
Non-Lead Protective Aprons for the Protection of Interventional Radiology Physicians from Radiation Exposure in Clinical Settings: An Initial Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
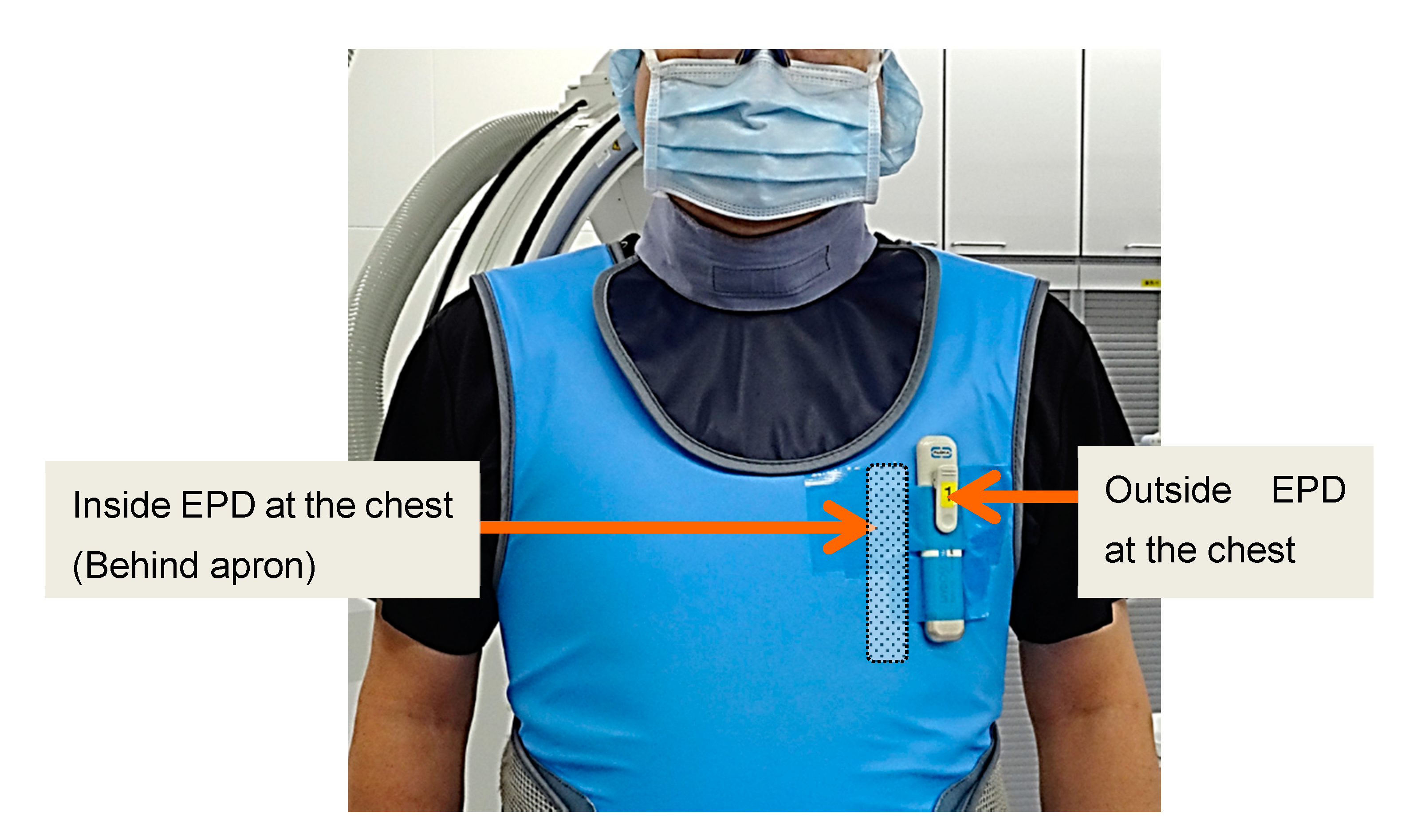
2.1. Protective Apron and Radiation Measurement
2.2. Cardiac Catheterization
3. Results
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Nemoto, M.; Chida, K. Reducing the breast cancer risk and radiation dose of radiography for scoliosis in children: A phantom study. Diagnostics 2020, 10, 753. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Radiological Protection (ICRP). Radiological Protection and Safety in Medicine; ICRP Publication 73; Pergamon: Oxford, UK, 1996; Volume 26, Available online: https://journals.sagepub.com/doi/pdf/10.1177/ANIB_26_2 (accessed on 28 August 2021).
