1. Introduction
Renal resection on terms of either radical or partial nephrectomy is a well-established local cure for the management of stage T1a and T1b RCC [
1,
2,
3,
4,
5,
6,
7,
8]. However, the advancement and the effective application of percutaneous ablation techniques in overall cancer care render them an efficient alternative and an attractive solution in the treatment of RCC. Percutaneous ablation is a nephron-sparing technique with similar metastasis-free survival and cancer-specific survival rates when compared to partial nephrectomy, with additional benefits of a shorter hospitalization and recovery time [
9]. Alam et al. has reported that throughout a 7 years follow-up period, percutaneous ablation, radical or partial nephrectomy resulted in almost a 100% cancer-specific survival rate without any difference between the three treatment arms [
10]. International guidelines advocate application of percutaneous ablation for RCC as an alternative therapeutic option for the management of localized masses with a diameter ≤3 cm, when complete ablation is technically feasible, for selected and counseled patients [
4,
5,
6,
7,
8,
9,
11]. Although there is an extensive and thorough literature regarding the application of radiofrequency ablation (RFA) and cryoablation (CA) in renal tumors, the respective literature for MWA remains limited. When compared to RFA, MWA is less affected by the heat-sink effect, rendering the technique (at least in theory) ideal for the hypervascular renal tumors [
12,
13,
14]. In theory, the high perfusion (4 times that of the liver) and potential heat dissipation of the kidney may alter the bio-heat equation, requiring a less sensitive to heat-sink effect treatment method for ablation.
The purpose of the present study is to evaluate the safety and efficacy of computed tomography-guided percutaneous microwave ablation (MWA) of renal cell carcinoma (RCC), along with identifying prognostic factors affecting the progression survival rate.
3. Results
Patient and lesion demographics are reported in
Table 1 and
Table 2. Tumor stage was T1a (82.6%) or T1b (17.4%), (
Table 1). The mean size of the lesions was 3 ± 1.3 cm, with maximum tumor size ranged from 1 to 6 cm. The mean follow up time was 35.6 months (SD = 21.1).
All procedures were performed under local anesthesia and conscious sedation and were well tolerated by all the patients. On a per lesion basis, as far as T1a RCCs were concerned, tumor remnants were noticed at one month follow up in three patients (3/57) (primary technical success 94.7%); all three patients were re-treated with an ablation session and no tumor remnant was depicted in the subsequent imaging follow-up (secondary technical success 100%). As far as T1b RCCs were concerned, tumor remnants were noticed at the one month follow up in four patients (4/12) patients (primary technical success 66.7%): 2/4 patients were re-treated with ablation combined with trans-arterial embolization, one patient was re-treated with ablation only and one patient refused any further treatment. Tumor recurrence was noted in 2/69 T1a clear cell RCC patients (2.9%) at one year of follow-up; both patients underwent a second ablation. A metastatic lesion was depicted in 2/69 (2.9%) patients, with T1a (clear cell RCC-metastatic lesion to the sacral bone was depicted 12 months post therapy and treated with ablation combined with sacroplasty) and T1b tumors (lesion was encountered in iliac bone 5 months post therapy and treated with ablation), respectively. Grade I self-limited complications included limited perinephric haematomas (n = 4) and small urinoma (n = 1) requiring nothing but observation; these complications were recorded in 5/69 (7.2%) patients (4/5 with T1a and 1/5 with T1b RCCs). Although evaluation of renal function was not included in the objectives of the study, all laboratory work-up (including urea and creatinine values) prior to contrast enhanced axial imaging during the follow-up period showed a lack of significant changes and deterioration.
