
Performance Evaluation of the KRYPTOR Compact PLUS Analyzer-Based B.R.A.H.M.S. CgA Ⅱ KRYPTOR Assay for Chromogranin A Measurement


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Linearity and Precision
2.3. CgA Values Relative to Patient Diagnosis
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Assay Characteristics
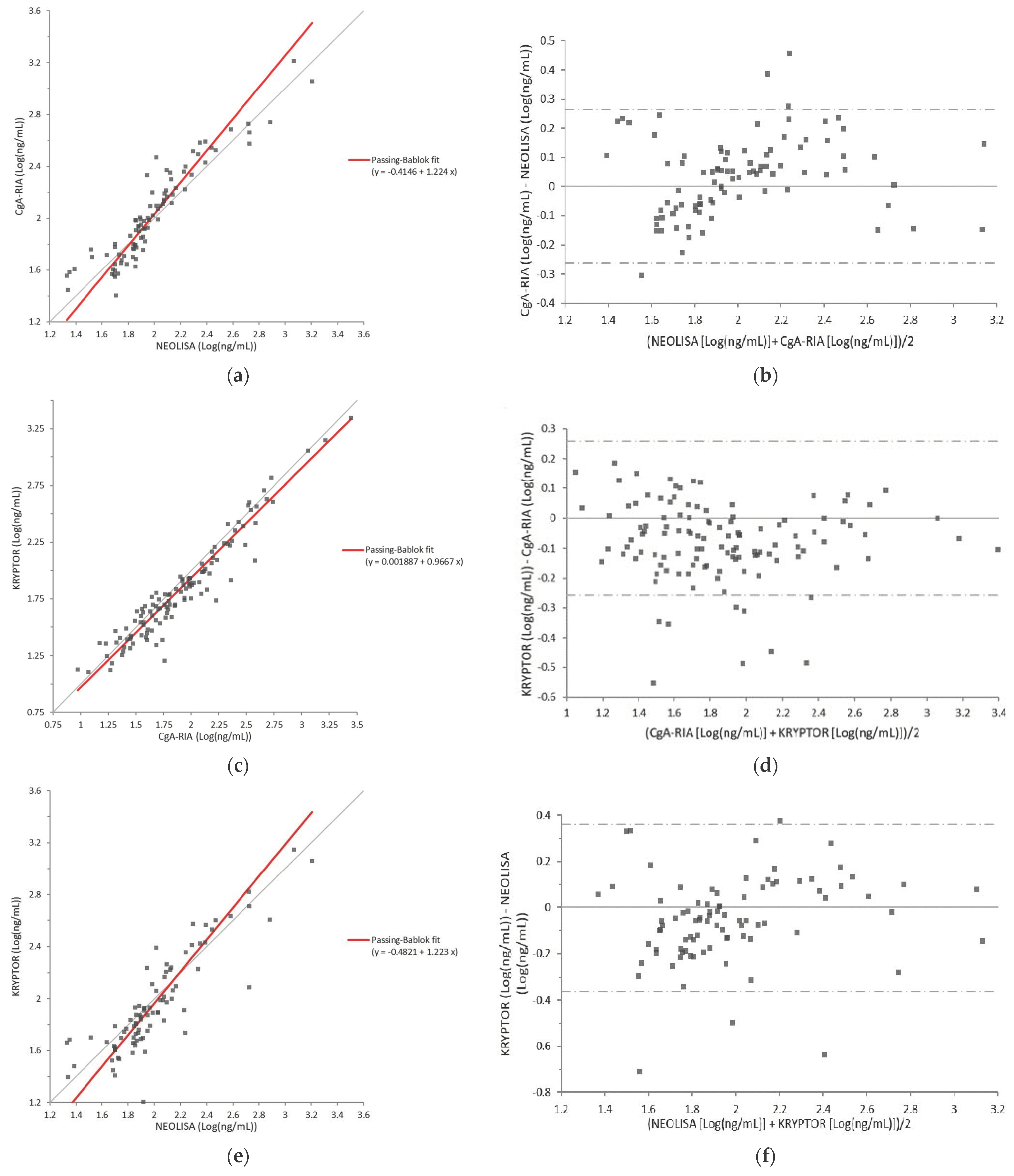
3.3. Correlation
3.3.1. CgA-RIA versus NEOLISA
3.3.2. CgA-RIA versus KRYPTOR
3.3.3. NEOLISA versus KRYPTOR
3.4. Linearity
3.5. Precision
3.6. CgA Values According to Patient Diagnosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Modlin, I.M.; Gustafsson, B.I.; Moss, S.F.; Pavel, M.; Tsolakis, A.V.; Kidd, M. Chromogranin A—Biological Function and Clinical Utility in Neuro Endocrine Tumor Disease. Ann. Surg. Oncol. 2010, 17, 2427–2443. [Google Scholar] [CrossRef]
- Barakat, M.T.; Meeran, K.; Bloom, S.R. Neuroendocrine tumours. Endocr. Relat. Cancer 2004, 11, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Rindi, G.; Klimstra, D.S.; Abedi-Ardekani, B.; Asa, S.L.; Bosman, F.T.; Brambilla, E.; Busam, K.J.; De Krijger, R.R.; Dietel, M.; El-Naggar, A.K.; et al. A common classification framework for neuroendocrine neoplasms: An International Agency for Research on Cancer (IARC) and World Health Organization (WHO) expert consensus proposal. Mod. Pathol. 2018, 31, 1770–1786. [Google Scholar] [CrossRef] [PubMed]