- Vano, E. Challenges for managing the cumulative effective dose for patients. Br. J. Radiol. 2020, 93, 20200814. [Google Scholar] [CrossRef]
- International Commission on Radiological Protection (ICRP). Diagnostic Reference Levels in Medical Imaging; ICRP Publication 135; Sage: Thousand Oaks, CA, USA, 2017; Volume 46, Available online: https://journals.sagepub.com/doi/pdf/10.1177/ANIB_46_1 (accessed on 28 August 2021).
- Morishima, Y.; Chida, K.; Watanabe, H. Estimation of the dose of radiation received by patient and physician during a videofluoroscopic swallowing study. Dysphagia 2016, 31, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Haga, Y.; Chida, K.; Sota, M.; Kaga, Y.; Abe, M.; Inaba, Y.; Suzuki, M.; Meguro, T.; Zuguchi, M. Hybrid operating room system for the treatment of thoracic and abdominal aortic aneurysms: Evaluation of the radiation dose received by patients. Diagnostics 2020, 10, 846. [Google Scholar] [CrossRef] [PubMed]
- Chida, K.; Kato, M.; Kagaya, Y.; Zuguchi, M.; Saito, H.; Ishibashi, T.; Takahashi, S.; Yamada, S.; Takai, Y. Radiation dose and radiation protection for patients and physicians during interventional procedure. J. Radiat. Res. 2010, 51, 97–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chida, K.; Inaba, Y.; Masuyama, H.; Yanagawa, I.; Mori, I.; Saito, H.; Maruoka, S.; Zuguchi, M. Evaluating the performance of a MOSFET dosimeter at diagnostic X-ray energies for interventional radiology. Radiol. Phys. Technol. 2009, 2, 58–61. [Google Scholar] [CrossRef]
- Inaba, Y.; Chida, K.; Murabayashi, Y.; Endo, M.; Otomo, K.; Zuguchi, M. An initial investigation of a wireless patient radiation dosimeter for use in interventional radiology. Radiol. Phys. Technol. 2020, 13, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Chida, K.; Kato, M.; Inaba, Y.; Kobayashi, R.; Nakamura, M.; Abe, Y.; Zuguchi, M. Real-time patient radiation dosimeter for use in interventional radiology. Phys. Medica 2016, 32, 1475–1478. [Google Scholar] [CrossRef]
- Chida, K.; Saito, H.; Zuguchi, M.; Shirotori, K.; Kumagai, S.; Nakayama, H.; Matsubara, K.; Kohzuki, M. Does digital acquisition reduce patients’ skin dose in cardiac interventional procedures? An experimental study. Am. J. Roentgenol. 2004, 183, 1111–1114. [Google Scholar] [CrossRef]
- International Commission on Radiological Protection (ICRP). Radiological Protection in Medicine; ICRP Publication 105; Elsevier: Amsterdam, The Netherlands, 2007; Volume 37, Available online: https://journals.sagepub.com/doi/pdf/10.1177/ANIB_37_6 (accessed on 28 August 2021).
