
Ultrasound Imaging of Acquired Myometrial Pseudoaneurysm: The Role of Manipulators as an Unusual Cause during Laparoscopic Surgery

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Case Report
- (i)
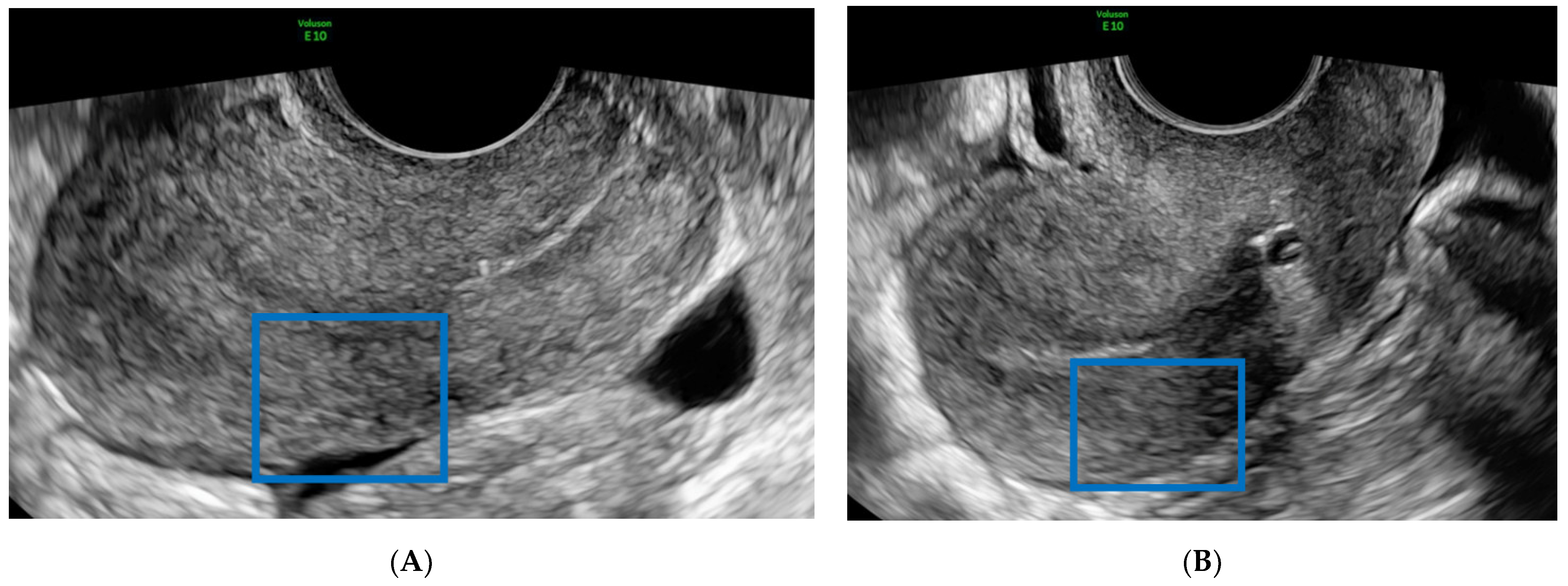
- The presence of a hypoechoic, presumably endometriotic, nodule of approximately 2 cm in the fixed vesicouterine plica;
- (ii)
- Asymmetric myometrium and some minimal focal vacuolar areas in the anterior part of the uterine corpus, suggesting diffuse adenomyosis;
- (iii)
- A unilocular avascular ground glass cyst of (49 × 36 × 56) mm suggestive of a typical endometrioma in the left ovary;
- (iv)
- Both right and left uterosacral ligaments were thickened without lesions evident at the US.