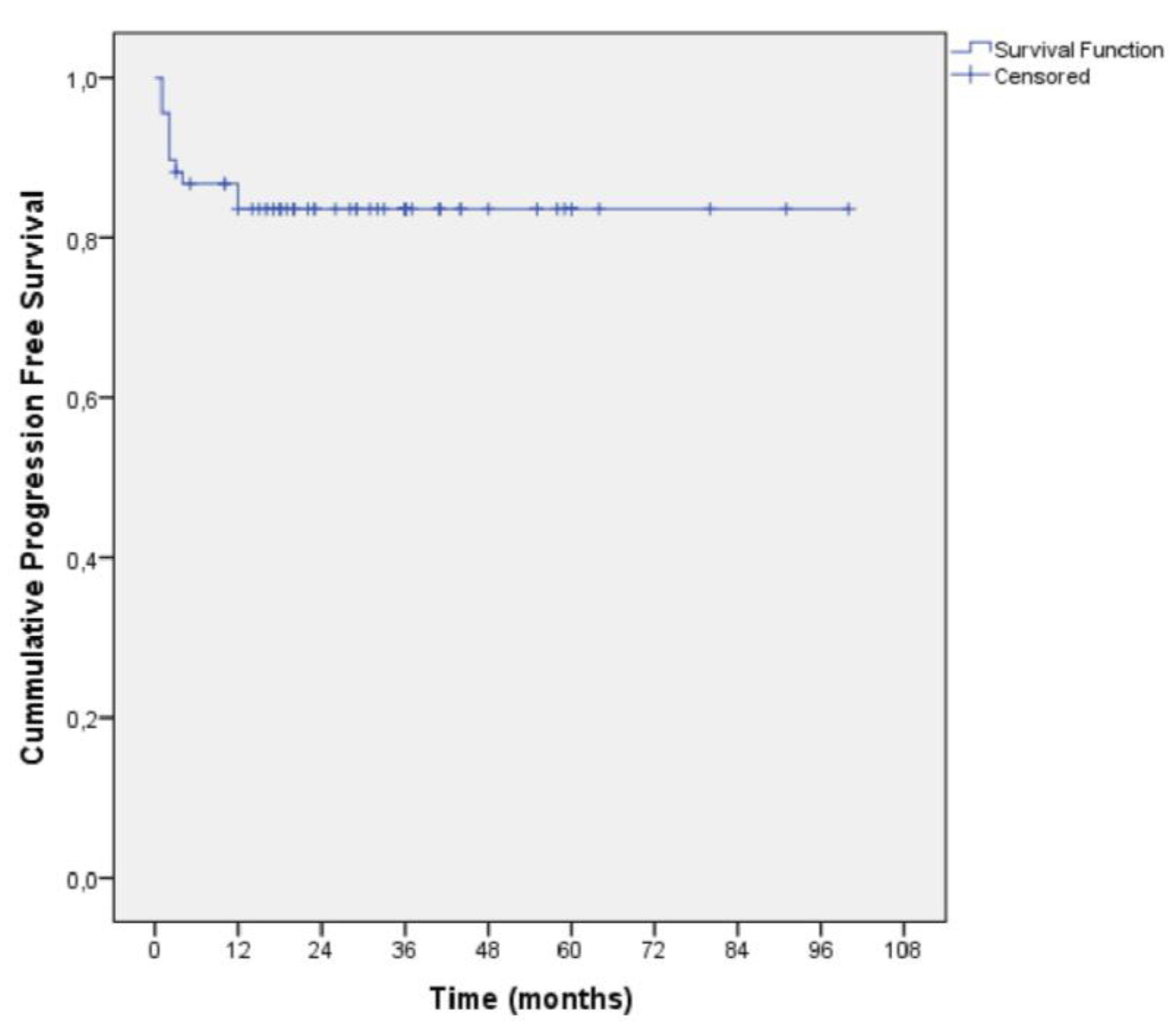
Mean survival time in the total sample was 35.6 months (SD = 21.1 months) whilst the median survival time was 33 months (interquartile range: 18–49 months) (
Figure 1). The recurrence free survival rate for T1a RCC was 94.7% (post secondary clinical success) and 90% (post primary clinical success). The mean progression free survival time from last ablation was 84.2 months (SE = 4.4 months). For T1a tumors, the cumulative progression free survival rate for 1, 6, 12 and 36 months were 100% (SE = 0%), 91.2% (SE = 3.7%), 91.2% (SE = 3.7%) and 87.5% (SE = 4.4%). For T1b tumors, the cumulative progression free rate for 1, 6, 12 and 36 months were 100% (SE = 0%), 63.6% (SE = 14.5%), 63.6% (SE = 14.5%) and 63.6% (SE = 14.5%).
