
Incidence, Clinical Presentation and Trends in Indication for Diagnostic Work-Up of Small Intestinal and Pancreatic Neuroendocrine Tumors

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Methods
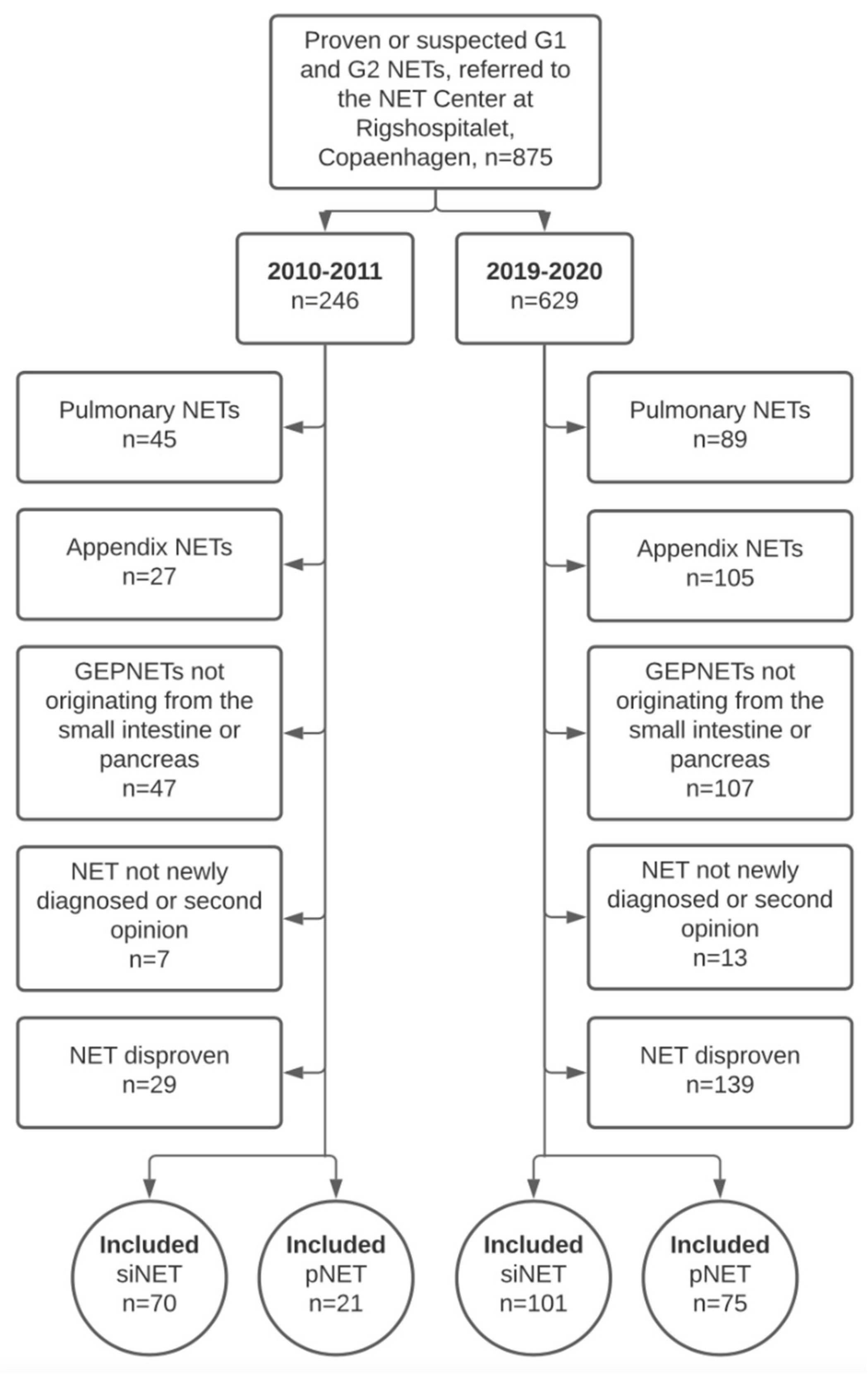
2.1. Study Population
2.2. Definitions
2.3. Statistics
2.4. Ethics
3. Results
3.1. Baseline Characteristics
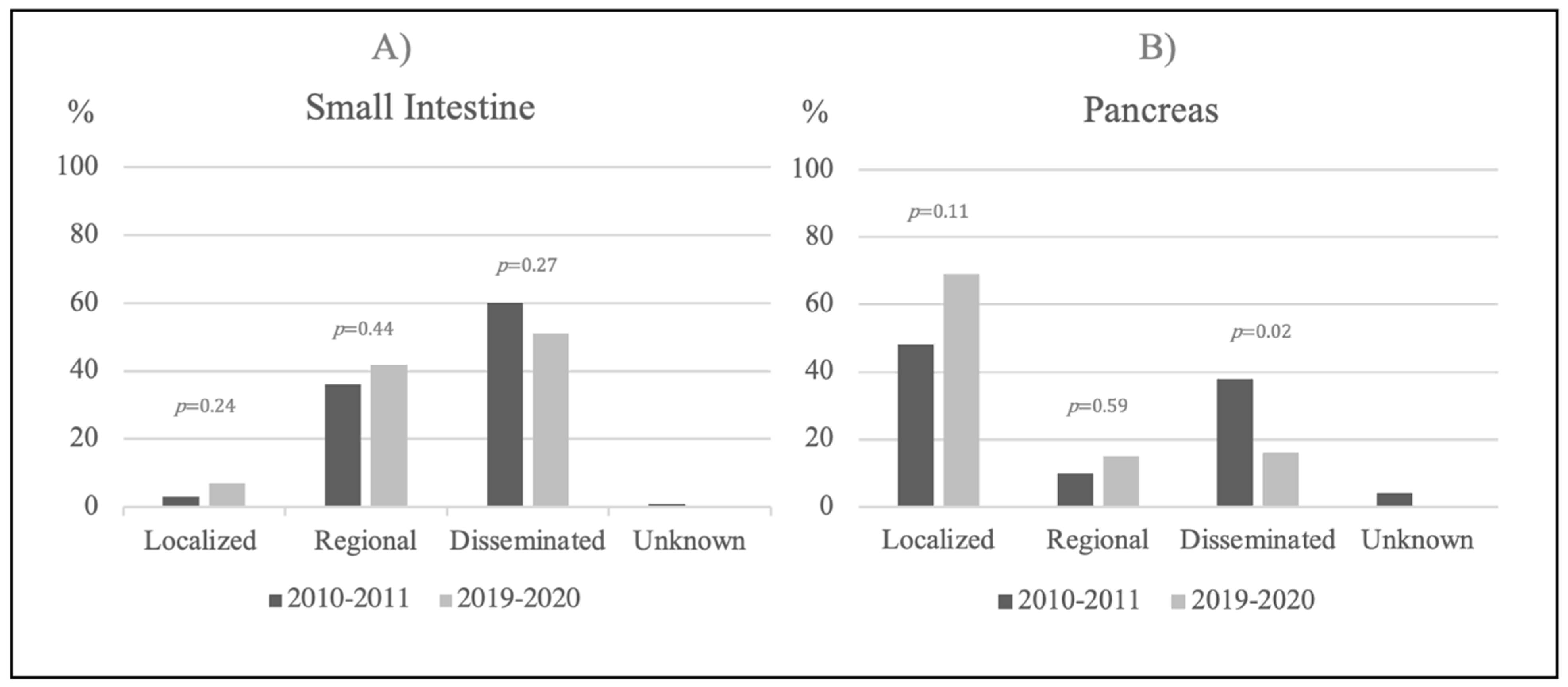
3.2. Small Intestinal NETs
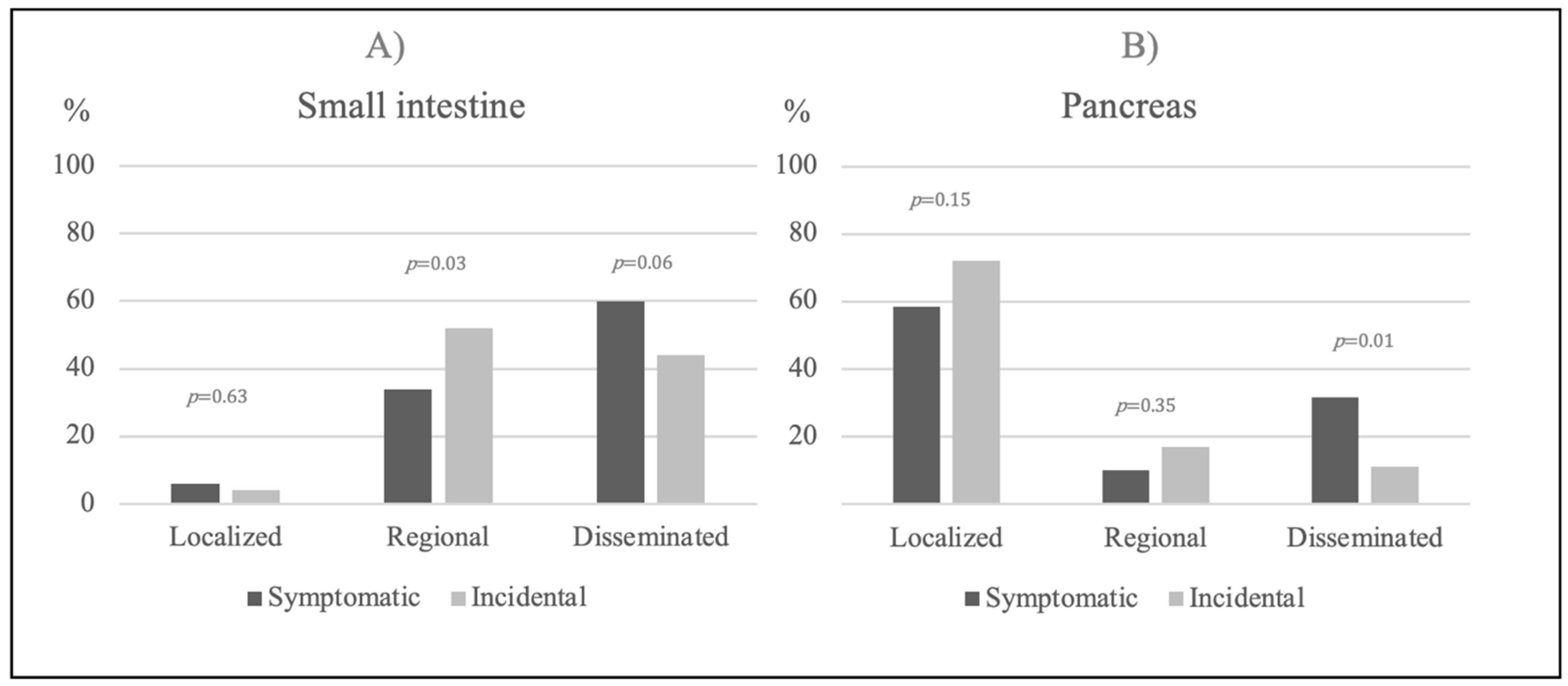
Symptomatic Disease vs. Incidental Findings
3.3. Pancreatic NETs
Symptomatic Disease vs. Incidental Findings
3.4. CT and MR Scans in Denmark
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, R.; Zheng-Pywell, R.; Chen, H.A.; Bibb, J.A.; Chen, H.; Rose, J.B. Management of Gastrointestinal Neuroendocrine Tumors. Clin. Med. Insights Endocrinol. Diabetes 2019, 12, 1179551419884058. [Google Scholar] [CrossRef] [PubMed]
- Klimstra, D.S.; Modlin, I.R.; Coppola, D.; Lloyd, R.V.; Suster, S. The Pathologic Classification of Neuroendocrine Tumors: A Review of Nomenclature, Grading, and Staging Systems. Pancreas 2010, 39, 707–712. [Google Scholar] [CrossRef]
- Klöppel, G. Neuroendocrine Neoplasms: Dichotomy, Origin and Classifications. Visc. Med. 2017, 33, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A. WHO Classification of Tumours Editorial Board The 2019 WHO Classification of Tumours of the Digestive System. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Booth, D.G.; Takagi, M.; Sanchez-Pulido, L.; Petfalski, E.; Vargiu, G.; Samejima, K.; Imamoto, N.; Ponting, C.P.; Tollervey, D.; Earnshaw, W.C.; et al. Ki-67 Is a PP1-Interacting Protein That Organises the Mitotic Chromosome Periphery. eLife 2014, 3. [Google Scholar] [CrossRef]
