
A New CT Analysis of Abdominal Wall after DIEP Flap Harvesting

 , , ,
, , ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
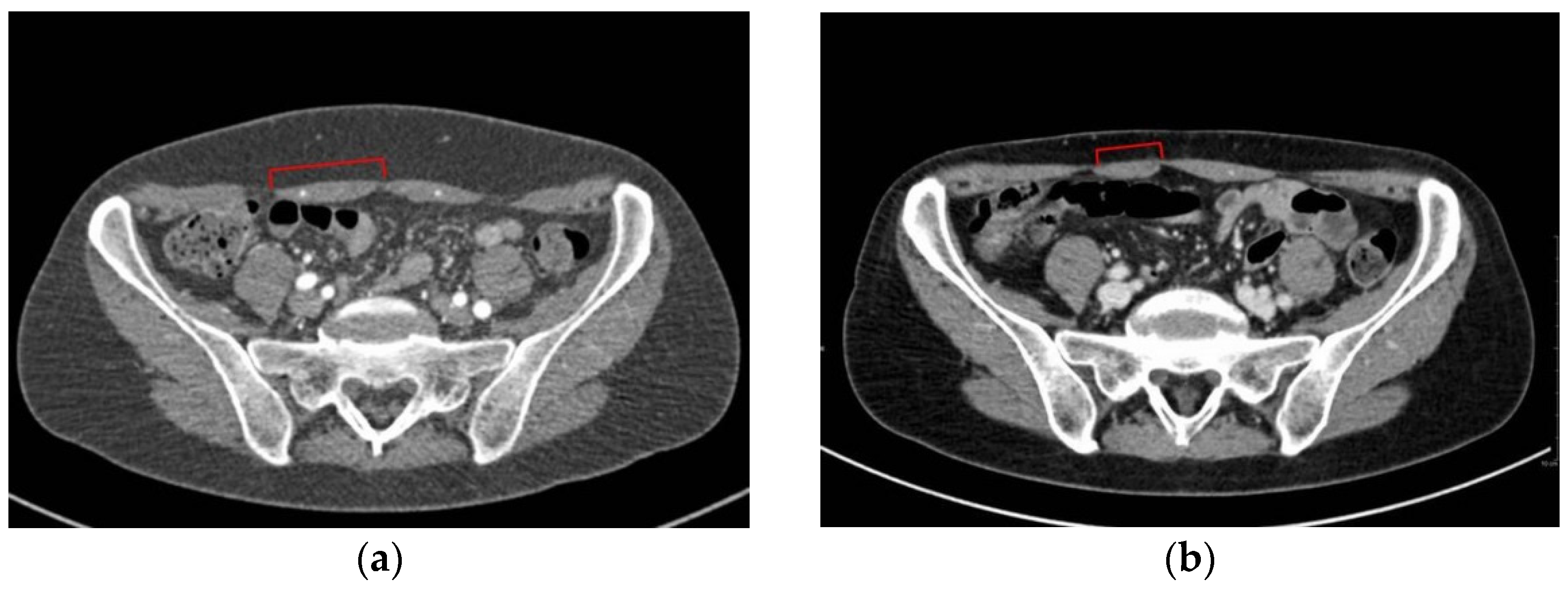
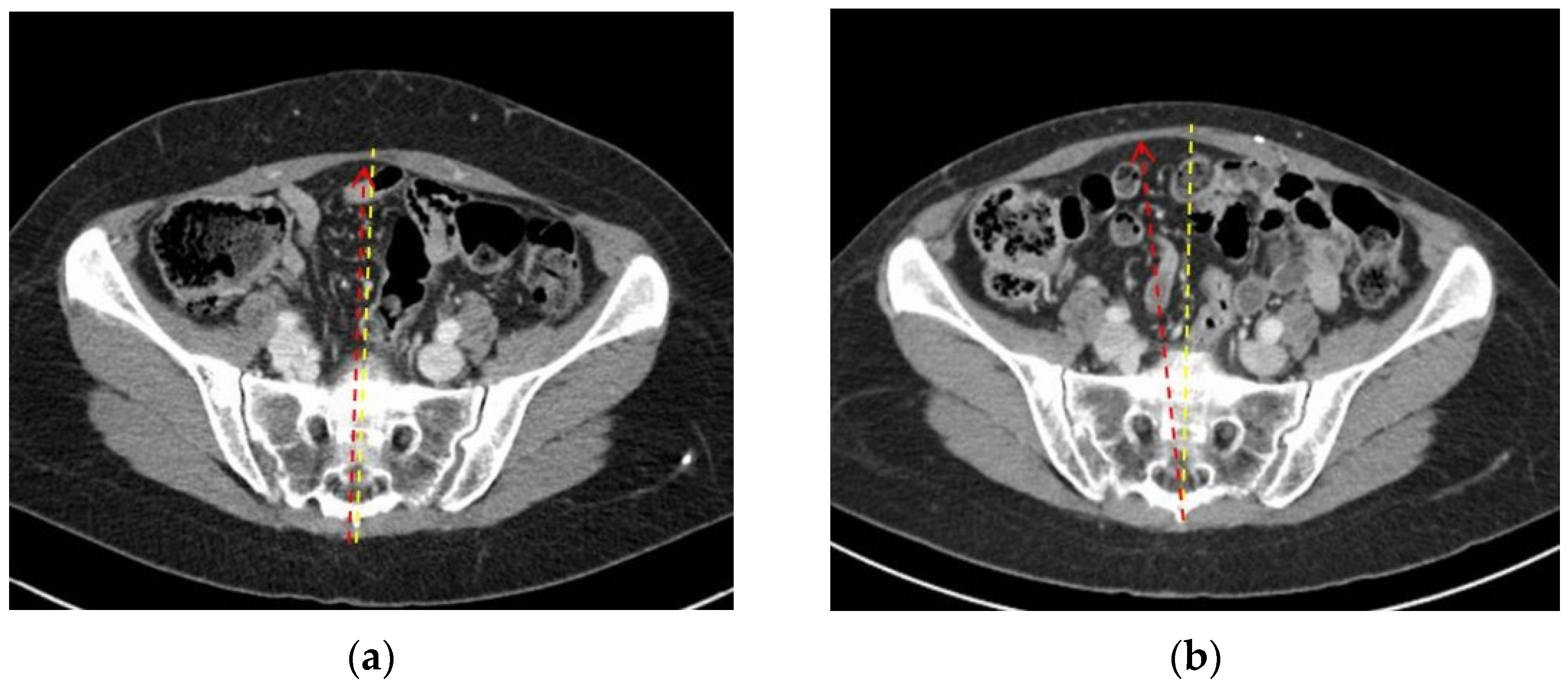
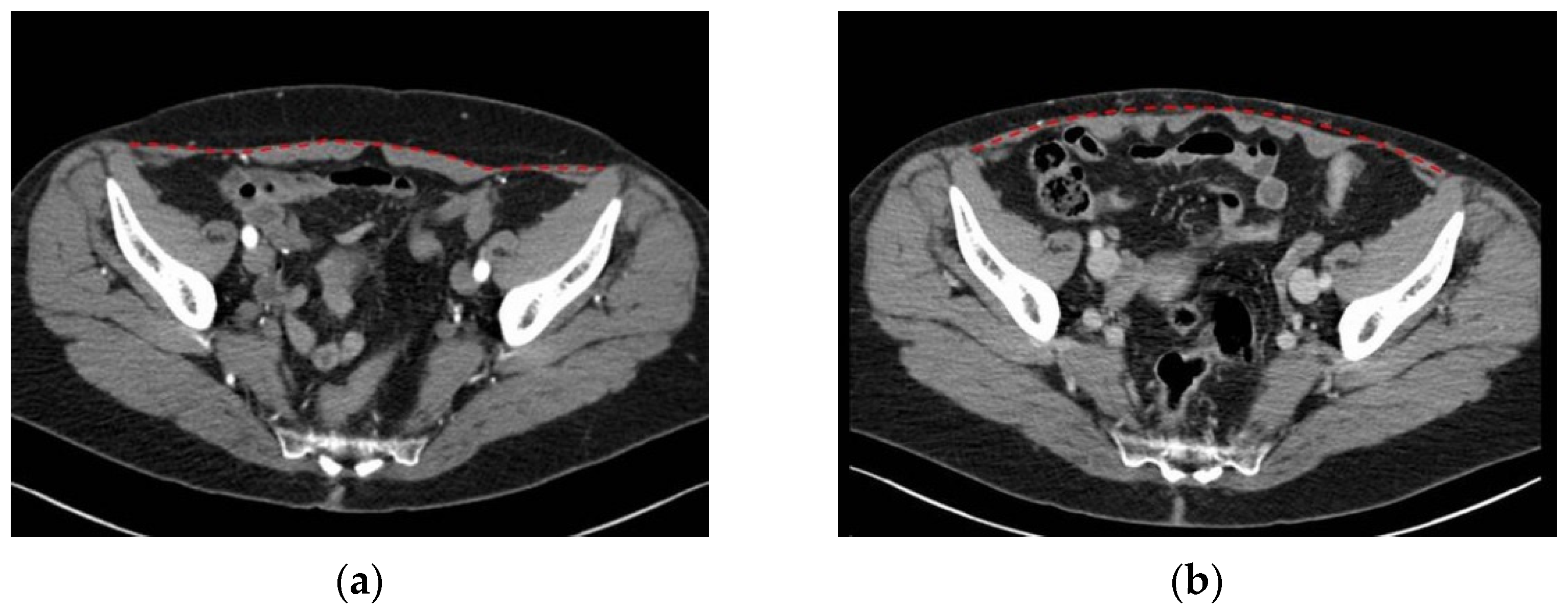
3.1. Two-Dimensional Evaluation
3.2. Muscle Quality Assessment
3.3. Physiatrist Investigation
3.3.1. Physical Examination
3.3.2. Pain and Impairment Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Craigie, J.E.; Allen, R.J.; Dellacroce, F.J.; Sullivan, S.K. Autogenous breast reconstruction with the deep inferior epigastric perforator flap. Clin. Plast. Surg. 2003, 30, 359–369. [Google Scholar] [CrossRef]
- Tan, M.G.; Isaranuwatchai, W.; DeLyzer, T.; Butler, K.; Hofer, S.O.P.; O’Neill, A.C.; Zhong, T. A cost-effectiveness analysis of DIEP vs free MS-TRAM flap for microsurgical breast reconstruction. J. Surg. Oncol. 2019, 119, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Jeong, W.; Lee, S.; Kim, J. Meta-analysis of flap perfusion and donor site complications for breast reconstruction using pedicled versus free TRAM and DIEP flaps. Breast 2018, 38, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Knox, A.D.C.; Ho, A.L.; Leung, L.; Tashakkor, A.Y.; Lennox, P.A.; Van Laeken, N.; Macadam, S.A. Comparison of Outcomes following Autologous Breast Reconstruction Using the DIEP and Pedicled TRAM Flaps: A 12-Year Clinical Retrospective Study and Literature Review. Plast. Reconstr. Surg. 2016, 138, 16–28. [Google Scholar] [CrossRef]
- Mathes, S.J.; Nahai, F. Classification of the vascular anatomy of muscles: Experimental and clinical correlation. Plast. Reconstr. Surg. 1981, 67, 177–187. [Google Scholar] [CrossRef]
- Boyd, J.B.; Taylor, G.I.; Corlett, R. The Vascular Territories of the Superior Epigastric and the Deep Inferior Epigastric Systems. Plast. Reconstr. Surg. 1984, 73, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Lhuaire, M.; Hivelin, M.; Dramé, M.; Abrahams, P.; Kianmanesh, R.; Fontaine, C.; Lantieri, L. Determining the best recipient vessel site for autologous microsurgical breast reconstruction with DIEP flaps: An anatomical study. J. Plast. Reconstr. Aesthetic Surg. 2017, 70, 781–791. [Google Scholar] [CrossRef]