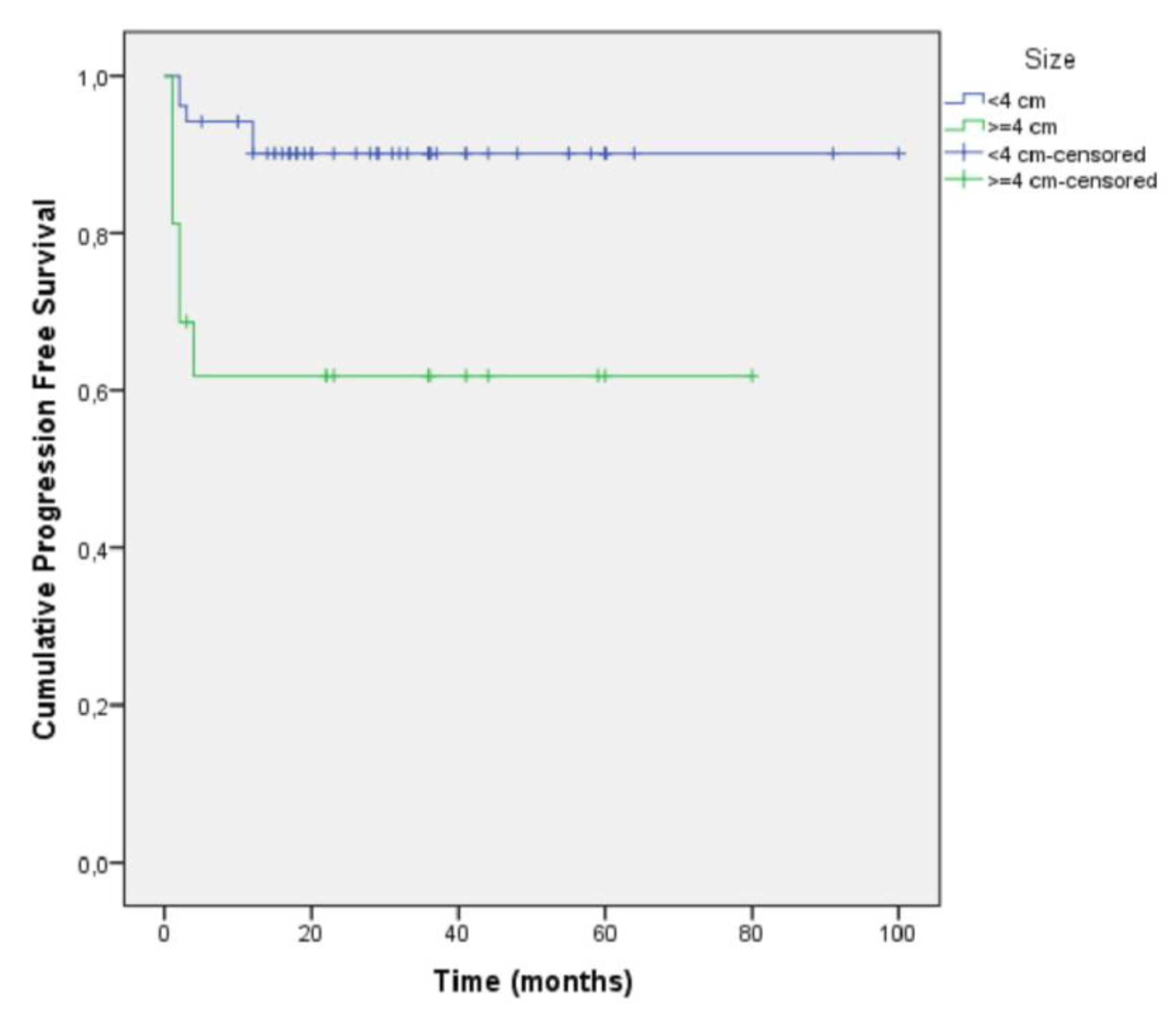
Patients of the T1b stage had a 3.72 times greater hazard for progression compared to patients of the T1a stage (
Figure 2,
Table 3).
