
Low Serum Levels of Soluble Receptor Activator of Nuclear Factor κ B Ligand (sRANKL) Are Associated with Metabolic Dysregulation and Predict Long-Term Mortality in Critically Ill Patients

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. sRANKL Measurements
2.3. Statistical Analysis
3. Results
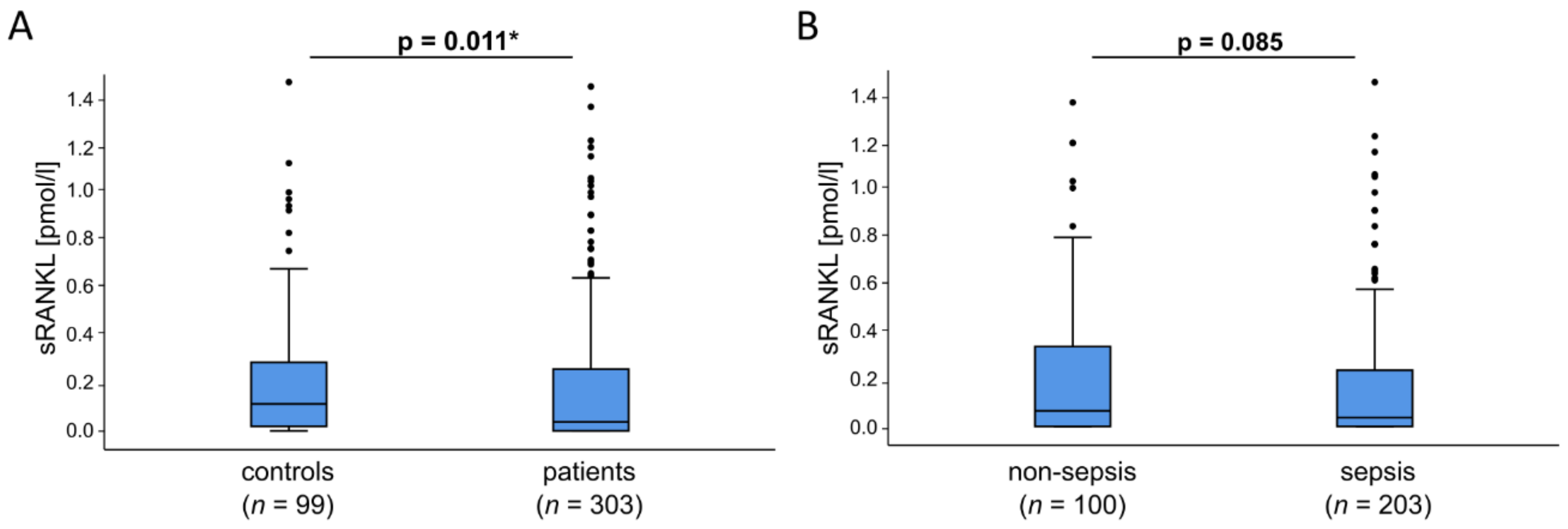
3.1. sRANKL Serum Levels Are Reduced in Critically Ill Patients at ICU Admission
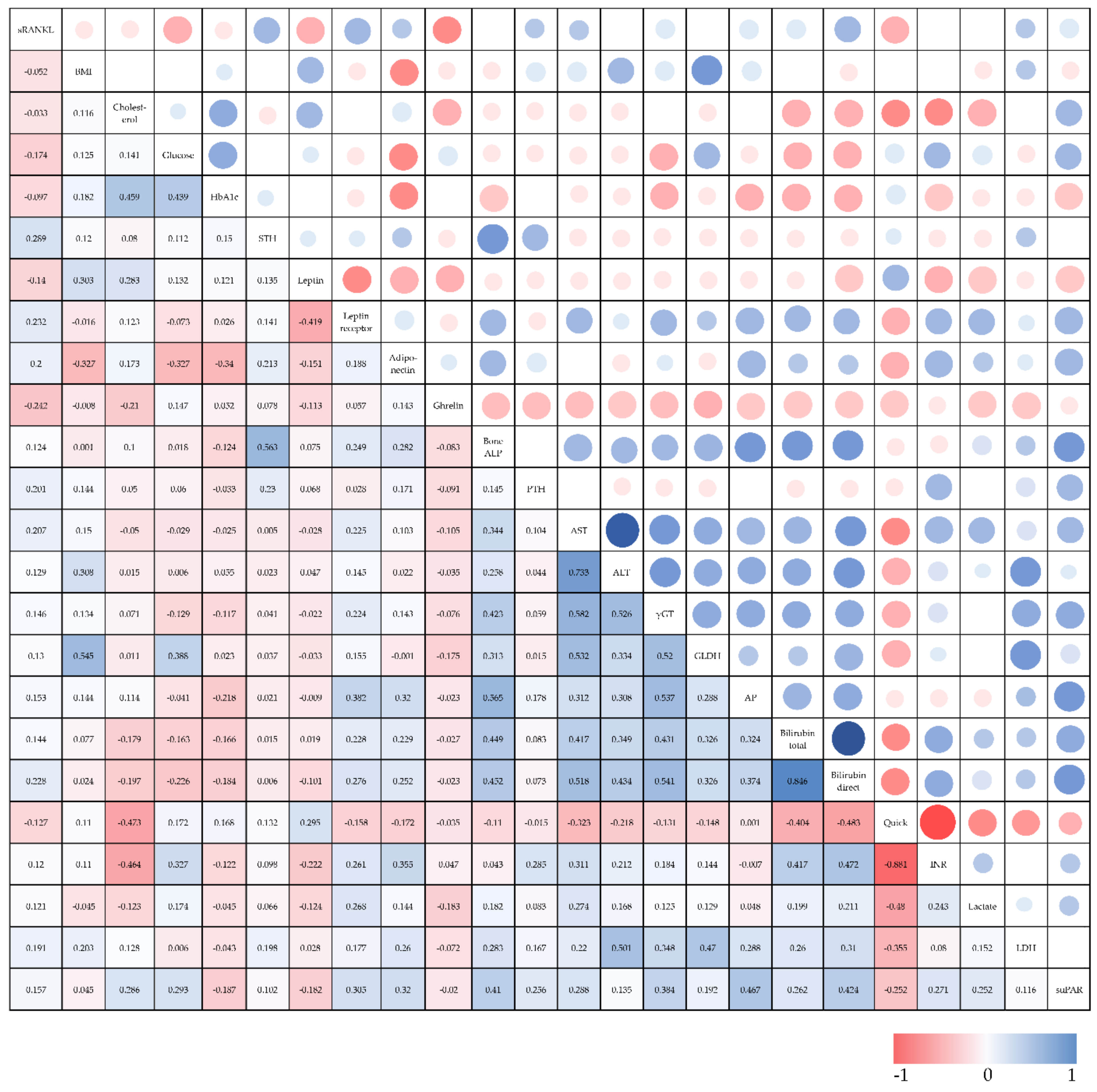
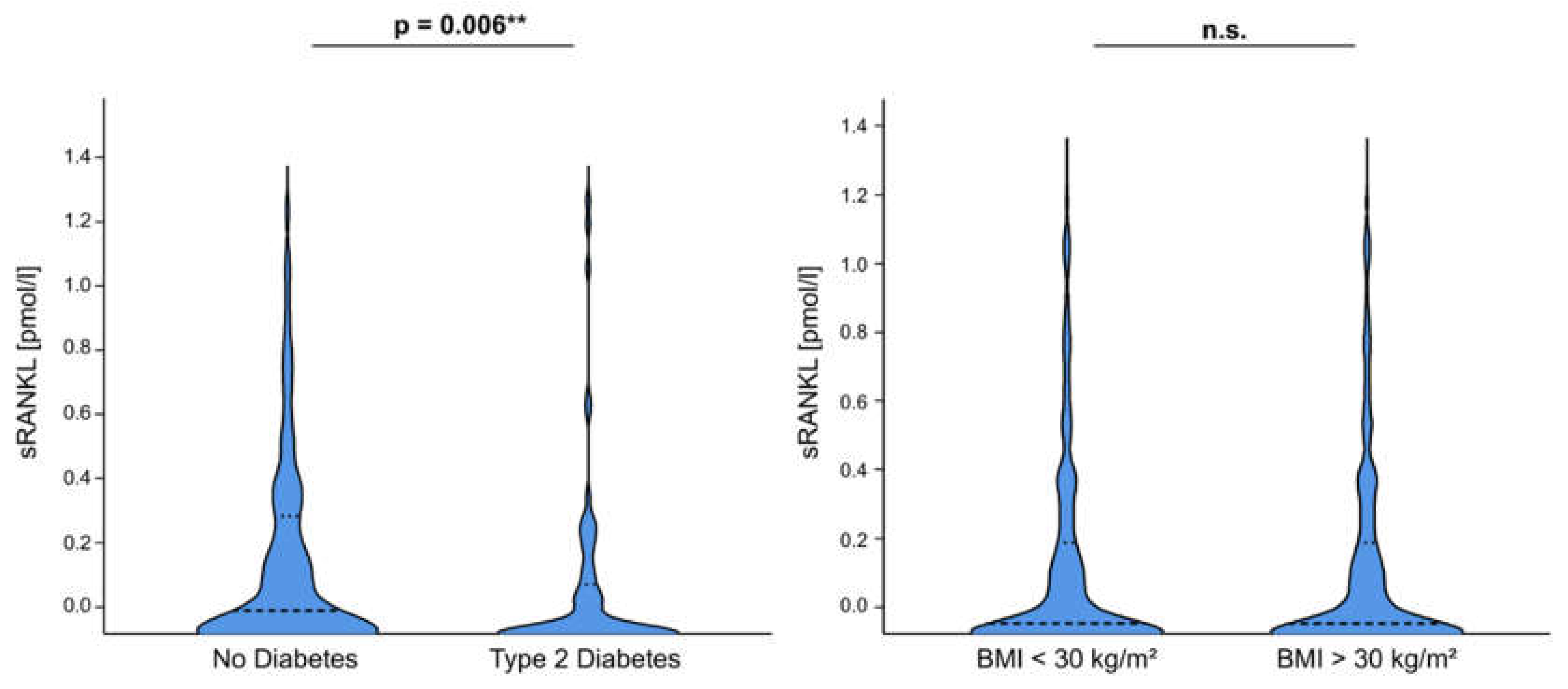
3.2. sRANKL Plasma Concentrations Are Associated with Pre-Existing Diabetes and Metabolism-Related Serum Markers in Critically Ill Patients
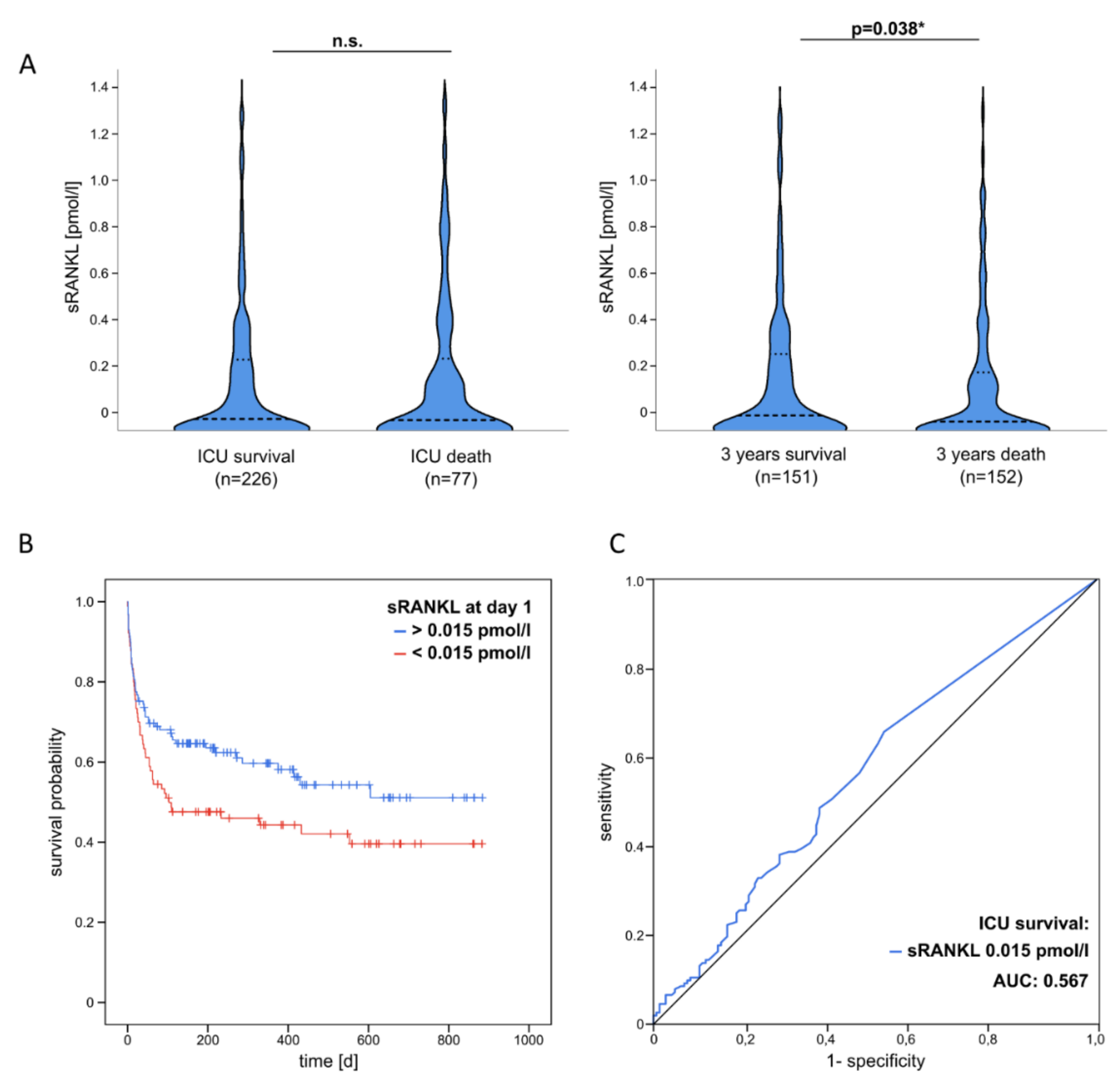
3.3. Decreased sRANKL Serum Levels at ICU Admission Are an Independent Predictor of Poor Overall Survival after Critical Illness
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef]
- Lever, A.; Mackenzie, I. Sepsis: Definition, epidemiology, and diagnosis. BMJ 2007, 335, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Pierrakos, C.; Vincent, J.-L. Sepsis biomarkers: A review. Crit. Care 2010, 14, R15. [Google Scholar] [CrossRef] [PubMed]
- Boyce, B.F.; Xing, L. Biology of RANK, RANKL, and osteoprotegerin. Arthritis Res. Ther. 2007, 9, S1. [Google Scholar] [CrossRef]
- Boyce, B.F.; Xing, L. Functions of RANKL/RANK/OPG in bone modeling and remodeling. Arch. Biochem. Biophys. 2008, 473, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Nagy, V.; Penninger, J.M. The RANKL-RANK Story. Gerontology 2015, 61, 534–542. [Google Scholar] [CrossRef]
- Kong, Y.-Y.; Yoshida, H.; Sarosi, I.; Tan, H.-L.; Timms, E.; Capparelli, C.; Morony, S.; Oliveira-dos-Santos, A.J.; Van, G.; Itie, A.; et al. OPGL is a key regulator of osteoclastogenesis, lymphocyte development and lymph-node organogenesis. Nature 1999, 397, 315–323. [Google Scholar] [CrossRef]
- Walsh, M.C.; Kim, N.; Kadono, Y.; Rho, J.; Lee, S.Y.; Lorenzo, J.; Choi, Y. Osteoimmunology: Interplay between the immune system and bone metabolism. Annu. Rev. Immunol. 2006, 24, 33–63. [Google Scholar] [CrossRef] [PubMed]
