
Cholesterol Efflux Capacity Associates with the Ankle-Brachial Index but Not All-Cause Mortality in Patients with Peripheral Artery Disease

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
3.2. Determinants of CEC in PAD Patients
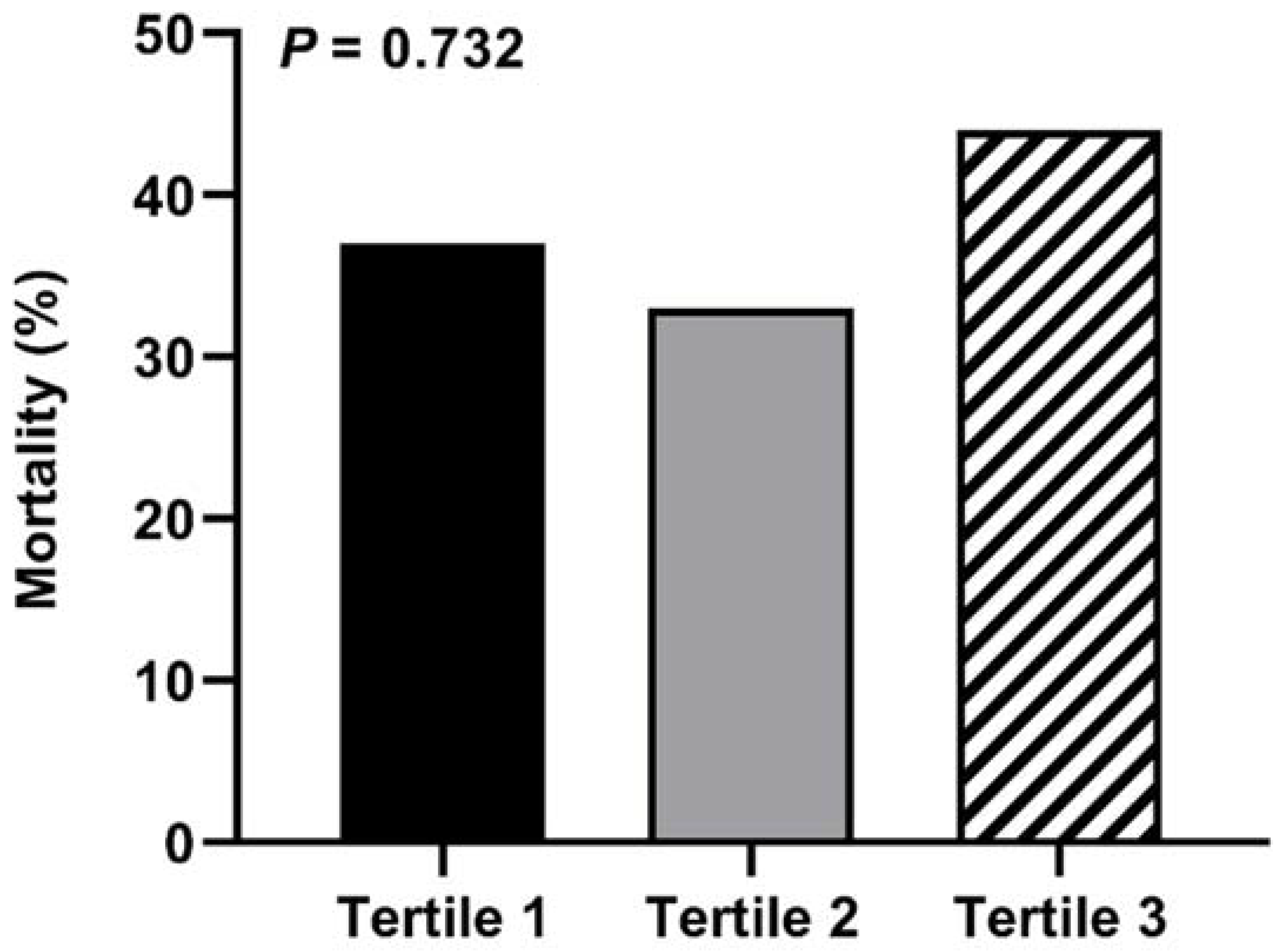
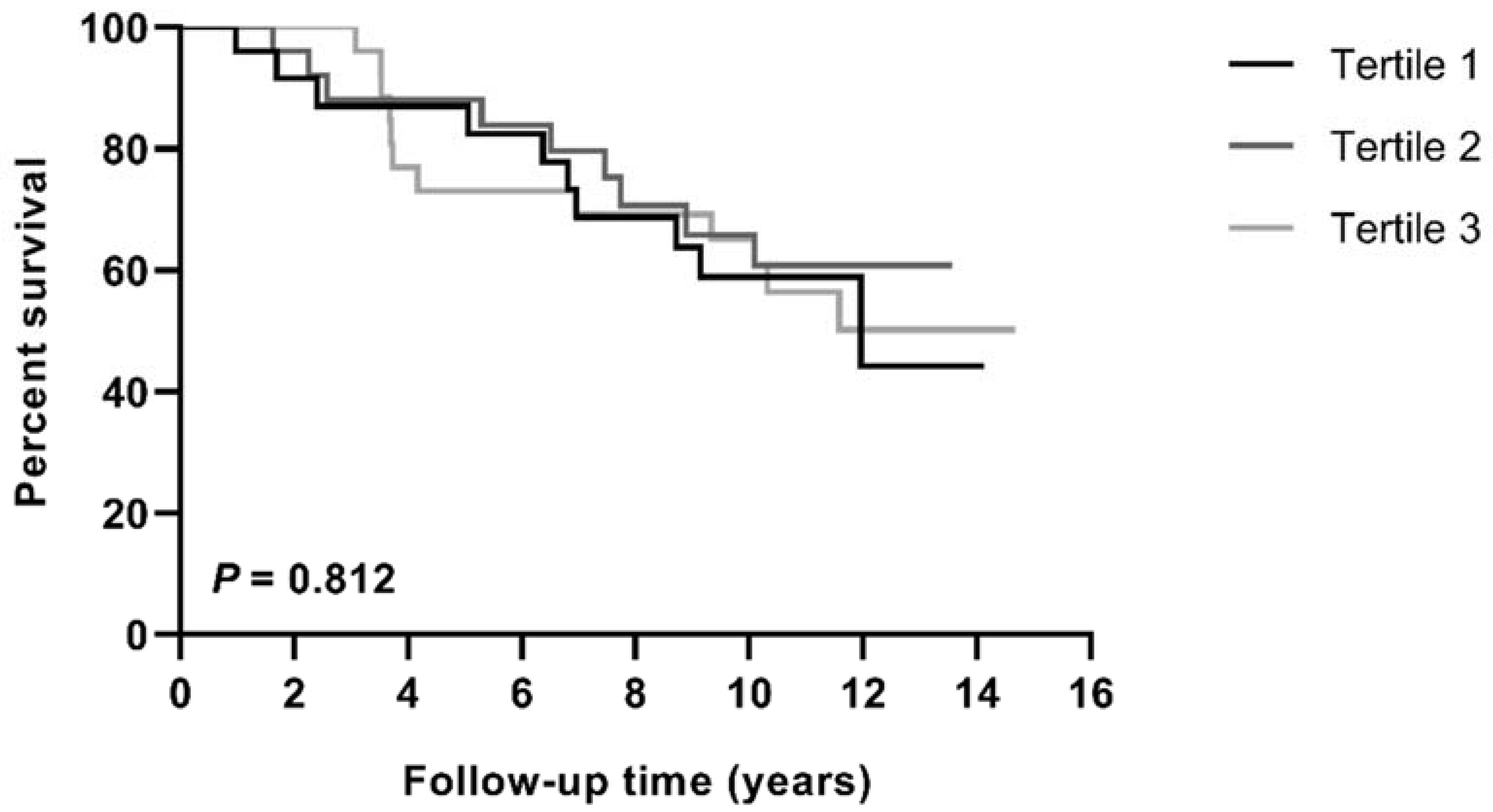
3.3. Association of Cholesterol Efflux with All-Cause Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Diehm, C.; Schuster, A.; Allenberg, J.R.; Darius, H.; Haberl, R.; Lange, S.; Pittrow, D.; von Stritzky, B.; Tepohl, G.; Trampisch, H.J. High prevalence of peripheral arterial disease and co-morbidity in 6880 primary care patients: Cross-sectional study. Atherosclerosis 2004, 172, 95–105. [Google Scholar] [CrossRef]
- Campia, U.; Gerhard-Herman, M.; Piazza, G.; Goldhaber, S.Z. Peripheral Artery Disease: Past, Present, and Future. Am. J. Med. 2019, 132, 1133–1141. [Google Scholar] [CrossRef]
- Alberts, M.J.; Bhatt, D.L.; Mas, J.L.; Ohman, E.M.; Hirsch, A.T.; Rother, J.; Salette, G.; Goto, S.; Smith, S.C., Jr.; Liau, C.S.; et al. Three-year follow-up and event rates in the international REduction of Atherothrombosis for Continued Health Registry. Eur. Heart J. 2009, 30, 2318–2326. [Google Scholar] [CrossRef] [Green Version]
- Marz, W.; Kleber, M.E.; Scharnagl, H.; Speer, T.; Zewinger, S.; Ritsch, A.; Parhofer, K.G.; von Eckardstein, A.; Landmesser, U.; Laufs, U. HDL cholesterol: Reappraisal of its clinical relevance. Clin. Res. Cardiol. 2017, 106, 663–675. [Google Scholar] [CrossRef] [Green Version]
- Annema, W.; von Eckardstein, A. Dysfunctional high-density lipoproteins in coronary heart disease: Implications for diagnostics and therapy. Transl. Res. 2016, 173, 30–57. [Google Scholar] [CrossRef] [Green Version]
- Rohatgi, A.; Khera, A.; Berry, J.D.; Givens, E.G.; Ayers, C.R.; Wedin, K.E.; Neeland, I.J.; Yuhanna, I.S.; Rader, D.R.; de Lemos, J.A.; et al. HDL cholesterol efflux capacity and incident cardiovascular events. N. Engl. J. Med. 2014, 371, 2383–2393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saleheen, D.; Scott, R.; Javad, S.; Zhao, W.; Rodrigues, A.; Picataggi, A.; Lukmanova, D.; Mucksavage, M.L.; Luben, R.; Billheimer, J.; et al. Association of HDL cholesterol efflux capacity with incident coronary heart disease events: A prospective case-control study. Lancet Diabetes Endocrinol. 