Multivariate analysis showed that sex (
p = 0.894), age (
p = 0.376), side (
p = 0.674), complication during ablation (
p = 0.705) and having a second ablation (
p = 0.670) were not associated with the progression free survival rate (
Table 4).
Additionally, our univariate and multivariate analysis for T1a tumors, separated in two subgroups: those with a diameter less than 3 cm and those with a diameter greater than 3 cm, showed that there was no statistically important difference regarding tumor progression between those groups (
Table 5 and
Table 6).
4. Discussion
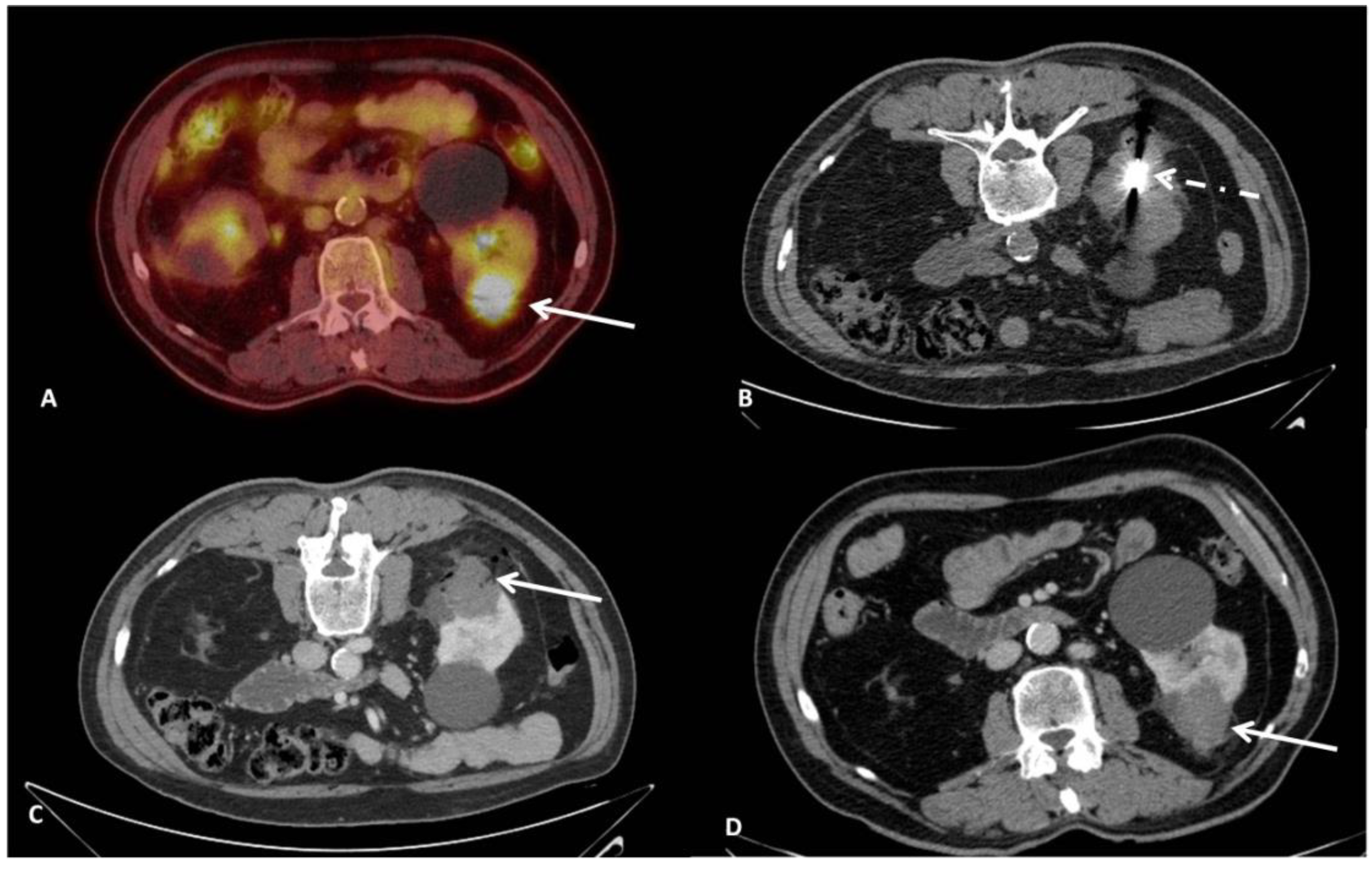
Although there is an extended literature regarding mid- and long-term outcomes of RFA and CA for RCCs, MWA has been less studied and there is still a lack of data concerning long term efficacy. The present study adds to the growing number of case series showing that CT-guided percutaneous microwave ablation (
Figure 3) is an efficacious and safe technique in terms of achieving local tumor control and recurrence-free response on both a per lesion and per patient basis [
20,
21,
22,
23,
24,
25,
26,
27,
28,
29,
30,
31,
32,
33,
34,
35,
36].
The results of the current study showed efficient progression free (100%, 86.7%, 86.7% and 83.5% for 1, 6, 12 and 36 months, respectively), recurrence free (94.7%) and overall survival rates (mean 35.6 months), in a follow up time of 36 months. Hao et al. treated 162 patients with ultrasound guided MWA for T1a RCCs; the median follow-up time was 45.5 months and the overall occurrence of local tumor progression was 3.0% [
33]. Survival rates at 1, 3 and 5 years were 98.7%, 89.5% and 82.1%, respectively [
