
The Utility of Conventional Amino Acid PET Radiotracers in the Evaluation of Glioma Recurrence also in Comparison with MRI

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
1.1. Posttreatment Evaluation
1.2. Magnetic Resonance Imaging (MRI)
- clinical deterioration (not attributable to other non-tumor causes and not due to steroid decrease);
- 25% or more increase in the sum of the products of perpendicular diameters between the first postradiotherapy scan and the scan at 12 weeks or later;
- increase (significant) in non-enhancing FLAIR/T2W lesions, not attributable to other non-tumor causes;
- any new contrast-enhancing lesion outside of the radiation field.
1.3. Amino Acid Tracer Positron Emission Tomography
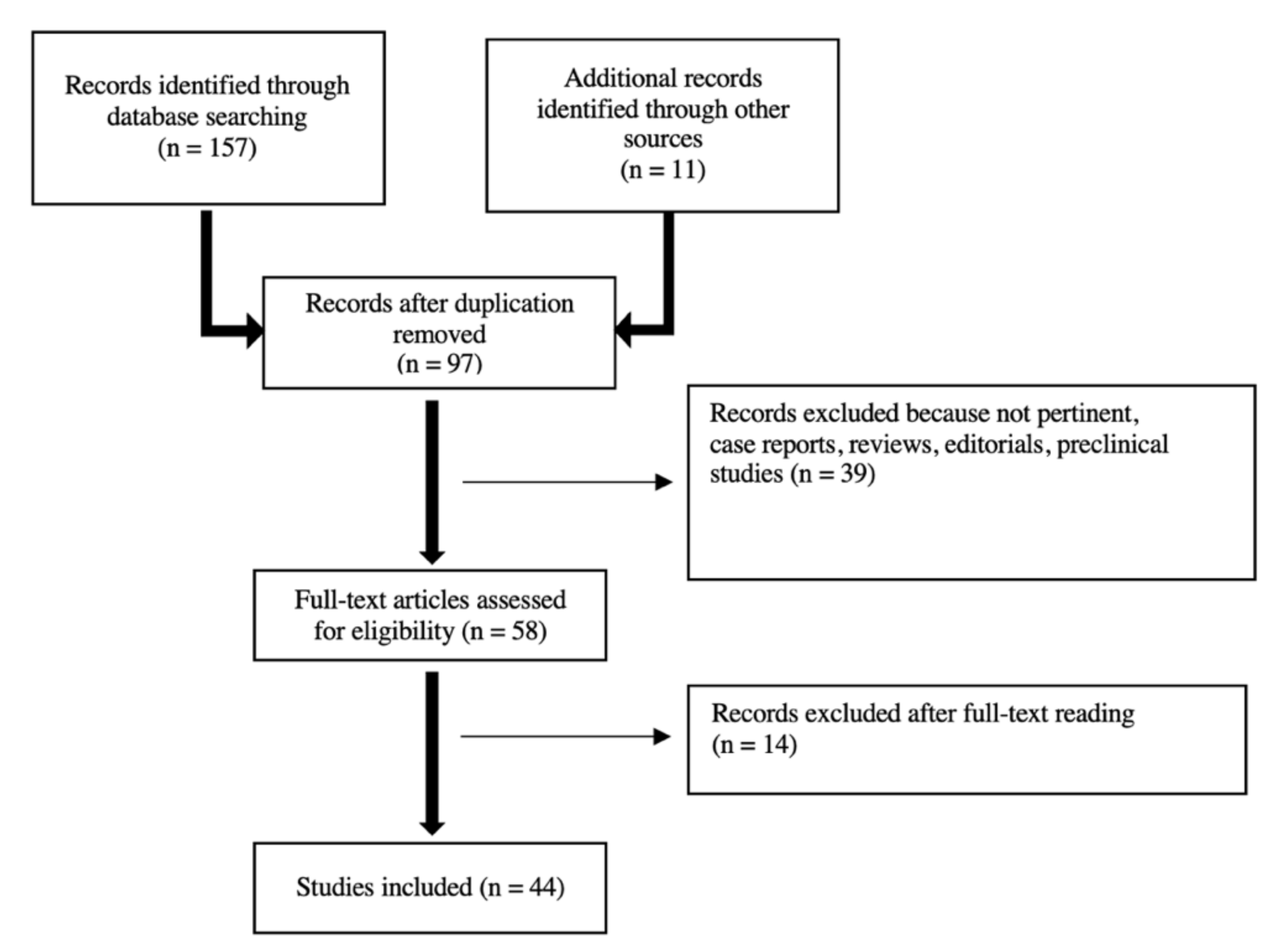
2. Search Strategy
3. FET
Comparison of FET PET with MRI
4. FDOPA
Comparison of FDOPA PET with MRI
5. MET
Comparison of MET PET with MRI
6. Other Amino Acid Transporters for Future Directions
7. Innovative Approaches
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ostrom, Q.T.; Patil, N.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. Corrigendum to: CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2013–2017. Neuro-Oncology 2020, 22, iv1–iv96. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO Classification of Tumours of the Central Nervous System. Acta Neuropathol. 2007, 114, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamborn, K.R.; Yung, W.K.A.; Chang, S.M.; Wen, P.Y.; Cloughesy, T.F.; DeAngelis, L.; Robins, H.I.; Lieberman, F.S.; Fine, H.A.; Fink, K.L.; et al. Progression-free survival: An important end point in evaluating therapy for recurrent high-grade gliomas. Neuro-Oncology 2008, 10, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Lacroix, M.; Toms, S.A. Maximum Safe Resection of Glioblastoma Multiforme. J. Clin. Oncol. 2014, 32, 727–728. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Mason, W.P.; Van Den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. New Engl. J. 2005, 352, 987–996. Available online: www.nejm.org (accessed on 7 February 2022). [CrossRef] [PubMed]
- Nabors, L.B.; Portnow, J.; Ahluwalia, M.; Baehring, J.; Brem, H.; Brem, S.; Butowski, N.; Campian, J.L.; Clark, S.W.; Fabiano, A.J.; et al. Central Nervous System Cancers, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 1537–1570. [Google Scholar] [CrossRef] [PubMed]
- Wick, W.; Gorlia, T.; Bendszus, M.; Taphoorn, M.; Sahm, F.; Harting, I.; Brandes, A.A.; Taal, W.; Domont, J.; Idbaih, A.; et al. Lomustine and Bevacizumab in Progressive Glioblastoma. New Engl. J. Med. 2017, 377, 1954–1963. [Google Scholar] [CrossRef] [PubMed]
- Leao, D.; Craig, P.; Godoy, L.; Da La Leite, C.; Policeni, B. Response Assessment in Neuro-Oncology Criteria for Gliomas: Practical Approach Using Conventional and Advanced Techniques. Am. J. Neuroradiol. 2019, 41, 10–20. [Google Scholar] [CrossRef]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; DeGroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated Response Assessment Criteria for High-Grade Gliomas: Response As-sessment in Neuro-Oncology Working Group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Larraya, J.G.; Lahutte, M.; Petrirena, G.; Reyes-Botero, G.; Gonzalez-Aguilar, A.; Houillier, C.; Guillevin, R.; Sanson, M.; Hoang-Xuan, K.; Delattre, J.Y. Response assessment in recurrent glioblastoma treated with irinotec-an-bevacizumab: Comparative analysis of the Macdonald, RECIST, RANO, and RECIST + F criteria. Neuro-Oncology 2012, 14, 667–673. [Google Scholar] [CrossRef]
- Galldiks, N.; Dunkl, V.; Stoffels, G.; Hutterer, M.; Rapp, M.; Sabel, M.; Reifenberger, G.; Kebir, S.; Dorn, F.; Blau, T.; et al. Diagnosis of pseudoprogression in patients with glioblastoma using O-(2-[18F]fluoroethyl)-l-tyrosine PET. Eur. J. Pediatr. 2014, 42, 685–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuplich, M.; Hadizadeh, D.R.; Kuchelmeister, K.; Scorzin, J.; Filss, C.; Langen, K.-J.; Schäfer, N.; Mack, F.; Schüller, H.; Simon, M.; et al. Late and Prolonged Pseudoprogression in Glioblastoma After Treatment With Lomustine and Temozolomide. J. Clin. Oncol. 2012, 30, e180–e183. [Google Scholar] [CrossRef] [PubMed]
- Brandsma, D.; Stalpers, L.; Taal, W.; Sminia, P.; van den Bent, M.J. Clinical features, mechanisms, and management of pseudoprogression in malignant gliomas. Lancet Oncol. 2008, 9, 453–461. [Google Scholar] [CrossRef]
- Reardon, D.A.; Wen, P.Y.; Desjardins, A.; Batchelor, T.T.; Vredenburgh, J.J. Glioblastoma multiforme: An emerging paradigm of anti-VEGF therapy. Expert Opin. Biol. Ther. 2008, 8, 541–553. [Google Scholar] [CrossRef] [PubMed]
- Law, I.; Albert, N.L.; Arbizu, J.; Boellaard, R.; Drzezga, A.; Galldiks, N.; La Fougère, C.; Langen, K.-J.; Lopci, E.; Lowe, V.; et al. Joint EANM/EANO/RANO practice guidelines/SNMMI procedure standards for imaging of gliomas using PET with radiolabelled amino acids and [18F]FDG: Version 1.0. Eur. J. Pediatr. 2018, 46, 540–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, P.Y.; Chang, S.M.; Van den Bent, M.J.; Vogelbaum, M.A.; Macdonald, D.R.; Lee, E.Q. Response Assessment in Neu-ro-Oncology Clinical Trials. J. Clin. Oncol. 2017, 35, 2439–2449. [Google Scholar] [CrossRef] [PubMed]
- Wan, B.; Wang, S.; Tu, M.; Wu, B.; Han, P.; Xu, H. The diagnostic performance of perfusion MRI for differentiating glioma recurrence from pseudoprogression: A meta-analysis. Medicine 2017, 96, e6333. [Google Scholar] [CrossRef]