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Isono, W.; Tsutsumi, R.; Wada-Hiraike, O.; Fujimoto, A.; Osuga, Y.; Yano, T.; Taketani, Y. Uterine artery pseudoaneurysm after cesarean section: Case report and literature review. J. Minim. Invasive Gynecol. 2010, 17, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Yun, S.Y.; Lee, D.H.; Cho, K.H.; Lee, H.M.; Choi, Y.H. Delayed Postpartum Hemorrhage Resulting From Uterine Artery Pseudoaneurysm Rupture. J. Emerg. Med. 2012, 42, e11–e14. [Google Scholar] [CrossRef] [PubMed]
- Vijayakumar, A.; Srinivas, A.; Chandrashekar, B.M.; Vijayakumar, A. Uterine vascular lesions. Rev. Obstet. Gynecol. 2013, 6, 69–79. [Google Scholar] [PubMed]
- Seki, T.; Hamada, Y.; Ichikawa, T.; Onota, S.; Nakata, M.; Takakura, S. Uterine artery pseudoaneurysm caused by a uterine manipulator. Gynecol. Minim. Invasive Ther. 2017, 6, 25–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, L.B.; Clark, E.T.; Gewertz, B.L. Anastomotic and other pseudoaneurysms. In Vascular Surgery, 5th ed.; Rutherford, R.B., Ed.; Saunders: Philadelphia, PA, USA, 2000; pp. 752–763. [Google Scholar]
- Saad, N.E.A.; Davies, M.G.; Waldman, D.L.; Fultz, P.J.; Rubens, D.J. Pseudoaneurysms and the Role of Minimally Invasive Techniques in Their Management. RadioGraphics 2005, 25, S173–S189. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yang, Q.; Zhang, N.; Wang, D. Uterine artery pseudoaneurysm after treatment of cesarean scar pregnancy: A case report. BMC Pregnancy Childbirth 2021, 21, 689. [Google Scholar] [CrossRef] [PubMed]
- Zwimpfer, T.A.; Monod, C.; Redling, K.; Willi, H.; Takes, M.; Fellmann-Fischer, B.; Manegold-Brauer, G.; Hösli, I. Uterine pseudoaneurysm on the basis of deep infiltrating endometriosis during pregnancy-a case report. BMC Pregnancy Childbirth 2021, 21, 282. [Google Scholar] [CrossRef] [PubMed]
- Ito, N.; Natimatsu, Y.; Tsukada, J.; Sato, A.; Hasegawa, I.; Lin, B.-L. Two cases of postmyomectomy pseudoaneurysm treated by transarterial embolization. Cardiovasc. Interv. Radiol. 2013, 36, 1681–1685. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Samuels, S.L.; Keeffe, E.B.; Cheung, R.C. Delayed fatal hemorrhage from pseudoaneurysm of the hepatic artery after percutaneous liver Biopsyam. J. Gastroenterol. 2001, 96, 233–237. [Google Scholar] [CrossRef]
- La Perna, L.; Olin, J.W.; Goines, D.; Childs, M.B.; Ouriel, K. Ultrasound-guided thrombin injection for the treatment of postcatheterization pseudoaneurysms. Circulation 2000, 102, 2391–2395. [Google Scholar] [CrossRef]
- Soudack, M.; Epelman, M.; Gaitini, D. Spontaneous Thrombosis of Hepatic Posttraumatic Pseudoaneurysms. J. Ultrasound Med. 2003, 22, 99–103. [Google Scholar] [CrossRef]
- Mahmoud, M.Z. “To-and-fro” waveform in the diagnosis of arterial pseudoaneurysms. World J. Radiol. 2015, 7, 89–99. [Google Scholar] [CrossRef]
- Janssen, P.F.; Brölmann, H.A.M.; Huirne, J.A.F. Causes and prevention of laparoscopic ureter injuries: An analysis of 31 cases during laparoscopic hysterectomy in the Netherlands. Surg. Endosc. 2012, 27, 946–956. [Google Scholar] [CrossRef]
- Mettler, L.; Nikam, Y.A. A comparative survey of various uterine manipulators used in operative laparoscopy. Gynecol. Surg. 2006, 3, 239–243. [Google Scholar] [CrossRef]
- Rossetti, A.; Sizzi, O. Instrument Test: Uterine Manipulators for Laparoscopic Hysterectomy. Online Videojournal of the International Society for Gynecologic Endoscopy. 2005. Available online: www.thetrocar.com.