- Modlin, I.M.; Champaneria, M.C.; Bornschein, J.; Kidd, M. Evolution of the Diffuse Neuroendocrine System–Clear Cells and Cloudy Origins. Neuroendocrinology 2006, 84, 69–82. [Google Scholar] [CrossRef] [PubMed]
- Goetze, J.P.; Alehagen, U.; Flyvbjerg, A.; Rehfeld, J.F. Chromogranin A as a biomarker in cardiovascular disease. Biomark. Med. 2014, 8, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Broedbaek, K.; Hilsted, L. Chromogranin A as biomarker in diabetes. Biomark. Med. 2016, 10, 1181–1189. [Google Scholar] [CrossRef]
- Natori, S.; Huttner, W.B. Chromogranin B (secretogranin I) promotes sorting to the regulated secretory pathway of processing intermediates derived from a peptide hormone precursor. Proc. Natl. Acad. Sci. USA 1996, 93, 4431–4436. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.; Tao-Cheng, J.-H.; Eiden, L.; Loh, Y. Chromogranin A, an “On/Off” Switch Controlling Dense-Core Secretory Granule Biogenesis. Cell 2001, 106, 499–509. [Google Scholar] [CrossRef] [Green Version]
- Konecki, D.S.; Benedum, U.M.; Gerdes, H.H.; Huttner, W.B. The primary structure of human chromogranin A and pan-creastatin. J. Biol. Chem. 1987, 262, 17026–17030. [Google Scholar] [CrossRef]
- Woulfe, J.; Deng, D.; Munoz, D. Chromogranin A in the central nervous system of the rat: Pan-neuronal expression of its mRNA and selective expression of the protein. Neuropeptides 1999, 33, 285–300. [Google Scholar] [CrossRef]
- ThermoFisher Scientific. TRACE—Powerful technology. Available online: https://www.brahms-instruments.com/trace-technology.html (accessed on 8 February 2021).