- Seeger, A.; Braun, C.; Skardelly, M.; Paulsen, F.; Schittenhelm, J.; Ernemann, U.; Bisdas, S. Comparison of Three Different MR Perfusion Techniques and MR Spectroscopy for Multiparametric Assessment in Distinguishing Recurrent High-Grade Gliomas from Stable Disease. Acad. Radiol. 2013, 20, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Kazda, T.; Bulik, M.; Pospisil, P.; Lakomy, R.; Smrcka, M.; Slampa, P.; Jancalek, R. Advanced MRI increases the diagnostic accuracy of recurrent glioblastoma: Single institu-tion thresholds and validation of MR spectroscopy and diffusion weighted MR imaging. NeuroImage Clin. 2016, 11, 316. [Google Scholar] [CrossRef] [Green Version]
- Papin-Michault, C.; Bonnetaud, C.; Dufour, M.; Almairac, F.; Coutts, M.; Patouraux, S.; Virolle, T.; Darcourt, J.; Burel-Vandenbos, F. Study of LAT1 Expression in Brain Metastases: Towards a Better Under-standing of the Results of Positron Emission Tomography Using Amino Acid Tracers. PLoS ONE 2016, 11, e0157139. [Google Scholar] [CrossRef] [Green Version]
- Youland, R.S.; Kitange, G.J.; Peterson, T.E.; Pafundi, D.H.; Ramiscal, J.A.; Pokorny, J.L.; Giannini, C.; Laack, N.N.; Parney, I.; Lowe, V.J.; et al. The role of LAT1 in 18F-DOPA uptake in malignant gliomas. J. Neuro-Oncol. 2012, 111, 11–18. [Google Scholar] [CrossRef]
- Wiriyasermkul, P.; Nagamori, S.; Tominaga, H.; Oriuchi, N.; Kaira, K.; Nakao, H.; Kitashoji, T.; Ohgaki, R.; Tanaka, H.; Endou, H.; et al. Transport of 3-Fluoro-l-α-Methyl-Tyrosine by Tumor-Upregulated L-Type Amino Acid Transporter 1: A Cause of the Tumor Uptake in PET. J. Nucl. Med. 2012, 53, 1253–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fueger, B.J.; Czernin, J.; Cloughesy, T.; Silverman, D.H.; Geist, C.L.; Walter, M.A.; Schiepers, C.; Nghiemphu, P.; Lai, A.; Phelps, M.E.; et al. Correlation of 6-18F-Fluoro-l-Dopa PET Uptake with Proliferation and Tumor Grade in Newly Diagnosed and Recurrent Gliomas. J. Nucl. Med. 2010, 51, 1532–1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundaram, S.K.; Muzik, O.; Chugani, D.C.; Mu, F.; Mangner, T.J.; Chugani, H.T. Quantification of protein synthesis in the human brain using l-[1-11C]-leucine PET: Incorporation of factors for large neutral amino acids in plasma and for amino acids recycled from tissue. J. Nucl. Med. 2006, 47, 1787–1795. [Google Scholar]
- Smith, C.B.; Schmidt, K.C.; Qin, M.; Burlin, T.V.; Cook, M.P.; Kang, J.; Saunders, R.C.; Bacher, J.D.; Carson, R.E.; Channing, M.A.; et al. Measurement of Regional Rates of Cerebral Protein Synthesis with l-[1-11C]leucine and PET with Correction for Recycling of Tissue Amino Acids: II. Validation in Rhesus Monkeys. J. Cereb. Blood Flow Metab. 2005, 25, 629–640. [Google Scholar] [CrossRef] [Green Version]
- Wester, H.J.; Herz, M.; Weber, W.; Heiss, P.; Senekowitsch-Schmidtke, R.; Schwaiger, M.; Stöcklin, G. Synthesis and Radiopharmacology of O-(2-[18F]fluoroethyl)-l-Tyrosine for Tumor Im-aging. J. Nucl. Med. 1999, 40, 205–212. [Google Scholar]
- Grosu, A.-L.; Astner, S.T.; Riedel, E.; Nieder, C.; Wiedenmann, N.; Heinemann, F.; Schwaiger, M.; Molls, M.; Wester, H.-J.; Weber, W.A. An Interindividual Comparison of O-(2-[18F]Fluoroethyl)-l-Tyrosine (FET)– and l-[Methyl-11C]Methionine (MET)–PET in Patients With Brain Gliomas and Metastases. Int. J. Radiat. Oncol. 2011, 81, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Becherer, A.; Karanikas, G.; Szabó, M.; Zettinig, G.; Asenbaum, S.; Marosi, C.; Henk, C.; Wunderbaldinger, P.; Czech, T.; Wadsak, W.; et al. Brain tumour imaging with PET: A comparison between [18F]fluorodopa and [11C]methionine. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 1561–1567. [Google Scholar] [CrossRef] [PubMed]
- Laudicella, R.; Quartuccio, N.; Argiroffi, G.; Alongi, P.; Baratto, L.; Califaretti, E.; Frantellizzi, V.; De Vincentis, G.; Del Sole, A.; Evangelista, L.; et al. Unconventional non-amino acidic PET radiotracers for molecular imaging in gliomas. Eur. J. Pediatr. 2021, 48, 3925–3939. [Google Scholar] [CrossRef]
- Langen, K.-J.; Stoffels, G.; Filss, C.; Heinzel, A.; Stegmayr, C.; Lohmann, P.; Willuweit, A.; Neumaier, B.; Mottaghy, F.M.; Galldiks, N. Imaging of amino acid transport in brain tumours: Positron emission tomography with O-(2-[18F]fluoroethyl)- L -tyrosine (FET). Methods 2017, 130, 124–134. [Google Scholar] [CrossRef]
- Heiss, P.; Mayer, S.; Herz, M.; Wester, H.J.; Schwaiger, M.; Senekowitsch-Schmidtke, R. Investigation of transport mechanism and uptake kinetics of O-(2-[18F]fluoroethyl)-l-tyrosine in vitro and in vivo. J. Nucl. Med. 1999, 40, 1367–1373. [Google Scholar] [PubMed]
- Rachinger, W.; Goetz, C.; Pöpperl, G.; Gildehaus, F.J.; Kreth, F.W.; Holtmannspötter, M.; Herms, J.; Koch, W.; Tatsch, K.; Tonn, J.C. Positron Emission Tomography with O-(2-[18F]fluoroethyl)-l-tyrosine versus Mag-netic Resonance Imaging in the Diagnosis of Recurrent Gliomas. Neurosurgery 2005, 57, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Debus, C.; Afshar-Oromieh, A.; Floca, R.; Ingrisch, M.; Knoll, M.; Debus, J.; Haberkorn, U.; Abdollahi, A. Feasibility and robustness of dynamic 18F-FET PET based tracer kinetic models applied to patients with recurrent high-grade glioma prior to carbon ion irradiation. Sci. Rep. 2018, 8, 14760. [Google Scholar] [CrossRef] [PubMed]
- Galldiks, N.; Stoffels, G.; Filss, C.; Rapp, M.; Blau, T.; Tscherpel, C.; Ceccon, G.; Dunkl, V.; Weinzierl, M.R.; Stoffel, M.; et al. The use of dynamic O-(2-18F-fluoroethyl)-l-tyrosine PET in the diagnosis of patients with progressive and recurrent glioma. Neuro-Oncology 2015, 17, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- Pyka, T.; Hiob, D.; Preibisch, C.; Gempt, J.; Wiestler, B.; Schlegel, J.; Straube, C.; Zimmer, C. Diagnosis of glioma recurrence using multiparametric dynamic 18F-fluoroethyl-tyrosine PET-MRI. Eur. J. Radiol. 2018, 103, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Pöpperl, G.; Kreth, F.W.; Herms, J.; Koch, W.; Mehrkens, J.H.; Gildehaus, F.J.; Kretzschmar, H.A.; Tonn, J.C.; Tatsch, K. Analysis of 18F-FET PET for Grading of Recurrent Gliomas: Is Evaluation of Uptake Kinetics Superior to Standard Methods? J. Nucl. Med. 2006, 47, 393–403. [Google Scholar] [PubMed]