2015, 3, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Shea, S.; Stein, J.H.; Jorgensen, N.W.; McClelland, R.L.; Tascau, L.; Shrager, S.; Heinecke, J.W.; Yvan-Charvet, L.; Tall, A.R. Cholesterol Mass Efflux Capacity, Incident Cardiovascular Disease, and Progression of Carotid Plaque. Arter. Thromb. Vasc. Biol. 2019, 39, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Soria-Florido, M.T.; Schroder, H.; Grau, M.; Fito, M.; Lassale, C. High density lipoprotein functionality and cardiovascular events and mortality: A systematic review and meta-analysis. Atherosclerosis 2020, 302, 36–42. [Google Scholar] [CrossRef]
- Liu, C.; Zhang, Y.; Ding, D.; Li, X.; Yang, Y.; Li, Q.; Zheng, Y.; Wang, D.; Ling, W. Cholesterol efflux capacity is an independent predictor of all-cause and cardiovascular mortality in patients with coronary artery disease: A prospective cohort study. Atherosclerosis 2016, 249, 116–124. [Google Scholar] [CrossRef]
- Guerin, M.; Silvain, J.; Gall, J.; Darabi, M.; Berthet, M.; Frisdal, E.; Hauguel-Moreau, M.; Zeitouni, M.; Kerneis, M.; Lattuca, B.; et al. Association of Serum Cholesterol Efflux Capacity With Mortality in Patients With ST-Segment Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2018, 72, 3259–3269. [Google Scholar] [CrossRef] [PubMed]
- Ritsch, A.; Scharnagl, H.; März, W. HDL cholesterol efflux capacity and cardiovascular events. N. Engl. J. Med. 2015, 372, 1870–1871. [Google Scholar] [CrossRef]
- Ritsch, A.; Duerr, A.; Kahler, P.; Hunjadi, M.; Stojakovic, T.; Silbernagel, G.; Scharnagl, H.; Kleber, M.E.; März, W. Cholesterol Efflux Capacity and Cardiovascular Disease: The Ludwigshafen Risk and Cardiovascular Health (LURIC) Study. Biomedicines 2020, 8, 524. [Google Scholar] [CrossRef] [PubMed]
- Touboul, P.J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Fatar, M.; et al. Mannheim carotid intima-media thickness consensus (2004–2006). An update on behalf of the Advisory Board of the 3rd and 4th Watching the Risk Symposium, 13th and 15th European Stroke Conferences, Mannheim, Germany, 2004, and Brussels, Belgium, 2006. Cerebrovasc. Dis. 2007, 23, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Scharnagl, H.; Heuschneider, C.; Sailer, S.; Kleber, M.E.; März, W.; Ritsch, A. Decreased cholesterol efflux capacity in patients with low cholesteryl ester transfer protein plasma levels. Eur. J. Clin. Investig. 2014, 44, 395–401. [Google Scholar] [CrossRef]
