
Concomitant Talocalcaneal Coalition as a Risk Factor for Early Relapse Following Ponseti Treatment of Idiopathic Clubfoot



Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
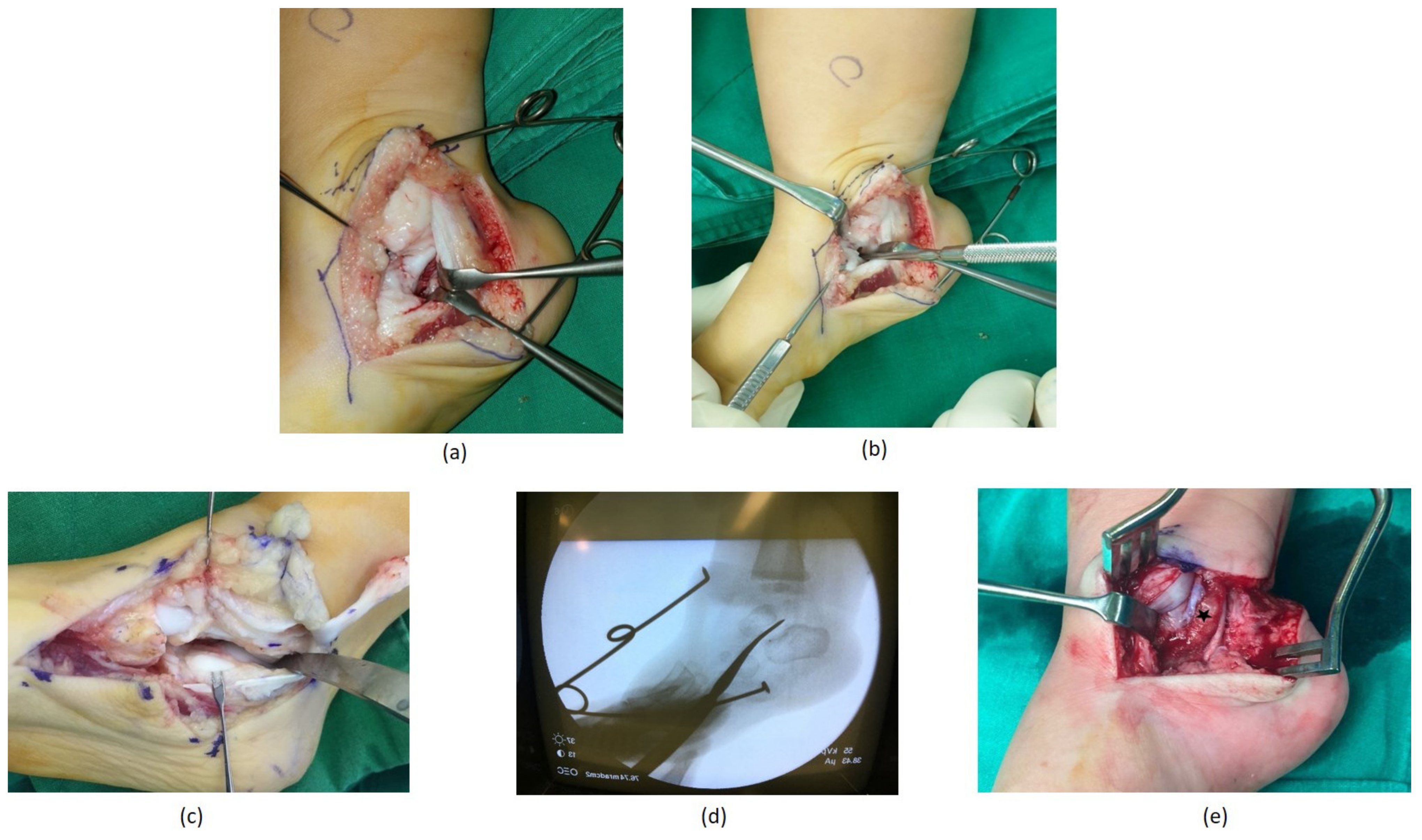
2.2. Surgical Technique
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ponseti, I.V. Treatment of Congenital Club Foot. J. Bone Joint Surg. Am. 1992, 74, 448–454. [Google Scholar] [CrossRef]
- Agarwal, A.; Rastogi, A.; Rastogi, P. Relapses in Clubfoot Treated with Ponseti Technique and Standard Bracing Protocol- A Systematic Analysis. J. Clin. Orthop. Trauma 2021, 18, 199–204. [Google Scholar] [CrossRef]
- Ponseti, I.V. Relapsing Clubfoot: Causes, Prevention, and Treatment. Iowa Orthop. J. 2002, 22, 55–56. [Google Scholar] [CrossRef]
- Ezra, E.; Hayek, S.; Gilai, A.N.; Khermosh, O.; Wientroub, S. Tibialis Anterior Tendon Transfer for Residual Dynamic Supination Deformity in Treated Club Feet. J. Pediatr. Orthop. Part B 2000, 9, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.H.; Hoyen, H.A.; Barthel, T. Tibialis Anterior Tendon Transfer after Clubfoot Surgery. Clin. Orthop. Relat. Res. 2009, 467, 1306–1313. [Google Scholar] [CrossRef] [Green Version]
- Moon, D.K.; Gurnett, C.A.; Aferol, H.; Siegel, M.J.; Commean, P.K.; Dobbs, M.B. Soft-Tissue Abnormalities Associated with Treatment-Resistant and Treatment-Responsive Clubfoot. J. Bone Jt. Surg. 2014, 96, 1249–1256. [Google Scholar] [CrossRef] [PubMed]
- Morcuende, J.A.; Dolan, L.A.; Dietz, F.R.; Ponseti, I.V. Radical Reduction in the Rate of Extensive Corrective Surgery for Clubfoot Using the Ponseti Method. Pediatrics 2004, 113, 376–380. [Google Scholar] [CrossRef]
- Eidelman, M.; Kotlarsky, P.; Herzenberg, J.E. Treatment of Relapsed, Residual and Neglected Clubfoot: Adjunctive Surgery. J. Child. Orthop. 2019, 13, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Stouten, J.H.; Besselaar, A.T.; Van Der Steen, M.C. Identification and Treatment of Residual and Relapsed Idiopathic Clubfoot in 88 Children. Acta Orthop. 2018, 89, 448–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhaskar, A.; Patni, P. Classification of Relapse Pattern in Clubfoot Treated with Ponseti Technique. Indian J. Orthop. 2013, 47, 370–376. [Google Scholar] [CrossRef]
- Mahan, S.T.; Spencer, S.A.; May, C.J.; Prete, V.I.; Kasser, J.R. Clubfoot Relapse: Does Presentation Differ Based on Age at Initial Relapse? J. Child. Orthop. 2017, 11, 367–372. [Google Scholar] [CrossRef] [PubMed]