- Weitzmann, M.N. Bone and the Immune System. Toxicol. Pathol. 2017, 45, 911–924. [Google Scholar] [CrossRef]
- Hanada, R.; Leibbrandt, A.; Hanada, T.; Kitaoka, S.; Furuyashiki, T.; Fujihara, H.; Trichereau, J.; Paolino, M.; Qadri, F.; Plehm, R.; et al. Central control of fever and female body temperature by RANKL/RANK. Nature 2009, 462, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Shimamura, M.; Nakagami, H.; Osako, M.K.; Kurinami, H.; Koriyama, H.; Zhengda, P.; Tomioka, H.; Tenma, A.; Wakayama, K.; Morishita, R. OPG/RANKL/RANK axis is a critical inflammatory signaling system in ischemic brain in mice. Proc. Natl. Acad. Sci. USA 2014, 111, 8191–8196. [Google Scholar] [CrossRef]
- Kiechl, S.; Wittmann, J.; Giaccari, A.; Knoflach, M.; Willeit, P.; Bozec, A.; Moschen, A.R.; Muscogiuri, G.; Sorice, G.P.; Kireva, T.; et al. Blockade of receptor activator of nuclear factor-kappaB (RANKL) signaling improves hepatic insulin resistance and prevents development of diabetes mellitus. Nat. Med. 2013, 19, 358–363. [Google Scholar] [CrossRef]
- Loosen, S.H.; Koch, A.; Tacke, F.; Roderburg, C.; Luedde, T. The Role of Adipokines as Circulating Biomarkers in Critical Illness and Sepsis. Int. J. Mol. Sci. 2019, 20, 4820. [Google Scholar] [CrossRef]
- Force, A.D.T.; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Buendgens, L.; Yagmur, E.; Bruensing, J.; Herbers, U.; Baeck, C.; Trautwein, C.; Koch, A.; Tacke, F. C-terminal proendothelin-1 (CT-proET-1) is associated with organ failure and predicts mortality in critically ill patients. J. Intensive Care 2017, 5, 25. [Google Scholar] [CrossRef] [PubMed]
- Koch, A.; Sanson, E.; Voigt, S.; Helm, A.; Trautwein, C.; Tacke, F. Serum adiponectin upon admission to the intensive care unit may predict mortality in critically ill patients. J. Crit. Care 2011, 26, 166–174. [Google Scholar] [CrossRef]