- Yang, L.; Long, J.; Li, Z.; Zhou, X.; Peng, X.; Song, D.; Zhou, B.; Lv, C.; Wu, P. The lateral thoracic vessels: A novel recipient site for breast reconstruction with DIEP flap. J. Plast. Reconstr. Aesthetic Surg. 2019, 72, 1530–1536. [Google Scholar] [CrossRef]
- Roos, S.; Fyhr, I.-M.; Sunnerhagen, K.S.; Moslemi, A.-R.; Oldfors, A.; Ullman, M. Histopathological changes in skeletal muscle associated with chronic ischaemia. Apmis 2016, 124, 935–941. [Google Scholar] [CrossRef]
- Chalothorn, D.; Moore, S.M.; Zhang, H.; Sunnarborg, S.W.; Lee, D.C.; Faber, J.E. Heparin-Binding Epidermal Growth Factor–Like Growth Factor, Collateral Vessel Development, and Angiogenesis in Skeletal Muscle Ischemia. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1884–1890. [Google Scholar] [CrossRef] [Green Version]
- Grinsell, D.; Azizeddin, A.; Overland, J. Intramuscular pathway and fascicular characteristics of the segmental intercostal innervation to rectus abdominis. ANZ J. Surg. 2020, 90, 1052–1056. [Google Scholar] [CrossRef] [PubMed]
- Stecco, C.; Azzena, G.P.; Macchi, V.; Porzionato, A.; Behr, A.; Rambaldo, A.; Tiengo, C.; De Caro, R. Rectus abdominis muscle innervation: An anatomical study with surgical implications in diep flap harvesting. Surg. Radiol. Anat. 2018, 40, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Rozen, W.M.; Ashton, M.W.; Murray, A.C.A.; Taylor, G.I. Avoiding Denervation of Rectus Abdominis in DIEP Flap Harvest: The Importance of Medial Row Perforators. Plast. Reconstr. Surg. 2008, 122, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.I.; Chang, E.I.; Soto-Miranda, M.A.; Zhang, H.; Nosrati, N.; Robb, G.L.; Chang, D.W. Comprehensive Analysis of Donor-Site Morbidity in Abdominally Based Free Flap Breast