- Chida, K.; Saito, H.; Otani, H.; Kohzuki, M.; Takahashi, S.; Yamada, S.; Shirato, K.; Zuguchi, M. Relationship between fluoroscopic time, dose—Area product, body weight, and maximum radiation skin dose in cardiac interventional procedures. Am. J. Roentgenol. 2006, 186, 774–778. [Google Scholar] [CrossRef]
- Chida, K.; Kagaya, Y.; Saito, H.; Takai, Y.; Takahashi, S.; Yamada, S.; Kohzuki, M.; Zuguchi, M. Total entrance skin dose: An effective indicator of maximum radiation dose to the skin during percutaneous coronary intervention. Am. J. Roentgenol. 2007, 189, W224–W227. [Google Scholar] [CrossRef]
- International Commission on Radiological Protection (ICRP). ICRP Statement on Tissue Reactions / Early and Late Effects of Radiation in Normal Tissues and Organs—Threshold Doses for Tissue Reactions in a Radiation Protection Context; ICRP Publication 118; Elsevier: Amsterdam, The Netherlands, 2012; Volume 41, Available online: https://journals.sagepub.com/doi/pdf/10.1177/ANIB_41_1-2 (accessed on 28 August 2021).
- Chida, K.; Kaga, Y.; Haga, Y.; Kataoka, N.; Kumasaka, E.; Meguro, T.; Zuguchi, M. Occupational dose in interventional radiology procedures. Am. J. Roentgenol. 2013, 200, 138–141. [Google Scholar] [CrossRef]
- Attigah, N.; Oikonomou, K.; Hinz, U.; Knoch, T.; Demirel, S.; Verhoeven, E.; Böckler, D. Radiation exposure to eye lens and operator hands during endovascular procedures in hybrid operating rooms. J. Vasc. Surg. 2016, 63, 198–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haga, Y.; Chida, K.; Kaga, Y.; Sota, M.; Meguro, T.; Zuguchi, M. Occupational eye dose in interventional cardiology procedures. Sci. Rep. 2017, 7, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Presidência da República. Casa Civil. Subchefia para Assuntos Jurídicos. Decreto—Lei nº 227, De 28 de Fevereiro de 1967. Dá Nova Redação ao Decreto-lei nº 1.985, de 29 de Janeiro de 1940 (Código de Minas). 1967. Available online: http://www.planalto.gov.br/ccivil_03/Decreto-Lei/Del0227.htm (accessed on 19 October 2020).
- Ishii, H.; Chida, K.; Satsurai, K.; Haga, Y.; Kaga, Y.; Abe, M.; Inaba, Y.; Zuguchi, M. A phantom study to determine the optimal placement of eye dosemeters on interventional cardiology staff. Radiat. Prot. Dosim. 2019, 185, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.J.; Magee, J.S. Assessment of eye and body dose for interventional radiologists, cardiologists, and other interventional staff. J. Radiol. Prot. 2013, 33, 445–460. [Google Scholar] [CrossRef]
- Chida, K.; Morishima, Y.; Masuyama, H.; Chiba, H.; Katahira, Y.; Inaba, Y.; Mori, I.; Maruoka, S.; Takahashi, S.; Kohzuki, M.; et al. Effect of radiation monitoring method and formula differences on estimated physician dose during percutaneous coronary intervention. Acta Radiol. 2009, 50, 170–173. [Google Scholar] [CrossRef]
- Vano, E.; Sanchez, R.M.; Fernández, J.M. Strategies to optimise occupational radiation protection in interventional cardiology using simultaneous registration of patient and staff doses. J. Radiol. Prot. 2018, 38, 1077–1088. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Chida, K.; Ishida, T.; Toyoshima, H.; Yoshida, Y.; Yoshioka, S.; Moroi, J.; Kinoshita, T. Occupational radiation ex-posure of the eye in neurovascular interventional physician. Radiat. Prot. Dosim. 2019, 185, 151–156. [Google Scholar] [CrossRef]
- Kato, M.; Chida, K.; Ishida, T.; Sasaki, F.; Toyoshima, H.; Oosaka, H.; Terata, K.; Abe, Y.; Kinoshita, T. Occupational radiation exposure dose of the eye in department of cardiac arrhythmia physician. Radiat. Prot. Dosim. 2019, 187, 361–368. [Google Scholar] [CrossRef]