- Koch, A.; Voigt, S.; Sanson, E.; Dückers, H.; Horn, A.; Zimmermann, H.W.; Trautwein, C.; Tacke, F. Prognostic value of circulating amino-terminal pro-C-type natriuretic peptide in critically ill patients. Crit. Care 2011, 15, R45. [Google Scholar] [CrossRef]
- Koch, A.; Sanson, E.; Helm, A.; Voigt, S.; Trautwein, C.; Tacke, F. Regulation and prognostic relevance of serum ghrelin concentrations in critical illness and sepsis. Crit. Care 2010, 14, R94. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Wilson, M.E.; Barwise, A.; Heise, K.J.; Loftsgard, T.O.; Dziadzko, M.; Cheville, A.; Majzoub, A.; Novotny, P.J.; Gajic, O.; Biehl, M. Long-Term Return to Functional Baseline After Mechanical Ventilation in the ICU. Crit. Care Med. 2018, 46, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Bilgir, O.; Yavuz, M.; Bilgir, F.; Akan, O.Y.; Bayindir, A.G.; Calan, M.; Bozkaya, G.; Yuksel, A. Relationship between insulin resistance, hs-CRP, and body fat and serum osteoprotegerin/RANKL in prediabetic patients. Minerva Endocrinol. 2018, 43, 19–26. [Google Scholar] [CrossRef]
- Kurihara, C.; Tanaka, T.; Yamanouchi, D. Hyperglycemia attenuates receptor activator of NF-kappaB ligand-induced macrophage activation by suppressing insulin signaling. J. Surg. Res. 2017, 214, 168–175. [Google Scholar] [CrossRef]
- Serrano-Piña, R.; Trujillo-Güiza, M.L.; Scougall Vilchis, R.J.; Layton-Tovar, C.F.; Mendieta-Zerón, H. sRANKL and its correlation with metabolic syndrome parameters in children. Int J. Paediatr. Dent. 2018, 28, 633–640. [Google Scholar] [CrossRef]
- Hillenbrand, A.; Knippschild, U.; Weiss, M.; Schrezenmeier, H.; Henne-Bruns, D.; Huber-Lang, M.; Wolf, A.M. Sepsis induced changes of adipokines and cytokines—septic patients compared to morbidly obese patients. BMC Surg. 2010, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Berg, A.H.; Combs, T.P.; Scherer, P.E. ACRP30/adiponectin: An adipokine regulating glucose and lipid metabolism. Trends Endocrinol. Metab. 2002, 13, 84–89. [Google Scholar] [CrossRef]