- Basuroy, R.; Bouvier, C.; Ramage, J.K.; Sissons, M.; Kent, A.; Srirajaskanthan, R. Presenting Symptoms and Delay in Diagnosis of Gastrointestinal and Pancreatic Neuroendocrine Tumours. Neuroendocrinology 2018, 107, 42–49. [Google Scholar] [CrossRef]
- Gade, A.K.; Olariu, E.; Douthit, N.T. Carcinoid Syndrome: A Review. Cureus 2020, 12, e7186. [Google Scholar] [CrossRef] [Green Version]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335. [Google Scholar] [CrossRef]
- Cetinkaya, R.B.; Aagnes, B.; Thiis-Evensen, E.; Tretli, S.; Bergestuen, D.S.; Hansen, S. Trends in Incidence of Neuroendocrine Neoplasms in Norway: A Report of 16,075 Cases from 1993 through 2010. Neuroendocrinology 2017, 104, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallet, J.; Law, C.H.L.; Cukier, M.; Saskin, R.; Liu, N.; Singh, S. Exploring the Rising Incidence of Neuroendocrine Tumors: A Population-Based Analysis of Epidemiology, Metastatic Presentation, and Outcomes. Cancer 2015, 121, 589–597. [Google Scholar] [CrossRef]
- Leoncini, E.; Boffetta, P.; Shafir, M.; Aleksovska, K.; Boccia, S.; Rindi, G. Increased Incidence Trend of Low-Grade and High-Grade Neuroendocrine Neoplasms. Endocrine 2017, 58, 368–379. [Google Scholar] [CrossRef] [Green Version]
- Das, S.; Dasari, A. Epidemiology, Incidence, and Prevalence of Neuroendocrine Neoplasms: Are There Global Differences? Curr. Oncol. Rep. 2021, 23, 43. [Google Scholar] [CrossRef]
- Sundin, A.; Arnold, R.; Baudin, E.; Cwikla, J.B.; Eriksson, B.; Fanti, S.; Fazio, N.; Giammarile, F.; Hicks, R.J.; Kjaer, A.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: Radiological, Nuclear Medicine & Hybrid Imaging. Neuroendocrinology 2017, 105, 212–244. [Google Scholar] [CrossRef]