- Brehm Hoej, L.; Parkner, T.; Soendersoe Knudsen, C.; Grønbaek, H. A comparison of three chromogranin A assays in patients with neuroendocrine tumours. J. Gastrointestin. Liver Dis. 2014, 23, 419–424. [Google Scholar] [CrossRef]
- Van der Knaap, R.H.P.; Kwekkeboom, D.J.; Ramakers, C.R.B.; de Rijke, Y.B. Evaluation of a new immunoassay for chro-mogranin A measurement on the Kryptor system. Pract. Lab. Med. 2015, 1, 5–11. [Google Scholar] [CrossRef] [Green Version]
- Degorce, F.; Goumon, Y.; Jacquemart, L.; Vidaud, C.; Bellanger, L.; Pons-Anicet, D.; Seguin, P.; Metz-Boutigue, M.H.; Aunis, D. A new human chromogranin A (CgA) immunoradiometric assay involving monoclonal antibodies raised against the unprocessed central domain (145-245). Br. J. Cancer 1998, 79, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Clinical and Laboratory Standards Institute. User Verification of Performance for Precision and Trueness. In Approved Guideline, 2nd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2014. [Google Scholar]
- Lim, M.; Erdman, P.; Cho, S.; Mathew, A.; Fleisher, M.; Thoren, K.L. Evaluation of CisBio ELISA for Chromogranin A Meas-urement. J. Appl. Lab. Med. 2019, 4, 11–18. [Google Scholar] [CrossRef]
- Stridsberg, M.; Eriksson, B.; Oberg, K.; Janson, E.T. A comparison between three commercial kits for chromogranin A meas-urements. J. Endocrinol. 2003, 177, 337–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stridsberg, M.; Oberg, K.; Li, Q.; Engström, U.; Lundqvist, G. Measurements of chromogranin A, chromogranin B (secretogranin I), chromogranin C (secretogranin II) and pancreastatin in plasma and urine from patients with carcinoid tumours and endocrine pancreatic tumours. J. Endocrinol. 1995, 144, 49–59. [Google Scholar] [CrossRef]
- Bluemn, E.G.; Coleman, I.M.; Lucas, J.M.; Coleman, R.T.; Hernandez-Lopez, S.; Tharakan, R. Androgen receptor path-way-independent prostate cancer is sustained through FGF signaling. Cancer Cell 2017, 32, 474–489. [Google Scholar] [CrossRef] [Green Version]
- Sciarra, A.; Di Silverio, F.; Autran, A.M.; Salciccia, S.; Gentilucci, A.; Alfarone, A.; Gentile, V. Distribution of High Chromogranin A Serum Levels in Patients with Nonmetastatic and Metastatic Prostate Adenocarcinoma. Urol. Int. 2009, 82, 147–151. [Google Scholar] [CrossRef]
- Malaguarnera, M.; Cristaldi, E.; Cammalleri, L.; Colonna, V.; Lipari, H.; Capici, A.; Cavallaro, A.; Beretta, M.; Alessandria, I.; Luca, S.; et al. Elevated chromogranin A (CgA) serum levels in the patients with advanced pancreatic cancer. Arch. Gerontol. Geriatr. 2009, 48, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Giusti, M.; Sidoti, M.; Augeri, C.; Rabitti, C.; Minuto, F. Effect of short-term treatment with low dosages of the proton-pump inhibitor omeprazole on serum chromogranin A levels in man. Eur. J. Endocrinol. 2004, 150, 299–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsiao, R.J.; Mezger, M.S.; O’Connor, D.T. Chromogranin A in uremia: Progressive retention of immunoreactive fragments. Kidney Int. 1990, 37, 955–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | Patients (n = 118) |