- Teoh, H.; Quan, A.; Bang, K.W.; Wang, G.; Lovren, F.; Vu, V.; Haitsma, J.J.; Szmitko, P.E.; Al-Omran, M.; Wang, C.-H.; et al. Adiponectin deficiency promotes endothelial activation and profoundly exacerbates sepsis-related mortality. Am. J. Physiol. Endocrinol. Metab. 2008, 295, E658–E664. [Google Scholar] [CrossRef]
- Koch, A.; Weiskirchen, R.; Zimmermann, H.W.; Sanson, E.; Trautwein, C.; Tacke, F. Relevance of serum leptin and leptin-receptor concentrations in critically ill patients. Mediat. Inflamm. 2010, 2010, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Trieb, K.; Windhager, R. Receptor activator of nuclear factor kappaB expression is a prognostic factor in human osteosarcoma. Oncol. Lett. 2015, 10, 1813–1815. [Google Scholar] [CrossRef]
- Lee, J.-A.; Jung, J.-S.; Kim, D.-H.; Lim, J.-S.; Kim, M.-S.; Kong, C.-B.; Song, W.-S.; Cho, W.-H.; Jeon, D.-G.; Lee, S.-Y.; et al. RANKL expression is related to treatment outcome of patients with localized, high-grade osteosarcoma. Pediatr. Blood Cancer 2011, 56, 738–743. [Google Scholar] [CrossRef]
- Afzal, M.Z.; Shirai, K. Immune checkpoint inhibitor (anti-CTLA-4, anti-PD-1) therapy alone versus immune checkpoint inhibitor (anti-CTLA-4, anti-PD-1) therapy in combination with anti-RANKL denosumuab in malignant melanoma: A retrospective analysis at a tertiary care center. Melanoma Res. 2018, 28, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Smyth, M.J.; Yagita, H.; McArthur, G.A. Combination Anti-CTLA-4 and Anti-RANKL in Metastatic Melanoma. J. Clin. Oncol. 2016, 34, e104–e106. [Google Scholar] [CrossRef]
- van Dam, P.A.; Verhoeven, Y.; Trinh, X.B.; Wouters, A.; Lardon, F.; Prenen, H.; Smits, E.; Baldewijns, M.; Lammens, M. RANK/RANKL signaling inhibition may improve the effectiveness of checkpoint blockade in cancer treatment. Crit. Rev. Oncol. Hematol. 2019, 133, 85–91. [Google Scholar] [CrossRef]