- Ross, A.M.; Segal, J.; Borenstein, D.; Jenkins, E.; Cho, S. Prevalence of spinal disc disease among interventional cardiologists. Am. J. Cardiol. 1997, 79, 68–70. [Google Scholar] [CrossRef]
- Goldstein, J.A.; Balter, S.; Cowley, M.; Hodgson, J.; Klein, L.W. Interventional committee of the society of cardiovascular interventions occupational hazards of interventional cardiologists: Prevalence of orthopedic health problems in contemporary practice. Catheter. Cardiovasc. Interv. 2004, 63, 407–411. [Google Scholar] [CrossRef]
- Pleis, J.R.; Ward, B.W.; Lucas, J.W. Summary health statistics for US adults: National Health Interview Survey, 2009. Vital Health Stat. 2010, 249, 1–207. [Google Scholar]
- Yaffe, M.J.; Mawdsley, G.E.; Lilley, M.; Servant, R.; Reh, G. Composite materials for X-ray protection. Health Phys. 1991, 60, 661–664. [Google Scholar] [CrossRef]
- Zuguchi, M.; Chida, K.; Taura, M.; Inaba, Y.; Ebata, A.; Yamada, S. Usefulness of non-lead aprons in radiation protection for physicians performing interventional procedures. Radiat. Prot. Dosim. 2008, 131, 531–534. [Google Scholar] [CrossRef]
- Chida, K.; Inaba, Y.; Saito, H.; Ishibashi, T.; Takahashi, S.; Kohzuki, M.; Zuguchi, M. Radiation dose of interventional radiology system using a flat-panel detector. Am. J. Roentgenol. 2009, 193, 1680–1685. [Google Scholar] [CrossRef]
- Chida, K.; Ohno, T.; Kakizaki, S.; Takegawa, M.; Yuuki, H.; Nakada, M.; Takahashi, S.; Zuguchi, M. Radiation dose to the pediatric cardiac catheterization and intervention patient. Am. J. Roentgenol. 2010, 195, 1175–1179. [Google Scholar] [CrossRef]
- Chida, K.; Inaba, Y.; Morishima, Y.; Taura, M.; Ebata, A.; Yanagawa, I.; Takeda, K.; Zuguchi, M. Comparison of dose at an interventional reference point between the displayed estimated value and measured value. Radiol. Phys. Technol. 2011, 4, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Nakamura, M.; Chida, K.; Zuguchi, M. Effectiveness of a novel real-time dosimeter in interventional radiology: A comparison of new and old radiation sensors. Radiol. Phys. Technol. 2018, 11, 445–450. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Radiological Protection (ICRP). Radiological Protection in Cardiology; ICRP Publication 120; Elsevier: Amsterdam, The Netherlands, 2013; Volume 42, Available online: https://journals.sagepub.com/doi/pdf/10.1177/ANIB_42_1 (accessed on 28 August 2021).
- Inaba, Y.; Nakamura, M.; Zuguchi, M.; Chida, K. Development of novel real-time radiation systems using 4-channel sensors. Sensors 2020, 20, 2741. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Chida, K.; Nakamura, M.; Toyoshima, H.; Terata, K.; Abe, Y. New real-time patient radiation dosimeter for use in radiofrequency catheter ablation. J. Radiat. Res. 2019, 60, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Inaba, Y.; Chida, K.; Kobayashi, R.; Zuguchi, M. A cross-sectional study of the radiation dose and image quality of X-ray equipment used in IVR. J. Appl. Clin. Med. Phys. 2016, 17, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Chida, K.; Kato, M.; Saito, H.; Ishibashi, T.; Takahashi, S.; Kohzuki, M.; Zuguchi, M. Optimizing patient radiation dose in intervention procedures. Acta Radiol. 2010, 51, 33–39. [Google Scholar] [CrossRef]
- International Commission on Radiological Protection (ICRP). Avoidance of Radiation Injuries from Medical Interventional Procedures; ICRP Publication 85; Pergamon: Oxford, UK, 2000; Volume 30, Available online: https://journals.sagepub.com/doi/pdf/10.1177/ANIB_30_2 (accessed on 28 August 2021).