- Maurer, G.D.; Brucker, D.P.; Stoffels, G.; Filipski, K.; Filss, C.P.; Mottaghy, F.M.; Galldiks, N.; Steinbach, J.P.; Hattingen, E.; Langen, K.J. 18F-FET PET Imaging in Differentiating Glioma Progression from Treat-ment-Related Changes: A Single-Center Experience. J. Nucl. Med. 2020, 61, 505–511. [Google Scholar] [CrossRef]
- Bashir, A.; Mathilde Jacobsen, S.; Mølby Henriksen, O.; Broholm, H.; Urup, T.; Grunnet, K.; Andrée Larsen, V.; Møller, S.; Skjøth-Rasmussen, J.; Skovgaard Poulsen, H.; et al. Recurrent glioblastoma versus late posttreatment changes: Diag-nostic accuracy of O-(2-[18F]fluoroethyl)-l-tyrosine positron emission tomography (18F-FET PET). Neuro-Oncology 2019, 21, 1595–1606. [Google Scholar] [CrossRef] [PubMed]
- Pöpperl, G.; Götz, C.; Rachinger, W.; Gildehaus, F.J.; Tonn, J.C.; Tatsch, K. Value of O-(2-[18F]fluoroethyl)-l-tyrosine PET for the diagnosis of recurrent glioma. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 1464–1470. [Google Scholar] [CrossRef] [PubMed]
- Kebir, S.; Fimmers, R.; Galldiks, N.; Schäfer, N.; Mack, F.; Schaub, C.; Stuplich, M.; Niessen, M.; Tzaridis, T.; Simon, M.; et al. Personalized Medicine and Imaging Late Pseudoprogression in Glioblastoma: Diagnos-tic Value of Dynamic O-(2-[18F]fluoroethyl)-l-Tyrosine PET. Clin. Cancer Res. 2016, 22, 2190–2196. [Google Scholar] [CrossRef] [Green Version]
- Galldiks, N.; Rapp, M.; Stoffels, G.; Fink, G.R.; Shah, N.J.; Coenen, H.H.; Sabel, M.; Langen, K.J. Response assessment of bevacizumab in patients with recurrent malignant glioma us-ing [18F]Fluoroethyl-l-tyrosine PET in comparison to MRI. Eur. J. Nucl. Med. Mol. Imaging 2012, 40, 22–33. [Google Scholar] [CrossRef]
- George, E.; Kijewski, M.F.; Dubey, S.; Belanger, A.P.; Reardon, D.A.; Wen, P.Y.; Kesari, S.; Horky, L.; Park, M.A.; Huang, R.Y. Voxel-Wise Analysis of Fluoroethyltyrosine PET and MRI in the Assessment of Recur-rent Glioblastoma During Antiangiogenic Therapy. Am. J. Roentgenol. 2018, 211, 1342–1347. [Google Scholar] [CrossRef] [PubMed]
- Hutterer, M.; Nowosielski, M.; Putzer, D.; Waitz, D.; Tinkhauser, G.; Kostron, H.; Stockhammer, G. O-(2-18F-Fluoroethyl)-l-Tyrosine PET Predicts Failure of Antiangiogenic Treat-ment in Patients with Recurrent High-Grade Glioma. J. Nucl. Med. 2011, 52, 856–864. [Google Scholar] [CrossRef] [Green Version]
- Kertels, O.; Mihovilovic, M.I.; Linsenmann, T.; Kessler, A.F.; Tran-Gia, J.; Kircher, M.; Lapa, C. Clinical Utility of Different Approaches for Detection of Late Pseudopro-gression in Glioblastoma With O-(2-[18F]Fluoroethyl)-l-Tyrosine PET. Clin. Nucl. Med. 2019, 44, 695–701. [Google Scholar] [CrossRef] [Green Version]
- Unterrainer, M.; Vettermann, F.; Brendel, M.; Holzgreve, A.; Lifschitz, M.; Zähringer, M.; Albert, N.L. Towards standardization of 18F-FET PET imaging: Do we need a consistent method of background activity assessment? EJNMMI Res. 2017, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Baradaran, H.; Delgado, D.; Askin, G.; Christos, P.; John Tsiouris, A.; Gupta, A. MR perfusion-weighted imaging in the evaluation of high-grade gliomas after treat-ment: A systematic review and meta-analysis. Neuro-Oncology 2017, 19, 118–127. [Google Scholar] [CrossRef] [Green Version]
- Steidl, E.; Langen, K.-J.; Abu Hmeidan, S.; Polomac, N.; Filss, C.P.; Galldiks, N.; Lohmann, P.; Keil, F.; Filipski, K.; Mottaghy, F.M.; et al. Sequential implementation of DSC-MR perfusion and dynamic [18F]FET PET allows efficient differentiation of glioma progression from treatment-related changes. Eur. J. Pediatr. 2020, 48, 1956–1965. [Google Scholar] [CrossRef]
- Verger, A.; Filss, C.P.; Lohmann, P.; Stoffels, G.; Sabel, M.; Wittsack, H.-J.; Kops, E.R.; Galldiks, N.; Fink, G.R.; Shah, N.J.; et al. Comparison of O-(2-18F-Fluoroethyl)-l-Tyrosine Positron Emission Tomography and Perfusion-Weighted Magnetic Resonance Imaging in the Diagnosis of Patients with Progressive and Recurrent Glioma: A Hybrid Positron Emission Tomography/Magnetic Resonance Study. World Neurosurg. 2018, 113, e727–e737. [Google Scholar] [CrossRef] [PubMed]
- Göttler, J.; Lukas, M.; Kluge, A.; Kaczmarz, S.; Gempt, J.; Ringel, F.; Mustafa, M.; Meyer, B.; Zimmer, C.; Schwaiger, M.; et al. Intra-lesional spatial correlation of static and dynamic FET-PET parameters with MRI-based cerebral blood volume in patients with untreated glioma. Eur. J. Pediatr. 2016, 44, 392–397. [Google Scholar] [CrossRef]
- Lohmeier, J.; Bohner, G.; Siebert, E.; Brenner, W.; Hamm, B.; Makowski, M.R. Quantitative biparametric analysis of hybrid 18F-FET PET/MR-neuroimaging for dif-ferentiation between treatment response and recurrent glioma. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sogani, S.K.; Jena, A.; Taneja, S.; Gambhir, A.; Mishra, A.K.; D’Souza, M.M.; Jadhav, G.K. Potential for differentiation of glioma recurrence from radionecrosis using integrated 18F-fluoroethyl-l-tyrosine (FET) positron emission tomography/magnetic resonance imaging: A prospective evaluation. Neurol. India 2017, 65, 293. [Google Scholar]
- Jena, A.; Taneja, S.; Gambhir, A.; Mishra, A.K.; D’souza, M.M.; Verma, S.M.; Sogani, S.K. Glioma recurrence versus radiation necrosis single-session multiparametric approach using simultaneous O-(2-18F-fluoroethyl)-l-tyrosine PET/MRI. Clin. Nucl. Med. 2016, 41, e228–e236. [Google Scholar] [CrossRef] [PubMed]