- Partelli, S.; Cirocchi, R.; Crippa, S.; Cardinali, L.; Fendrich, V.; Bartsch, D.K.; Falconi, M. Systematic Review of Active Surveillance versus Surgical Management of Asymptomatic Small Non-Functioning Pancreatic Neuroendocrine Neoplasms. BJS Br. J. Surg. 2017, 104, 34–41. [Google Scholar] [CrossRef]
- Gaujoux, S.; Partelli, S.; Maire, F.; D’Onofrio, M.; Larroque, B.; Tamburrino, D.; Sauvanet, A.; Falconi, M.; Ruszniewski, P. Observational Study of Natural History of Small Sporadic Nonfunctioning Pancreatic Neuroendocrine Tumors. J. Clin. Endocrinol. Metab. 2013, 98, 4784–4789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, L.C.; Grant, C.S.; Salomao, D.R.; Fletcher, J.G.; Takahashi, N.; Fidler, J.L.; Levy, M.J.; Huebner, M. Small, Nonfunctioning, Asymptomatic Pancreatic Neuroendocrine Tumors (PNETs): Role for Nonoperative Management. Surgery 2012, 152, 965–974. [Google Scholar] [CrossRef]
- De Jong, M.; Valkema, R.; Jamar, F.; Kvols, L.K.; Kwekkeboom, D.J.; Breeman, W.A.P.; Bakker, W.H.; Smith, C.; Pauwels, S.; Krenning, E.P. Somatostatin Receptor-Targeted Radionuclide Therapy of Tumors: Preclinical and Clinical Findings. Semin. Nucl. Med. 2002, 32, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Menon, B.K.; Kalshetty, A.; Bhattacharjee, A.; Basu, S. Standardized Uptake Values and Ratios on 68Ga-DOTATATE PET-Computed Tomography for Normal Organs and Malignant Lesions and Their Correlation with Krenning Score in Patients with Metastatic Neuroendocrine Tumors. Nucl. Med. Commun. 2020, 41, 1095–1099. [Google Scholar] [CrossRef]
- Andreassen, M.; Ilett, E.; Wiese, D.; Slater, E.P.; Klose, M.; Hansen, C.P.; Gercke, N.; Langer, S.W.; Kjaer, A.; Maurer, E.; et al. Surgical Management, Preoperative Tumor Localization, and Histopathology of 80 Patients Operated on for Insulinoma. J. Clin. Endocrinol. Metab. 2019, 104, 6129–6138. [Google Scholar] [CrossRef] [PubMed]