- Hunjadi, M.; Lamina, C.; Kahler, P.; Bernscherer, T.; Viikari, J.; Lehtimäki, T.; Kähönen, M.; Hurme, M.; Juonala, M.; Taittonen, L.; et al. HDL cholesterol efflux capacity is inversely associated with subclinical cardiovascular risk markers in young adults: The cardiovascular risk in Young Finns study. Sci. Rep. 2020, 10, 19223. [Google Scholar] [CrossRef]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Bjorck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [CrossRef] [Green Version]
- Clemens, R.K.; Annema, W.; Baumann, F.; Roth-Zetzsche, S.; Seifert, B.; von Eckardstein, A.; Amann-Vesti, B.R. Cardiac biomarkers but not measures of vascular atherosclerosis predict mortality in patients with peripheral artery disease. Clin. Chim. Acta Int. J. Clin. Chem. 2019, 495, 215–220. [Google Scholar] [CrossRef]
- Yoon, H.J.; Kim, K.H.; Park, H.; Cho, J.Y.; Hong, Y.J.; Park, H.W.; Kim, J.H.; Ahn, Y.; Jeong, M.H.; Cho, J.G.; et al. Carotid plaque rather than intima-media thickness as a predictor of recurrent vascular events in patients with acute ischemic stroke. Cardiovasc. Ultrasound 2017, 15, 19. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Fang, X.; Hua, Y.; Tang, Z.; Guan, S.; Wu, X.; Liu, H.; Liu, B.; Wang, C.; Zhang, Z.; et al. Carotid Artery Plaques, Carotid Intima-Media Thickness, and Risk of Cardiovascular Events and All-Cause Death in Older Adults: A 5-Year Prospective, Community-Based Study. Angiology 2018, 69, 120–129. [Google Scholar] [CrossRef]
- Otaki, Y.; Takahashi, H.; Watanabe, T.; Yamaura, G.; Funayama, A.; Arimoto, T.; Shishido, T.; Miyamoto, T.; Kubota, I. Heart-type fatty acid binding protein and high-sensitivity troponin T are myocardial damage markers that could predict adverse clinical outcomes in patients with peripheral artery disease. BBA Clin. 2015, 4, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Linnemann, B.; Sutter, T.; Herrmann, E.; Sixt, S.; Rastan, A.; Schwarzwaelder, U.; Noory, E.; Buergelin, K.; Beschorner, U.; Zeller, T. Elevated cardiac troponin T is associated with higher mortality and amputation rates in patients with peripheral arterial disease. J. Am. Coll. Cardiol. 2014, 63, 1529–1538. [Google Scholar] [CrossRef] [Green Version]