Reconstruction. Plast. Reconstr. Surg. 2013, 132, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Lindenblatt, N.; Gruenherz, L.; Farhadi, J. A systematic review of donor site aesthetic and complications after deep inferior epigastric perforator flap breast reconstruction. Gland Surg. 2019, 8, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-T.; Park, J.-W.; Mun, G.-H. Impact of Rectus Muscle Injury during Perforator Dissection on Functional Donor Morbidity after Deep Inferior Epigastric Perforator Flap Breast Reconstruction. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2484. [Google Scholar] [CrossRef] [PubMed]
- Uda, H.; Tomioka, Y.K.; Sarukawa, S.; Sunaga, A.; Sugawara, Y. Comparison of abdominal wall morbidity between medial and lateral row-based deep inferior epigastric perforator flap. J. Plast. Reconstr. Aesthetic Surg. 2015, 68, 1550–1555. [Google Scholar] [CrossRef]
- Seal, S.K.F.; Hewitt, M.K.; Martin, M.L.; Brasher, P.M.A.; Macadam, S.A. Preoperative and Postoperative Assessment of Rectus Abdominis Muscle Size and Function following DIEP Flap Surgery. Plast. Reconstr. Surg. 2018, 141, 1261–1270. [Google Scholar] [CrossRef]
- Broyles, J.M.; Schuenke, M.D.; Patel, S.R.; Vail, C.M.; Broyles, H.V.; Dellon, A.L. Defining the Anatomy of the Tendinous Intersections of the Rectus Abdominis Muscle and Their Clinical Implications in Functional Muscle Neurotization. Ann. Plast. Surg. 2018, 80, 50–53. [Google Scholar] [CrossRef]
- Edmunds, K.J.; Gíslason, M.K.; Arnadottir, I.D.; Marcante, A.; Piccione, F.; Gargiulo, P. Quantitative Computed Tomography and Image Analysis for Advanced Muscle Assessment. Eur. J. Transl. Myol. 2016, 26, 6015. [Google Scholar] [CrossRef]
- Mah, P.; Reeves, T.E.; McDavid, W.D. Deriving Hounsfield units using grey levels in cone beam computed tomography. Dentomaxillofac. Radiol. 2010, 39, 323–335. [Google Scholar] [CrossRef] [PubMed]