33]. Similar outcomes have been reported by Guo et al., who performed CT guided microwave ablation for T1a renal tumors in 106 patients [
28]. At the first follow-up imaging study, complete response was achieved in 101 (95.3%) patients and partial response was achieved in 5 (4.7%) patients; the 1-, 2-, and 3-year local progression-free survival rates were 100.0%, 92.8% and 90.6%, respectively and 3-year overall survival were 99.0%, 97.7%, and 94.6%, respectively [
28]. Several authors have demonstrated consistent outcomes to our study (
Table 7).
Similar to other studies, in the present case series the treatment of RCC lesions with microwave ablation was successful and well tolerated; one major difference of the present study is that all patients were treated under local anesthesia combined with intravenous analgesia; however, this resulted in no significant differences concerning the efficacy and safety rates [
21,
22,
23,
24,
25,
26,
27,
28,
29,
30,
34,
35]. Furthermore, in tumors with a close proximity to renal pelvis/ureter, a ureteral stent was placed. Overall success rates as well as complication rates were comparable to that of other MWA (
Table 6), RFA and CA studies [
37,
38,
39,
40,
41,
42,
43]. In a recent propensity-matched analysis comparing percutaneous MWA versus laparoscopic PN for the treatment of T1a RCC, authors reported no significant differences between the two treatment arms regarding oncologic outcomes and complications [
44]. In terms of minimizing invasiveness and bleeding complications, robotic partial nephrectomy has also emerged as a safe and effective surgical approach for renal tumors; until now however, there have not been prospective comparative studies against percutaneous therapies [
45].