- Singh, T.P.; Morris, D.R.; Smith, S.; Moxon, J.V.; Golledge, J. Systematic Review and Meta-Analysis of the Association Between C-Reactive Protein and Major Cardiovascular Events in Patients with Peripheral Artery Disease. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2017, 54, 220–233. [Google Scholar] [CrossRef]
- Qiu, C.; Zhao, X.; Zhou, Q.; Zhang, Z. High-density lipoprotein cholesterol efflux capacity is inversely associated with cardiovascular risk: A systematic review and meta-analysis. Lipids Health Dis. 2017, 16, 212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annema, W.; Dikkers, A.; de Boer, J.F.; Dullaart, R.P.; Sanders, J.S.; Bakker, S.J.; Tietge, U.J. HDL Cholesterol Efflux Predicts Graft Failure in Renal Transplant Recipients. J. Am. Soc. Nephrol. 2016, 27, 595–603. [Google Scholar] [CrossRef] [Green Version]
- Cahill, L.E.; Sacks, F.M.; Rimm, E.B.; Jensen, M.K. Cholesterol efflux capacity, HDL cholesterol, and risk of coronary heart disease: A nested case-control study in men. J. Lipid Res. 2019, 60, 1457–1464. [Google Scholar] [CrossRef]
- Li, X.M.; Tang, W.H.; Mosior, M.K.; Huang, Y.; Wu, Y.; Matter, W.; Gao, V.; Schmitt, D.; Didonato, J.A.; Fisher, E.A.; et al. Paradoxical association of enhanced cholesterol efflux with increased incident cardiovascular risks. Arter. Thromb. Vasc. Biol. 2013, 33, 1696–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, P.K.; Jorgensen, N.W.; McClelland, R.L.; Allison, M.; Stein, J.H.; Yvan-Chavret, L.; Tall, A.R.; Shea, S. Cholesterol mass efflux capacity and risk of peripheral artery disease: The Multi-Ethnic Study of Atherosclerosis. Atherosclerosis 2020, 297, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Yubero-Serrano, E.M.; Alcala-Diaz, J.F.; Gutierrez-Mariscal, F.M.; Arenas-de Larriva, A.P.; Pena-Orihuela, P.J.; Blanco-Rojo, R.; Martinez-Botas, J.; Torres-Pena, J.D.; Perez-Martinez, P.; Ordovas, J.M.; et al. Association between cholesterol efflux capacity and peripheral artery disease in coronary heart disease patients with and without type 2 diabetes: From the CORDIOPREV study. Cardiovasc. Diabetol. 2021, 20, 72. [Google Scholar] [CrossRef] [PubMed]