- Guerriero, S.; Condous, G.; van den Bosch, T.; Valentin, L.; Leone, F.P.G.; Van Schoubroeck, D.; Exacoustos, C.; Installé, A.J.F.; Martins, W.P.; Abrao, M.S.; et al. Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis, including terms, definitions and measurements: A consensus opinion from the International Deep Endometriosis Analysis (IDEA) group. Ultrasound Obstet. Gynecol. 2016, 48, 318–332. [Google Scholar] [CrossRef]
- Dohan, A.; Soyer, P.; Subhani, A.; Hequet, D.; Fargeaudou, Y.; Morel, O.; Boudiaf, M.; Gayat, E.; Barranger, E.; Le Dref, O.; et al. Postpartum hemorrhage resulting from pelvic pseudoaneurysm: A retrospective analysis of 588 consecutive cases treated by arterial embolization. Cardiovasc. Interv. Radiol. 2013, 36, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Boi, L.; Savastano, S.; Beghetto, M.; Dall’Acqua, J.; Mansi Montenegro, G. Embolization of iatrogenic uterine pseudoaneurysm. Gynecol. Minim. Invasive Ther. 2017, 6, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Múnera, F.; Soto, J.A.; Palacio, D.; Velez, S.M.; Medina, E. Diagnosis of Arterial Injuries Caused by Penetrating Trauma to the Neck: Comparison of Helical CT Angiography and Conventional Angiography. Radiology 2000, 216, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Soto, J.A.; Múnera, F.; Morales, C.; Lopera, J.E.; Holguín, D.; Guarín, O.; Castrillón, G.; Sanabria, A.; García, G. Focal Arterial Injuries of the Proximal Extremities: Helical CT Arteriography as the Initial Method of Diagnosis. Radiology 2001, 218, 188–194. [Google Scholar] [CrossRef]
- Neri, E.; Bonanomi, G.; Vignali, C.; Cioni, R.; Ferrari, M.; Petruzzi, P.; Bartolozzi, C. Spiral CT virtual endoscopy of abdominal arteries: Clinical applications. Abdom. Imaging 2000, 25, 59–61. [Google Scholar] [CrossRef]
- Nastri, M.V.; Baptista, L.P.S.; Baroni, R.H.; Blasbalg, R.; De Ávila, L.F.; Leite, C.C.; De Castro, C.C.; Cerri, G.G. Gadolinium-enhanced Three-dimensional MR Angiography of Takayasu Arteritis. RadioGraphics 2004, 24, 773–786. [Google Scholar] [CrossRef]
- Saboo, S.S.; Juan, Y.-H.; Belkin, M.; Sacks, A.; Khandelwal, A.; Steigner, M.L.; Rybicki, F.J. Multi-detector CT angiography in case of concomitant pseudoaneurysm and arteriovenous fistula of the lateral superior geniculate artery. Postgrad. Med. J. 2013, 90, 118–119. [Google Scholar] [CrossRef]
- Sharma, R.K.; Gore, R.; Rosen, B.D.; Arbab-Zadeh, A. Diagnosis of left ventricular pseudoaneurysm by cardiac CT angiography. J. Cardiovasc. Comput. Tomogr. 2014, 8, 246–247. [Google Scholar] [CrossRef]
- Wu, S.-H.; Wu, D.-K. Active bleeding from intercostal artery pseudoaneurysm after a percutaneous tube thoracostomy drainage procedure: Diagnosis with CT angiography and treatment with transarterial coil embolisation. BMJ Case Rep. 2018, 2018, bcr-2018-225795. [Google Scholar] [CrossRef] [Green Version]
- Jesinger, R.A.; Thoreson, A.A.; Lamba, R. Abdominal and pelvic aneurysms and pseudoaneurysms: Imaging review with clinical, radiologic, and treatment correlation. RadioGraphics 2013, 33, E71–E96. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, B.S.; Haddad, H.L.; Saddekni, S.; Lockhart, M.E. Diagnosis and Management of Pseudoaneurysms: An Update. Curr. Probl. Diagn. Radiol. 2009, 38, 170–188. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Wauters, J.; Van Calenbergh, S.; Van Schoubroeck, D.; Maleux, G.; Bosch, T.V.D.; Spitz, B. Color Doppler imaging is a valuable tool for the diagnosis and management of uterine vascular malformations. Ultrasound Obstet. Gynecol. 2003, 21, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Hata, T.; Inubashiri, E.; Kanenishi, K.; Tanaka, H.; Shiota, A.; Ohno, M. Three-dimensional power Doppler sonographic features of uterine vascular malformation. Ultrasound Obstet. Gynecol. 2004, 24, 806–808. [Google Scholar] [CrossRef]
- Ghi, T.; Giunchi, S.; Rossi, C.; Pilu, G.; Savelli, L.; Mollo, F.; Pelusi, G. Three-dimensional power Doppler sonography in the diagnosis of arteriovenous malformation of the uterus. J. Ultrasound Med. 2005, 24, 727–731. [Google Scholar] [CrossRef]