- Corvino, A.; De Rosa, D.; Sbordone, C.; Nunziata, A.; Corvino, F.; Varelli, C.; Catalano, O. Diastasis of rectus abdominis muscles: Patterns of anatomical variation as demonstrated by ultrasound. Pol. J. Radiol. 2019, 84, e542–e548. [Google Scholar] [CrossRef] [PubMed]
- Perret, C.; Poiraudeau, S.; Fermanian, J.; Colau, M.M.L.; Benhamou, M.A.M.; Revel, M. Validity, reliability, and responsiveness of the fingertip-to-floor test. Arch. Phys. Med. Rehabil. 2001, 82, 1566–1570. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.S.; Shoaf, L.D.; Riddle, D.L. The Relationship of Lumbar Flexion to Disability in Patients with Low Back Pain. Phys. Ther. 2000, 80, 240–250. [Google Scholar] [CrossRef] [Green Version]
- Schober, P. The lumbar vertebral column in backache. Munch. Med. Wochenschr. 1937, 84, 336–338. [Google Scholar]
- Tousignant, M.; Poulin, L.; Marchand, S.; Viau, A.; Place, C. The Modified—Modified Schober Test for range of motion assessment of lumbar flexion in patients with low back pain: A study of criterion validity, intra- and inter-rater reliability and minimum metrically detectable change. Disabil. Rehabil. 2005, 27, 553–559. [Google Scholar] [CrossRef]
- Parfrey, K.C.; Docherty, D.; Workman, R.C.; Behm, D.G. The effects of different sit- and curl-up positions on activation of abdominal and hip flexor musculature. Appl. Physiol. Nutr. Metab. 2008, 33, 888–895. [Google Scholar] [CrossRef]
- Fairbank, J.C.T.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 25, 2940–2953, discussion 2952. [Google Scholar] [CrossRef]
- Monticone, M.; Baiardi, P.; Ferrari, S.; Foti, C.; Mugnai, R.; Pillastrini, P.; Vanti, C.; Zanoli, G. Development of the Italian Version of the Oswestry Disability Index (ODI-I): A cross-cultural adaptation, reliability, and validity study. Spine 2009, 34, 2090–2095. [Google Scholar] [CrossRef]
- Stevens, M.L.; Lin, C.C.-W.; Maher, C. The Roland Morris Disability Questionnaire. J. Physiother. 2016, 62, 116. [Google Scholar] [CrossRef] [Green Version]