- Carideo, L.; Minniti, G.; Mamede, M.; Scaringi, C.; Russo, I.; Scopinaro, F.; Cicone, F. 18F-DOPA uptake parameters in glioma: Effects of patients’ characteristics and prior treatment history. Br. J. Radiol. 2018, 91, 20170847. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.-H.; Ahn, B.-C. Current Radiopharmaceuticals for Positron Emission Tomography of Brain Tumors. Brain Tumor Res. Treat. 2018, 6, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, K.; Czernin, J.; Cloughesy, T.; Lai, A.; Pomykala, K.L.; Benz, M.R.; Buck, A.K.; Phelps, M.E.; Chen, W. Comparison of visual and semiquantitative analysis of 18F-FDOPA-PET/CT for recurrence detection in glioblastoma patients. Neuro-Oncology 2013, 16, 603–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, K.; Jutabha, P.; Endou, H.; Sagara, H.; Anzai, N. LAT1 Is a Critical Transporter of Essential Amino Acids for Immune Reactions in Ac-tivated Human T Cells. J. Immunol. 2013, 191, 4080–4085. [Google Scholar] [CrossRef] [PubMed]
- Zaragori, T.; Ginet, M.; Marie, P.-Y.; Roch, V.; Grignon, R.; Gauchotte, G.; Rech, F.; Blonski, M.; Lamiral, Z.; Taillandier, L.; et al. Use of static and dynamic [18F]-F-DOPA PET parameters for detecting patients with glioma recurrence or progression. EJNMMI Res. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Karunanithi, S.; Sharma, P.; Kumar, A.; Khangembam, B.C.; Bandopadhyaya, G.P.; Kumar, R.; Bal, C. 18F-FDOPA PET/CT for detection of recurrence in patients with glioma: Prospec-tive comparison with 18F-FDG PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1025–1035. [Google Scholar] [CrossRef]
- Karunanithi, S.; Sharma, P.; Kumar, A.; Khangembam, B.C.; Bandopadhyaya, G.P.; Kumar, R.; Goenka, A.; Gupta, D.K.; Malhotra, A.; Bal, C. Comparative diagnostic accuracy of contrast-enhanced MRI and 18F-FDOPA PET-CT in recurrent glioma. Eur. Radiol. 2013, 23, 2628–2635. [Google Scholar] [CrossRef]
- Youland, R.S.; Pafundi, D.H.; Brinkmann, D.H.; Lowe, V.J.; Morris, J.M.; Kemp, B.J.; Hunt, C.H.; Giannini, C.; Parney, I.F.; Laack, N.N. Prospective trial evaluating the sensitivity and specificity of 3,4-dihydroxy-6-[18F]-fluoro-l-phenylalanine (18F-DOPA) PET and MRI in patients with recurrent gliomas. J. Neuro-Oncol. 2018, 137, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Cicone, F.; Filss, C.; Minniti, G.; Espagnet, M.C.R.; Papa, A.; Scaringi, C.; Galldiks, N.; Bozzao, A.; Shah, N.J.; Scopinaro, F.; et al. Volumetric assessment of recurrent or progressive gliomas: Comparison between F-DOPA PET and perfusion-weighted MRI. Eur. J. Pediatr. 2015, 42, 905–915. [Google Scholar] [CrossRef] [PubMed]
- Ledezma, C.J.; Chen, W.; Sai, V.; Freitas, B.; Cloughesy, T.; Czernin, J.; Pope, W. 18F-FDOPA PET/MRI fusion in patients with primary/recurrent gliomas: Initial experi-ence. Eur. J. Radiol. 2009, 71, 242–248. [Google Scholar] [CrossRef]
- Bund, C.; Heimburger, C.; Imperiale, A.; Lhermitte, B.; Chenard, M.P.; Lefebvre, F.; Namer, I.J. FDOPA PET-CT of Nonenhancing Brain Tumors. Clin. Nucl. Med. 2017, 42, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Karavaeva, E.; Harris, R.J.; Leu, K.; Shabihkhani, M.; Yong, W.H.; Pope, W.; Lai, A.; Nghiemphu, P.L.; Liau, L.; Chen, W.; et al. Relationship Between [18F]FDOPA PET Uptake, Apparent Diffusion Coefficient (ADC), and Proliferation Rate in Recurrent Malignant Gliomas. Mol. Imaging Biol. 2014, 17, 434–442. [Google Scholar] [CrossRef] [Green Version]
- Jung, T.-Y.; Min, J.-J.; Bom, H.-S.; Jung, S.; Kim, I.-Y.; Lim, S.-H.; Kim, D.-Y.; Kwon, S.Y. Prognostic value of post-treatment metabolic tumor volume from 11C-methionine PET/CT in recurrent malignant glioma. Neurosurg. Rev. 2016, 40, 223–229. [Google Scholar] [CrossRef]
- Hatakeyama, T.; Kawai, N.; Nishiyama, Y.; Yamamoto, Y.; Sasakawa, Y.; Ichikawa, T.; Tamiya, T. 11C-methionine (MET) and 18F-fluorothymidine (FLT) PET in patients with newly diagnosed glioma. Eur. J. Pediatr. 2008, 35, 2009–2017. [Google Scholar] [CrossRef] [PubMed]
- He, Q.; Zhang, L.; Zhang, B.; Shi, X.; Yi, C.; Zhang, X. Diagnostic accuracy of 13N-ammonia PET, 11C-methionine PET and 18F-fluorodeoxyglucose PET: A comparative study in patients with suspected cerebral glioma. BMC Cancer 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Tsuyuguchi, N.; Takami, T.; Sunada, I.; Iwai, Y.; Yamanaka, K.; Tanaka, K.; Nishikawa, M.; Ohata, K.; Torii, K.; Morino, M.; et al. Methionine Positron Emission Tomography for Differentiation of Recurrent Brain Tumor and Radiation Necrosis after Stereotactic Radiosurgery-In Malignant Gliomam. Ann. Nucl. Med. 2004, 18, 291–296. [Google Scholar] [CrossRef]
- D’Souza, M.M.; Sharma, R.; Jaimini, A.; Panwar, P.; Saw, S.; Kaur, P.; Mondal, A.; Mishra, A.; Tripathi, R.P. 11C-MET PET/CT and Advanced MRI in the Evaluation of Tumor Recurrence in High-Grade Gliomas. Clin. Nucl. Med. 2014, 39, 791–798. [Google Scholar] [CrossRef]
- Minamimoto, R.; Saginoya, T.; Kondo, C.; Tomura, N.; Ito, K.; Matsuo, Y.; Matsunaga, S.; Shuto, T.; Akabane, A.; Miyata, Y.; et al. Differentiation of Brain Tumor Recurrence from Post-Radiotherapy Necrosis with 11C-Methionine PET: Visual Assessment versus Quantitative Assessment. PLoS ONE 2015, 10, e0132515. [Google Scholar] [CrossRef] [PubMed]
- Kits, A.; Martin, H.; Sânchez-Crespo, A.; Delgado, A.F. Diagnostic accuracy of 11C-methionine PET in detecting neuropathologically confirmed recurrent brain tumor after radiation therapy. Ann. Nucl. Med. 2017, 32, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Deuschl, C.; Kirchner, J.; Poeppel, T.D.; Schaarschmidt, B.; Kebir, S.; El Hindy, N.; Hense, J.; Quick, H.H.; Glas, M.; Herrmann, K.; et al. 11C–MET PET/MRI for detection of recurrent glioma. Eur. J. Nucl. Med. Mol. Imaging 2017, 45, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Terakawa, Y.; Tsuyuguchi, N.; Iwai, Y.; Yamanaka, K.; Higashiyama, S.; Takami, T.; Ohata, K. Diagnostic Accuracy of 11C-Methionine PET for Differentiation of Recurrent Brain Tumors from Radiation Necrosis After Radiotherapy. J. Nucl. Med. 2008, 49, 694–699. [Google Scholar] [CrossRef] [Green Version]