- Albaghdadi, M.S.; Wang, Z.; Gao, Y.; Mutharasan, R.K.; Wilkins, J. High-Density Lipoprotein Subfractions and Cholesterol Efflux Capacity Are Not Affected by Supervised Exercise but Are Associated with Baseline Interleukin-6 in Patients with Peripheral Artery Disease. Front. Cardiovasc. Med. 2017, 4, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, K.S.; Mikhailidis, D.P.; Hamilton, G.; Seifalian, A.M. A review of the carotid and femoral intima-media thickness as an indicator of the presence of peripheral vascular disease and cardiovascular risk factors. Cardiovasc. Res. 2002, 54, 528–538. [Google Scholar] [CrossRef] [Green Version]
- Gepner, A.D.; Young, R.; Delaney, J.A.; Tattersall, M.C.; Blaha, M.J.; Post, W.S.; Gottesman, R.F.; Kronmal, R.; Budoff, M.J.; Burke, G.L.; et al. Comparison of coronary artery calcium presence, carotid plaque presence, and carotid intima-media thickness for cardiovascular disease prediction in the Multi-Ethnic Study of Atherosclerosis. Circ. Cardiovasc. Imaging 2015, 8, e002262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowkes, F.G.; Aboyans, V.; Fowkes, F.J.; McDermott, M.M.; Sampson, U.K.; Criqui, M.H. Peripheral artery disease: Epidemiology and global perspectives. Nat. Rev. Cardiol. 2017, 14, 156–170. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Kumbhani, D.J.; Steg, P.G.; Cannon, C.P.; Eagle, K.A.; Smith, S.C., Jr.; Goto, S.; Ohman, E.M.; Elbez, Y.; Sritara, P.; Baumgartner, I.; et al. Statin therapy and long-term adverse limb outcomes in patients with peripheral artery disease: Insights from the REACH registry. Eur. Heart J. 2014, 35, 2864–2872. [Google Scholar] [CrossRef] [Green Version]
- Heart Protection Study Collaborative Group. Randomized trial of the effects of cholesterol-lowering with simvastatin on peripheral vascular and other major vascular outcomes in 20,536 people with peripheral arterial disease and other high-risk conditions. J. Vasc. Surg. 2007, 45, 645–654.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridker, P.M.; Stampfer, M.J.; Rifai, N. Novel risk factors for systemic atherosclerosis: A comparison of C-reactive protein, fibrinogen, homocysteine, lipoprotein(a), and standard cholesterol screening as predictors of peripheral arterial disease. JAMA 2001, 285, 2481–2485. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Criqui, M.H.; Denenberg, J.O.; Knoke, J.D.; Ridker, P.M.; Fronek, A. Risk factors for progression of peripheral arterial disease in large and small vessels. Circulation 2006, 113, 2623–2629. [Google Scholar] [CrossRef] [Green Version]