- Padua, R.; Padua, L.; Ceccarelli, E.; Romanini, E.; Zanoli, G.; Bondì, R.; Campi, A. Italian version of the Roland Disability Questionnaire, specific for low back pain: Cross-cultural adaptation and validation. Eur. Spine J. 2002, 11, 126–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, A.; Nicklas, B. Age-related changes in fat deposition in mid-thigh muscle in women: Relationships with metabolic cardiovascular disease risk factors. Int. J. Obes. 1999, 23, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inacio, M.; Ryan, A.S.; Bair, W.-N.; Prettyman, M.; Beamer, B.A.; Rogers, M.W. Gluteal muscle composition differentiates fallers from non-fallers in community dwelling older adults. BMC Geriatr. 2014, 14, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joueidi, Y.; Vieillefosse, S.; Cardaillac, C.; Mortier, A.; Oppenheimer, A.; Deffieux, X.; Thubert, T. Impact of the diastasis of the rectus abdominis muscles on the pelvic-perineal symptoms: Review of the literature. Prog. Urol. 2019, 29, 544–559. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pt | Age | BMI * | Birth ** | Comorbidity | Affected Breast | Donor Site *** | Perforator Vessels Side/Number/Row |
|---|---|---|---|---|---|---|---|
| 1 | 54 | 34.4 | 2 | hypertension, smoker | Left | Ipsilateral | Left/2/medial |
| 2 | 50 | 30.9 | 2 | sarcoidosis | Left | Ipsilateral | Left/2/medial |
| 3 | 62 | 31.2 | 2 | hyperthyroidism, depression | Left | Contralateral | Right/2/medial |
| 4 | 61 | 34.4 | 3 | diabetes, hypertension, hyperaldosteronism, dyslipidaemia | Right | Ipsilateral | Right/2/medial |
| 5 | 45 | 35.8 | 1 | none | Right | Ipsilateral | Right/1/medial |
| 6 | 39 | 26.3 | 3 | hypothyroidism | Right | Ipsilateral | Right/2/medial |
| 7 | 52 | 29.7 | 2 | hypercholesterolaemia | Right | Ipsilateral | Right/2/lateral |
| 8 | 60 | 28.5 | 3 | none | Bilateral | Bilateral | Right/2/medial Left/1/medial |
| 9 | 56 | 30.4 | none | none | Bilateral | Bilateral | Right/1/medial Left/2/medial |
| 10 | 56 | 24.9 | none | hypothyroidism | Right | Contralateral | Left/2/medial |