- Shishido, H.; Kawai, N.; Miyake, K.; Yamamoto, Y.; Nishiyama, Y.; Tamiya, T. Diagnostic Value of 11C-Methionine (MET) and 18F-Fluorothymidine (FLT) Positron Emission Tomography in Recurrent High-Grade Gliomas; Differentiation from Treatment-Induced Tissue Necrosis. Cancers 2012, 4, 244–256. [Google Scholar] [CrossRef]
- Tripathi, M.; Sharma, R.; Varshney, R.; Jaimini, A.; Jain, J.; Souza, M.M.; Bal, J.; Pandey, S.; Kumar, N.; Mishra, A.K.; et al. Comparison of F-18 FDG and C-11 methionine PET/CT for the evaluation of re-current primary brain tumors. Clin. Nucl. Med. 2012, 37, 158–163. [Google Scholar] [CrossRef]
- Dandois, V.; Rommel, D.; Renard, L.; Jamart, J.; Cosnard, G. Substitution of 11C-methionine PET by perfusion MRI during the follow-up of treat-ed high-grade gliomas: Preliminary results in clinical practice. J. Neuroradiol. 2010, 37, 89–97. [Google Scholar] [CrossRef]
- Qiao, Z.; Zhao, X.; Wang, K.; Zhang, Y.; Fan, D.; Yu, T.; Shen, H.; Chen, Q.; Ai, L. Utility of Dynamic Susceptibility Contrast Perfusion-Weighted MR Imaging and 11C-Methionine PET/CT for Differentiation of Tumor Recurrence from Radiation Injury in Patients with High-Grade Glio-mas. Am. J. Neuroradiol. 2019, 40, 253–259. [Google Scholar] [CrossRef] [Green Version]
- McConathy, J.; Yu, W.; Jarkas, N.; Seo, W.; Schuster, D.M.; Goodman, M.M. Radiohalogenated nonnatural amino acids as PET and SPECT tumor imaging agents. Med. Res. Rev. 2011, 32, 868–905. [Google Scholar] [CrossRef]
- Sai, K.K.S.; Huang, C.; Yuan, L.; Zhou, D.; Piwnica-Worms, D.; Garbow, J.R.; Engelbach, J.A.; Mach, R.H.; Rich, K.M.; McConathy, J. 18F-AFETP, 18F-FET, and 18F-FDG Imaging of Mouse DBT Gliomas. J. Nucl. Med. 2013, 54, 1120. [Google Scholar]
- Fuchs, B.C.; Bode, B.P. Amino acid transporters ASCT2 and LAT1 in cancer: Partners in crime? Semin. Cancer Biol. 2005, 15, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Uchino, H.; Kanai, Y.; Kim, D.K.; Wempe, M.F.; Chairoungdua, A.; Morimoto, E.; Anders, M.W.; Endou, H. Transport of Amino Acid-Related Compounds Mediated by L-Type Amino Acid Trans-porter 1 (LAT1): Insights Into the Mechanisms of Substrate Recognition. Mol. Pharmacol. 2002, 61, 729–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, W.; McConathy, J.; Olson, J.J.; Goodman, M.M. System a amino acid transport-targeted brain and systemic tumor PET imaging agents 2-amino-3-[18F]fluoro-2-methylpropanoic acid and 3-[18F]fluoro-2-methyl-2-(methylamino)propanoic acid. Nucl. Med. Biol. 2014, 42, 8–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McConathy, J.; Martarello, L.; Malveaux, E.J.; Camp, V.M.; Simpson, N.E.; Simpson, C.P.; Bowers, G.D.; Olson, J.J.; Goodman, M.M. Radiolabeled Amino Acids for Tumor Imaging with PET: Radiosynthesis and Biological Evaluation of 2-Amino-3-[18F]fluoro-2-methylpropanoic Acid and 3-[18F]Fluoro-2-methyl-2-(methylamino)propanoic Acid. J. Med. Chem. 2002, 45, 2240–2249. [Google Scholar] [CrossRef]
- McConathy, J.; Martarello, L.; Malveaux, E.J.; Camp, V.M.; Simpson, N.E.; Simpson, C.P.; Bowers, G.D.; Zhang, Z.; Olson, J.J.; Goodman, M.M. Synthesis and evaluation of 2-amino-4-[18F]fluoro-2-methylbutanoic acid (FAMB): Relationship of amino acid transport to tumor imaging properties of branched fluorinated amino acids. Nucl. Med. Biol. 2003, 30, 477–490. [Google Scholar] [CrossRef]
- Yu, W.; McConathy, J.; Williams, L.; Camp, V.M.; Malveaux, E.J.; Zhang, Z.; Olson, J.J.; Goodman, M.M. Synthesis, Radiolabeling, and Biological Evaluation of (R)- and (S)-2-Amino-3-[18F]Fluoro-2-Methylpropanoic Acid (FAMP) and (R)- and (S)-3-[18F]Fluoro-2-Methyl-2-N-(Methylamino)propanoic Acid (NMeFAMP) as Potential PET Radioligands for Imaging Brain Tumors. J. Med. Chem. 2009, 53, 876–886. [Google Scholar] [CrossRef] [Green Version]
- Bouhlel, A.; Zhou, D.; Li, A.; Yuan, L.; Rich, K.M.; McConathy, J. Synthesis, Radiolabeling, and Biological Evaluation of (R)- and (S)-2-Amino-5-[18F]fluoro-2-methylpentanoic Acid ((R)-, (S)-[18F]FAMPe) as Potential Positron Emission Tomography Tracers for Brain Tumors. J. Med. Chem. 2015, 58, 3817–3829. [Google Scholar] [CrossRef] [Green Version]
- Yu, W.; McConathy, J.; Olson, J.; Camp, V.M.; Goodman, M.M. Facile Stereospecific Synthesis and Biological Evaluation of (S)- and (R)-2-Amino-2-methyl-4-[123I]iodo-3-(E)-butenoic Acid for Brain Tumor Imaging with Single Photon Emission Computerized Tomography. J. Med. Chem. 2007, 50, 6718–6721. [Google Scholar] [CrossRef] [PubMed]
- McConathy, J.; Zhou, D.; Shockley, S.E.; Jones, L.A.; Griffin, E.A.; Lee, H.; Adams, S.J.; Mach, R.H. Click synthesis and biologic evaluation of (R)-and (S)-2-Amino-3-[1-(2-[18F]Fluoroethyl)-1H-[1,2,3]Triazol-4-yl]propanoic acid for brain tumor imaging with positron emission tomography. Mol. Imaging 2010, 9, 329–342. [Google Scholar] [CrossRef]
- Floeth, F.W.; Pauleit, D.; Wittsack, H.J.; Langen, K.J.; Reifenberger, G.; Hamacher, K.; Messing-Jünger, M.; Zilles, K.; Weber, F.; Stummer, W.; et al. Multimodal metabolic imaging of cerebral gliomas: Positron emission tomography with [18F]fluoroethyl-l-tyrosine and magnetic resonance spectroscopy. J. Neurosurg. 2005, 102, 318–321. [Google Scholar] [CrossRef] [Green Version]
- Lau, E.W.; Drummond, K.J.; Ware, R.E.; Drummond, E.; Hogg, A.; Ryan, G.; Grigg, A.; Callahan, J.; Hicks, R.J. Comparative PET study using F-18 FET and F-18 FDG for the evaluation of pa-tients with suspected brain tumour. J. Clin. Neurosci. 2010, 17, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Laudicella, R.; Iagaru, A.; Minutoli, F.; Gaeta, M.; Baldari, S.; Bisdas, S. PET/MR in neuro-oncology: Is it ready for prime-time? Clin. Transl. Imaging 2020, 8, 233–235. [Google Scholar] [CrossRef]