- de Groot, A.F.; Appelman-Dijkstra, N.M.; van der Burg, S.H.; Kroep, J.R. The anti-tumor effect of RANKL inhibition in malignant solid tumors—A systematic review. Cancer Treat. Rev. 2018, 62, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Deeks, E.D. Author Correction to: Denosumab: A Review in Postmenopausal Osteoporosis. Drugs Aging 2018, 35, 261. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, K.; Kusunoki, N.; Hasunuma, T.; Kawai, S. Changes of serum soluble receptor activator for nuclear factor-kappaB ligand after glucocorticoid therapy reflect regulation of its expression by osteoblasts. J. Clin. Endocrinol. Metab. 2012, 97, E1909–E1917. [Google Scholar] [CrossRef] [PubMed]
- Loosen, S.H.; Schulze-Hagen, M.; Püngel, T.; Bündgens, L.; Wirtz, T.; Kather, J.N.; Vucur, M.; Paffenholz, P.; Demir, M.; Bruners, P.; et al. Skeletal Muscle Composition Predicts Outcome in Critically Ill Patients. Crit. Care Explor. 2020, 2, e0171. [Google Scholar] [CrossRef]
- Wirtz, T.H.; Loosen, S.H.; Schulze-Hagen, M.; Weiskirchen, R.; Buendgens, L.; Abu Jhaisha, S.; Brozat, J.F.; Puengel, T.; Vucur, M.; Paffenholz, P.; et al. CT-based determination of excessive visceral adipose tissue is associated with an impaired survival in critically ill patients. PLoS ONE 2021, 16, e0250321. [Google Scholar] [CrossRef]
- Pepper, D.J.; Sun, J.; Welsh, J.; Cui, X.; Suffredini, A.F.; Eichacker, P.Q. Increased body mass index and adjusted mortality in ICU patients with sepsis or septic shock: A systematic review and meta-analysis. Crit. Care 2016, 20, 181. [Google Scholar] [CrossRef]
- Muscedere, J.; Waters, B.; Varambally, A.; Bagshaw, S.M.; Boyd, J.G.; Maslove, D.; Sibley, S.; Rockwood, K. The impact of frailty on intensive care unit outcomes: A systematic review and meta-analysis. Intensive Care Med. 2017, 43, 1105–1122. [Google Scholar] [CrossRef]
- Panizo, S.; Cardus, A.; Encinas, M.; Parisi, E.; Valcheva, P.; Lopez-Ongil, S.; Coll, B.; Fernandez, E.; Valdivielso, J.M. RANKL increases vascular smooth muscle cell calcification through a RANK-BMP4-dependent pathway. Circ. Res. 2009, 104, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, C.; Piemonte, S.; Colangelo, L.; De