There seems to be a relation between size and local tumor control (tumor size is generally considered a survival prognostic indicator after percutaneous ablation). Several findings in the present study were noteworthy; there was no statistically significant difference regarding tumor progression/recurrence when comparing T1a tumors with a diameter <3 cm to those with a diameter between 3–4 cm (i.e., progression free survival rate was comparable among all T1a RCC patients). The results of the present study indicate that microwave ablation seems to be an efficacious technique for T1a RCC lesions, even for those at the higher (3–4 cm) size of the subgroup without any compromises upon safety. Although international guidelines advocate application of thermal ablation as an alternative option for the management of localized renal cancer <3 cm in size, the present study indicated that microwave ablation in T1a RCC patients with lesions ≥3 cm resulted in comparable overall survival and progression free survival rates to those with a tumor size <3 cm. The results of the present study can provide evidence to expand the indications of microwave ablation in treating T1a RCC in terms of tumor size.
On the other hand, LCT of MWA for T1b lesions was moderate (for 1, 6, 12 and 36 months were 100%, 63.6%, 63.6% and 63.6%, respectively), adding to the growing number of publications pointing out that either multi antennae approaches or combined therapies with trans-arterial embolization could be necessary for higher success rates [
46,
47,
48]. Potentially, cryoablation with all its advantages including multi-probe placement, ice ball visibility and ability for ice sculpting could serve as an attractive alternative for T1b RCC lesions [
49].
Current guidelines remain skeptical regarding the use of thermal ablation techniques in renal tumors with size greater than 3 cm and in T1b renal tumors, due to the increased rates of recurrence. A large Dutch series retrospectively studied the primary and secondary efficacy of percutaneous microwave ablation of histologically proven T1 renal cell carcinomas and proved that primary efficacy was significantly lower for T1b lesions (52%) compared to T1a lesions (89%). Secondary efficacy rates were not statistically different (99% and 95%, respectively) [
27]. Moreover, in the study of Yu et al., the size of the tumor (>4 cm) was statistically significant for tumor progression; the technical success rate was lower in larger tumors, without this difference being statistically significant [
35]. On the contrary, Shakeri et al. showed that size (>4 cm) had a significant impact on the technical success (
p = 0.039), regardless of the location of the tumor; the size was not statistically associated with complications, progression and survival rates [
26]. Hao et al. reported that although the progression free rate was lower for tumors sizing 3–4 cm in comparison to greater sizes, this difference was not proven to be statistically significant [
33]. The same authors reported that recurrence rates did not affect the overall survival rates after adequate repetitive treatment [
33]. The mean size in the current study was one of the greatest in the available literature. In our analysis only T1b tumors (>4 cm) were significantly associated with increased risk for progression, whereas no significant difference was observed between the subgroups of T1a tumors. Tumor size did not seem to affect the overall survival rates and it was not associated with the complication rate.
Recent trials comparing MWA, RFA and cryoablation have demonstrated significantly decreased procedure times in favor of MWA with similar complication rates and renal function changes post-procedure [
50,
51]. Similarly, De Cobelli et al. [
43] compared percutaneous MWA and cryoablation for T1a RCC and showed comparable safety and efficacy between the two modalities. In cryoablation, the use of multiple probes and the ablation protocol (with a alternating freeze-thawing cycles) itself prolongs the procedural time; moreover, an additional advantage of the MWA is the reduced cost over cryoablation [
51]. All procedures in the present study were performed under local anesthesia and were well tolerated. In current literature, there is a lack of studies comparing intraprocedural pain between different thermal techniques in renal tumors. However, studies in liver and lung tumors showed that MWA is less painful compared to RFA [
52,
53,
54,
55].
The limitations of the present study include its retrospective nature and the small number of patients with larger (T1b) tumors. Biopsy results in terms of the Fuhrman grading and histologic subtype were not taken in account. Additional limitations include a lack of comparisons to RFA, CWA or surgery.
In summary, the results of the present study show that CT guided percutaneous MWA is an effective technique for treatment of T1a renal cell carcinomas, irrespective of tumor size at this stage. T1b tumors were associated with higher progression rates, therefore a size >4 cm seems to be a significant factor affecting efficacy. Large randomized controlled studies are warranted to observe treatment effectiveness and compare the results with those of other treatment options.


 ,
, 



{kind=link}
{kind=link}
{kind=link}