- Tixier, F.; Le Rest, C.C.; Hatt, M.; Albarghach, N.; Pradier, O.; Metges, J.P.; Corcos, L.; Visvikis, D. Intratumor heterogeneity characterized by textural features on baseline 18F-FDG PET im-ages predicts response to concomitant radiochemotherapy in esophageal cancer. J. Nucl. Med. 2011, 52, 369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kebir, S.; Khurshid, Z.; Gaertner, F.C.; Essler, M.; Hattingen, E.; Fimmers, R.; Scheffler, B.; Herrlinger, U.; Bundschuh, R.A.; Glas, M. Unsupervised consensus cluster analysis of [18F]-fluoroethyl-l-tyrosine positron emission tomography identified textural features for the diagnosis of pseudoprogression in high-grade glioma. Oncotarget 2016, 8, 8294–8304. [Google Scholar] [CrossRef] [Green Version]
- Kebir, S.; Schmidt, T.; Weber, M.; Lazaridis, L.; Galldiks, N.; Langen, K.-J.; Kleinschnitz, C.; Hattingen, E.; Herrlinger, U.; Lohmann, P.; et al. A Preliminary Study on Machine Learning-Based Evaluation of Static and Dynamic FET-PET for the Detection of Pseudoprogression in Patients with IDH-Wildtype Glioblastoma. Cancers 2020, 12, 3080. [Google Scholar] [CrossRef] [PubMed]
- Lohmann, P.; Elahmadawy, M.A.; Gutsche, R.; Werner, J.M.; Bauer, E.K.; Ceccon, G.; Kocher, M.; Lerche, C.W.; Rapp, M.; Fink, G.R.; et al. FET PET Radiomics for Differentiating Pseudoprogression from Early Tu-mor Progression in Glioma Patients Post-Chemoradiation. Cancers 2020, 12, 3835. [Google Scholar] [CrossRef] [PubMed]
- Paprottka, K.J.; Kleiner, S.; Preibisch, C.; Kofler, F.; Schmidt-Graf, F.; Delbridge, C.; Bernhardt, D.; Combs, S.E.; Gempt, J.; Meyer, B.; et al. Fully automated analysis combining [18F]-FET-PET and multiparametric MRI in-cluding DSC perfusion and APTw imaging: A promising tool for objective evaluation of glioma progression. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4445–4455. [Google Scholar] [CrossRef]
- Hotta, M.; Minamimoto, R.; Miwa, K. 11C-methionine-PET for differentiating recurrent brain tumor from radiation necrosis: Radiomics approach with random forest classifier. Sci. Rep. 2019, 9, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Qiao, Z.; Zhao, X.; Li, X.; Wang, X.; Wu, T.; Chen, Z.; Fan, D.; Chen, Q.; Ai, L. Individualized discrimination of tumor recurrence from radiation necrosis in glioma patients using an integrated radiomics-based model. Eur. J. Pediatr. 2019, 47, 1400–1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Authors [Ref.] | Year | Number of Patients | Glioma Grade (n) | PET Parameter | MRI/Other Imaging Modality Parameter | Main Findings |
|---|---|---|---|---|---|---|
| Galldiks et al. [35] | 2015 | 124 | 55 grade II 19 grade III 50 grade IV | TBRmax TBRmean TTP | CeMRI | Compared with the diagnostic accuracy of conventional MRI (85%) to diagnose tumor progression or recurrence, a higher accuracy (93%) was achieved by [18F]FET PET when a TBRmean ≥ 2.0 or TTP < 45 min was present (sensitivity, 93%; specificity, 100%; accuracy, 93%; positive predictive value, 100%; p < 0.001). |
| Pyka et al. [36] | 2018 | 47 | 3 grade II 16 grade III 27 grade IV | TBR TTP | rCBV ADC | Sensitivities and specificities for static PET were 80 and 85%, 66% and 77% for PWI, 62 and 77% for DWI, and 64 and 79% for PET TTP, respectively. Multiparametric analysis resulted in an AUC of 0.89, notably yielding a sensitivity of 76% vs. 56% for PET alone at 100% specificity. |
| Popperl et al. [37] | 2006 | 45 | 26 grade II 7 grade III 12 grade IV | SUVmax TBRmax TTP | ND | TAC slightly and steadily increased in tumor-free patients and in LGG, whereas HGG showed an early peak around 10–15 min after injection followed by a decrease. |
| Maurer et al. [38] | 2020 | 127 | 21 grade II 36 grade III 68 grade IV 2 ND | TBRmax TBRmean TTP slope | ND | The highest accuracy for differentiating progression from TRCs was achieved by a combination of TBRmax and slope (sensitivity, 86%; specificity, 67%; accuracy, 81%). The accuracy of [18F]FET PET was higher in IDH-wildtype gliomas than in IDH-mutant ones (p < 0.001) |
| Bashir et al. [39] | 2019 | 146 | 146 grade IV | TBRmax TBRmean BTV | ND | TBRmax is a powerful imaging biomarker to detect recurrent GBM (sensitivity 99%, specificity 94%; p < 0.0001). BTV is independently and inversely correlated with OS. |
| Pöpperl et al. [40] | 2004 | 53 | 27 grade IV 16 grade III 9 grade II 1 grade I | SUVmax TBRmax | ND | Best differentiation between benign posttherapeutic effects and tumor recurrence was observed at a threshold value of 2.0 for the TBR, with a discriminatory power of 100%. For the absolute values of SUVmax, the best differentiation was seen at a threshold value of 2.2. |
| Kebir et al. [41] | 2016 | 26 | 26 grade IV | TBRmax TBRmean TTP | ND | TBRmax and TBRmeanwere significantly higher in patients with true progression than in patients with late PSP, whereas TTP was significantly shorter. ROC analysis yielded an optimal cutoff value of 1.9 for TBRmax to differentiate between true progression and late PSP (sensitivity 84%, specificity 86%, accuracy 85%, p < 0.015). |
| Galldiks et al. [42] | 2012 | 10 | 1 grade III 9 grade IV | TBRmax TBRmean TTP | ND | A reduction in TBRmean of ≥17% at follow-up differentiated responders (PFS ≥ 6 months) from non-responders (PFS < 6 months) with excellent sensitivity (83%) and specificity (100%). Moreover, TTP and kinetic patterns at baseline and follow-up differentiated responders from non-responders with a favourable diagnostic performance. |