- Criqui, M.H.; Vargas, V.; Denenberg, J.O.; Ho, E.; Allison, M.; Langer, R.D.; Gamst, A.; Bundens, W.P.; Fronek, A. Ethnicity and peripheral arterial disease: The San Diego Population Study. Circulation 2005, 112, 2703–2707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Aguilar, E.; Orbe, J.; Fernandez-Montero, A.; Fernandez-Alonso, S.; Rodriguez, J.A.; Fernandez-Alonso, L.; Paramo, J.A.; Roncal, C. Reduced high-density lipoprotein cholesterol: A valuable, independent prognostic marker in peripheral arterial disease. J. Vasc. Surg. 2017, 66, 1527–1533.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| First (n = 27) | Second (n = 27) | Third (n = 27) | p-Value | |
|---|---|---|---|---|
| CEC | 85.0 (79.0–88.5) | 99.0 (95.5–102.0) | 118.0 (111.0–135.0) | <0.001 |
| Patient Characteristics | ||||
| Male gender, n (%) | 22 (82) | 21 (78) | 21 (79) | 0.928 |
| Age, years | 68.3 ± 8.9 | 68.5 ± 11.5 | 66.2 ± 8.9 | 0.648 |
| Smoking, n (%) | 19 (70) | 12 (44) | 14 (52) | 0.142 |
| History of MI, n (%) | 12 (44) | 5 (19) a | 4 (15) b | 0.026 |
| History of CVA, n (%) | 15 (56) | 12 (44) | 11 (41) | 0.525 |
| Diabetes, n (%) | 10 (37) | 5 (19) | 7 (26) | 0.306 |
| Dyslipidemia, n (%) | 21 (78) | 18 (67) | 23 (85) | 0.271 |
| Hypertension, n (%) | 22 (82) | 21 (78) | 22 (82) | 0.925 |
| BMI, kg/m2 | 25.6 (24.1–28.5) | 25.7 (23.3–29.0) | 24.0 (22.0–27.8) | 0.223 |
| Lipid Profile | ||||
| Cholesterol, mmol/L | 4.2 ± 1.1 | 4.5 ± 1.1 | 4.6 ± 0.9 | 0.317 |
| HDL-cholesterol, mmol/L | 1.16 ± 0.36 | 1.25 ± 0.34 | 1.42 ± 0.41 b | 0.033 |
| LDL-cholesterol, mmol/L | 2.5 ± 1.8 | 2.7 ± 0.6 | 3.0 ± 0.8 | 0.665 |
| Non-HDL cholesterol, mmol/L | 3.0 ± 1.2 | 3.3 ± 1.0 | 3.2 ± 0.8 | 0.721 |
| Triglycerides, mmol/L | 1.95 (1.51–3.00) | 1.50 (0.98–1.99) | 2.01 (1.12–2.52) | 0.051 |
| ApoA-I, g/L | 1.36 ± 0.24 | 1.48 ± 0.21 | 1.56 ± 0.28 b | 0.012 |
| ApoB, g/L | 0.94 ± 0.17 | 0.90 ± 0.22 | 0.92 ± 0.19 | 0.688 |
| Lp(a), mg/L | 224 (77–701) | 150 (47–212) | 146 (38–565) | 0.401 |
| Homocysteine, µmol/L | 14.7 (12.2–19.3) | 13.7 (11.5–16.0) | 12.9 (10.7–15.0) | 0.171 |
| Inflammation | ||||
| CRP, mg/L | 4.1 (2.2–6.3) | 3.1 (1.6–6.4) | 2.8 (1.3–4.8) | 0.424 |
| Kidney Function | ||||
| eGFR, ml/min/1.73 m2 | 67 ± 20 | 70 ± 20 | 63 ± 21 | 0.410 |
| Extent of PAD | ||||
| ABI | 0.76 ± 0.17 | 0.80 ± 0.23 | 0.89 ± 0.18 b | 0.042 |
| cIMT, mm | 0.78 ± 0.13 | 0.77 ± 0.16 | 0.76 ± 0.11 | 0.792 |
| Fontaine stage | 0.596 | |||