|---|---|
| Age, years | |
| Mean (SD) | 59.9 (17.1) |
| Sex, n (%) | |
| Male | 73 (61.9) |
| Female | 45 (38.1) |
| Main diagnosis, n (%) | |
| GEP-NET | |
| Pancreas | 19 (16.1) |
| Liver | 1 (0.8) |
| Stomach | 1 (0.8) |
| Appendix | 1 (0.8) |
| Rectum | 1 (0.8) |
| Paraganglioma | 1 (0.8) |
| Pituitary | |
| Tumor | 19 (16.1) |
| Other | 2 (1.7) |
| Thyroid disease | 6 (5.1) |
| Adrenal gland tumor | 12 (10.2) |
| Prostate cancer | 30 (25.4) |
| Pancreatic tumor | 14 (11.9) |
| Liver | |
| Hepatitis | 1 (0.8) |
| HCC | 1 (0.8) |
| Von Hippel–Lindau disease | 2 (1.7) |
| MEN1 | 1 (0.8) |
| Other | 6 (5.1) |
| PPI administration, n (%) | 23 (19.5) |
| Assay | |||
|---|---|---|---|
| NEOLISA Chromogranin A | B.R.A.H.M.S. CgA Ⅱ | CgA-RIA CT | |
| Method | ELISA | TRACE * | RIA |
| Company name | EuroDiagnostica (Malmö, Sweden) | Thermo Fisher Scientific (Waltham, MA USA) | CisBio (Codolet, France) |
| Antibody | 2 monoclonal | 2 monoclonal | 2 monoclonal |
| Epitope | Residues 236–251, 264–279 [12] | Residues 250–301, unknown [13] | Residues 145–245 [14] |
| Unit | ng/mL, nmol/L, U/L | ng/mL | ng/mL |
| Recommended specimen | Serum, EDTA/heparin plasma | Serum, EDTA plasma | Serum, plasma |
| Cut-off | Heparin plasma: ≤108 ng/mL (or 3.0 nM or 35 U/L) | Serum: <101.9 ng/mL | Serum: <98 ng/mL |
| Operating mode | Batch | Random-access | Batch |
| Incubation time | 105 min | 29 min | 120 min |
| Required sample volume | 50 µL | 14 µL | 50 µL |
| CgA | Below Cut-Off | Above Cut-Off | Total | Cohen’s κ | |
|---|---|---|---|---|---|
| NEOLISA | |||||
| CgA-RIA | Below cut-off * | 82 | 0 | 82 | 0.826 (95% CI: 0.771–0.881) |
| Above cut-off * | 9 | 32 | 41 | ||
| Total | 91 | 32 | 123 | ||
| CgA-RIA | |||||
| KRYPTOR | Below cut-off † | 82 | 12 | 94 | 0.763 (95% CI: 0.700–0.826) |
| Above cut-off † | 0 | 29 | 29 | ||
| Total | 82 | 41 | 123 | ||
| KRYPTOR | |||||
| NEOLISA | Below cut-off ‡ | 87 | 4 | 91 | 0.760 (95% CI: 0.692–0.828) |
| Above cut-off ‡ | 7 | 25 | 32 | ||
| Total | 94 | 29 | 123 | ||
| Imprecision (%CV) | |||||
|---|---|---|---|---|---|
| Chromogranin A | Mean | SD | Within-Run | Between-Day | Total |
| Low | 75.55 | 1.44 | 1.72 | 1.94 | 1.19 |
| High | 486.6 | 10.46 | 1.44 | 2.26 | 1.86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.J.; Roh, J.; Kim, S.; Lee, K.-A.; Park, Y. Performance Evaluation of the KRYPTOR Compact PLUS Analyzer-Based B.R.A.H.M.S. CgA Ⅱ KRYPTOR Assay for Chromogranin A Measurement. Diagnostics 2021, 11, 2400. https://doi.org/10.3390/diagnostics11122400
Choi YJ, Roh J, Kim S, Lee K-A, Park Y. Performance Evaluation of the KRYPTOR Compact PLUS Analyzer-Based B.R.A.H.M.S. CgA Ⅱ KRYPTOR Assay for Chromogranin A Measurement. Diagnostics. 2021; 11(12):2400. https://doi.org/10.3390/diagnostics11122400
Chicago/Turabian StyleChoi, Yu Jeong, Juhye Roh, Sinyoung Kim, Kyung-A Lee, and Younhee Park. 2021. "Performance Evaluation of the KRYPTOR Compact PLUS Analyzer-Based B.R.A.H.M.S. CgA Ⅱ KRYPTOR Assay for Chromogranin A Measurement" Diagnostics 11, no. 12: 2400. https://doi.org/10.3390/diagnostics11122400