- Børglum, T.; Rehfeld, J.F.; Drivsholm, L.B.; Hilsted, L. Processing-Independent Quantitation of Chromogranin A in Plasma from Patients with Neuroendocrine Tumors and Small-Cell Lung Carcinomas. Clin. Chem. 2007, 53, 438–446. [Google Scholar] [CrossRef] [Green Version]
- Johnbeck, C.B.; Knigge, U.; Loft, A.; Berthelsen, A.K.; Mortensen, J.; Oturai, P.; Langer, S.W.; Elema, D.R.; Kjaer, A. Head-to-Head Comparison of 64Cu-DOTATATE and 68Ga-DOTATOC PET/CT: A Prospective Study of 59 Patients with Neuroendocrine Tumors. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2017, 58, 451–457. [Google Scholar] [CrossRef] [Green Version]
- Boyar Cetinkaya, R.; Vatn, M.; Aabakken, L.; Bergestuen, D.S.; Thiis-Evensen, E. Survival and Prognostic Factors in Well-Differentiated Pancreatic Neuroendocrine Tumors. Scand. J. Gastroenterol. 2014, 49, 734–741. [Google Scholar] [CrossRef]
- Zerbi, A.; Falconi, M.; Rindi, G.; Fave, G.D.; Tomassetti, P.; Pasquali, C.; Capitanio, V.; Boninsegna, L.; Di Carlo, V. Clinicopathological Features of Pancreatic Endocrine Tumors: A Prospective Multicenter Study in Italy of 297 Sporadic Cases. Am. J. Gastroenterol. 2010, 105, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Pfeifer, A.; Knigge, U.; Binderup, T.; Mortensen, J.; Oturai, P.; Loft, A.; Berthelsen, A.K.; Langer, S.W.; Rasmussen, P.; Elema, D.; et al. 64 Cu-DOTATATE PET for Neuroendocrine Tumors: A Prospective Head-to-Head Comparison with 111 In-DTPA-Octreotide in 112 Patients. J. Nucl. Med. 2015, 56, 847–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lousberg, L.; Collignon, J.; Detry, O. Appendiceal Neuroendrocrine Neoplasms: Incidentaloma or Something We Should Worry About? Curr. Opin. Gastroenterol. 