- Vañó, E.; González, L.; Beneytez, F.; Moreno, F. Lens injuries induced by occupational exposure in non-optimized interventional radiology laboratories. Br. J. Radiol. 1998, 71, 728–733. [Google Scholar] [CrossRef]
- Kato, M.; Chida, K.; Sato, T.; Oosaka, H.; Tosa, T.; Munehisa, M.; Kadowaki, K. The necessity of follow-up for radiation skin injuries in patients after percutaneous coronary interventions: Radiation skin injuries will often be overlooked clinically. Acta Radiol. 2012, 53, 1040–1044. [Google Scholar] [CrossRef] [PubMed]
- Koenig, A.; Maas, J.; Viniol, S.; Etzel, R.; Fiebich, M.; Thomas, R.; Mahnken, A. Scatter radiation reduction with a radiation-absorbing pad in interventional radiology examinations. Eur. J. Radiol. 2020, 132, 109245. [Google Scholar] [CrossRef]
- Chida, K.; Takahashi, T.; Ito, D.; Shimura, H.; Takeda, K.; Zuguchi, M. Clarifying and visualizing sources of staff-received scattered radiation in interventional procedures. Am. J. Roentgenol. 2011, 197, W900–W903. [Google Scholar] [CrossRef]
- Chida, K.; Morishima, Y.; Inaba, Y.; Taura, M.; Ebata, A.; Takeda, K.; Shimura, H.; Zuguchi, M. Physician-received scatter radiation with angiography systems used for interventional radiology: Comparison among many X-ray systems. Radiat. Prot. Dosim. 2011, 149, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Chida, K.; Kobayashi, R.; Kaga, Y.; Zuguchi, M. Fundamental study of a real-time occupational dosimetry system for interventional radiology staff. J. Radiol. Prot. 2014, 34, N65–N71. [Google Scholar] [CrossRef]
- Kuon, E.; Schmitt, M.; Dahm, J.B. Significant reduction of radiation exposure to operator and staff during cardiac interventions by analysis of radiation leakage and improved lead shielding. Am. J. Cardiol. 2002, 89, 44–49. [Google Scholar] [CrossRef]
- Haga, Y.; Chida, K.; Kimura, Y.; Yamanda, S.; Sota, M.; Abe, M.; Kaga, Y.; Meguro, T.; Zuguchi, M. Radiation eye dose to medical staff during respiratory endoscopy under X-ray fluoroscopy. J. Radiat. Res. 2020, 61, 691–696. [Google Scholar] [CrossRef]
- Endo, M.; Haga, Y.; Sota, M.; Tanaka, A.; Otomo, K.; Murabayashi, Y.; Abe, M.; Kaga, Y.; Inaba, Y.; Suzuki, M.; et al. Evaluation of novel X-ray protective eyewear in reducing the eye dose to interventional radiology physicians. J. Radiat. Res. 2021, 62, 414–419. [Google Scholar] [CrossRef]
- Inaba, Y.; Hitachi, S.; Watanuki, M.; Chida, K. Occupational radiation dose to eye lenses in CT-guided interventions using MDCT-fluoroscopy. Diagnostics 2021, 11, 646. [Google Scholar] [CrossRef] [PubMed]
- Morishima, Y.; Chida, K.; Muroya, Y.; Utsumi, Y. Effectiveness of a New lead-shielding device and additional filter for reducing staff and patient radiation exposure during videofluoroscopic swallowing study using a human phantom. Dysphagia 2018, 33, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Morishima, Y.; Chida, K.; Meguro, T. Effectiveness of additional lead shielding to protect staff from scattering radiation during endoscopic retrograde cholangiopancreatography procedures. J. Radiat. Res. 2018, 59, 225–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishii, H.; Haga, Y.; Sota, M.; Inaba, Y.; Chida, K. Performance of the DOSIRIS™ eye lens dosimeter. J. Radiol. Prot. 2019, 39, N19–N26. [Google Scholar] [CrossRef]