| 11 | 60 | 18.2 | none | hypertension, hypercholesterolaemia | Left | Contralateral | Right/2/medial |
| 12 | 52 | 29.5 | 2 | none | Left | Contralateral | Right/2/medial |
| Pt | Side * | Level ** | Right Pre-Op | Right Post-Op | Right Δ *** | Left Pre-Op | Left Post-Op | Left Δ *** | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Width | Thickness | Width | Thickness | Width | Thickness | Width | Thickness | Width | Thickness | Width | Thickness | |||
| 1 | Left Ipsi | above | 82 | 7 | 84 | 8 | 2 | 1 | 87 | 7 | 91 | 8 | 3 | 1 |
| below | 63 | 7 | 75 | 7 | 12 | 0 | 81 | 8 | 82 | 6 | 1 | −2 | ||
| 2 | Left Ipsi | above | 97 | 11 | 81 | 10 | −16 | −1 | 109 | 8 | 82 | 10 | −27 | 2 |
| below | 84 | 12 | 70 | 12 | −14 | 0 | 102 | 9 | 100 | 12 | −2 | 3 | ||
| 3 | Left Contra | above | 78 | 10 | 72 | 10 | −6 | 0 | 78 | 9 | 75 | 10 | −3 | 1 |
| below | 69 | 13 | 65 | 6 | −4 | −7 | 59 | 13 | 65 | 21 | 6 | 8 | ||
| 4 | Right Ipsi | above | 83 | 10 | 82 | 9 | −1 | −1 | 82 | 8 | 92 | 9 | 10 | 1 |
| below | 69 | 14 | 41 | 14 | −28 | 0 | 67 | 15 | 63 | 17 | −4 | 2 | ||
| 5 | Right Ipsi | above | 74 | 11 | 73 | 13 | −1 | 2 | 72 | 11 | 75 | 11 | 3 | 0 |
| below | 72 | 15 | 63 | 16 | −9 | 1 | 61 | 14 | 65 | 14 | 4 | 0 | ||
| 6 | Right Ipsi | above | 64 | 11 | 71 | 7 | 7 | −4 | 64 | 9 | 69 | 7 | 5 | −2 |
| below | 50 | 11 m/10 l | 62 | 7 m/11 l | −12 | −4 m/−1 l | 48 | 10 m/9 l | 66 | 16 m/16 l | 18 | 6 m/7 l | ||
| 7 | Right Ipsi | above | 85 | 8 | 88 | 11 | 3 | 3 | 75 | 10 | 83 | 11 | 8 | 1 |
| below | 78 | 11 | 63 | 15 | −15 | 4 | 77 | 10 | 81 | 11 | 4 | 1 | ||
| 8 | Bilateral | above | 69 | 10 | 70 | 9 | 1 | −1 | 64 | 8 | 75 | 9 | 9 | 1 |
| below | 58 | 10 m/9 l | 68 | 10 m/12 l | 10 | 0 m/−3 l | 58 | 11 m/10 l | 69 | 11 m/14 l | 11 | 0 m/4 l | ||
| 9 | Bilateral | above | 58 | 11 | 62 | 8 | 4 | −3 | 57 | 9 | 56 | 7 | −1 | −2 |
| below | 57 | 9 | 54 | 10 | −3 | 1 | 55 | 11 | 33 | 9 | −2 | −2 | ||
