 10.4103/jpi.jpi_37_20 | [23] | Retrospective | Diagnostic | Classification | Appendix, colon & rectum, duodenum, pancreas, small intestine, stomach, total (icl. lung) | Histology | CNN | Y | N | Y | N | |||
| Saccomandi P | 2016 | 10.1007/s10103-016-1948-1 | [24] | Retrospective | Prognostic | Regression | Pancreas | Histology | Inverse Monte Carlo | N | N | N | N | |||
| Saftoiu A | 2008 | 10.1016/j.gie.2008.04.031 | [25] | Prospective | Diagnostic | Classification | Pancreas | Imaging (EUS) | MLP | Y | 10-fold | Y | N | |||
| Soldevilla B | 2021 | 10.3390/cancers13112634 | [26] | Prospective | Diagnostic | Classification | Not specified | Plasma | OPLS-DA supervised model | Y | 0.779–0.982 | N | N | N | ||
| Song Y | 2018 | 10.7150/jca.26649 | [27] | Retrospective | Prognostic | Classification | Pancreas | Database | DL, LR, SVM, RF | Y | 10-fold | Y | 0.870 (DL) | N | ||
| Song C | 2021 | 10.21037/atm-21-25 | [28] | Retrospective | Prognostic | Classification | Pancreas | Imaging (CT) | SVM (various models) | Y | 0.580–0.830 | 10-fold | Y | 0.480–0.770 | Y | 0.520–0.560 |
| Telalovic JH | 2021 | 10.3390/diagnostics11050804 | [29] | Retrospective | Prognostic | Classification | GI; pancreas | Database | DT, GB GNB, KNN, MLP, MNB, LR, RF, SVC, XT | Y | 10-fold | Y | N | |||
| Tirosh A | 2019 | 10.1002/cncr.31930 | [30] | Prospective | Diagnostic | Classification | Pancreas | GWAS | Unsupervised clustering analysis | N | N | N | N | |||
| Udristoiu AL | 2021 | 10.1371/journal.pone.0251701 | [31] | Prospective | Diagnostic | Classification | Pancreas | Imaging (EUS) | CNN-LSTM (different models) | Y | N | Y | 0.970–0.990 | N | ||
| van Gerven MAJ | 2007 | 10.1016/j.artmed.2006.09.003 | [32] | Retrospective | Prognostic | Classification | Not specified | Database | NTC | Y | leave-one-out | N | N | |||
| Wan Y | 2021 | 10.1002/mp.15199 | [34] | Retrospective | Prognostic | Classification | Pancreas | Imaging (CT) | SAE, hybrid (SAE+handcrafted) | Y | 0.766–0.934 | 5-fold | Y | 0.739 | N | |
| Wang Q | 2020 | 10.1042/BSR20193860 | [35] | Prospective | Diagnostic | Classification | Small intestine | Gene expression assay | ANN | N | N | N | N | |||
| Wang Q | 2021 | 10.3389/fonc.2021.725988 | [36] | Retrospective | Diagnostic | Classification | Liver | Gene expression assay | SVM | N | N | Y | 0.945–1.000 | N | ||
| Wehrend J | 2021 | 10.1186/s13550-021-00839-x | [37] | Retrospective | Diagnostic | Classification | Liver | Imaging (PET/CT) | CNN | Y | 5-fold | Y | 0.700–0.730 ** | N | ||
| Xing F | 2013 | 10.1007/978-3-642-40811-3_55 | [38] | Prospective | Diagnostic | Classification | Pancreas | Histology | SVM | N | N | Y | N | |||
| Xing F | 2014 | 10.1109/TBME.2013.2291703 | [39] | Prospective | Diagnostic | Classification | GEP | Histology | SVM | N | 3-fold | N | N | |||
| Xing F | 2015 | 10.1007/978-3-319-24574-4_40 | [40] | Prospective | Diagnostic | Classification | Not specified | Histology | CNN | N | N | Y | N | |||
| Xing F | 2016 | 10.1007/978-3-319-46726-9_22 | [41] | Prospective | Diagnostic | Classification | Pancreas | Histology | CNN | Y | N | Y | N | |||
| Xing F | 2016 | 10.1109/TMI.2015.2481436 | [42] | Prospective | Diagnostic | Classification | Pancreas | Histology | CNN | Y | N | Y | N | |||
| Xing F | 2019 | 10.1109/TBME.2019.2900378 | [43] | Prospective | Diagnostic | Classification | Pancreas | Histology | FCN-8s, FCRNA, FCRNB, FRCN, KiNet, SFCNOPI, U-Net | Y | N | Y | 0.525–0.724 | N | ||
| Zhang X | 2020 | 10.1200/CCI.19.00108 | [45] | Retrospective | Diagnostic | Classification | Pancreas | Histology | GADA | Y | 0.627–0.857 | 2-fold | Y | 0.462–0.775 | N | |
| Zhang T | 2021 | 10.3389/fonc.2020.521831 | [46] | Retrospective | Prognostic | Classification | Pancreas | Imaging (CT) | DC + AdaBoost, DC + GBDT, XGB + RF | Y | N | Y | 0.570–0.860 | N | ||
| Zhou RQ | 2019 | 10.12998/wjcc.v7.i13.1611 | [47] | Retrospective | Prognostic | Classification | Pancreas | Histology | LDA, LR, MLP, SVM | N | leave-one-out | Y | N | |||
| Zimmerman NM | 2021 | 10.2217/fon-2020-1254 | [48] | Retrospective | Prognostic | Classification | Multiple | Database | DT | N | N | N | N | |||
| Outcome | Number of Studies (%) | Reference No. |
|---|---|---|
| Tumor type identification | 10 (18.9) | [12,18,19,21,23,25,31,36,37,51] |
| Tumor grade | 10 (18.9) | [10,11,17,34,46,47,49,50,52,53] |
| Tumor detection | 5 (9.4) | [14,20,26,33,43] |
| 5-year survival | 2 (3.8) | [22,27] |
| Cell segmentation | 2 (3.8) | [40,42] |
| Disease progression | 2 (3.8) | [13,29] |
| Disease recurrence | 2 (3.8) | [28,53] |
| Ki-67 scoring | 2 (3.8) | [38,39] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pantelis, A.G.; Panagopoulou, P.A.; Lapatsanis, D.P. Artificial Intelligence and Machine Learning in the Diagnosis and Management of Gastroenteropancreatic Neuroendocrine Neoplasms—A Scoping Review. Diagnostics 2022, 12, 874. https://doi.org/10.3390/diagnostics12040874
Pantelis AG, Panagopoulou PA, Lapatsanis DP. Artificial Intelligence and Machine Learning in the Diagnosis and Management of Gastroenteropancreatic Neuroendocrine Neoplasms—A Scoping Review. Diagnostics. 2022; 12(4):874. https://doi.org/10.3390/diagnostics12040874
Chicago/Turabian StylePantelis, Athanasios G., Panagiota A. Panagopoulou, and Dimitris P. Lapatsanis. 2022. "Artificial Intelligence and Machine Learning in the Diagnosis and Management of Gastroenteropancreatic Neuroendocrine Neoplasms—A Scoping Review" Diagnostics 12, no. 4: 874. https://doi.org/10.3390/diagnostics12040874