2020, 36, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Ebbehoj, A.; Stochholm, K.; Jacobsen, S.F.; Trolle, C.; Jepsen, P.; Robaczyk, M.G.; Rasmussen, Å.K.; Feldt-Rasmussen, U.; Thomsen, R.W.; Søndergaard, E.; et al. Incidence and Clinical Presentation of Pheochromocytoma and Sympathetic Paraganglioma: A Population-Based Study. J. Clin. Endocrinol. Metab. 2021, 106, e2251–e2261. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, M.; Decristoforo, C.; Kendler, D.; Dobrozemsky, G.; Heute, D.; Uprimny, C.; Kovacs, P.; Von Guggenberg, E.; Bale, R.; Virgolini, I.J. 68Ga-DOTA-Tyr3-Octreotide PET in Neuroendocrine Tumors: Comparison with Somatostatin Receptor Scintigraphy and CT. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2007, 48, 508–518. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Small Intestinal NET, Pre Referral | |||
| 2010–2011 | 2019–2020 | p-Value | |
| Number (n) of Cases | 70 | 101 | |
| Age | 65 ± 12 | 65 ± 12 | 0.99 |
| Female, n (%) | 36 (51) | 44 (44) | 0.31 |
| Incidence (per 100,000) | 1.39 | 1.84 | 0.05 |
| Age adjusted incidence (pr 100,000) | 1.39 | 1.76 | 0.30 |
| Incidental findings, n (%) | 19 (27) | 31 (31) | 0.62 |
| Incidental finding on imaging or endoscopy, n (%) | 12 (17) | 24 (24) | 0.30 |
| Incidental finding after surgery, n (%) | 7 (10) | 7 (7) | 0.47 |
| Symptoms leading to initial investigation | 51 (73) | 70 (70) | 0.62 |
| GI symptoms, n (%) | 28 (40) | 43 (43) | 0.74 |
| GI symptoms + flushing, n (%) | 5 (7) | 7 (7) | 0.96 |
| Flushing, n (%) | 2 (3) | 2 (2) | 0.71 |
| Unspecific symptoms, n (%) | 6 (9) | 5 (5) | 0.34 |
| Acute surgery for ileus, n (%) | 10 (14) | 13 (13) | 0.79 |
| Histologic diagnosis at time of referral to NET center (%) | 62 (89) | 81 (80) | 0.15 |
| Small Intestinal NET, Post Referral | |||
| Diagnosis based on | |||
| Histology, n (%) | 70 (100) | 97 (96) | 0.09 |
| Imaging, n (%) | 0 | 4 (4) | 0.09 |