Martino, V.; Diacinti, D.; Ferrone, F.; Piazzolla, V.; Fassino, V.; Nieddu, L.; Minisola, S.; et al. Inhibition of the RANKL with denosumab has no effect on circulating markers of atherosclerosis in women with postmenopausal osteoporosis: A pilot study. Endocrine 2021, 71, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Zhang, R.; Zhao, H.; Liu, T.; Ren, M.; Song, Y.; Liu, S.; Cong, H. Relationship between serum levels of osteoproteins, inflammatory cytokines and coronary heart disease and disease severity. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2019, 31, 588–593. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All Patients | Sepsis | Non-Sepsis | p * |
|---|---|---|---|---|
| Number | 303 | 203 | 100 | |
| Sex (male/female) | 185/118 | 124/79 | 61/39 | n.s. |
| Age median, (range in years) | 63 (18–89) | 65 (21–89) | 60 (18–85) | n.s. |
| BMI median, (range in kg/m2) | 26 (16–87) | 26 (17–87) | 26 (16–53) | n.s. |
| Type 2 Diabetes presence (%) | 82 (27) | 54 (27) | 28 (28) | n.s. |
| APACHE-II score, median (range) | 18 (2–43) | 19 (3–43) | 15 (2–33) | <0.001 |
| SOFA score, median (range) | 9 (0–19) | 10 (0–19) | 7 (0–17) | 0.001 |
| SAPS 2 score, median (range) | 43 (0–80) | 44 (0–79) | 42 (13–80) | n.s. |
| Mechanical ventilation, n (%) | 226 (75) | 160 (79) | 66 (66) | 0.016 |
| Vasopressor demand, n (%) | 167 (55) | 123 (60) | 44 (44) | <0.001 |
| ICU days, median (range) | 9 (1–357) | 12 (1–137) | 7 (1–357) | <0.001 |
| 30-day mortality, n (%) | 95 (31) | 67 (33) | 28 (28) | <0.001 |
| 3-year mortality, n (%) | 152 (50) | 88 (43) | 64 (64) | <0.001 |
| sRANKL, median (range in pmol/L) | 0.04 (0–2.58) | 0.04 (0–2.58) | 0.07 (0–1.79) | 0.085 |
| CRP, median (range in mg/L) | 93 (5–230) | 152 (5–230) | 17 (5–230) | <0.001 |
| Leucocytes, median (range in per nL) | 12.5 (1.8–149.0) | 12.9 (1.8–149.0) | 12.1 (1.8–29.6) | 0.025 |
| Cystatin C, median (range in mg/L) | 1.81 (0.41–7.57) | 2.00 (0.41–7.57) | 1.26 (0.41–5.41) | <0.001 |