- Asai, S.; Asada, H.; Furuya, M.; Ishimoto, H.; Tanaka, M.; Yoshimura, Y. Pseudoaneurysm of the uterine artery after laparoscopic myomectomy. Fertil. Steril. 2009, 91, 929.e1–929.e3. [Google Scholar] [CrossRef]
- Polat, P.; Suma, S.; Kantarcý, M.; Alper, F.; Levent, A. Color Doppler US in the Evaluation of Uterine Vascular Abnormalities. RadioGraphics 2002, 22, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Butori, N.; Coulange, L.; Filipuzzi, L.; Krausé, D.; Loffroy, R. Pseudoaneurysm of the uterine artery after cesarean delivery. Obstet. Gynecol. 2009, 113, 540–543. [Google Scholar] [CrossRef]
- Polak, J.F. The peripheral arteries. In Diagnostic Ultrasound, 2nd ed.; Rumack, C.M., Wilson, S.R., Charboneau, J.W., Eds.; Mosby Inc.: St. Louis, CA, USA, 1988; pp. 921–941. [Google Scholar]
- Ludwin, A.; Martins, W.P.; Ludwin, I. Managing uterine artery pseudoaneurysm after myomectomy. Ultrasound Obstet. Gynecol. 2017, 52, 413–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henrich, W.; Fuchs, I.; Luttkus, A.; Hauptmann, S.; Dudenhausen, J.W. pseudoaneurysm of the uterine artery after cesarean Delivery. J. Ultrasound Med. 2002, 21, 1431–1434. [Google Scholar] [CrossRef]
- Cavoretto, P.; Cioffi, R.; Mangili, G.; Petrone, M.; Bergamini, A.; Rabaiotti, E.; Valsecchi, L.; Candiani, M.; Seckl, M.J. A Pictorial Ultrasound Essay of Gestational Trophoblastic Disease. J. Ultrasound Med. 2019, 39, 597–613. [Google Scholar] [CrossRef] [PubMed]
- Shah, Q.; Friedman, J.; Mamourian, A. Spontaneous resolution of traumatic pseudoaneurysm of the middle meningeal artery. Am. J. Neuroradiol. 2005, 26, 2530–2532. [Google Scholar]
- Takahashi, H.; Baba, Y.; Usui, R.; Ohkuchi, A.; Kijima, S.; Matsubara, S. Spontaneous resolution of post-delivery or post-abortion uterine artery pseudoaneurysm: A report of three cases. J. Obstet. Gynaecol. Res. 2016, 42, 730–733. [Google Scholar] [CrossRef]
- Lee, W.K.; Roche, C.J.; Duddalwar, V.A.; Buckley, A.R.; Morris, D. Pseudoaneurysm of the uterine artery after abdominal hysterectomy: Radiologic diagnosis and management. Am. J. Obstet. Gynecol. 2001, 185, 1269–1272. [Google Scholar] [CrossRef]
- Oishi, H.; Wada-Hiraike, O.; Osuga, Y.; Yano, T.; Kozuma, S.; Taketani, Y. Spontaneous cessation and recurrence of massive uterine bleeding can occur in uterine artery pseudoaneurysm after laparoscopically assisted myomectomy. J. Obstet. Gynaecol. Res. 2012, 39, 598–602. [Google Scholar] [CrossRef]
- Ghai, S.; Rajan, D.K.; Asch, M.R.; Muradali, D.; Simons, M.E.; TerBrugge, K.G. Efficacy of Embolization in Traumatic Uterine Vascular Malformations. J. Vasc. Interv. Radiol. 2003, 14, 1401–1408. [Google Scholar] [CrossRef]
- Takeda, A.; Koike, W.; Imoto, S.; Nakamura, H. Conservative management of uterine artery pseudoaneurysm after laparoscopic-assisted myomectomy and subsequent pregnancy outcome: Case series and review of the literature. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 182, 146–153. [Google Scholar] [CrossRef]
- Sanguin, S.; Lanta-Delmas, S.; Le Blanche, A.; Grardel-Chambenoit, E.; Merviel, P.; Gondry, J.; Fauvet, R. Diagnostic et traitement des malformations artério-veineuses utérines (MAVU) en 2011. Gynécologie Obs. Fertil. 2011, 39, 722–727. [Google Scholar] [CrossRef]
- Haak, L.V.D.; Alleblas, C.; Nieboer, T.; Rhemrev, J.P.; Jansen, F.W. Efficacy and safety of uterine manipulators in laparoscopic surgery: A review. Arch. Gynecol. Obstet. 2015, 292, 1003–1011. [Google Scholar] [CrossRef] [Green Version]
- AKavallaris, A.; Chalvatzas, N.; Kelling, K.; Bohlmann, M.K.; Diedrich, K.; Hornemann, A. Total laparoscopic hysterectomy without uterine manipulator: Description of a new technique and its outcome. Arch. Gynecol. Obstet. 2010, 283, 1053–1057. [Google Scholar] [CrossRef]
- Abd-El-Maeboud, K.H.; Elbohoty, A.E.H.; Amer, M.I.M.; Tharwat, A.A.; Khalifa, A.A.-A. Comparison of simple uterine manipulator-injector (SUMI) with the Cohen cannula in gynecologic laparoscopy. Middle East. Fertil. Soc. J. 2011, 16, 278–283. [Google Scholar] [CrossRef]
- Storz, K. Karl Storz GmbH & KG. Available online: www.karlstorz.com (accessed on 24 November 2021).