- Morishima, Y.; Chida, K.; Katahira, Y. The effectiveness of additional lead-shielding drape and low pulse rate fluoroscopy in protecting staff from scatter radiation during cardiac resynchronization therapy (CRT). Jpn. J. Radiol. 2019, 37, 95–101. [Google Scholar] [CrossRef] [Green Version]
- Dixon, R.G.; Khiatani, V.; Statler, J.D.; Walser, E.M.; Midia, M.; Miller, D.L.; Bartal, G.; Collins, J.D.; Gross, K.A.; Stecker, M.S.; et al. Society of interventional radiology: Occupational back and neck pain and the interventional radiologist. J. Vasc. Interv. Radiol. 2017, 28, 195–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornelis, F.H.; Razakamanantsoa, L.; Ammar, M.B.; Lehrer, R.; Haffaf, I.; El-Mouhadi, S.; Gardavaud, F.; Najdawi, M.; Barral, M. Ergonomics in interventional radiology: Awareness is mandatory. Medicina 2021, 57, 500. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Protective Apron | Number of Procedures | Cumulative AK | Fluoroscopy Time | ||
|---|---|---|---|---|---|
| Pb-Equivalent [mm] | Total | CAG | PCI | [Mean ± SD, mGy] | [Mean ± SD, min] |
| Non-lead | 78 | 32 | 46 | 1345.7 ± 1378.9 | 34.5 ± 27.7 |
| 0.25 | |||||
| Non-lead | 51 | 19 | 27 | 1345.3 ± 1637.3 | 31.7 ± 27.1 |
| 0.35 | |||||
| Lead | 50 | 23 | 27 | 1037.2 ± 824.7 | 30.4 ± 21.7 |
| 0.25 | |||||
| Lead | 50 | 26 | 24 | 812.3 ± 704.9 | 21.2 ± 15.5 |
| 0.35 | |||||
| Protective Apron | Apron Weight | Outside (External) Dose | Inside (Internal) Dose | Shielding Effects | Comfortably |
|---|---|---|---|---|---|
| Pb-Equivalent [mm] | [kg] | [Mean ± SD, μSv] | [Mean ± SD, μSv] | [%] | |
| Non-lead | 1.8 | 142.6 ± 199.3 | 5.5 ± 7.1 | 96.1 | Excellent |
| 0.25 | |||||
| Non-lead | 2.9 | 123.9 ± 99.3 | 1.8 ± 1.5 | 98.5 | Good |
| 0.35 | |||||
| Lead | 3.0 | 166.4 ± 153.6 | 4.6 ± 4.7 | 97.3 | Somewhat poor |
| 0.25 | |||||
| Lead | 3.8 | 209.2 ± 163.1 | 2.2 ± 1.9 | 98.9 | Very poor |
| 0.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kato, M.; Chida, K.; Munehisa, M.; Sato, T.; Inaba, Y.; Suzuki, M.; Zuguchi, M. Non-Lead Protective Aprons for the Protection of Interventional Radiology Physicians from Radiation Exposure in Clinical Settings: An Initial Study. Diagnostics 2021, 11, 1613. https://doi.org/10.3390/diagnostics11091613
Kato M, Chida K, Munehisa M, Sato T, Inaba Y, Suzuki M, Zuguchi M. Non-Lead Protective Aprons for the Protection of Interventional Radiology Physicians from Radiation Exposure in Clinical Settings: An Initial Study. Diagnostics. 2021; 11(9):1613. https://doi.org/10.3390/diagnostics11091613
Chicago/Turabian StyleKato, Mamoru, Koichi Chida, Masato Munehisa, Tadaya Sato, Yohei Inaba, Masatoshi Suzuki, and Masayuki Zuguchi. 2021. "Non-Lead Protective Aprons for the Protection of Interventional Radiology Physicians from Radiation Exposure in Clinical Settings: An Initial Study" Diagnostics 11, no. 9: 1613. https://doi.org/10.3390/diagnostics11091613