| Bilirubin, median (range in mg/dL) | 0.8 (0.1–40.4) | 0.78 (0.1–40.4) | 0.8 (0.1–39.1) | n.s. |
| Etiology in Critically Ill Patients | Sepsis n = 203 |
|---|---|
| Pulmonary (%) | 115 (57) |
| Abdominal (%) | 33 (16) |
| Urogenital (%) | 8 (4) |
| Other (%) | 47 (23) |
| Etiology of non-sepsis in critically ill patients | Non-Sepsis n = 100 |
| Cardio-pulmonary disorder (%) | 35 (35) |
| Decompensated liver cirrhosis (%) | 17 (17) |
| Acute pancreatitis (%) | 13 (13) |
| Severe gastrointestinal hemorrhage (%) | 7 (7) |
| Acute liver failure (%) | 4 (4) |
| Other (%) | 24 (24) |
| ICU Patients | |||
|---|---|---|---|
| r | p | ||
| Obesity and diabetes | |||
| BMI | −0.052 | 0.385 | |
| Triglycerides | −0.006 | 0.926 | |
| Cholesterol | −0.033 | 0.605 | |
| HDL | −0.092 | 0.317 | |
| LDL | −0.056 | 0.543 | |
| Glucose | −0.174 ** | 0.003 ** | |
| HbA1c | −0.097 | 0.282 | |
| Insulin | −0.054 | 0.553 | |
| C−Peptide | 0.008 | 0.926 | |
| STH | 0.289 ** | 0.002 ** | |
| Leptin | −0.140 | 0.119 | |
| Leptin receptor | 0.232 ** | 0.009 ** | |
| Adiponectin | 0.2 * | 0.03 * | |
| Ghrelin | −0.242 ** | 0.01 * | |
| Bone metabolism | |||
| Bone ALP | 0.124 | 0.208 | |
| PTH | 0.201 * | 0.027 * | |
| Vitamin D3 | −0.009 | 0.927 | |
| Serum calcium | 0.01 | 0.859 | |
| Markers of inflammation | |||
| CRP | −0.022 | 0.707 | |
| Procalcitonin | 0.076 | 0.262 | |
| IL6 | 0.087 | 0.186 | |
| TNFα | 0.209 * | 0.047 * | |
| Liver injury and cholestasis | |||
| AST | 0.207 ** | <0.001 *** | |
| ALT | 0.129 * | 0.026 * | |
| γGT | 0.146 * | 0.011 * | |
| GLDH | 0.13 * | 0.032 * | |
| AP | 0.153 * | 0.01 * | |
| Bilirubin total | 0.144 * | 0.012 * | |
| Bilirubin direct | 0.228 ** | 0.001 ** | |
| Prothrombin time | 0.085 | 0.144 | |
| Quick | −0.127 * | 0.028 * | |
| INR | 0.12 * | 0.04 * | |
| Albumin | −0.078 | 0.304 | |
| Urea | −0.023 | 0.695 | |
| Lactate | 0.121 * | 0.039 * | |
| LDH | 0.191 * | <0.001 *** | |
| NTproBNP | −0.043 | 0.596 | |
| Renal function | |||
| Cystatin C | 0.022 | 0.764 | |