| George et al. [43] | 2018 | 13 | 13 grade IV | Dynamic acquisition | CeMRI | An only moderate correlation between FET PET uptake and CeMRI. FET PET may have a prognostic role in the follow-up of patients with recurrent GBM undergoing antiangiogenic therapy. |
| Hutterer et al. [44] | 2011 | 11 | 11 grade IV | SUVmax TBRmax | ND | In HGG patients undergoing antiangiogenic treatment, [18F]FET PET seems to be predictive for treatment failure. |
| Kertels et al. [45] | 2019 | 36 | 36 grade IV | TBR * | ND | [18F]FET PET is a reliable tool for the detection of late PSP in GBM, irrespective of the analytical approach. |
| Steidl et al. [48] | 2020 | 104 | 9 grade II 24 grade III 70 grade IV 1 other | TBRmax slope | rCBVmax | The sensitivity of the rCBVmax was low (0.53), while the sensitivity of the combined TBRmaxand slope values was substantially higher (0.96). In the subgroup of IDH-mutant tumors, PWI appeared to be more reliable than [18F]FET PET. |
| Verger et al. [49] | 2018 | 31 | 2 grade II 3 grade III 27 grade IV | TBRmax TBRmean TTP slope | rCBF rCBV | TBRmaxwas the only parameter that showed a significant diagnostic power to discriminate between TRC and progressive/recurrent gliomas. The best cutoff value for TBRmaxwas 2.61, with a sensitivity of 80%, a specificity of 86%, a PPV of 95%, an NPV of 55%, and an accuracy of 81%. [18F]FET PET is superior to PWI for diagnosing progressive or recurrent gliomas. |
| GoÖttler et al. [50] | 2016 | 30 | 3 grade II 4 grade III 23 grade IV | TBRmean TTP slope | rCBV | Static and dynamic FET uptake measures and rCBV are interdependent and exhibit only a poor spatial overlap: the mean distance between the tumor hotspots of FET uptake and rCBV was 20.0 +/− 14.1 mm. |
| Lohmeier et al. [51] | 2019 | 42 | 40 HGG 2 LGG | SUVmax SUVmean TBRmax TBRmean | rADCmean | The ADCmean in the metabolically most active regions was higher in patients with recurrent glioma than in patients with TRC. The highest accuracy (90%) was achieved when both DWI and [18F]FET PET-derived parameters were combined in a biparametric approach. |
| Sogani et al. [52] | 2017 | 32 | N.S. | TBRmax TBRmean | N rCBV ADCmean Cho/Cr | The diagnostic accuracy, sensitivity, and specificity for recurrence detection using all three MRI parameters were 93.75%, 96%, and 85.7%, respectively. The addition of FET PET TBR values improved these values further to 96.87%, 100%, and 85.7%, respectively. |
| Jena et al. [53] | 2016 | 26 | N.S. | TBRmax TBRmean | N rCBV ADCmean Cho/Cr | The diagnostic accuracy of [18F]FET PET/MRI TBR values for the correct identification of recurrence of brain gliomas reached 93.8% using TBRmax of 2.11 or greater and 87.5% using TBRmean of 1.437 or greater. The highest accuracy (96.9%) was obtained when both the TBRmax was greater than 2.11 (or TBRmean > 1.44) and the Cho/Cr ratio > 1.42. |
| Authors [Ref] | Year | Number of Patients | Glioma Grade (n) | PET Parameter | MRI/Other Imaging Modality Parameter | Main Findings |
|---|---|---|---|---|---|---|
| Herrmann et al. [56] | 2014 | 110 | 33 grade III 77 grade IV | Visual analysis SUVmax SUVmean TNRmax TSRmax | ND | FDOPA PET showed a diagnostic accuracy of 82% (sensitivity, 89.6%; specificity, 72.4%) in distinguishing recurrence from TRC. Moreover, FDOPA PET is highly prognostic of PFS. |
| Zaragoni et al. [58] | 2020 | 51 | 18 grade II 8 grade III 25 grade IV | TNRmax TSRmax MTV TTP | ND | All studied PET parameters, except TTP, were significant univariate predictors of glioma recurrence/progression (p < 0.001), with a global diagnostic accuracy of 96% being reached with TNRmax, TSRmax, and MTV. All PET parameters, except TTP, were also significant predictors of PFS, although none were predictive of OS |
| Karunanithi et al. [59] | 2013 | 28 | 2 grade I 8 grade II 5 grade III 13 grade IV | SUVmax TNRmax TSRmax TWRmax TCRmax | ND | The sensitivity, specificity and accuracy of [18F]FDG PET were 47.6%, 100%, and 60.7%, respectively, and those of [18F]FDOPA PET/CT were 100%, 85.7%, and 96.4%, respectively. The difference in the findings between [18F]FDG PET/CT and [18F]FDOPA PET/CT was significant (p = 0.0005). The difference was significant for LGGs but not for HGGs. |
| Karunanithi et al. [60] | 2013 | 35 | 2 grade I 9 grade II 8 grade III 16 grade IV | SUVmax TNRmax TSRmax TWRmax TCRmax | CeMRI | Comparison between CeMRI and [18F]FDOPA PET for detecting recurrent glioma showed a diagnostic accuracy of 80% vs. 97.1%, overall sensitivity 92.3% vs. 100%, and specificity 44.4% vs. 88.8%, respectively. |
| Youland et al. [61] | 2018 | 13 | 2 grade II 4 grade III 7 grade IV | SUVmax SUVmean TNRmax | CeMRI | Regions of high PET avidity with an SUVmax > 1.36 or TNRmax > 2.0 had better sensitivity and specificity for tumor than CeMRI. |
| Cicone et al. [62] | 2015 | 44 | 3 unverified 11 grade II 17 grade III 19 grade IV | Visual analysis TBRmean | rCBV | The regions with increased FDOPA uptake were much larger than those with increased rCBV values. In addition, TBRmean is significantly higher for FDOPA uptake than for rCBV maps, indicating that PET is superior to PWI for differentiating between tumor and normal brain tissue. |
| Ledezma et al. [63] | 2009 | 91 | 33 grade II 24 grade III 34 grade IV | Visual analysis | CeMRI | FDOPA detected most gliomas with sensitivity 95.2% (vs. MRI 90.5%), irrespective of tumor grade, labelling both enhancing and non-enhancing tumors equally well. FDOPA may be better at differentiating a non-enhancing tumor from other causes of MRI-T2w signal change such as gliosis and oedema. |