| 10 | Right Contra | above | 64 | 10 | 66 | 10 | 2 | 0 | 60 | 10 | 68 | 11 | 8 | 1 |
| below | 45 | 4 | 47 | 6 | 2 | 2 | 48 | 14 | 51 | 15 | 3 | 1 | ||
| 11 | Left Contra | above | 45 | 9 | 38 | 10 | −7 | 1 | 41 | 10 | 36 | 11 | −5 | 1 |
| below | 44 | 8 | 30 | 8 | −14 | 0 | 43 | 8 | 51 | 9 | 8 | 1 | ||
| 12 | Left Contra | above | 66 | 11 | 65 | 10 | −1 | 1 | 66 | 11 | 64 | 10 | −2 | −1 |
| below | 80 | 11 | 74 | 9 | −6 | −2 | 67 | 11 | 73 | 11 | 6 | 0 | ||
| Pz | Breast/Rectus Side * | Level ** | Right Pre-Op | Right Post-Op | Right Δ | Left Pre-Op | Left Post-Op | Left Δ |
|---|---|---|---|---|---|---|---|---|
| 1 | Left/Ipsilateral | above | 1 | 1 | 0 | 1 | 1 | 0 |
| below | 1 | 1 | 0 | 1 | 1 | 0 | ||
| 2 | Left/Ipsilateral | above | 1 | 1 | 0 | 1 | 1 | 0 |
| below | 1 | 1 | 0 | 1 | 3 | +2 | ||
| 3 | Left/Contralateral | above | 1 | 2 | +1 | 2 | 2 | 0 |
| below | 1 | 4 | +3 | 1 | 1 | 0 | ||
| 4 | Right/Ipsilateral | above | 1 | 1 | 0 | 1 | 1 | 0 |
| below | 1 | 1 | 0 | 1 | 1 | 0 | ||
| 5 | Right/Ipsilateral | above | 1 | 1 | 0 | 1 | 1 | 0 |
| below | 2 | 2 | 0 | 2 | 2 | 0 | ||
| 6 | Right/Ipsilateral | above | 1 | 1 | 0 | 1 | 1 | 0 |
| below | 1 | 1 | 0 | 1 | 1 | 0 | ||
| 7 | Right/Ipsilateral | above | 1 | 1 | 0 | 1 | 1 | 0 |
| below | 1 | 1 | 0 | 1 | 1 | 0 | ||
| 8 | Bilateral | above | 3 | 3 | 0 | 2 | 2 | 0 |
| below | 1 | 1 | 0 | 1 | 1 | 0 | ||
| 9 | Bilateral | above | 1 | 1 | 0 | 1 | 1 | 0 |
| below | 1 | 1 | 0 | 1 | 1 | 0 | ||
| 10 | Right/Contralateral | above | 1 | 1 | 0 | 1 | 1 | 0 |
| below | 4 | 4 | 0 | 1 | 1 | 0 | ||
| 11 | Left/Contralateral | above | 1 | 2 | +1 | 1 | 1 | 0 |
| below | 1 | 1 | 0 | 1 | 1 | 0 | ||
| 12 | Left/Contralateral | above | 1 | 1 | 0 | 1 | 1 | 0 |
| below | 1 | 1 | 0 | 1 | 1 | 0 |
| Pt | Breast/Rectus Side | Diastasis (Fingers) | Diastasis (US) | Schober Test | Trunk Flexion | Strength Test |
|---|---|---|---|---|---|---|
| 1 | Left/Ipsilateral | 3 | 32 | 0 | 0 | 10 |
| 2 | Left/Ipsilateral | 0 | 0 | 0 | 0 | 10 |