| 68Ga-DOTATOC PET-CT/64Cu-DOTATATE PET-CT, n (%) | 0 | 99 (98) | <0.001 |
| 111In-octreotide scintigraphy, n (%) | 65 (93) | 0 (0) | <0.001 |
| Stage | 0.30 | ||
| Localized, n (%) | 2 (3) | 7 (7) | 0.24 |
| Regional, n (%) | 25 (36) | 42 (42) | 0.44 |
| Disseminated, n (%) | 42 (60) | 52 (51) | 0.27 |
| Unknown, n (%) | 1 (1) | 0 | - |
| Metastases above diaphragm, n (%) | 10 (14) | 22 (22) | 0.22 |
| Bone metastases, n (%) | 4 (6) | 11 (11) | 0.24 |
| Tumor size (cm) | 2.5 (1.5–3.5) | 1.9 (1.4–2.9) | 0.06 |
| p-CgA (before surgery) nm/L | 1485 (227–10,575) | 317 (140–1760) | 0.01 |
| Ki-67 index (tumor or metastasis), (%) | 4 (2–6) | 4 (2–7) | 0.13 |
| Pancreatic NET, Pre Referral | |||
| 2010–2011 | 2019–2020 | p-Value | |
| Number (n) of Cases | 21 | 75 | |
| Age | 64 ± 15 | 61 ± 13 | 0.50 |
| Female/male | 7/14 | 36/39 | 0.23 |
| Incidence (pr 100,000) | 0.42 | 1.39 | <0.001 |
| Age adjusted incidence (pr 100,000) | 0.42 | 1.34 | <0.001 |
| Incidental findings, n (%) | 4 (19) | 43 (57) | 0.002 |
| Incidental finding on imaging, n (%) | 4 (19) | 37 (49) | 0.01 |
| Incidental finding after surgery, n (%) | 0 | 6 (8) | 0.18 |
| Symptoms/reason leading to initial investigation | 17 | 32 | 0.002 |
| GI-symptoms, n (%) | 10 (48) | 9 (12) | <0.001 |
| Attack-like phenomena, n (%) | 3 (14) | 8 (11) | 0.66 |
| Unspecific symptoms, n (%) | 4 (19) | 11 (15) | 0.63 |
| MEN1 follow up, n (%) | 0 | 4 (5) | 0.28 |
| Histologic diagnosis at time of referral to NET center (%) | 13 (62) | 28 (37) | 0.04 |
| Pancreatic NET, Post Referral | |||
| Type of tumor | |||
| Non-functioning, n (%) | 14 (67) | 65 (87) | 0.03 |
| Functioning, n (%) | 7 (33) | 10 (13) | 0.03 |
| Diagnosis based on | |||
| Histology, n (%) | 20 (95) | 47 (63) | 0.004 |
| Imaging, n (%) | 1 (5) | 28 (37) | 0.004 |