| Stage I | 11 (41) | 10 (37) | 11 (41) | |
| Stage IIa | 7 (26) | 11 (41) | 12 (44) | |
| Stage IIb | 8 (30) | 4 (15) | 4 (15) | |
| Stage IIc | 1 (4) | 2 (7) | 0 (0) | |
| Stage III | 0 (0) | 0 (0) | 0 (0) | |
| Stage IV | 0 (0) | 0 (0) | 0 (0) |
| Determinant | β Coefficient | p-Value |
|---|---|---|
| Patient Characteristics | ||
| Age | −0.149 | 0.183 |
| BMI | −0.164 | 0.134 |
| Lipid Profile | ||
| Cholesterol | 0.028 | 0.800 |
| HDL-cholesterol | 0.333 | 0.003 |
| Non-HDL cholesterol | −0.093 | 0.398 |
| LDL-cholesterol | −0.112 | 0.616 |
| Triglycerides | −0.155 | 0.158 |
| ApoA-I | 0.363 | 0.001 |
| ApoB | −0.060 | 0.584 |
| Lp(a) | −0.179 | 0.119 |
| Homocystein | −0.161 | 0.154 |
| Inflammation | ||
| CRP | −0.141 | 0.204 |
| Kidney Function | ||
| eGFR | −0.186 | 0.089 |
| Extent of PAD | ||
| ABI | 0.258 | 0.018 |
| cIMT | −0.085 | 0.456 |
| HR Per 1-SD Increment [95%CI] | p-Value | |
|---|---|---|
| Crude | 0.843 (0.587–1.208) | 0.352 |
| Corrected for gender | 0.867 (0.599–1.255) | 0.449 |
| Corrected for age and gender | 0.925 (0.639–1.340) | 0.680 |
| Corrected for age, gender, and HDL-C | 0.953 (0.651–1.398) | 0.807 |
| Corrected for age, gender, and ABI | 0.932 (0.625–1.389) | 0.729 |
| Corrected for age, gender, and smoking | 0.992 (0.675–1.457) | 0.967 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clemens, R.K.; Hunjadi, M.; Ritsch, A.; Rohrer, L.; Meier, T.O.; Amann-Vesti, B.; von Eckardstein, A.; Annema, W. Cholesterol Efflux Capacity Associates with the Ankle-Brachial Index but Not All-Cause Mortality in Patients with Peripheral Artery Disease. Diagnostics 2021, 11, 1407. https://doi.org/10.3390/diagnostics11081407
Clemens RK, Hunjadi M, Ritsch A, Rohrer L, Meier TO, Amann-Vesti B, von Eckardstein A, Annema W. Cholesterol Efflux Capacity Associates with the Ankle-Brachial Index but Not All-Cause Mortality in Patients with Peripheral Artery Disease. Diagnostics. 2021; 11(8):1407. https://doi.org/10.3390/diagnostics11081407
Chicago/Turabian StyleClemens, Robert K., Monika Hunjadi, Andreas Ritsch, Lucia Rohrer, Thomas O. Meier, Beatrice Amann-Vesti, Arnold von Eckardstein, and Wijtske Annema. 2021. "Cholesterol Efflux Capacity Associates with the Ankle-Brachial Index but Not All-Cause Mortality in Patients with Peripheral Artery Disease" Diagnostics 11, no. 8: 1407. https://doi.org/10.3390/diagnostics11081407