- van Praag, V.M.; Lysenko, M.; Harvey, B.; Yankanah, R.; Wright, J.G. Casting Is Effective for Recurrence Following Ponseti Treatment of Clubfoot. J. Bone Jt. Surg. 2018, 100, 1001–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovell, M.E.; Morcuende, J.A. Neuromuscular Disease as the Cause of Late Clubfoot Relapses: Report of 4 Cases. Iowa Orthop. J. 2007, 27, 82–84. [Google Scholar]
- Radler, C.; Mindler, G.T. Treatment of Severe Recurrent Clubfoot. Foot Ankle Clin. 2015, 20, 563–586. [Google Scholar] [CrossRef] [PubMed]
- Callahan, R.A. Talipes Equinovarus Associated with an Absent Posterior Tibial Tendon and a Tarsal Coalition: A Case Report. Clin. Orthop. Relat. Res. 1980, 146, 231–233. [Google Scholar] [CrossRef]
- Seetharama Rao, B.; Joseph, B. Varus and Equinovarus Deformities of the Foot Associated with Tarsal Coalition. Foot 1994, 4, 95–99. [Google Scholar] [CrossRef]
- Spero, C.R.; Simon, G.S.; Tornetta, P. Clubfeet and Tarsal Coalition. J. Pediatr. Orthop. 1994, 14, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Van Rysselberghe, N.L.; Souder, C.D.; Mubarak, S.J. Unsuspected Tarsal Coalitions in Equinus and Varus Foot Deformities. J. Pediatr. Orthop. Part B 2020, 29, 370–374. [Google Scholar] [CrossRef]
- Staheli, L. Clubfoot: Ponseti Management, 3rd ed.; Global HELP Organization: Seattle, WA, USA, 2009; ISBN 978-1-60189-002-3. [Google Scholar]
- Morrisey, T. Surgical correction of clubfoot. In Atlas of Pediatric Orthopedics; Lippincott-Raven: Philadelphia, PA, USA, 1996; pp. 669–693. [Google Scholar]
- Azar, F.M.; Beaty, J.H. Campbell’s Operative Orthopaedics, 14th ed.; Daugherty, K., Jones, L., Eds.; Elsevier Inc.: Philadelphia, PA, USA, 2021; ISBN 9780323672184. [Google Scholar]
- Bor, N.; Coplan, J.A.; Herzenberg, J.E. Ponseti Treatment for Idiopathic Clubfoot: Minimum 5-Year Followup. Clin. Orthop. Relat. Res. 2009, 467, 1263–1270. [Google Scholar] [CrossRef] [Green Version]
- Bhatiwal, S.K.; Chopra, B.L.; Khajotia, B.L.; Chauhan, S. Idiopathic Clubfoot Treated by Ponseti Method: A Series of 300 Cases. Int. J. Res. Orthop. 2018, 4, 954. [Google Scholar] [CrossRef]
- Hallaj-Moghaddam, M.; Moradi, A.; Ebrahimzadeh, M.H.; Habibzadeh Shojaie, S.R. Ponseti Casting for Severe Club Foot Deformity: Are Clinical Outcomes Promising? Adv. Orthop. 2015, 2015, 821690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, S.L.; Lavy, C.B.D. Correlation of Clinical and Ultrasonographic Findings after Achilles Tenotomy in Idiopathic Club Foot. J. Bone Jt. Surg. Ser. B 2006, 88, 377–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Sex | Affected Foot | Initial Number of Casts Including Final Cast after Tenotomy | Earliest Signs of Relapse | Time to Relapse (in Weeks) | Affected Subtalar Facet | Age at Coalition Resection (in Months) | Follow-Up Duration (in Months) |