| 3 | Left/Contralateral | 2.5 | 40 | 0 | 0 | 4 |
| 4 | Right/Ipsilateral | 3 | 18 | 0 | 9 | 10 |
| 5 | Right/Ipsilateral | 3 | 20 | 0 | 6 | 10 |
| 6 | Right/Ipsilateral | 1 | 28 | 0 | 0 | 4 |
| 7 | Right/Ipsilateral | 1 | 0 | 0 | 0 | 10 |
| 8 | Bilateral | 2 | 24 | 0 | 0 | 10 |
| 9 | Bilateral | 1.5 | 16 | 0 | 0 | 10 |
| 10 | Right/Contralateral | 2 | 12 | 0 | 14 | 10 |
| 11 | Left/Contralateral | 2 | 22 | 0 | 0 | 8 |
| 12 | Left/Contralateral | 3 | 28 | 0 | 0 | 3 |
| Pt | Breast/Rectus Side | VAS Abdomen | VAS Lower Back | ODI-I | RMDQ-I |
|---|---|---|---|---|---|
| 1 | Left/Ipsilateral | 7 | 5 | 0 | 0 |
| 2 | Left/Ipsilateral | 13 | 7 | 6 | 1 |
| 3 | Left/Contralateral | 79 | 100 | 42 | 11 |
| 4 | Right/Ipsilateral | 68 | 4 | 28 | 6 |
| 5 | Right/Ipsilateral | 22 | 0 | 2 | 0 |
| 6 | Right/Ipsilateral | 3 | 1 | 0 | 0 |
| 7 | Right/Ipsilateral | 16 | 51 | 6 | 1 |
| 8 | Bilateral | 96 | 8 | 18 | 2 |
| 9 | Bilateral | 0 | 0 | 0 | 0 |
| 10 | Right/Contralateral | 0 | 57 | 12 | 0 |
| 11 | Left/Contralateral | 28 | 8 | 0 | 1 |
| 12 | Left/Contralateral | 36 | 0 | 8 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brambullo, T.; Kohlscheen, E.; Faccio, D.; Messana, F.; Vezzaro, R.; Pranovi, G.; Masiero, S.; Zampieri, S.; Ravara, B.; Bassetto, F.; et al. A New CT Analysis of Abdominal Wall after DIEP Flap Harvesting. Diagnostics 2022, 12, 683. https://doi.org/10.3390/diagnostics12030683
Brambullo T, Kohlscheen E, Faccio D, Messana F, Vezzaro R, Pranovi G, Masiero S, Zampieri S, Ravara B, Bassetto F, et al. A New CT Analysis of Abdominal Wall after DIEP Flap Harvesting. Diagnostics. 2022; 12(3):683. https://doi.org/10.3390/diagnostics12030683
Chicago/Turabian StyleBrambullo, Tito, Eva Kohlscheen, Diego Faccio, Francesco Messana, Roberto Vezzaro, Giulia Pranovi, Stefano Masiero, Sandra Zampieri, Barbara Ravara, Franco Bassetto, and et al. 2022. "A New CT Analysis of Abdominal Wall after DIEP Flap Harvesting" Diagnostics 12, no. 3: 683. https://doi.org/10.3390/diagnostics12030683