| 68Ga-DOTATOC PET-CT/64Cu-DOTATATE PET-CT, n (%) | 0 | 68 (91) | <0.001 |
| 111In-octreotide scintigraphy, n (%) | 18 (86) | 0 (0) | <0.001 |
| Stage | 0.03 | ||
| Localized, n (%) | 10 (48) | 52 (69) | 0.11 |
| Regional, n (%) | 2 (10) | 11 (15) | 0.59 |
| Disseminated, n (%) | 8 (38) | 12 (16) | 0.02 |
| Unknown, n (%) | 1 (4) | - | - |
| Metastases above diaphragm, n (%) | 3 (14) | 6 (8) | 0.64 |
| Bone metastases, n (%) | 0 | 4 (5) | 0.18 |
| Tumor size (cm) | 2.5 (1.8–8.3) | 1.6 (1–2.6) | 0.03 |
| p-CgA (before surgery) nm/L | 259 (83–1590) | 92 (68–170) | 0.02 |
| Ki-67 Index (tumor or metastasis), % | 5 (2–8) | 4 (2–9) | 0.56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stensbøl, A.B.; Krogh, J.; Holmager, P.; Klose, M.; Oturai, P.; Kjaer, A.; Hansen, C.P.; Federspiel, B.; Langer, S.W.; Knigge, U.; et al. Incidence, Clinical Presentation and Trends in Indication for Diagnostic Work-Up of Small Intestinal and Pancreatic Neuroendocrine Tumors. Diagnostics 2021, 11, 2030. https://doi.org/10.3390/diagnostics11112030
Stensbøl AB, Krogh J, Holmager P, Klose M, Oturai P, Kjaer A, Hansen CP, Federspiel B, Langer SW, Knigge U, et al. Incidence, Clinical Presentation and Trends in Indication for Diagnostic Work-Up of Small Intestinal and Pancreatic Neuroendocrine Tumors. Diagnostics. 2021; 11(11):2030. https://doi.org/10.3390/diagnostics11112030
Chicago/Turabian StyleStensbøl, Anna Bryan, Jesper Krogh, Pernille Holmager, Marianne Klose, Peter Oturai, Andreas Kjaer, Carsten Palnæs Hansen, Birgitte Federspiel, Seppo W. Langer, Ulrich Knigge, and et al. 2021. "Incidence, Clinical Presentation and Trends in Indication for Diagnostic Work-Up of Small Intestinal and Pancreatic Neuroendocrine Tumors" Diagnostics 11, no. 11: 2030. https://doi.org/10.3390/diagnostics11112030