|---|---|---|---|---|---|---|---|---|
| 1 | F | Right | 5 | forefoot pronation, cavus, equinus | 3 | posterior | 4 | 173 |
| 2 | M | Right | 6 | cavus, equinus, forefoot adduction | 7 | anterior | 27 | 133 |
| Left | 6 | cavus, equinus | 7 | anterior | 27 | 133 | ||
| 3 | M | Left | 5 | cavus, equinus | 8 | posterior | 41 | 34 |
| 4 | F | Right | 7 | cavus, equinus, forefoot adduction | 8 | middle and posterior | 17 | 38 |
| Left | 7 | cavus, equinus, forefoot adduction | 8 | middle and posterior | 17 | 38 | ||
| 5 | M | Left | 6 | cavus, equinus | 7 | middle | 12 | 22 |
| 6 | M | Right | 6 | cavus, equinus | 7 | middle | 14 | 14 |
| Left | 6 | cavus, equinus | 7 | middle and posterior | 14 | 14 | ||
| 7 | M | Right | 6 | cavus, equinus, forefoot adduction | 8 | posterior | 16 | 8 |
| Left | 6 | cavus, equinus, forefoot adduction | 8 | posterior | 16 | 8 | ||
| 8 | M | Right | 6 | cavus, equinus | 7 | anterior, middle, and posterior | 12 | 6 |
| Patient Number | Affected Foot | Preoperative Anteroposterior Talocalcaneal Angle (°) | Preoperative Lateral Talocalcaneal Angle (°) | Anteroposterior Talocalcaneal Angle at Final Follow-Up (°) | Lateral Talocalcaneal Angle at Final Follow-Up (°) |
|---|---|---|---|---|---|
| 1 | Right | 20.8 | 22.2 | 30.4 | 37.2 |
| 2 | Right | 24.2 | 26.9 | 30.5 | 26.9 |
| Left | 26.1 | 27.0 | 31.4 | 27.6 | |
| 3 | Left | 27.0 | 1.0 | 32.9 | 27.6 |
| 4 | Right | 8.7 | 17.8 | 30.8 | 32.8 |
| Left | 22.1 | 24.8 | 31.7 | 26.8 | |
| 5 | Left | 15.9 | 18.7 | 30.9 | 26.5 |
| 6 | Right | 28.8 | 23.4 | 31.9 | 25.8 |
| Left | 25.8 | 34.1 | 32.5 | 25.4 | |
| 7 | Right | 20.2 | 29.3 | 34.4 | 33.9 |
| Left | 16.8 | 38.4 | 33.4 | 39.1 | |
| 8 | Right | 32.4 | 30.8 | 33.9 | 38.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shah, M.; Rhee, I.; Lee, S.K.; Alhassan, M.S.; Kim, H.W. Concomitant Talocalcaneal Coalition as a Risk Factor for Early Relapse Following Ponseti Treatment of Idiopathic Clubfoot. Diagnostics 2021, 11, 1682. https://doi.org/10.3390/diagnostics11091682
Shah M, Rhee I, Lee SK, Alhassan MS, Kim HW. Concomitant Talocalcaneal Coalition as a Risk Factor for Early Relapse Following Ponseti Treatment of Idiopathic Clubfoot. Diagnostics. 2021; 11(9):1682. https://doi.org/10.3390/diagnostics11091682
Chicago/Turabian StyleShah, Mudit, Isaac Rhee, Seung Kyu Lee, Mohammed Salman Alhassan, and Hyun Woo Kim. 2021. "Concomitant Talocalcaneal Coalition as a Risk Factor for Early Relapse Following Ponseti Treatment of Idiopathic Clubfoot" Diagnostics 11, no. 9: 1682. https://doi.org/10.3390/diagnostics11091682