- Keriakos, R.; Zaklama, M. The RUMI manipulator and Koh colpotomiser system for total laparoscopic hysterectomy. BJOG An. Int. J. Obstet. Gynaecol. 2000, 107, 274–277. [Google Scholar] [CrossRef] [Green Version]
- Hegde, C.V. Mangeshikar Uterine Manipulator. J. Obstet. Gynecol. India 2016, 66, 134–136. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.-H.; Yeh, G.-P.; Hsieh, T.-C. Iatrogenic uterine rupture caused by overinflation of RUMI manipulator balloon. J. Minim. Invasive Gynecol. 2005, 12, 174–176. [Google Scholar] [CrossRef] [PubMed]
- Akdemir, A.; Cirpan, T. Iatrogenic uterine perforation and bowel penetration using a Hohlmanipulator: A case report. Int. J. Surg. Case Rep. 2014, 5, 271–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalek, Y.A.; Bitar, R.; Christoforou, C.; Garzon, S.; Tropea, A.; Biondi, A.; Sleiman, Z. Uterine manipulator in total laparoscopic hysterectomy: Safety and usefulness. Updat. Surg. 2019, 72, 1247–1254. [Google Scholar] [CrossRef]
- Zygouris, D.; Chalvatzas, N.; Gkoutzioulis, A.; Anastasiou, G.; Kavallaris, A. Total laparoscopic hysterectomy without uterine manipulator. A retrospective study of 1023 cases. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 253, 254–258. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Manipulator | Characteristics | Employment | Advantages | Disadvantages |
|---|---|---|---|---|
| Hohl [15,53,54] | Traumatic Reusable Pneumoperitoneum | (T)LH |
|
|
| Clermont-Ferrand [15,49] | Traumatic Reusable Pneumoperitoneum | (T)LH Endometriosis of cul-de-sac |
|
|
| Vcare [46] | Not reusable Pneumoperitoneum | (T)LH |
|
|
| RUMI a [15,50,52,54] | Traumatic Partially reusable Pneumoperitoneum | (T)LH |
|
|
| Clearview [46,54] | Traumatic Not reusable Not maintain the pneumoperitoneum | All procedures except (T)LH |
|
|
| Dr Mangeshikar [15,51] | Traumatic Reusable Pneumoperitoneum | (T)LH Endometriosis of cul-de-sac |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buonomo, F.; de Almeida Fiorillo, C.; Oliveira de Souza, D.; Mucelli, F.P.; Biffi, S.; Romano, F.; Di Lorenzo, G.; Bussolaro, S.; Ricci, G. Ultrasound Imaging of Acquired Myometrial Pseudoaneurysm: The Role of Manipulators as an Unusual Cause during Laparoscopic Surgery. Diagnostics 2022, 12, 164. https://doi.org/10.3390/diagnostics12010164
Buonomo F, de Almeida Fiorillo C, Oliveira de Souza D, Mucelli FP, Biffi S, Romano F, Di Lorenzo G, Bussolaro S, Ricci G. Ultrasound Imaging of Acquired Myometrial Pseudoaneurysm: The Role of Manipulators as an Unusual Cause during Laparoscopic Surgery. Diagnostics. 2022; 12(1):164. https://doi.org/10.3390/diagnostics12010164
Chicago/Turabian StyleBuonomo, Francesca, Clarice de Almeida Fiorillo, Danilo Oliveira de Souza, Fabio Pozzi Mucelli, Stefania Biffi, Federico Romano, Giovanni Di Lorenzo, Sofia Bussolaro, and Giuseppe Ricci. 2022. "Ultrasound Imaging of Acquired Myometrial Pseudoaneurysm: The Role of Manipulators as an Unusual Cause during Laparoscopic Surgery" Diagnostics 12, no. 1: 164. https://doi.org/10.3390/diagnostics12010164