| GFR | 0.043 | 0.533 | |
| Clinical scores | |||
| APACHE−II | 0.008 | 0.897 | |
| SOFA | 0.054 | 0.538 | |
| SAPS 2 | −0.085 | 0.38 | |
| New and experimental biomarkers | |||
| suPAR | 0.157 * | 0.022 * |  |
| Parameter | Univariate Cox Regression | |
|---|---|---|
| p-Value | Hazard Ratio (95% CI) | |
| sRANKL | 0.048 * | 0.678 (0.461–0.996) |
| Age | 0.002 ** | 1.022 (1.008–1.036) |
| Sex | 0.398 | 1.185 (0.800–1.754) |
| BMI | 0.045 * | 0.965 (0.931–0.999) |
| Leukocytes | 0.340 | 0.989 (0.967–1.012) |
| CRP | 0.314 | 1.001 (0.999–1.003) |
| Bilirubin total | 0.005 ** | 1.057 (1.026–1.088) |
| Creatinine | 0.532 | 1.020 (0.959–1.085) |
| Hemoglobin | 0.029 * | 0.991 (0.982–0.999) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puengel, T.; Weber, B.; Wirtz, T.H.; Buendgens, L.; Loosen, S.H.; Geisler, L.; Özdirik, B.; Hamesch, K.; Jhaisha, S.A.; Brozat, J.F.; et al. Low Serum Levels of Soluble Receptor Activator of Nuclear Factor κ B Ligand (sRANKL) Are Associated with Metabolic Dysregulation and Predict Long-Term Mortality in Critically Ill Patients. Diagnostics 2022, 12, 62. https://doi.org/10.3390/diagnostics12010062
Puengel T, Weber B, Wirtz TH, Buendgens L, Loosen SH, Geisler L, Özdirik B, Hamesch K, Jhaisha SA, Brozat JF, et al. Low Serum Levels of Soluble Receptor Activator of Nuclear Factor κ B Ligand (sRANKL) Are Associated with Metabolic Dysregulation and Predict Long-Term Mortality in Critically Ill Patients. Diagnostics. 2022; 12(1):62. https://doi.org/10.3390/diagnostics12010062
Chicago/Turabian StylePuengel, Tobias, Beate Weber, Theresa H. Wirtz, Lukas Buendgens, Sven H. Loosen, Lukas Geisler, Burcin Özdirik, Karim Hamesch, Samira Abu Jhaisha, Jonathan F. Brozat, and et al. 2022. "Low Serum Levels of Soluble Receptor Activator of Nuclear Factor κ B Ligand (sRANKL) Are Associated with Metabolic Dysregulation and Predict Long-Term Mortality in Critically Ill Patients" Diagnostics 12, no. 1: 62. https://doi.org/10.3390/diagnostics12010062