| Bund et al. [64] | 2017 | 53 | 35 LGG 18 HGG | SUVmax TNRmax | Cho/Cr Cho/NAA | Significant correlation between FDOPA SUVmaxand the MRS ratios was shown, which correspond to the proliferative and infiltrative characteristics of the tumor, respectively. A threshold of 2.16 in TNR at 30 min is useful to discriminate LGGs and HGGs. |
| Karavaeva et al. [65] | 2015 | 29 | 9 grade III 20 grade IV | SUVmean | ADC | Areas of high [18F]FDOPA uptake exhibited low ADC, and areas of hyperintensity T2/FLAIR with low [18F]FDOPA uptake exhibited high ADC. Median [18F]FDOPA uptake was positively correlated, and median ADC was inversely correlated with mitotic index from resected tumor tissue. |
| Authors [Ref] | Year | Number of Patients | Glioma Grade (n) | PET Parameter | MRI/Other Imaging Modality Parameter | Main Findings |
|---|---|---|---|---|---|---|
| Grosu et al. [28] | 2011 | 29/42 | 1 grade I 2 grade II 11 grade III 14 grade IV | SUVmean TBRmean | ND | FET PET and MET PET provide comparable diagnostic information with a sensitivity of 91% and specificity of 100% for both radiotracers. |
| Jung et al. [66] | 2016 | 42 | 12 grade III 30 grade IV | TBRmax TBRmean MTV | ND | TBR and MTV had a diagnostic value to differentiate recurrence from posttreatment effect. Unlike TBR, MTV was shown to be an independent factor in patients with recurrence. |
| Tsuyuguchi et al. [69] | 2004 | 11 | 3 grade III 8 grade IV | Visual analysis, SUVmean TBRmean | ND | MET PET reached a sensitivity, specificity, and accuracy in detecting tumor recurrence of 100%, 60%, and 82%, respectively. |
| D’Souza et al. [70] | 2014 | 29 | 16 grade III 12 grade IV | SUVmax SUVmean | rCBV Cho/Cr Cho/NAA | The sensitivity, specificity, and accuracy of MET PET in identifying tumor recurrence/residual were 94.7%, 80%, and 89.6%, respectively, whereas those of MRI were 84.2%, 90%, and 86.2%, respectively. |
| Minamimoto et al. [71] | 2015 | 31/70 | 12 grade III 19 grade IV | Visual analysis, SUVmax SUVmean TBRmax TBRmean | ND | The TBRmax and TBRmean was significantly higher for tumor recurrence than for radiation-induced necrosis (p < 0.02). The visual assessment showed no significant difference from the quantitative assessment of MET PET with a relevant cutoff value for the differentiation of recurrent brain tumors from radiation-induced necrosis. |
| Kits et al. [72] | 2018 | 23/30 | 5 grade II 8 grade III 10 grade IV | TBRmeancortex TBRmeanmirror TBRmaxcortex TBRmaxmirror | ND | Clinically relevant cutoffs were TBRmaxmirror ≥ 1.99 giving a specificity of 100% for tumor recurrence with a sensitivity of 76% and TBRmaxcortex ≥ 1.58 giving a sensitivity and specificity of 90 and 78%, respectively. |
| Deuschl et al. [73] | 2017 | 50 | 14 grade II 16 grade III 20 grade IV | SUVmax SUVmean TBRmax TBRmean | CeMRI | Diagnostic accuracy was 82% for MRI, 88% for [11C]MET PET, and 96% for hybrid [11C]MET PET/MRI. |
| Terakawa et al. [74] | 2008 | 26/77 | 6 grade II 6 grade III 14 grade IV | SUVmax SUVmean TBRmax TBRmean | ND | TBRmean value seems to provide the best sensitivity and specificity in differentiating glioma recurrence from RN. |
| Shishido et al. [75] | 2012 | 21 | 8 grade III 13 grade IV | SUVmax SUVmean TBRmax TBRmean | ND | The average TBR of recurrent gliomas was significantly higher than that of necrotic lesions on MET PET (p < 0.01). |
| Tripathi et al. [76] | 2012 | 37 | 2 grade I 13 grade II 8 grade III 12 grade IV | SUVmax TBRmax | ND | Using a cutoff for TBRmax > 1.9 to differentiate recurrence from no recurrence, the sensitivity of MET was 94.7%, whereas specificity was 88.89%. |
| Dandois et al. [77] | 2010 | 28 | 14 grade III 14 grade IV | ND | rCBV | rCBV reached equal performances in differentiating tumor recurrence and RN than MET PET. Cutoff value of rCBV for differentiating tumor from necrosis was 182% (sensitivity, 81.5%; specificity, 100%). |
| Qiao et al. [78] | 2019 | 33 | 10 grade III 23 grade IV | SUVmax SUVmean TBRmax TBRmean | rCBVmean | Combining the assessment of TBRmax and TBRmean and relative rCBVmean, the highest sensitivity (0.848) and specificity (1.0) was shown. |
| Authors [Ref.] | Patients | WHO Grade | RF | Classification Model | Accuracy |
|---|---|---|---|---|---|
| Kebir et al. [94] | 14 | III/IV | [18F]FET | Unsupervised consensus clustering | 75% |
| Kebir et al. [95] | 44 | IV | [18F]FET | linear discriminant analysis | AUC 93% |
| Lohmann et al. [96] | 34 | IV | [18F]FET | random forest | 70% |
| Paprottka et al. [97] | 66 | I-IV | [18F]FET | random forest | 86% |
| Hotta et al. [98] | 41 | ND | [11C]MET | random forest | 92.2% |
| Wang et al. [99] | 160 | II/III/IV | [11C]MET | random forest | AUC 93.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santo, G.; Laudicella, R.; Linguanti, F.; Nappi, A.G.; Abenavoli, E.; Vergura, V.; Rubini, G.; Sciagrà, R.; Arnone, G.; Schillaci, O.; et al. The Utility of Conventional Amino Acid PET Radiotracers in the Evaluation of Glioma Recurrence also in Comparison with MRI. Diagnostics 2022, 12, 844. https://doi.org/10.3390/diagnostics12040844
Santo G, Laudicella R, Linguanti F, Nappi AG, Abenavoli E, Vergura V, Rubini G, Sciagrà R, Arnone G, Schillaci O, et al. The Utility of Conventional Amino Acid PET Radiotracers in the Evaluation of Glioma Recurrence also in Comparison with MRI. Diagnostics. 2022; 12(4):844. https://doi.org/10.3390/diagnostics12040844
Chicago/Turabian StyleSanto, Giulia, Riccardo Laudicella, Flavia Linguanti, Anna Giulia Nappi, Elisabetta Abenavoli, Vittoria Vergura, Giuseppe Rubini, Roberto Sciagrà, Gaspare Arnone, Orazio Schillaci, and et al. 2022. "The Utility of Conventional Amino Acid PET Radiotracers in the Evaluation of Glioma Recurrence also in Comparison with MRI" Diagnostics 12, no. 4: 844. https://doi.org/10.3390/diagnostics12040844